
Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and Risk of All-Cause Mortality and Cardiovascular Mortality: A 20-Year Follow-Up Cohort Study of 42,875 US Adults

Abstract
:1. Introduction
2. Materials and Methods
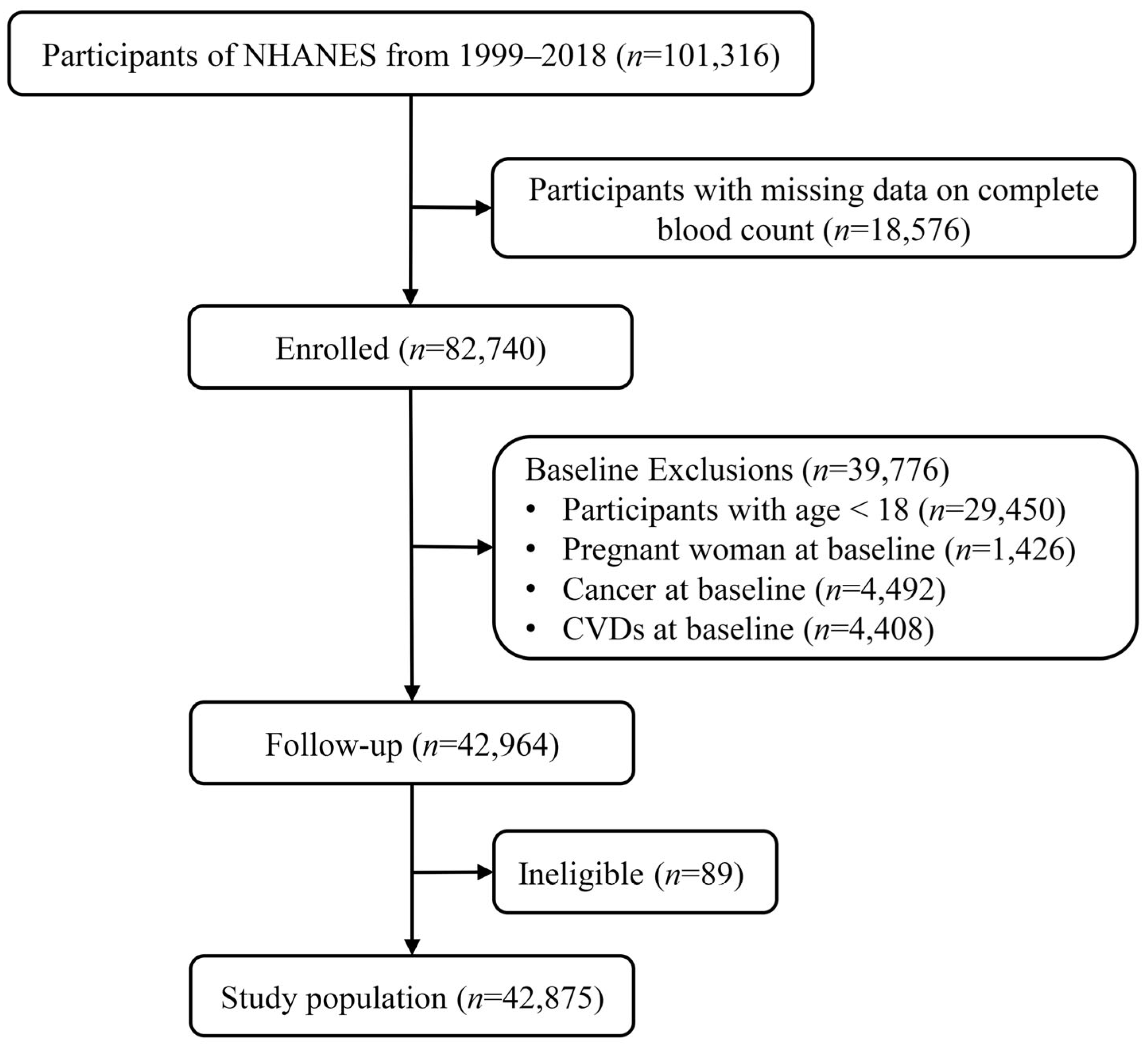
2.1. Study Design and Participants
2.2. Definition of SII and SIRI and Classification into Groups
2.3. Determination of Mortality Outcomes
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Population Stratified by SII/SIRI
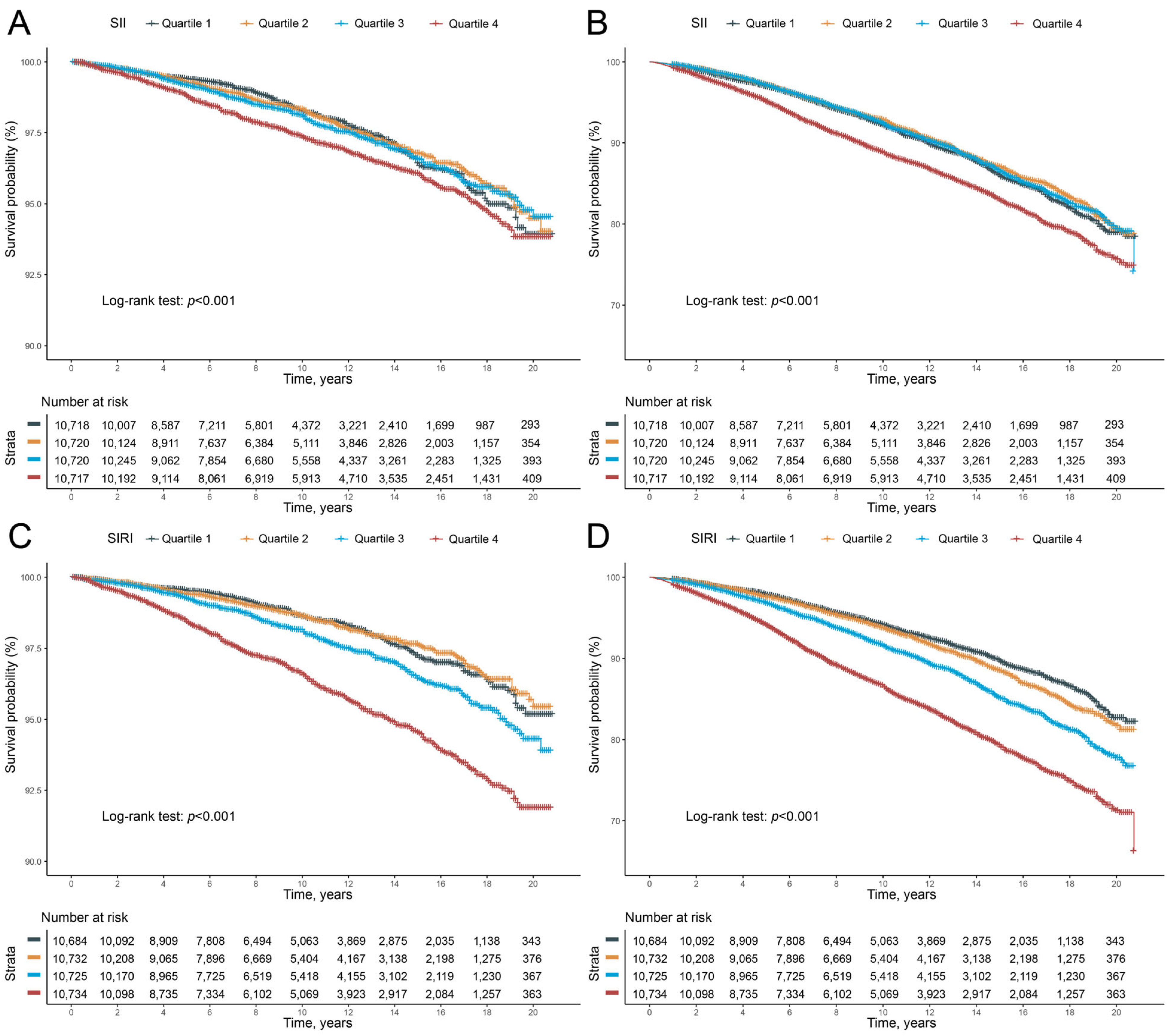
3.2. Prediction of All-Cause Mortality and Cardiovascular Mortality with SII
3.3. Prediction of All-Cause Mortality and Cardiovascular Mortality with SIRI
3.4. Subgroup Analysis
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lancet, T. An epidemic of risk factors for cardiovascular disease. Lancet 2011, 377, 527. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risks. J. Am. Coll. Cardiol. 2020, 76, 2980–2981. [Google Scholar] [CrossRef] [PubMed]
- Dhande, I.; Doris, P. Genomics and Inflammation in Cardiovascular Disease. Compr. Physiol. 2021, 11, 2433–2454. [Google Scholar] [CrossRef]
- Baena-Díez, J.M.; Garcia-Gil, M.; Comas-Cufí, M.; Ramos, R.; Prieto-Alhambra, D.; Salvador-González, B.; Elosua, R.; Dégano, I.R.; Peñafiel, J.; Grau, M. Association between chronic immune-mediated inflammatory diseases and cardiovascular risk. Heart 2018, 104, 119–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyss, C.A.; Neidhart, M.; Altwegg, L.; Spanaus, K.S.; Yonekawa, K.; Wischnewsky, M.B.; Corti, R.; Kucher, N.; Roffi, M.; Eberli, F.R.; et al. Cellular actors, Toll-like receptors, and local cytokine profile in acute coronary syndromes. Eur. Heart J. 2010, 31, 1457–1469. [Google Scholar] [CrossRef]
- Chaudhury, A.; Noiret, L.; Higgins, J.M. White blood cell population dynamics for risk stratification of acute coronary syndrome. Proc. Natl. Acad. Sci. USA 2017, 114, 12344–12349. [Google Scholar] [CrossRef] [Green Version]
- Mehu, M.; Narasimhulu, C.A.; Singla, D.K. Inflammatory Cells in Atherosclerosis. Antioxidants 2022, 11, 233. [Google Scholar] [CrossRef]
- Zayani, Y.; Allal-Elasmi, M.; Jacob, M.P.; Zidi, W.; Zaroui, A.; Feki, M.; Mourali, S.; Mechmech, R.; Kaabachi, N. Peripheral blood levels of matrix and inflammatory mediators are elevated in Tunisian patients with acute coronary syndromes. Clin. Lab. 2013, 59, 169–175. [Google Scholar] [CrossRef]
- Fiechter, M.; Ghadri, J.R.; Jaguszewski, M.; Siddique, A.; Vogt, S.; Haller, R.B.; Halioua, R.; Handzic, A.; Kaufmann, P.A.; Corti, R.; et al. Impact of inflammation on adverse cardiovascular events in patients with acute coronary syndromes. J. Cardiovasc. Med. 2013, 14, 807–814. [Google Scholar] [CrossRef]
- Mo, X.; Li, T.; Ji, G.; Lu, W.; Hu, Z. Peripheral polymorphonuclear leukocyte activation as a systemic inflammatory response in ischemic stroke. Neurol. Sci. 2013, 34, 1509–1516. [Google Scholar] [CrossRef]
- Mrdjen, D.; Hartmann, F.J.; Becher, B. High Dimensional Cytometry of Central Nervous System Leukocytes During Neuroinflammation. Inflammation 2017, 1559, 321–332. [Google Scholar] [CrossRef]
- Maimaiti, S.; Muhanmode, Y.; Maimaitirexiati, X. The role and prognostic value of human peripheral blood interleukin-27, C-reactive protein and serum amyloid A in inflammatory response of sepsis. Minerva Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Dentali, F.; Nigro, O.; Squizzato, A.; Gianni, M.; Zuretti, F.; Grandi, A.M.; Guasti, L. Impact of neutrophils to lymphocytes ratio on major clinical outcomes in patients with acute coronary syndromes: A systematic review and meta-analysis of the literature. Int. J. Cardiol. 2018, 266, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Liu, H.; Wang, H.; Tao, Q.; Lin, X.; Ge, S.; Zhai, Z. The Predictive Value of Potential Hematological Biomarkers in Acute Coronary Syndrome. Clin. Lab. 2019, 65, e181232. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Chen, R.; Liu, L.; Liu, X.; Hou, J.; Liao, J.; Zhang, P.; Huang, J.; Lu, L.; Chen, L.; et al. Systemic immune-inflammation index and incident cardiovascular diseases among middle-aged and elderly Chinese adults: The Dongfeng-Tongji cohort study. Atherosclerosis 2021, 323, 20–29. [Google Scholar] [CrossRef]
- Jin, Z.; Wu, Q.; Chen, S.; Gao, J.; Li, X.; Zhang, X.; Zhou, Y.; He, D.; Cheng, Z.; Zhu, Y.; et al. The Associations of Two Novel Inflammation Indexes, SII and SIRI with the Risks for Cardiovascular Diseases and All-Cause Mortality: A Ten-Year Follow-Up Study in 85,154 Individuals. J. Inflamm. Res. 2021, 14, 131–140. [Google Scholar] [CrossRef]
- Li, J.; He, D.; Yu, J.; Chen, S.; Wu, Q.; Cheng, Z.; Wei, Q.; Xu, Y.; Zhu, Y.; Wu, S. Dynamic Status of SII and SIRI Alters the Risk of Cardiovascular Diseases: Evidence from Kailuan Cohort Study. J. Inflamm. Res. 2022, 15, 5945–5957. [Google Scholar] [CrossRef]
- Hua, X.; Duan, F.; Zhai, W.; Song, C.; Jiang, C.; Wang, L.; Huang, J.; Lin, H.; Yuan, Z. A Novel Inflammatory-Nutritional Prognostic Scoring System for Patients with Early-Stage Breast Cancer. J. Inflamm. Res. 2022, 15, 381–394. [Google Scholar] [CrossRef]
- Ye, Z.; Hu, T.; Wang, J.; Xiao, R.; Liao, X.; Liu, M.; Sun, Z. Systemic immune-inflammation index as a potential biomarker of cardiovascular diseases: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 886995. [Google Scholar] [CrossRef]
- Lin, K.-B.; Fan, F.-H.; Cai, M.-Q.; Yu, Y.; Fu, C.-L.; Ding, L.-Y.; Sun, Y.-D.; Sun, J.-W.; Shi, Y.-W.; Dong, Z.-F.; et al. Systemic immune inflammation index and system inflammation response index are potential biomarkers of atrial fibrillation among the patients presenting with ischemic stroke. Eur. J. Med. Res. 2022, 27, 1–8. [Google Scholar] [CrossRef]
- Brämer, G. International Statistical Classification of Diseases and Related Health Problems; Tenth Revision; WHO: Geneva, The Switzerland, 1988; pp. 32–36. [Google Scholar]
- Lee, J.-S.; Park, J.; Kim, J. Dietary factors related to hypertension risk in Korean adults-data from the Korean national health and nutrition examination survey III. Nutr. Res. Pract. 2011, 5, 60–65. [Google Scholar] [CrossRef] [Green Version]
- WHO Expert Committee. Physical status: The use and interpretation of anthropometry. World Health Organ. Tech. Rep. Ser. 1995, 854, 312–344. [Google Scholar]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, E.K.; Blair, S.N.; Franklin, A.B.; Macera, A.C.; Heath, G.W.; Thompson, P.D.; Bauman, A.; et al. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081–1093. [Google Scholar] [CrossRef] [Green Version]
- Giavarina, D.; Husain-Syed, F.; Ronco, C. Clinical Implications of the New Equation to Estimate Glomerular Filtration Rate. Nephron 2021, 145, 508–512. [Google Scholar] [CrossRef]
- Azambuja, M.I.R. Inflammation as the cause of coronary heart disease. Lancet Infect. Dis. 2010, 10, 142–143. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, Q.; Wang, R.; Ji, H.; Chen, Y.; Quan, X.-Q.; Zhang, C. Systemic Immune-Inflammatory Index Predicts Clinical Outcomes for Elderly Patients with Acute Myocardial Infarction Receiving Percutaneous Coronary Intervention. Experiment 2019, 25, 9690–9701. [Google Scholar] [CrossRef]
- Esenboğa, K.; Kurtul, A.; Yamantürk, Y.Y.; Tan, T.S.; Tutar, D.E. Systemic immune-inflammation index predicts no-reflow phenomenon after primary percutaneous coronary intervention. Acta Cardiol. 2021, 77, 59–65. [Google Scholar] [CrossRef]
- Bağcı, A.; Aksoy, F. Systemic immune–inflammation index predicts new-onset atrial fibrillation after ST elevation myocardial infarction. Biomarkers Med. 2021, 15, 731–739. [Google Scholar] [CrossRef]
- Sayın, M.R.; Özderya, A.; Konuş, A.H.; Yerlikaya, M.G.; Maz, M.A.; Çırakoğlu, F.; Uzun, G.; Kara, F. The use of systemic immune-inflammation index to predict new onset atrial fibrillation in the context of acute coronary syndrome. Kardiologiia 2022, 62, 59–64. [Google Scholar] [CrossRef]
- Li, J.; Yuan, Y.; Liao, X.; Yu, Z.; Li, H.; Zheng, J. Prognostic Significance of Admission Systemic Inflammation Response Index in Patients With Spontaneous Intracerebral Hemorrhage: A Propensity Score Matching Analysis. Front. Neurol. 2021, 12, 718032. [Google Scholar] [CrossRef]
- Dong, X.; Nao, J.; Gao, Y. Peripheral Monocyte Count Predicts Outcomes in Patients with Acute Ischemic Stroke Treated with rtPA Thrombolysis. Neurotox. Res. 2019, 37, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Vedder, D.; Gerritsen, M.; Nurmohamed, M.T.; van Vollenhoven, R.F.; Lood, C. A neutrophil signature is strongly associated with increased cardiovascular risk in gout. Rheumatology 2020, 60, 2783–2790. [Google Scholar] [CrossRef] [PubMed]
- Rogacev, K.S.; Cremers, B.; Zawada, A.M.; Seiler, S.; Binder, N.; Ege, P.; Große-Dunker, G.; Heisel, I.; Hornof, F.; Jeken, J.; et al. CD14++CD16+ Monocytes Independently Predict Cardiovascular Events. J. Am. Coll. Cardiol. 2012, 60, 1512–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.-L.; Wu, C.-H.; Hsu, P.-F.; Chen, S.-C.; Huang, S.-S.; Chan, W.L.; Lin, S.-J.; Chou, C.-Y.; Chen, J.-W.; Pan, J.-P.; et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur. J. Clin. Investig. 2020, 50, e13230. [Google Scholar] [CrossRef]
- Zhou, Y.-X.; Li, W.-C.; Xia, S.-H.; Xiang, T.; Tang, C.; Luo, J.-L.; Lin, M.-J.; Xia, X.-W.; Wang, W.-B. Predictive Value of the Systemic Immune Inflammation Index for Adverse Outcomes in Patients With Acute Ischemic Stroke. Front. Neurol. 2022, 13, 836595. [Google Scholar] [CrossRef]
- Aziz, M.H.; Sideras, K.; Aziz, N.A.; Mauff, K.; Haen, R.; Roos, D.; Saida, L.; Suker, M.; van der Harst, E.; Mieog, J.S.; et al. The Systemic-immune-inflammation Index Independently Predicts Survival and Recurrence in Resectable Pancreatic Cancer and its Prognostic Value Depends on Bilirubin Levels. Ann. Surg. 2019, 270, 139–146. [Google Scholar] [CrossRef]
- Taqueti, V.R.; Di Carli, M.F.; Jerosch-Herold, M.; Sukhova, G.K.; Murthy, V.L.; Folco, E.J.; Kwong, R.Y.; Ozaki, C.K.; Belkin, M.; Nahrendorf, M.; et al. Increased Microvascularization and Vessel Permeability Associate With Active Inflammation in Human Atheromata. Circ. Cardiovasc. Imaging 2014, 7, 920–929. [Google Scholar] [CrossRef] [Green Version]
- von Ungern-Sternberg, S.N.I.; Vogel, S.; Walker-Allgaier, B.; Geue, S.; Maurer, A.; Wild, A.-M.; Münzer, P.; Chatterjee, M.; Heinzmann, D.; Kremmer, E.; et al. Extracellular Cyclophilin A Augments Platelet-Dependent Thrombosis and Thromboinflammation. Thromb. Haemost. 2017, 117, 2063–2078. [Google Scholar] [CrossRef]
- Kim, K.H.; Barazia, A.; Cho, J. Real-time Imaging of Heterotypic Platelet-neutrophil Interactions on the Activated Endothelium During Vascular Inflammation and Thrombus Formation in Live Mice. JoVE 2013, 74, e50329. [Google Scholar] [CrossRef] [Green Version]
- Ankeny, R.F.; Hinds, M.T.; Nerem, R.M. Dynamic Shear Stress Regulation of Inflammatory and Thrombotic Pathways in Baboon Endothelial Outgrowth Cells. Tissue Eng. Part A 2013, 19, 1573–1582. [Google Scholar] [CrossRef] [Green Version]
- Milan-Mattos, J.; Anibal, F.; Perseguini, N.; Minatel, V.; Rehder-Santos, P.; Castro, C.; Vasilceac, F.; Mattiello, S.; Faccioli, L.; Catai, A. Effects of natural aging and gender on pro-inflammatory markers. Braz. J. Med. Biol. Res. 2019, 52, e8392. [Google Scholar] [CrossRef] [Green Version]
- Guan, Y.; Zhang, C.; Lyu, G.; Huang, X.; Zhang, X.; Zhuang, T.; Jia, L.; Zhang, L.; Zhang, C.; Li, C.; et al. Senescence-activated enhancer landscape orchestrates the senescence-associated secretory phenotype in murine fibroblasts. Nucleic Acids Res. 2020, 48, 10909–10923. [Google Scholar] [CrossRef]
- Yousefzadeh, M.J.; Flores, R.R.; Zhu, Y.; Schmiechen, Z.C.; Brooks, R.W.; Trussoni, C.E.; Cui, Y.; Angelini, L.; Lee, K.A.; McGowan, S.J.; et al. An aged immune system drives senescence and ageing of solid organs. Nature 2021, 594, 100–105. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Quartiles of SII | p Value | |||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | ||
| Participants, n | 10,718 | 10,720 | 10,720 | 10,717 | |
| Age, years | 44.47 (18.10) | 44.44 (17.80) | 44.21 (17.79) | 44.69 (18.54) | 0.298 |
| Male, % | 5895 (55.0) | 5453 (50.9) | 5108 (47.6) | 4627 (43.2) | <0.001 |
| Race/ethnicity, % | <0.001 | ||||
| Mexican American | 1736 (16.2) | 2210 (20.6) | 2323 (21.7) | 2309 (21.5) | |
| Other Hispanic | 862 (8.0) | 1000 (9.3) | 961 (9.0) | 904 (8.4) | |
| Non-Hispanic White | 3125 (29.2) | 4186 (39.0) | 4655 (43.4) | 5063 (47.2) | |
| Non-Hispanic Black | 3755 (35.0) | 2170 (20.2) | 1776 (16.6) | 1586 (14.8) | |
| Other race | 1240 (11.6) | 1154 (10.8) | 1005 (9.4) | 855 (8.0) | |
| Education level, % | 0.001 | ||||
| Below high school | 2906 (27.1) | 2929 (27.3) | 2931 (27.3) | 2949 (27.5) | |
| High school | 2336 (21.8) | 2305 (21.5) | 2449 (22.8) | 2543 (23.7) | |
| Above high school | 5476 (51.1) | 5486 (51.2) | 5340 (49.8) | 5225 (48.8) | |
| Poverty, % | 2358 (22.0) | 2223 (20.7) | 2274 (21.2) | 2388 (22.3) | 0.022 |
| Smoking status, % | <0.001 | ||||
| Never smokers | 6451 (60.2) | 6386 (59.6) | 6240 (58.2) | 5831 (54.4) | |
| Former smokers | 2127 (19.8) | 2185 (20.4) | 2145 (20.0) | 2239 (20.9) | |
| Current smokers | 2140 (20.0) | 2149 (20.0) | 2335 (21.8) | 2647 (24.7) | |
| Drinking status, % | <0.001 | ||||
| Non-drinkers | 2430 (22.7) | 2436 (22.7) | 2242 (20.9) | 2446 (22.8) | |
| Low-to-moderate drinkers | 7488 (69.9) | 7516 (70.1) | 7656 (71.4) | 7345 (68.5) | |
| Heavy drinkers | 800 (7.5) | 768 (7.2) | 822 (7.7) | 926 (8.6) | |
| BMI status, % | 0.011 | ||||
| <25.0 | 3841 (35.8) | 3454 (32.2) | 3237 (30.2) | 3340 (31.2) | |
| 25.0–29.9 | 3603 (33.6) | 3677 (34.3) | 3566 (33.3) | 3241 (30.2) | |
| >29.9 | 3274 (30.5) | 3589 (33.5) | 3917 (36.5) | 4136 (38.6) | |
| Physical activity, % | <0.001 | ||||
| Inactive | 2475 (23.1) | 2482 (23.2) | 2632 (24.6) | 2922 (27.3) | |
| Insufficiently active | 3786 (35.3) | 3988 (37.2) | 4150 (38.7) | 4133 (38.6) | |
| Active | 4457 (41.6) | 4250 (39.6) | 3938 (36.7) | 3662 (34.2) | |
| Energy intake, kcal/day | 1984.00 [1473.37, 2600.50] | 1977.00 [1494.00, 2595.00] | 1960.50 [1472.00, 2568.62] | 1922.50 [1462.50, 2535.50] | <0.001 |
| eGFR, mL/min/1.73 m2 | 100.52 (22.87) | 100.14 (22.58) | 100.33 (23.06) | 99.22 (24.54) | <0.001 |
| ALT, U/L | 21.00 [16.00, 29.00] | 21.00 [16.00, 29.00] | 21.00 [16.00, 29.00] | 20.00 [15.00, 27.00] | <0.001 |
| AST, U/L | 23.00 [20.00, 28.00] | 23.00 [19.00, 27.00] | 22.00 [19.00, 27.00] | 22.00 [18.00, 26.00] | <0.001 |
| Hypertension, % | 2837 (26.5) | 2788 (26.0) | 2859 (26.7) | 3110 (29.0) | <0.001 |
| Diabetes, % | 905 (8.4) | 966 (9.0) | 875 (8.2) | 1030 (9.6) | 0.001 |
| WBC count, 103/μL | 5.80 [4.90, 6.90] | 6.60 [5.60, 7.70] | 7.20 [6.10, 8.40] | 8.20 [6.90, 9.90] | <0.001 |
| Neutrophils count, 103/μL | 2.80 [2.20, 3.40] | 3.60 [3.00, 4.30] | 4.30 [3.60, 5.10] | 5.50 [4.60, 6.70] | <0.001 |
| Monocyte count, 103/μL | 0.50 [0.40, 0.60] | 0.50 [0.40, 0.60] | 0.50 [0.40, 0.70] | 0.60 [0.50, 0.70] | <0.001 |
| Lymphocyte count, 103/μL | 2.30 [1.90, 2.80] | 2.20 [1.80, 2.60] | 2.00 [1.70, 2.50] | 1.80 [1.50, 2.30] | <0.001 |
| Platelet count, 103/μL | 211.00 [180.00, 243.00] | 238.00 [209.00, 273.00] | 260.00 [227.00, 297.00] | 294.00 [253.00, 342.00] | <0.001 |
| SIRI | 0.57 [0.42, 0.77] | 0.87 [0.68, 1.10] | 1.14 [0.89, 1.45] | 1.69 [1.25, 2.31] | <0.001 |
| Variables | Quartiles of SIRI | p Value | |||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | ||
| Participants, n | 10,684 | 10,732 | 10,725 | 10,734 | |
| Age, years | 43.05 (17.06) | 43.98 (17.48) | 44.58 (17.99) | 46.19 (19.47) | <0.001 |
| Male, % | 4616 (43.2) | 5031 (46.9) | 5429 (50.6) | 6007 (56.0) | <0.001 |
| Race/ethnicity, % | <0.001 | ||||
| Mexican American | 1797 (16.8) | 2340 (21.8) | 2297 (21.4) | 2144 (20.0) | |
| Other Hispanic | 828 (7.7) | 1013 (9.4) | 975 (9.1) | 911 (8.5) | |
| Non-Hispanic White | 2642 (24.7) | 4105 (38.3) | 4834 (45.1) | 5448 (50.8) | |
| Non-Hispanic Black | 4075 (38.1) | 2154 (20.1) | 1645 (15.3) | 1413 (13.2) | |
| Other race | 1342 (12.6) | 1120 (10.4) | 974 (9.1) | 818 (7.6) | |
| Education level, % | <0.001 | ||||
| Below high school | 2795 (26.2) | 2969 (27.7) | 2941 (27.4) | 3010 (28.0) | |
| High school | 2229 (20.9) | 2352 (21.9) | 2400 (22.4) | 2652 (24.7) | |
| Above high school | 5660 (53.0) | 5411 (50.4) | 5384 (50.2) | 5072 (47.3) | |
| Poverty, % | 2348 (22.0) | 2270 (21.2) | 2258 (21.1) | 2367 (22.1) | 0.150 |
| Smoking status, % | <0.001 | ||||
| Never smokers | 6897 (64.6) | 6473 (60.3) | 6151 (57.4) | 5387 (50.2) | |
| Former smokers | 1905 (17.8) | 2203 (20.5) | 2177 (20.3) | 2411 (22.5) | |
| Current smokers | 1882 (17.6) | 2056 (19.2) | 2397 (22.3) | 2936 (27.4) | |
| Drinking status, % | <0.001 | ||||
| Non-drinkers | 2716 (25.4) | 2381 (22.2) | 2281 (21.3) | 2176 (20.3) | |
| Low-to-moderate drinkers | 7273 (68.1) | 7598 (70.8) | 7611 (71.0) | 7523 (70.1) | |
| Heavy drinkers | 695 (6.5) | 753 (7.0) | 833 (7.8) | 1035 (9.6) | |
| BMI status, % | <0.001 | ||||
| <25.0 | 3898 (36.5) | 3469 (32.3) | 3220 (30.0) | 3285 (30.6) | |
| 25.0–29.9 | 3501 (32.8) | 3616 (33.7) | 3541 (33.0) | 3429 (31.9) | |
| >29.9 | 3285 (30.7) | 3647 (34.0) | 3964 (37.0) | 4020 (37.5) | |
| Physical activity, % | <0.001 | ||||
| Inactive | 2520 (23.6) | 2560 (23.9) | 2549 (23.8) | 2882 (26.8) | |
| Insufficiently active | 3927 (36.8) | 4078 (38.0) | 4084 (38.1) | 3968 (37.0) | |
| Active | 4237 (39.7) | 4094 (38.1) | 4092 (38.2) | 3884 (36.2) | |
| Energy intake, kcal/day | 1913.00 [1439.00, 2503.00] | 1955.05 [1467.00, 2570.38] | 1977.00 [1496.68, 2586.00] | 1999.00 [1498.00, 2631.97] | <0.001 |
| eGFR, ml/min/1.73 m2 | 103.09 (22.07) | 100.83 (22.09) | 99.40 (23.06) | 96.91 (25.30) | <0.001 |
| ALT, U/L | 20.00 [15.00, 27.00] | 21.00 [16.00, 29.00] | 21.00 [16.00, 29.00] | 21.00 [16.00, 29.00] | <0.001 |
| AST, U/L | 22.00 [19.00, 27.00] | 22.00 [19.00, 27.00] | 22.00 [19.00, 27.00] | 22.00 [19.00, 27.00] | 0.902 |
| Hypertension, % | 2642 (24.7) | 2718 (25.3) | 2860 (26.7) | 3374 (31.4) | <0.001 |
| Diabetes, % | 796 (7.5) | 908 (8.5) | 941 (8.8) | 1131 (10.5) | <0.001 |
| WBC count, 103/μL | 5.50 [4.70, 6.50] | 6.50 [5.60, 7.60] | 7.30 [6.30, 8.50] | 8.60 [7.30, 10.10] | <0.001 |
| Neutrophils count, 103/μL | 2.70 [2.20, 3.20] | 3.60 [3.10, 4.20] | 4.40 [3.70, 5.10] | 5.60 [4.70, 6.70] | <0.001 |
| Monocyte count, 103/μL | 0.40 [0.30, 0.50] | 0.50 [0.40, 0.60] | 0.60 [0.50, 0.70] | 0.70 [0.60, 0.80] | <0.001 |
| Lymphocyte count, 103/μL | 2.20 [1.80, 2.70] | 2.10 [1.70, 2.60] | 2.10 [1.70, 2.60] | 1.90 [1.50, 2.40] | <0.001 |
| Platelet count, 103/μL | 239.00 [203.00, 281.00] | 246.00 [210.00, 289.00] | 251.00 [214.00, 296.00] | 258.50 [218.00, 305.00] | <0.001 |
| SII | 291.19 [219.20, 375.67] | 413.77 [332.81, 518.14] | 523.89 [422.93, 653.14] | 748.52 [590.89, 983.48] | <0.001 |
| Q1 | Q2 | Q3 | Q4 | p Trend | |
|---|---|---|---|---|---|
| Levels of SII | <335.36 | 355.36–468.83 | 468.84–655.55 | >655.56 | |
| Cardiovascular mortality | |||||
| No. deaths/total | 203/10,718 | 222/10,720 | 249/10,720 | 324/10,717 | |
| Crude | Reference | 1.00 (0.83–1.21) | 1.05 (0.88–1.27) | 1.32 (1.11–1.57) | 0.002 |
| Model 1 | Reference | 1.12 (0.92–1.35) | 1.20 (0.99–1.45) | 1.43 (1.19–1.71) | 0.001 |
| Model 2 | Reference | 1.09 (0.90–1.32) | 1.16 (0.96–1.40) | 1.33 (1.11–1.59) | 0.015 |
| All-cause mortality | |||||
| No. deaths/total | 897/10,718 | 923/10,720 | 1008/10,720 | 1422/10,717 | |
| Crude | Reference | 0.94 (0.86–1.03) | 0.97 (0.88–1.06) | 1.31 (1.21–1.43) | <0.001 |
| Model 1 | Reference | 1.01 (0.92–1.11) | 1.05 (0.96–1.15) | 1.38 (1.26–1.50) | <0.001 |
| Model 2 | Reference | 0.99 (0.91–1.09) | 1.03 (0.94–1.13) | 1.29 (1.18–1.41) | <0.001 |
| Q1 | Q2 | Q3 | Q4 | p Trend | |
|---|---|---|---|---|---|
| Levels of SIRI | <0.68 | 0.68–0.98 | 0.99–1.42 | >1.43 | |
| Cardiovascular mortality | |||||
| No. deaths/total | 177/10,684 | 181/10,732 | 246/10,725 | 394/10,734 | |
| Crude | Reference | 0.98 (0.80–1.21) | 1.35 (1.12–1.64) | 2.26 (1.89–2.70) | <0.001 |
| Model 1 | Reference | 0.90 (0.73–1.12) | 1.18 (0.96–1.44) | 1.60 (1.32–1.94) | <0.001 |
| Model 2 | Reference | 0.88 (0.71–1.09) | 1.10 (0.90–1.34) | 1.39 (1.14–1.68) | <0.001 |
| All-cause mortality | |||||
| No. deaths/total | 737/10,684 | 851/10,732 | 1080/10,725 | 1582/10,734 | |
| Crude | Reference | 1.11 (1.01–1.22) | 1.43 (1.30–1.57) | 2.18 (2.00–2.38) | <0.001 |
| Model 1 | Reference | 1.01 (0.91–1.12) | 1.22 (1.11–1.35) | 1.57 (1.43–1.72) | <0.001 |
| Model 2 | Reference | 0.99 (0.90–1.10) | 1.16 (1.05–1.28) | 1.39 (1.26–1.52) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xia, Y.; Xia, C.; Wu, L.; Li, Z.; Li, H.; Zhang, J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and Risk of All-Cause Mortality and Cardiovascular Mortality: A 20-Year Follow-Up Cohort Study of 42,875 US Adults. J. Clin. Med. 2023, 12, 1128. https://doi.org/10.3390/jcm12031128
Xia Y, Xia C, Wu L, Li Z, Li H, Zhang J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and Risk of All-Cause Mortality and Cardiovascular Mortality: A 20-Year Follow-Up Cohort Study of 42,875 US Adults. Journal of Clinical Medicine. 2023; 12(3):1128. https://doi.org/10.3390/jcm12031128
Chicago/Turabian StyleXia, Yiyuan, Chunlei Xia, Lida Wu, Zheng Li, Hui Li, and Junxia Zhang. 2023. "Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and Risk of All-Cause Mortality and Cardiovascular Mortality: A 20-Year Follow-Up Cohort Study of 42,875 US Adults" Journal of Clinical Medicine 12, no. 3: 1128. https://doi.org/10.3390/jcm12031128