
Implant-Supported Overdentures: Current Status and Preclinical Testing of a Novel Attachment System


Abstract
:1. Introduction
2. Materials and Methods
2.1. Retrospective Analysis of Complications
2.2. Patient Survey
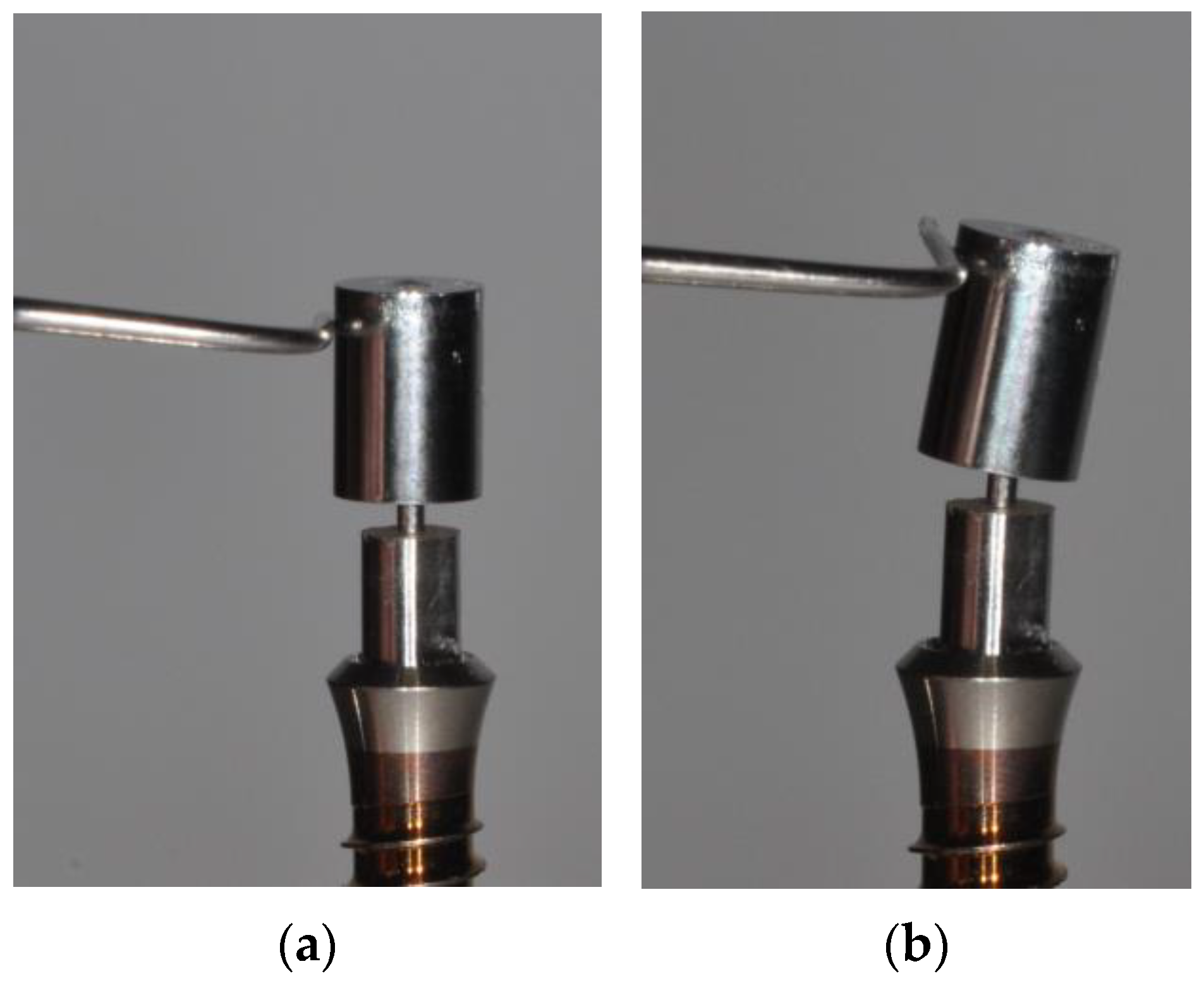
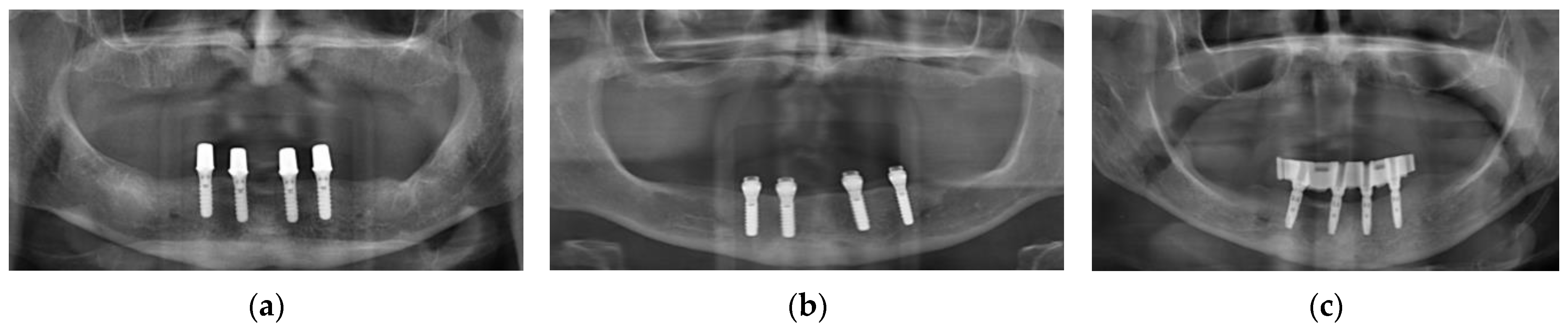
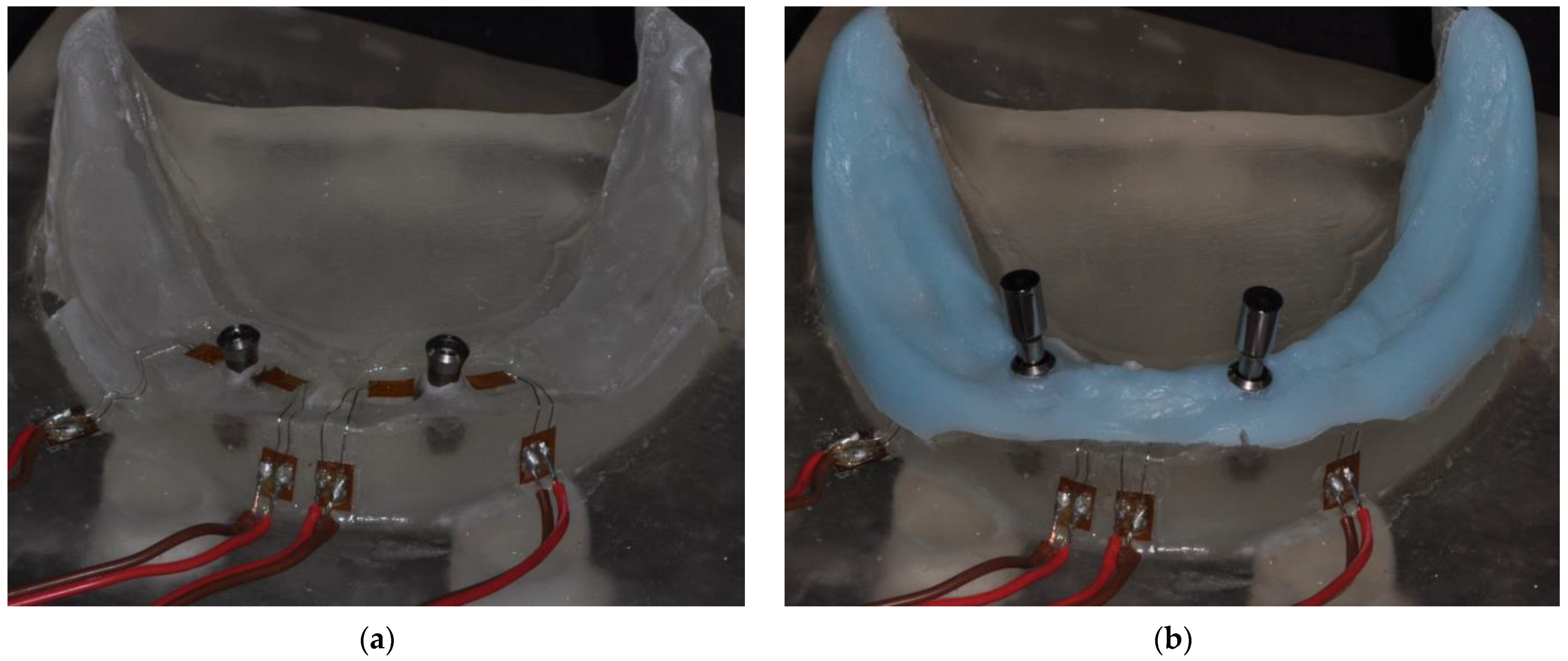
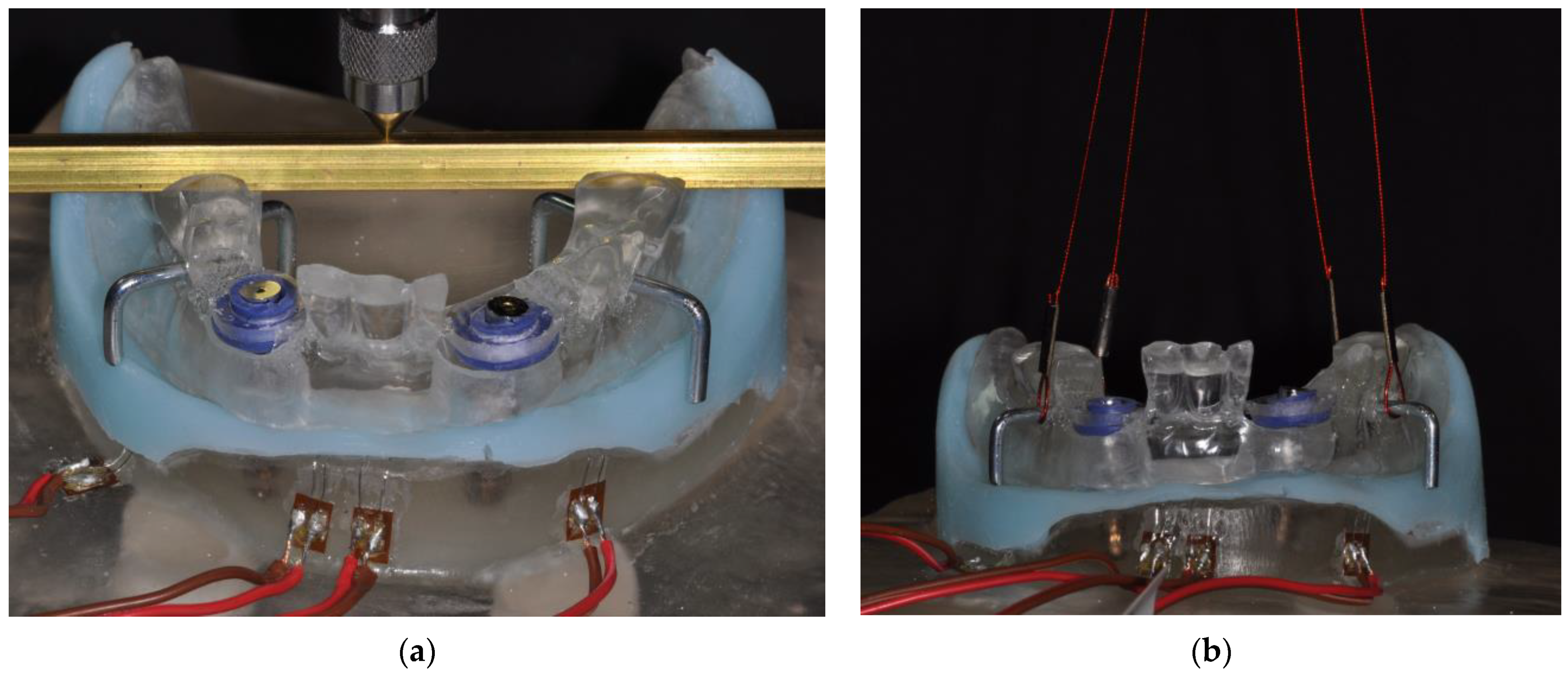
2.3. Testing of a Novel Attachment System
3. Results
3.1. Retrospective Analysis of Complications
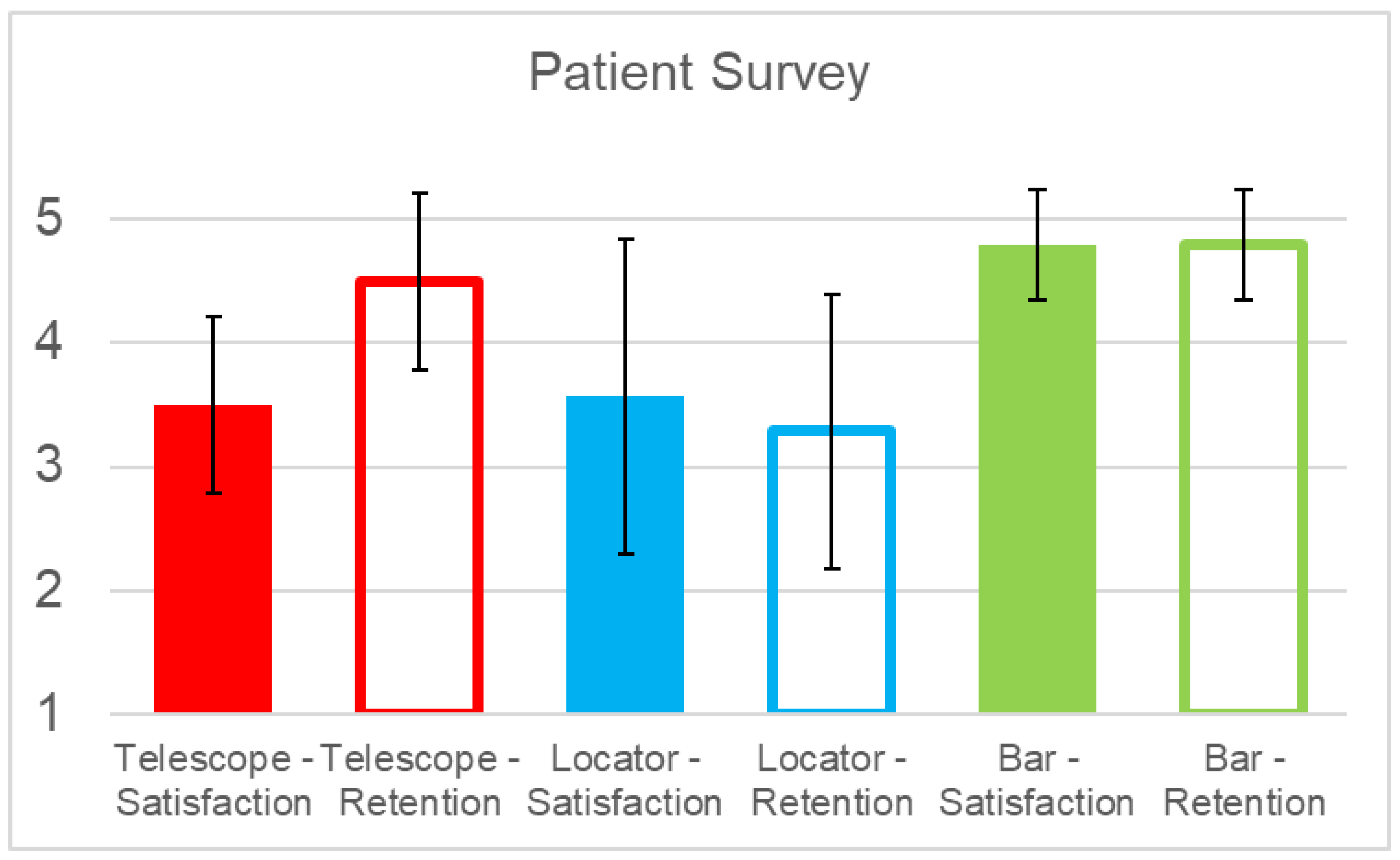
3.2. Patient Survey
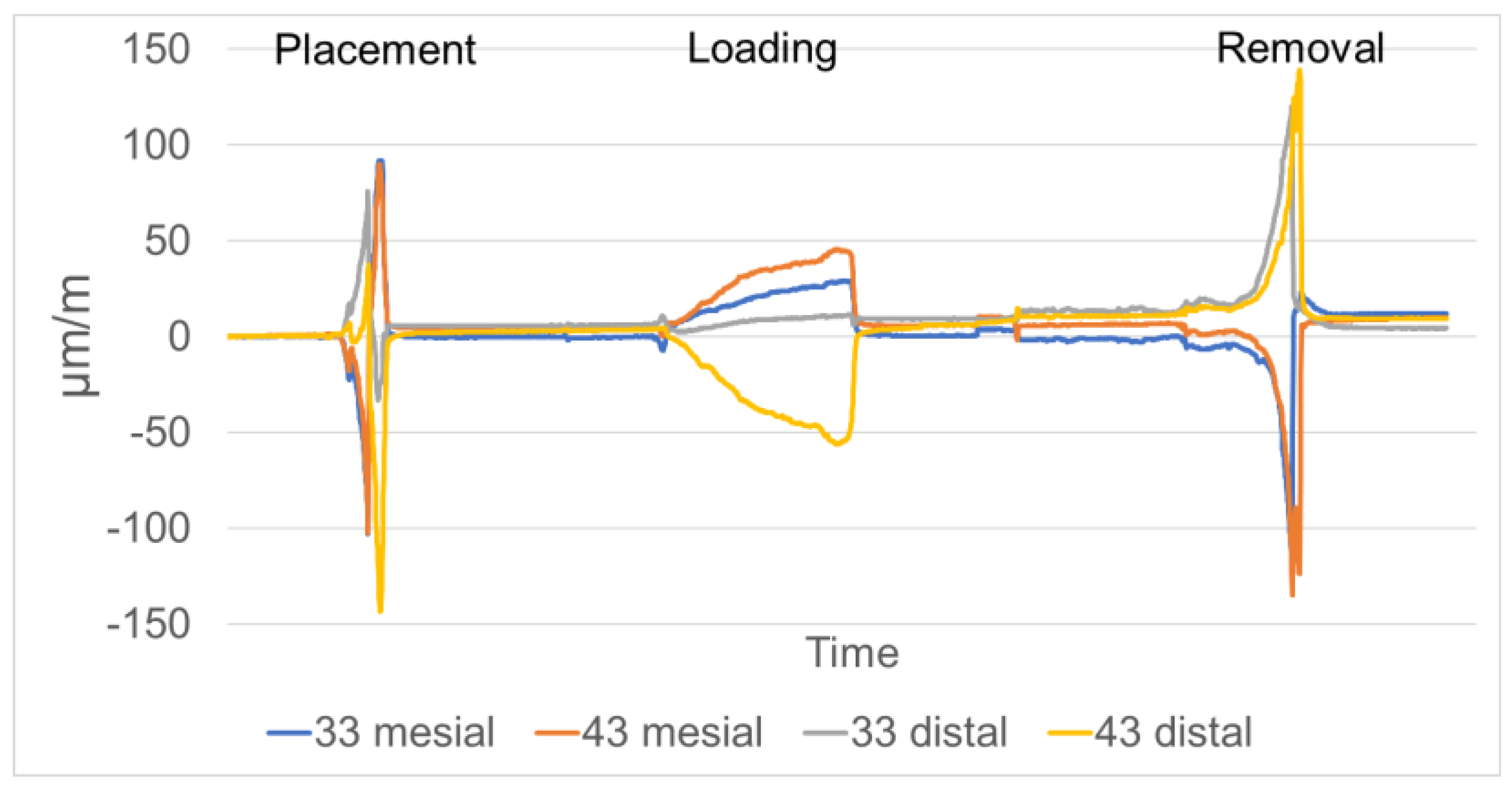
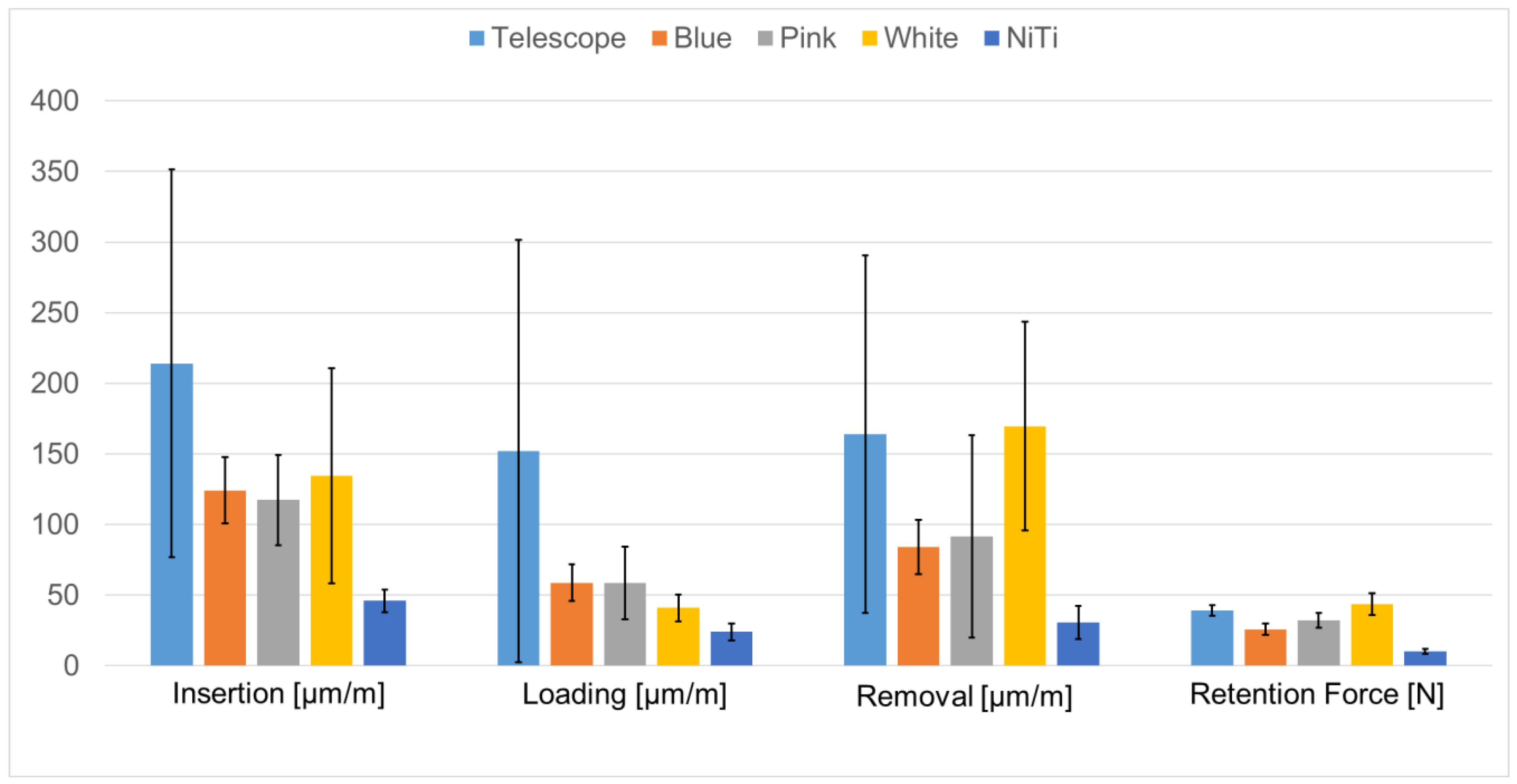
3.3. Testing of a Novel Attachment System
4. Discussion
5. Conclusions
- Locator-type attachments are problematic with respect to adjusting and maintaining retention;
- Individually fabricated telescopic crowns do not warrant the higher laboratory costs associated with them and are problematic in terms of adjusting retention as well as in transferring loads to the supporting implants;
- While yet at an early, preclinical stage, the flexible NiTi attachment tested may constitute an alternative solution with well-controlled retention and reduced wear at the male/female attachment interface;
- Apart from technical aspects, biologic complications associated with implant therapy continue to be problematic and should be monitored during the maintenance phase.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomason, J.M. The McGill Consensus Statement on Overdentures. Mandibular 2-implant overdentures as first choice standard of care for edentulous patients. Eur. J. Prosthodont. Restor. Dent. 2002, 10, 95–96. [Google Scholar]
- Possebon, A.P.D.R.; Schuster, A.J.; Miranda, S.B.; Marcello-Machado, R.M.; Chagas-Júnior, O.L.; Faot, F. Do implant-retained mandibular overdentures maintain radiographic, functional, and patient-centered outcomes after 3 years of loading? Clin. Oral Implants Res. 2020, 31, 936–945. [Google Scholar] [CrossRef]
- Keshk, A.M.; Alqutaibi, A.Y.; Algabri, R.S.; Swedan, M.S.; Kaddah, A. Prosthodontic maintenance and peri-implant tissue conditions for telescopic attachment-retained mandibular implant overdenture: Systematic review and meta-analysis of randomized clinical trials. Eur. J. Dent. 2017, 11, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Stoker, G.T.; Wismeijer, D.; van Waas, M.A. An eight-year follow-up to a randomized clinical trial of aftercare and cost-analysis with three types of mandibular implant-retained overdentures. J. Dent. Res. 2007, 86, 276–280. [Google Scholar] [CrossRef]
- Timmerman, R.; Stoker, G.T.; Wismeijer, D.; Oosterveld, P.; Vermeeren, J.I.; van Waas, M.A. An eight-year follow-up to a randomized clinical trial of participant satisfaction with three types of mandibular implant-retained overdentures. J. Dent. Res. 2004, 83, 630–633. [Google Scholar] [CrossRef] [PubMed]
- Kappel, S.; Klotz, A.L.; Eberhard, L.; Lorenzo Bermejo, J.; Rammelsberg, P.; Giannakopoulos, N.N. Maxillary implant overdentures on two or four implants. A prospective randomized cross-over clinical trial of implant and denture success and survival. Clin. Oral Implants Res. 2021, 32, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Rehmann, P.; Rudel, K.; Podhorsky, A.; Wöstmann, B. Three-Year Analysis of Fixed and Removable Telescopic Attachment-Retained Implant-Supported Dental Prostheses: Survival and Need for Maintenance. Int. J. Oral Maxillofac. Implants 2015, 30, 918–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodacre, B.J.; Goodacre, S.E.; Goodacre, C.J. Prosthetic complications with implant prostheses (2001–2017). Eur. J. Oral Implantol. 2018, 11 (Suppl. 1), S27–S36. [Google Scholar]
- Guédat, C.; Nagy, U.; Schimmel, M.; Müller, F.; Srinivasan, M. Clinical performance of LOCATOR® attachments: A retrospective study with 1-8 years of follow-up. Clin. Exp. Dent. Res. 2018, 4, 132–145. [Google Scholar] [CrossRef]
- Brunello, G.; Gervasi, M.; Ricci, S.; Tomasi, C.; Bressan, E. Patients’ perceptions of implant therapy and maintenance: A questionnaire-based survey. Clin. Oral Implans. Res. 2020, 31, 917–927. [Google Scholar] [CrossRef]
- Fromentin, O.; Lassauzay, C.; Nader, S.A.; Feine, J.; de Albuquerque, R.F., Jr. Wear of ball attachments after 1 to 8 years of clinical use: A qualitative analysis. Int. J. Prosthodont. 2011, 24, 270–272. [Google Scholar] [PubMed]
- Patodia, C.; Sutton, A.; Gozalo, D.; Font, K. Cost and complications associated with implant-supported overdentures with a resilient-attachment system: A retrospective study. J. Prosthet. Dent. 2022, 128, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Hahnel, S.; Alamanos, C.; Schneider-Feyrer, S.; Stöckle, M.; Rosentritt, M. Investigation of Clinical and Laboratory Wear in Locator-Supported, Implant-Retained Overdentures. Int. J. Prosthodont. 2018, 31, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Gonda, T.; Maeda, Y.; Walton, J.N.; MacEntee, M.I. Fracture incidence in mandibular overdentures retained by one or two implants. J. Prosthet. Dent. 2010, 103, 178–181. [Google Scholar] [CrossRef]
- Goodacre, C.J.; Bernal, G.; Rungcharassaeng, K.; Kan, J.Y. Clinical complications with implants and implant prostheses. J. Prosthet. Dent. 2003, 90, 121–132. [Google Scholar] [CrossRef]
- Brandt, S.; Brandt, J.; Ketabi, A.R.; Lauer, H.C.; Kunzmann, A. Locator® versus ceramic/electroplated double-crown attachments: A prospective study on the intraindividual comparison of implant-supported mandibular prostheses. Clin. Oral Investig. 2019, 23, 763–770. [Google Scholar] [CrossRef]
- Krennmair, G.; Weinländer, M.; Krainhöfner, M.; Piehslinger, E. Implant-supported mandibular overdentures retained with ball or telescopic crown attachments: A 3-year prospective study. Int. J. Prosthodont. 2006, 19, 164–170. [Google Scholar]
- Matthys, C.; De Vijlder, W.; Besseler, J.; Glibert, M.; De Bruyn, H. Cost-effectiveness analysis of two attachment systems for mandibular overdenture. Clin. Oral Implants Res. 2020, 31, 615–624. [Google Scholar] [CrossRef] [Green Version]
- Krennmair, G.; Sütö, D.; Seemann, R.; Piehslinger, E. Removable four implant-supported mandibular overdentures rigidly retained with telescopic crowns or milled bars: A 3-year prospective study. Clin. Oral Implants Res. 2012, 23, 481–488. [Google Scholar] [CrossRef]
- Lian, M.; Zhao, K.; Wang, F.; Huang, W.; Zhang, X.; Wu, Y. Stud vs Bar Attachments for Maxillary Four-Implant-Supported Overdentures: 3- to 9-year Results from a Retrospective Study. Int. J. Oral Maxillofac. Implants 2019, 34, 936–946. [Google Scholar] [CrossRef]
- Weigl, P.; Trimpou, G.; Lorenz, J.; Nentwig, G.H.; Lauer, H.C. Prefabricated taper crowns for the retention of implant superstructures: Three-year results of a prospective clinical trial. J. Prosthet. Dent. 2019, 121, 618–622. [Google Scholar] [CrossRef] [PubMed]
- Karl, M.; Winter, W.; Taylor, T.D.; Heckmann, S.M. In vitro study on passive fit in implant-supported 5-unit fixed partial dentures. Int. J. Oral Maxillofac. Implants 2004, 19, 30–37. [Google Scholar]
- ELsyad, M.A.; Abo Hatem, O.E.; Shawky, A.F.; Emera, R.M.K. Effect of Different Degrees of Mesial Implant Inclination on the Retention and Stability of Two-Implant Mandibular Overdentures Retained with Stud Attachments: An In Vitro Study. Int. J. Oral Maxillofac. Implants 2018, 33, 259–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passia, N.; Ghazal, M.; Kern, M. Long-term retention behaviour of resin matrix attachment systems for overdentures. J. Mech. Behav. Biomed. Mater. 2016, 57, 88–94. [Google Scholar] [CrossRef]
- Maniewicz, S.; Badoud, I.; Herrmann, F.R.; Chebib, N.; Ammann, P.; Schimmel, M.; Müller, F.; Srinivasan, M. In vitro retention force changes during cyclic dislodging of three novel attachment systems for implant overdentures with different implant angulations. Clin. Oral Implants Res. 2020, 31, 315–327. [Google Scholar] [CrossRef]
- Matthys, C.; Vervaeke, S.; Besseler, J.; De Bruyn, H. Five-year study of mandibular overdentures on stud abutments: Clinical outcome, patient satisfaction and prosthetic maintenance-Influence of bone resorption and implant position. Clin. Oral Implants Res. 2019, 30, 940–951. [Google Scholar] [CrossRef]
- Rosen, P.S.; Froum, S.J.; Sarmiento, H.; Wadhawani, C.P. A Revised Peri-implantitis Classification Scheme: Adding Three-Dimensional Considerations to Facilitate Prognosis and Treatment Planning. Int. J. Periodontics. Restor. Dent. 2022, 42, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Gallo, S.; Pascadopoli, M.; Pellegrini, M.; Pulicari, F.; Manfredini, M.; Zampetti, P.; Spadari, F.; Maiorana, C.; Scribante, A. Latest Findings of the Regenerative Materials Application in Periodontal and Peri-Implant Surgery: A Scoping Review. Bioengineering 2022, 9, 594. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Taccardi, D.; Scribante, A. Home Oral Care of Periodontal Patients Using Antimicrobial Gel with Postbiotics, Lactoferrin, and Aloe Barbadensis Leaf Juice Powder vs. Conventional Chlorhexidine Gel: A Split-Mouth Randomized Clinical Trial. Antibiotics 2022, 11, 118. [Google Scholar] [CrossRef]
- Grobecker-Karl, T.; Kafitz, L.; Karl, M. Effect of Implant Position and Attachment Type on the Biomechanical Behavior of Mandibular Single Implant Prostheses. Eur. J. Prosthodont. Restor. Dent. 2020, 28, 152–160. [Google Scholar]
- Besselink, P.A. Recent Developments on Shape Memory Applications. J. Phys. IV 1997, 7, 581–590. [Google Scholar] [CrossRef]
- Shayanfard, P.; Wendler, F.; Hempel, P.; Karl, M. Design and Numerical-Method-Aided Optimization of a Novel Attachment System for Implant-Retained Dental Prostheses Using NiTi Shape Memory Alloys. Appl. Sci. 2023, 13, 491. [Google Scholar] [CrossRef]
- Jia, Z.; Tu, J.; Wang, K.; Jiang, G.; Wang, W. Allergic Reaction following Implantation of a Nitinol Alloy Inferior Vena Cava Filter. J. Vasc. Interv. Radiol. 2015, 26, 1375–1377. [Google Scholar] [CrossRef] [PubMed]
- Morshedi, M.M.; Kinney, T.B. Nickel hypersensitivity in patients with inferior vena cava filters: Case report and literature and MAUDE database review. J. Vasc. Interv. Radiol. 2014, 25, 1187–1191. [Google Scholar] [CrossRef]
- Shah, K.C.; Linsley, C.S.; Wu, B.M. Evaluation of a shape memory implant abutment system: An up to 6-month pilot clinical study. J. Prosthet. Dent. 2020, 123, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.C.; Chao, D.; Wu, B.M.; Jensen, O.T. Shape-memory Retained Complete Arch Guided Implant Treatment Using Nitinol (Smileloc) Abutments. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 427–435. [Google Scholar] [CrossRef]
- Shah, K.C.; Seo, Y.R.; Wu, B.M. Clinical application of a shape memory implant abutment system. J. Prosthet. Dent. 2017, 117, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.G.; Cho, W.T.; Lim, H.K.; Hwang, S.H.; Bae, J.H.; Bae, G.H.; Lee, J.Y.; Huh, J.B. Influence of an Implant Fixture including a Freely Removable Micro-Locking Implant Prosthesis on Peri-Implant Tissues and Implant Prostheses: A Prospective Clinical Study. J. Clin. Med. 2021, 10, 3321. [Google Scholar] [CrossRef]
- Jensen, O.T.; Jansen, C.E.; Seo, Y.; Yellich, G. Guided Nitinol-Retained (Smileloc) Single-Tooth Dental Restorations. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 437–446. [Google Scholar] [CrossRef]
- Pautke, C.; Kolk, A.; Brokate, M.; Wehrstedt, J.C.; Kneissl, F.; Miethke, T.; Steinhauser, E.; Horch, H.H.; Deppe, H. Development of novel implant abutments using the shape memory alloy nitinol: Preliminary results. Int. J. Oral Maxillofac. Implants 2009, 24, 477–483. [Google Scholar]
- Bouhy, A.; Rompen, E.; Lamy, M.; Legros, C.; Lecloux, G.; Lambert, F. Maxillary implant overdenture retained by four unsplinted attachments and opposed by a natural or fixed dentition: One-year clinical outcomes. Clin. Oral Implants. Res. 2020, 31, 747–767. [Google Scholar] [CrossRef] [PubMed]
- Karl, M.; Taylor, T.D. Bone Adaptation Induced by Non-Passively Fitting Implant Superstructures: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implants 2016, 31, 369–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elkerdawy, M.W.; Radi, I.A. Effect of dislodging forces on mandibular implant attachment-retained overdenture. Implant Dent. 2011, 20, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Heckmann, S.M.; Winter, W.; Meyer, M.; Weber, H.P.; Wichmann, M.G. Overdenture attachment selection and the loading of implant and denture-bearing area. Part 2: A methodical study using five types of attachment. Clin. Oral Implants Res. 2001, 12, 640–647. [Google Scholar] [CrossRef]
- Weng, D.; Richter, E.J. Maxillary removable prostheses retained by telescopic crowns on two implants or two canines. Int. J. Periodontics. Restor. Dent. 2007, 27, 35–41. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Telescope | Locator | Bar | ||
|---|---|---|---|---|
| Number of jaws | 24 | 29 | 25 | |
| Number of implants | 109 | 100 | 104 | |
| Mean number of implants per jaw | 4.5 (±0.9) | 3.4 (±1.3) | 4.2 (±0.5) | |
| Implants lost during observation period | T < 90 d | 1 | 1 | 0 |
| 90 d < T < 365 d | 0 | 0 | 0 | |
| 365 d < T < 730 d | 0 | 1 | 0 | |
| T > 730 d | 4 | 1 | 1 | |
| Attachment associated complications | Total number | 34 | 56 | 9 |
| T < 90 d | 9 | 16 | 2 | |
| 90 d < T < 365 d | 4 | 7 | 2 | |
| 365 d < T < 730 d | 5 | 8 | 0 | |
| T > 730 d | 16 | 25 | 5 | |
| most frequent | Decementation of primary telescopic crown | Replacement of insert | Replacement of clips | |
| second most frequent | Adjustment of friction⑩(Reduction) | Loosening/Loss of Locator abutment | Activation of clips/Screw loosening | |
| Remark | 16 complications occurred in one specific prosthesis | 10 complications occurred in one specific prosthesis | No cumulation of complications in a specific prosthesis | |
| Telescope | Locator | Bar | ||||
|---|---|---|---|---|---|---|
| Overall Satisfaction | ||||||
| p-value | corrected p-value | p-value | corrected p-value | p-value | corrected p-value | |
| Telescope | - | - | 0.880 | 0.880 | 0.052 | 0.156 |
| Locator | 0.175 | 0.349 | - | - | 0.070 | 0.156 |
| Bar | 0.462 | 0.462 | 0.022 * | 0.065 | - | - |
| Retention | ||||||
| (a) Prosthesis Placement | |||||
| Telescope | Locator Blue | Locator Pink | Locator White | NiTi | |
| Telescope | - | 0.989 | 0.937 | 0.900 | 0.027 * |
| Locator Blue | - | 0.998 | 0.994 | 0.109 | |
| Locator Pink | - | 1.000 | 0.215 | ||
| Locator White | - | 0.269 | |||
| NiTi | - | ||||
| (b) Loading | |||||
| Telescope | Locator Blue | Locator Pink | Locator White | NiTi | |
| Telescope | - | 0.009 * | 0.999 | 0.777 | 0.074 |
| Locator Blue | - | 0.989 | 0.640 | 0.039 * | |
| Locator Pink | - | 0.900 | 0.143 | ||
| Locator White | - | 0.640 | |||
| NiTi | - | ||||
| (c) Prosthesis Removal | |||||
| Telescope | Locator Blue | Locator Pink | Locator White | NiTi | |
| Telescope | - | 0.925 | 0.854 | 0.989 | 0.109 |
| Locator Blue | - | 1.000 | 0.688 | 0.516 | |
| Locator Pink | - | 0.566 | 0.640 | ||
| Locator White | - | 0.027 * | |||
| NiTi | - | ||||
| (d) Retention force | |||||
| Telescope | Locator Blue | Locator Pink | Locator White | NiTi | |
| Telescope | - | 0.318 | 0.836 | 0.991 | 0.021 * |
| Locator Blue | - | 0.919 | 0.119 | 0.827 | |
| Locator Pink | - | 0.553 | 0.308 | ||
| Locator White | - | 0.004 * | |||
| NiTi | - | ||||
| Locator Blue | Locator Pink | Locator White | |
|---|---|---|---|
| Manufacturer information | 0.7 kg | 1.4 kg | 2.3.kg |
| Expected for 2 attachments | 13.73 N | 27.46 N | 45.12 N |
| Recorded (Figure 7) | 25.92 N | 32.12 N | 43.72 N |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wendler, F.; Diehl, L.; Shayanfard, P.; Karl, M. Implant-Supported Overdentures: Current Status and Preclinical Testing of a Novel Attachment System. J. Clin. Med. 2023, 12, 1012. https://doi.org/10.3390/jcm12031012
Wendler F, Diehl L, Shayanfard P, Karl M. Implant-Supported Overdentures: Current Status and Preclinical Testing of a Novel Attachment System. Journal of Clinical Medicine. 2023; 12(3):1012. https://doi.org/10.3390/jcm12031012
Chicago/Turabian StyleWendler, Frank, Lisa Diehl, Pejman Shayanfard, and Matthias Karl. 2023. "Implant-Supported Overdentures: Current Status and Preclinical Testing of a Novel Attachment System" Journal of Clinical Medicine 12, no. 3: 1012. https://doi.org/10.3390/jcm12031012