
Adiponectin, Leptin and Resistin in Patients with Psoriasis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Assessment of Adiponectin, Leptin, and Resistin Concentrations in the Plasma of Patients with Psoriasis and Control Subjects
2.3. Statistical Analysis
3. Results
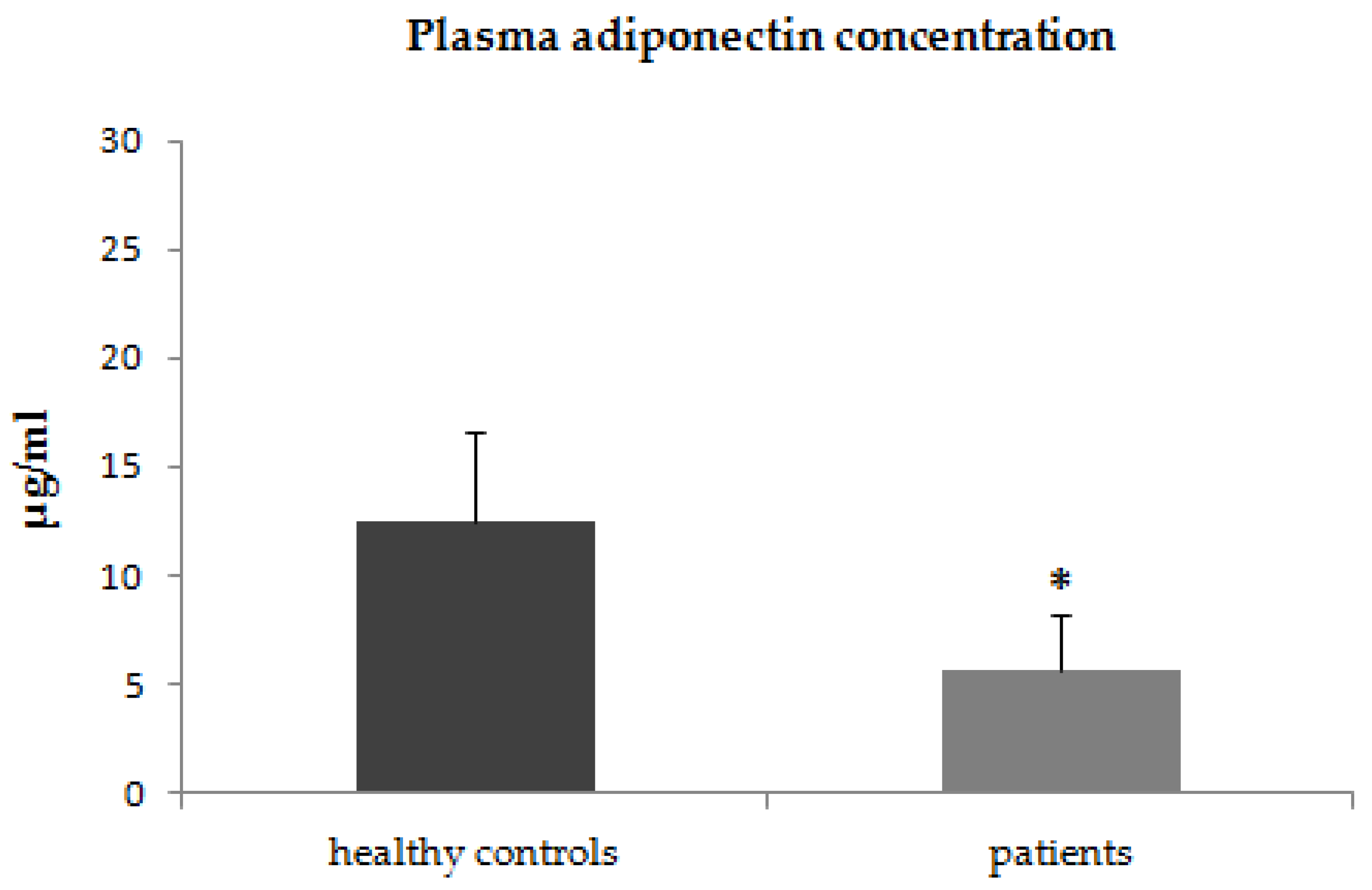
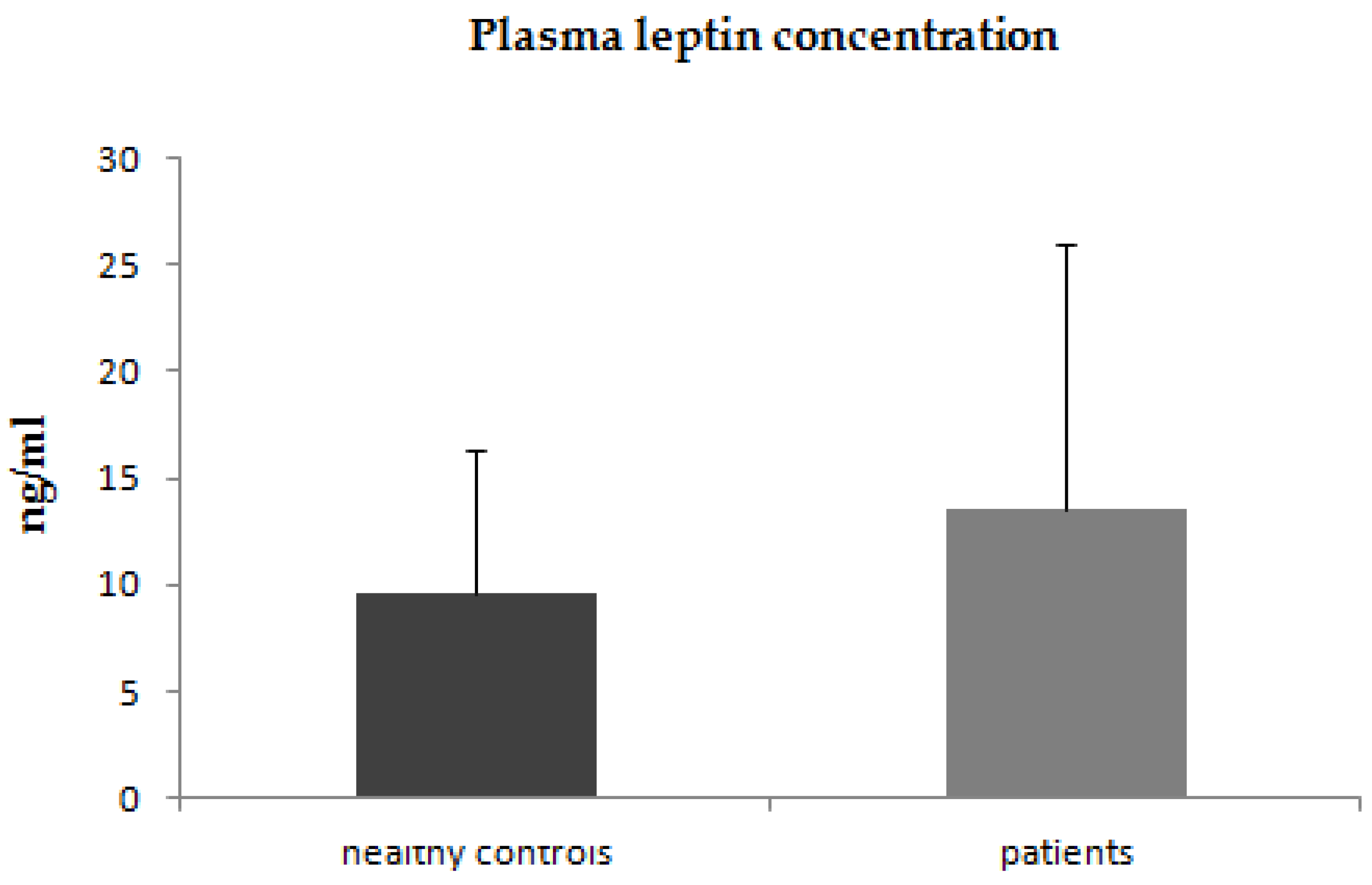
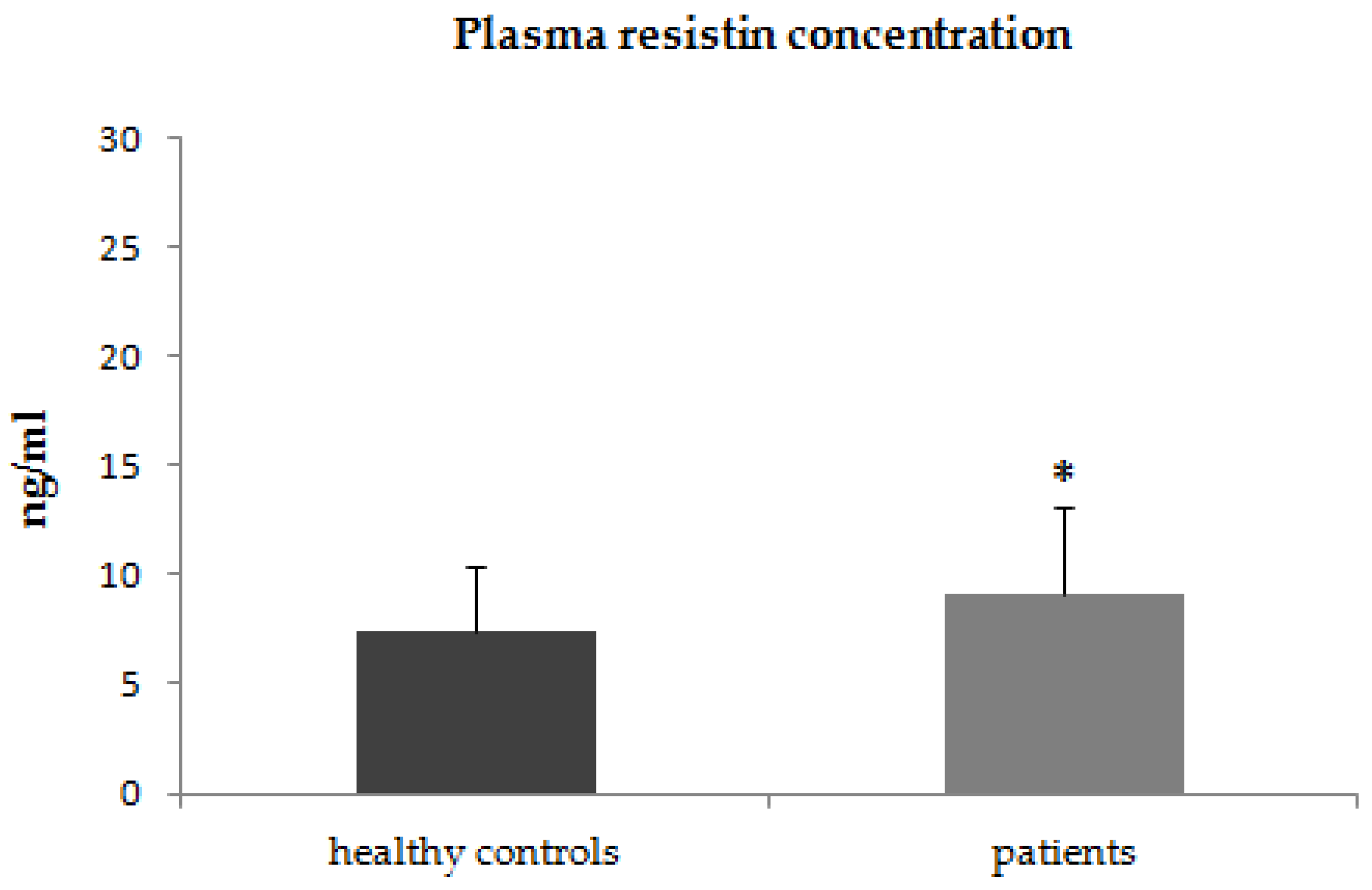
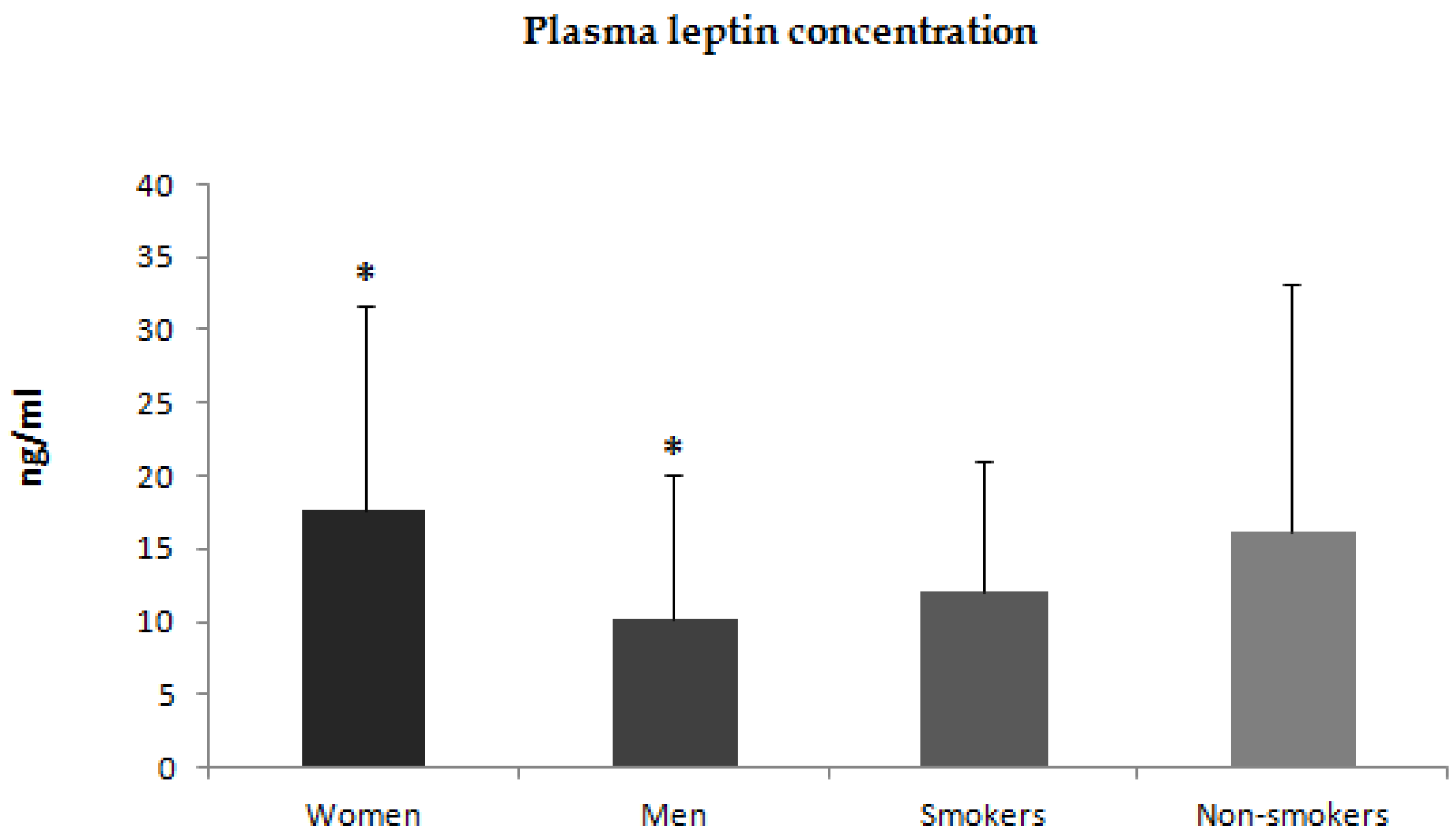
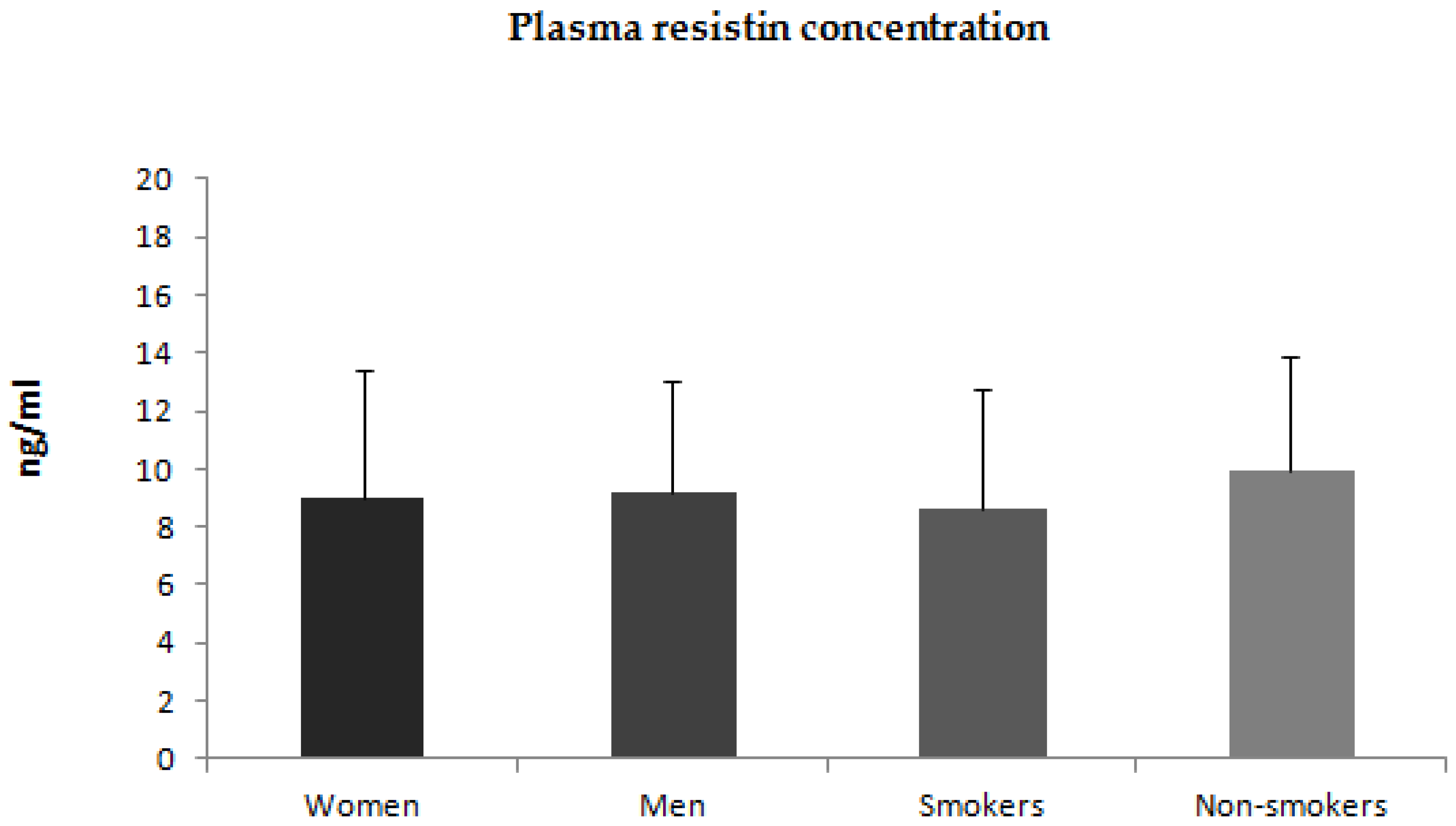
3.1. Assessment of Adiponectin, Leptin and Resistin Plasma Concentrations in Patients with Psoriasis and Control Subjects
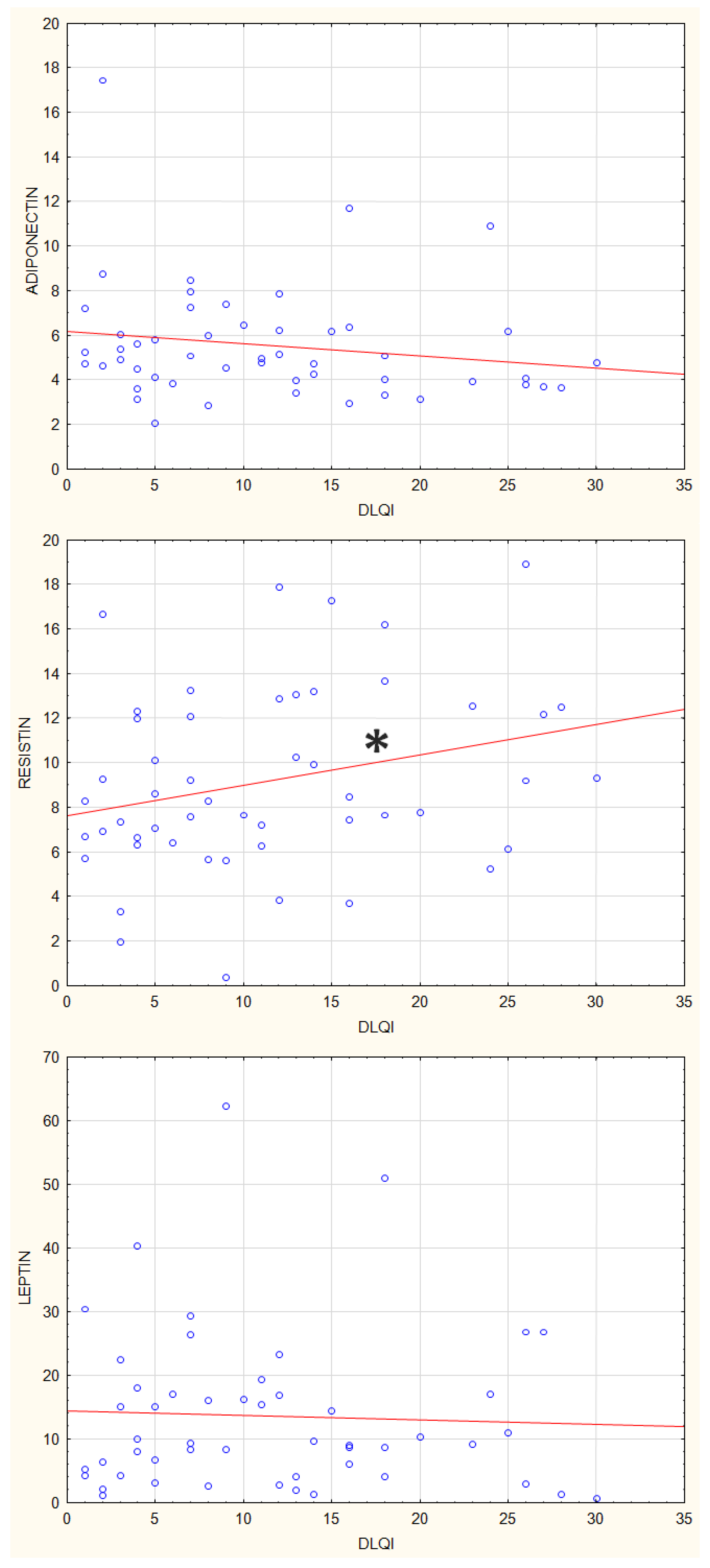
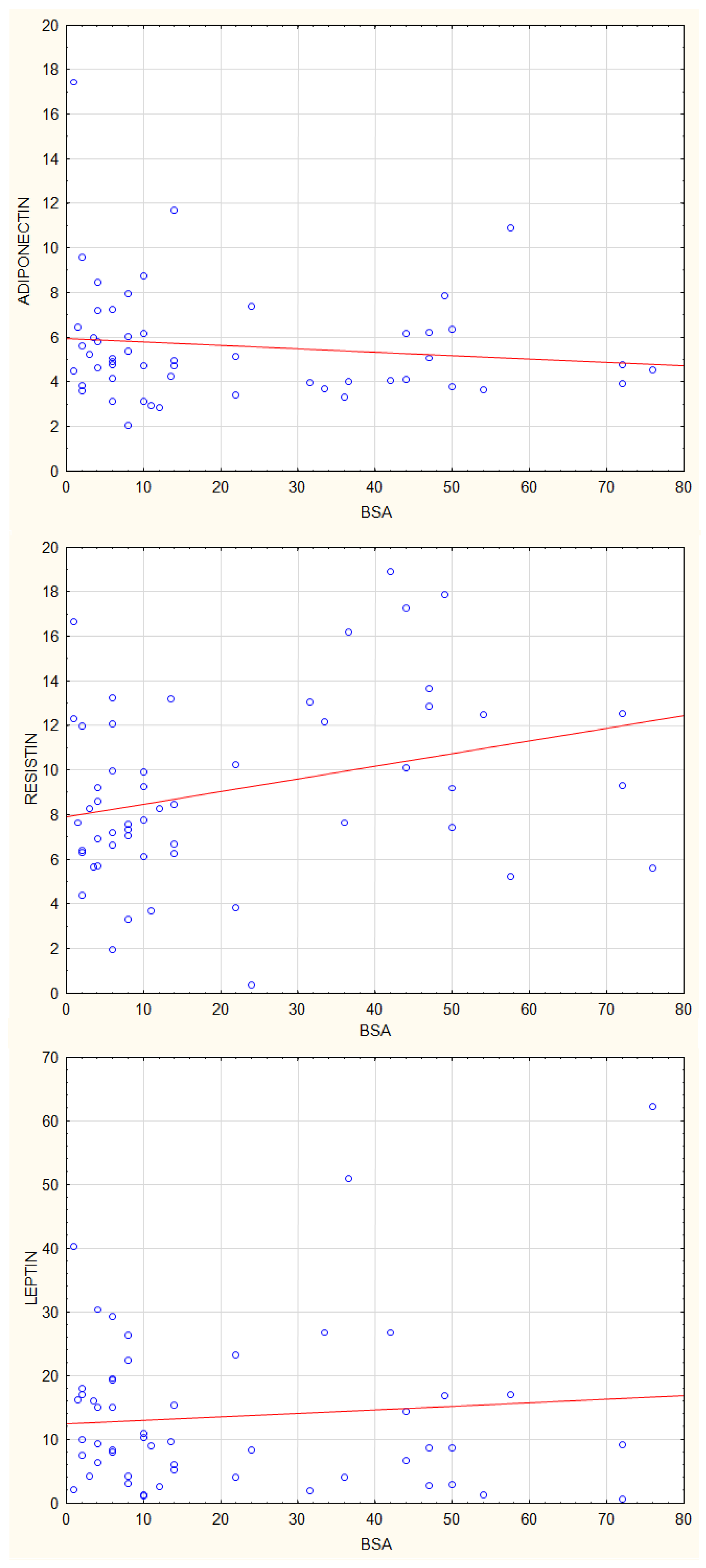
3.2. Correlations between Plasma Concentrations of Adiponectin, Leptin and Resistin and Disease Activity Parameters in Patients with Psoriasis
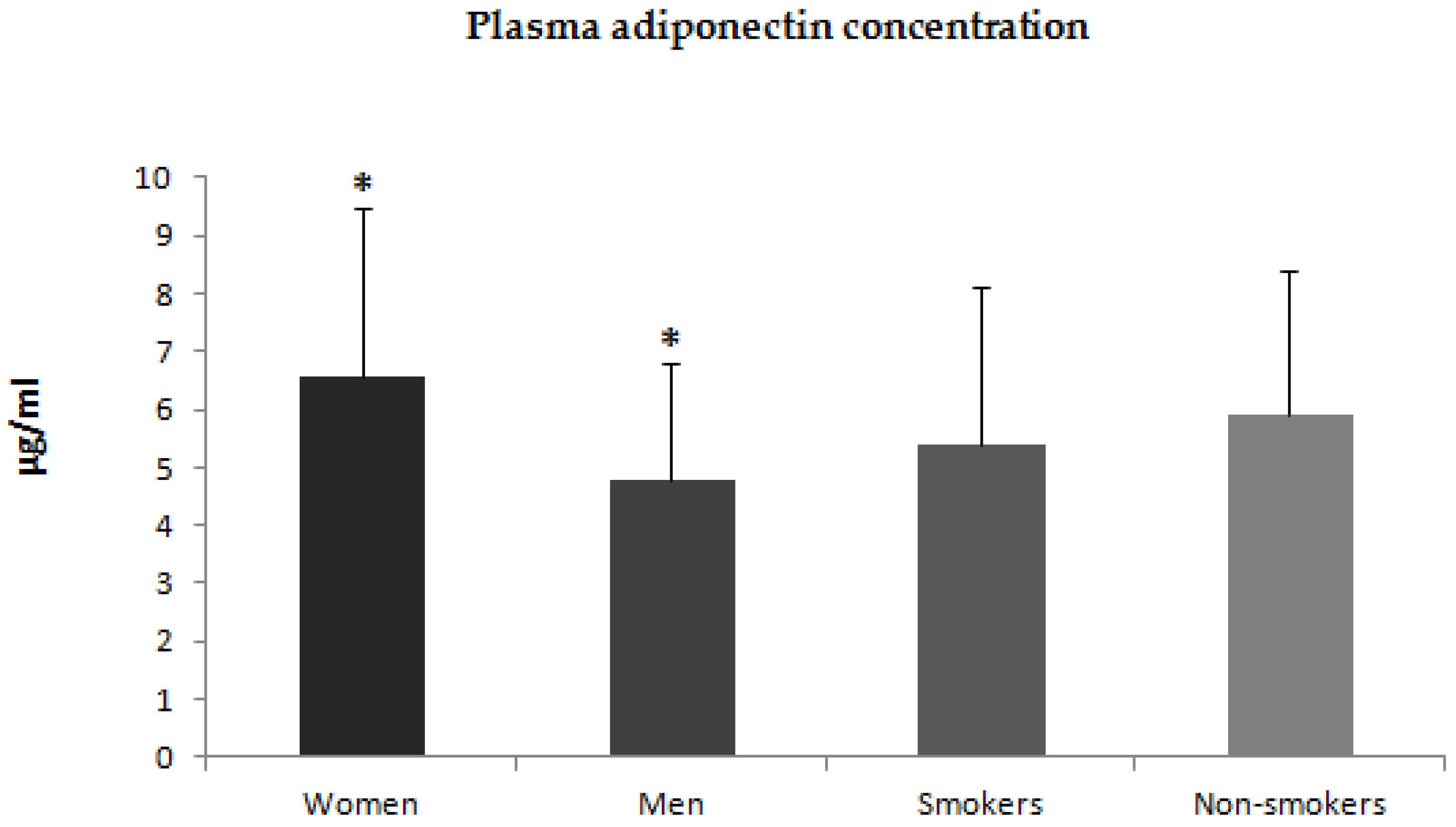
3.3. Correlations between Plasma Concentrations of Adiponectin, Leptin, and Resistin and Clinical Parameters in Patients with Psoriasis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Di Meglio, P.; Villanova, F.; Nestle, F.O. Psoriasis. Cold Spring Harb. Perspect. Med. 2014, 4, a015354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M. Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project team. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, C.E.; Barker, J.N. Pathogenesis and clinical features of psoriasis. Lancet 2007, 370, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Alexis, A.F.; Blackcloud, P. Psoriasis in skin of color: Epidemiology, genetics, clinical presentation, and treatment nuances. J. Clin. Aesthet. Dermatol. 2014, 7, 16–24. [Google Scholar]
- Tokura, Y.; Phadungsaksawasdi, P.; Kurihara, K.; Fujiyama, T.; Honda, T. Pathophysiology of Skin Resident Memory T Cells. Front. Immunol. 2021, 11, 618897. [Google Scholar] [CrossRef]
- Boehncke, W.H.; Brembilla, N.C. Autoreactive T-Lymphocytes in Inflammatory Skin Diseases. Front. Immunol. 2019, 10, 1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, P.; Wang, M.; Gao, H.; Zheng, A.; Li, J.; Mu, D.; Tong, J. The Role of Helper T Cells in Psoriasis. Front. Immunol. 2021, 12, 788940. [Google Scholar] [CrossRef] [PubMed]
- Kelsen, J.; Dige, A.; Christensen, M.; D’Amore, F.; Iversen, L. Frequency and clonality of peripheral γδ T cells in psoriasis patients receiving anti-tumour necrosis factor-α therapy. Clin. Exp. Immunol. 2014, 177, 142–148. [Google Scholar] [CrossRef]
- Fantuzzi, G. Adipose tissue, adipokines, and inflammation. J. Allergy Clin. Immunol. 2005, 115, 911–919. [Google Scholar] [CrossRef]
- Perera, G.K.; Di Meglio, P.; Nestle, F.O. Psoriasis. Annu. Rev. Pathol. 2012, 7, 385–422. [Google Scholar] [CrossRef]
- Lynch, M.; Ahern, T.; Sweeney, C.M.; Malara, A.; Tobin, A.M.; O’Shea, D.; Kirby, B. Adipokines, psoriasis, systemic inflammation, and endothelial dysfunction. Int. J. Dermatol. 2017, 56, 1103–1118. [Google Scholar] [CrossRef] [PubMed]
- Gerdes, S.; Rostami-Yazdi, M.; Mrowietz, U. Adipokines and psoriasis. Exp. Dermatol. 2011, 20, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Seminara, N.; Abuabara, K.; Shin, D.; Langan, S.; Kimmel, S.; Margolis, D.; Troxel, A.; Gelfand, J. Validity of The Health Improvement Network (THIN) for the study of psoriasis. Br. J. Dermatol. 2011, 164, 602–609. [Google Scholar] [CrossRef] [Green Version]
- Słuczanowska-Głabowska, S.; Jaworska, W.; Staniszewska, M.; Tkacz, M.; Safranow, K.; Łuczkowska, K.; Zagrodnik, E.; Stecewicz, I.; Machaliński, B.; Pawlik, A. Plasma Levels of Interleukins 36α, 36β, and 37 in Patients with Psoriasis and Their Correlation with Disease Activity Parameters. J. Clin. Med. 2022, 11, 5254. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Zhu, Y.J.; Zou, S.; Zhou, P.; Hu, Y.W.; Zhao, Q.X.; Gu, L.N.; Zhang, H.Z.; Wang, Z.; Li, J. Metabolic Syndrome and Psoriasis: Mechanisms and Future Directions. Front. Immunol. 2021, 12, 711060. [Google Scholar] [CrossRef] [PubMed]
- Farkhondeh, T.; Llorens, S.; Pourbagher-Shahri, A.M.; Ashrafizadeh, M.; Talebi, M.; Shakibaei, M.; Samarghandian, S. An Overview of the Role of Adipokines in Cardiometabolic Diseases. Molecules 2020, 25, 5218. [Google Scholar] [CrossRef]
- Johnston, A.; Arnadottir, S.; Gudjonsson, J.E.; Aphale, A.; Sigmarsdottir, A.A.; Gunnarsson, S.I.; Steinsson, J.T.; Elder, J.T.; Valdimarsson, H. Obesity in psoriasis: Leptin and resistin as mediators of cutaneous inflammation. Br. J. Dermatol. 2008, 159, 342–350. [Google Scholar] [CrossRef] [Green Version]
- Su, X.; Zhang, G.; Cheng, Y.; Wang, B. Leptin in skin disease modulation. Clin. Chim. Acta 2021, 516, 8–14. [Google Scholar] [CrossRef]
- Su, X.; Cheng, Y.; Chang, D. The Important Role of Leptin in Modulating the Risk of Dermatological Diseases. Front. Immunol. 2021, 11, 593564. [Google Scholar] [CrossRef]
- Bahceci, M.; Gokalp, D.; Bahceci, S.; Tuzcu, A.; Atmaca, S.; Arikan, S. The correlation between adiposity and adiponectin, tumor necrosis factor alpha, interleukin-6 and high sensitivity C-reactive protein levels. Is adipocyte size associated with inflammation in adults? J. Endocrinol. Investig. 2007, 30, 210–214. [Google Scholar] [CrossRef]
- He, Y.; Lu, L.; Wei, X.; Jin, D.; Qian, T.; Yu, A.; Sun, J.; Cui, J.; Yang, Z. The multimerization and secretion of adiponectin are regulated by TNF-alpha. Endocrine 2016, 51, 456–468. [Google Scholar] [CrossRef] [PubMed]
- Hulthe, J.; Hultén, L.M.; Fagerberg, B. Low adipocyte-derived plasma protein adiponectin concentrations are associated with the metabolic syndrome and small dense low-density lipoprotein particles: Atherosclerosis and insulin resistance study. Metabolism 2003, 52, 1612–1614. [Google Scholar] [CrossRef] [PubMed]
- Spranger, J.; Kroke, A.; Möhlig, M.; Bergmann, M.M.; Ristow, M.; Boeing, H.; Pfeiffer, A.F. Adiponectin and protection against type 2 diabetes mellitus. Lancet 2003, 361, 226–228, Erratum in Lancet 2002, 361, 1060. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Wu, C.Y.; Shen, J.L.; Chu, S.Y.; Chen, C.K.; Chang, Y.T.; Chen, C.M. Psoriasis independently associated with hyperleptinemia contributing to metabolic syndrome. Arch. Dermatol. 2008, 144, 1571–1575. [Google Scholar] [CrossRef] [Green Version]
- Wolk, K.; Sabat, R. Adipokines in psoriasis: An important link between skin inflammation and metabolic alterations. Rev. Endocr. Metab. Disord. 2016, 17, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, S.; Catarino, C.; Santos-Silva, A. The triad psoriasis-obesity-adipokine profile. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1876–1885. [Google Scholar] [CrossRef]
- Versini, M.; Jeandel, P.Y.; Rosenthal, E.; Shoenfeld, Y. Obesity in autoimmune diseases: Not a passive bystander. Autoimmun. Rev. 2014, 13, 981–1000. [Google Scholar] [CrossRef]
- Sterry, W.; Strober, B.E.; Menter, A.; International Psoriasis Council. Obesity in psoriasis: The metabolic, clinical and therapeutic implications. Report of an interdisciplinary conference and review. Br. J. Dermatol. 2007, 157, 649–655. [Google Scholar] [CrossRef]
- Wong, Y.; Nakamizo, S.; Tan, K.J.; Kabashima, K. An Update on the Role of Adipose Tissues in Psoriasis. Front. Immunol. 2019, 10, 1507. [Google Scholar] [CrossRef]
- Bai, F.; Zheng, W.; Dong, Y.; Wang, J.; Garstka, M.A.; Li, R.; An, J.; Ma, H. Serum levels of adipokines and cytokines in psoriasis patients: A systematic review and meta-analysis. Oncotarget 2017, 9, 1266–1278. [Google Scholar] [CrossRef] [Green Version]
- Gerdes, S.; Osadtschy, S.; Rostami-Yazdi, M.; Buhles, N.; Weichenthal, M.; Mrowietz, U. Leptin, adiponectin, visfatin and retinol-binding protein-4-mediators of comorbidities in patients with psoriasis? Exp. Dermatol. 2012, 21, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Shibata, S.; Saeki, H.; Tada, Y.; Karakawa, M.; Komine, M.; Tamaki, K. Serum high molecular weight adiponectin levels are decreased in psoriasis patients. J. Dermatol. Sci. 2009, 55, 62–63. [Google Scholar] [CrossRef] [PubMed]
- Ouchi, N.; Kihara, S.; Funahashi, T.; Nakamura, T.; Nishida, M.; Kumada, M.; Okamoto, Y.; Ohashi, K.; Nagaretani, H.; Kishida, K.; et al. Reciprocal association of C-reactive protein with adiponectin in blood stream and adipose tissue. Circulation 2003, 107, 671–674. [Google Scholar] [CrossRef] [Green Version]
- Fantuzzi, G. Adiponectin and inflammation: Consensus and controversy. J. Allergy Clin. Immunol. 2008, 121, 326–330. [Google Scholar] [CrossRef]
- Baran, A.; Flisiak, I.; Jaroszewicz, J.; Świderska, M. Effect of psoriasis activity on serum adiponectin and leptin levels. Postepy. Dermatol. Alergol. 2015, 32, 101–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghoshal, K.; Chatterjee, T.; Chowdhury, S.; Sengupta, S.; Bhattacharyya, M. Adiponectin Genetic Variant and Expression Coupled with Lipid Peroxidation Reveal New Signatures in Diabetic Dyslipidemia. Biochem. Genet. 2021, 59, 781–798. [Google Scholar] [CrossRef] [PubMed]
- Łączna, M.; Kopytko, P.; Tkacz, M.; Zgutka, K.; Czerewaty, M.; Tarnowski, M.; Larysz, D.; Tkacz, R.; Kotrych, D.; Piotrowska, K.; et al. Adiponectin Is a Component of the Inflammatory Cascade in Rheumatoid Arthritis. J. Clin. Med. 2022, 11, 2740. [Google Scholar] [CrossRef]
- Campanati, A.; Orciani, M.; Consales, V.; Lazzarini, R.; Ganzetti, G.; Di Benedetto, G.; Di Primio, R.; Offidani, A. Characterization and profiling of immunomodulatory genes in resident mesenchymal stem cells reflect the Th1-Th17/Th2 imbalance of psoriasis. Arch. Dermatol. Res. 2014, 306, 915–920. [Google Scholar] [CrossRef]
- Surendar, J.; Frohberger, S.J.; Karunakaran, I.; Schmitt, V.; Stamminger, W.; Neumann, A.L.; Wilhelm, C.; Hoerauf, A.; Hübner, M.P. Adiponectin Limits IFN-γ and IL-17 Producing CD4 T Cells in Obesity by Restraining Cell Intrinsic Glycolysis. Front. Immunol. 2019, 10, 2555. [Google Scholar] [CrossRef] [Green Version]
- Shibata, S.; Tada, Y.; Hau, C.S.; Mitsui, A.; Kamata, M.; Asano, Y.; Sugaya, M.; Kadono, T.; Masamoto, Y.; Kurokawa, M.; et al. Adiponectin regulates psoriasiform skin inflammation by suppressing IL-17 production from γδ-T cells. Nat. Commun. 2015, 6, 7687. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, H.; Tsuji, H.; Takahashi, I.; Hashimoto, Y.; Ishida-Yamamoto, A.; Iizuka, H. Plasma adiponectin and leptin levels in Japanese patients with psoriasis. Br. J. Dermatol. 2008, 159, 1207–1208. [Google Scholar] [CrossRef] [PubMed]
- Eder, L.; Jayakar, J.; Pollock, R.; Pellett, F.; Thavaneswaran, A.; Chandran, V.; Rosen, C.F.; Gladman, D.D. Serum adipokines in patients with psoriatic arthritis and psoriasis alone and their correlation with disease activity. Ann. Rheum. Dis. 2013, 72, 1956–1961. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Han, Y.; Jose, P.A.; Zeng, C. Loss of Adiponectin-Induced Renal Sodium Excretion in Hypertension. J. Am. Soc. Hypertens. 2016, 10 (Suppl. S1), e4. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, S.; Huang, H.; Zeng, A.; Han, Y.; Zeng, C.; Zheng, S.; Ren, H.; Wang, Y.; Huang, Y.; et al. GRK4-mediated adiponectin receptor-1 phosphorylative desensitization as a novel mechanism of reduced renal sodium excretion in hypertension. Clin. Sci. Lond. 2020, 134, 2453–2467. [Google Scholar] [CrossRef] [PubMed]
- Cerman, A.A.; Bozkurt, S.; Sav, A.; Tulunay, A.; Elbaşi, M.O.; Ergun, T. Serum leptin levels, skin leptin and leptin receptor expression in psoriasis. Br. J. Dermatol. 2008, 159, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, J.; Zhao, Y.; Geng, L.; Song, F.; Chen, H.D. Psoriasis is associated with increased levels of serum leptin. Br. J. Dermatol. 2008, 158, 1134–1135. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, S.; Oliveira, H.; Reis, F.; Belo, L.; Rocha, S.; Quintanilha, A.; Figueiredo, A.; Teixeira, F.; Castro, E.; Rocha-Pereira, P.; et al. Circulating adipokine levels in Portuguese patients with psoriasis vulgaris according to body mass index, severity and therapy. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 1386–1394. [Google Scholar] [CrossRef]
- Kyriakou, A.; Patsatsi, A.; Sotiriadis, D.; Goulis, D.G. Serum Leptin, Resistin, and Adiponectin Concentrations in Psoriasis: A Meta-Analysis of Observational Studies. Dermatology 2017, 233, 378–389. [Google Scholar] [CrossRef]
- Mitsuyama, S.; Abe, F.; Kimura, M.; Yoshida, M.; Higuchi, T. Association between leptin gene expression in subcutaneous adipose tissue and circulating leptin levels in obese patients with psoriasis. Arch. Dermatol. Res. 2015, 307, 539–544. [Google Scholar] [CrossRef]
- El-Boghdady, N.A.; Ismail, M.F.; Abd-Alhameed, M.F.; Ahmed, A.S.; Ahmed, H.H. Bidirectional Association Between Psoriasis and Obesity: Benefits and Risks. J. Interferon. Cytokine. Res. 2018, 38, 12–19. [Google Scholar] [CrossRef]
- Nakajima, H.; Nakajima, K.; Tarutani, M.; Sano, S. Clear association between serum levels of adipokines and T-helper 17-related cytokines in patients with psoriasis. Clin. Exp. Dermatol. 2013, 38, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Xue, K.; Liu, H.; Jian, Q.; Liu, B.; Zhu, D.; Zhang, M.; Gao, L.; Li, C. Leptin induces secretion of pro-inflammatory cytokines by human keratinocytes in vitro--a possible reason for increased severity of psoriasis in patients with a high body mass index. Exp. Dermatol. 2013, 22, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.J.; Zhang, C.; Li, M.; Zhu, C.Y.; Shi, G.; Fan, Y.M. Leptin levels in patients with psoriasis: A meta-analysis. Clin. Exp. Dermatol. 2013, 38, 478–483. [Google Scholar] [CrossRef]
- Tripathi, D.; Kant, S.; Pandey, S.; Ehtesham, N.Z. Resistin in metabolism, inflammation, and disease. FEBS J. 2020, 287, 3141–3149. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Yang, X.Q.; Cheng, J.; Hui, R.S.; Gao, T.W. Increased Th17 cells are accompanied by FoxP3(+) Treg cell accumulation and correlated with psoriasis disease severity. Clin. Immunol. 2010, 135, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Seth, D.; Ehlert, A.N.; Golden, J.B.; Damiani, G.; McCormick, T.S.; Cameron, M.J.; Cooper, K.D. Interaction of Resistin and Systolic Blood Pressure in Psoriasis Severity. J. Invest. Dermatol. 2020, 140, 1279–1282. [Google Scholar] [CrossRef]
- Huang, H.; Shen, E.; Tang, S.; Tan, X.; Guo, X.; Wang, Q.; Ding, H. Increased serum resistin levels correlate with psoriasis: A meta-analysis. Lipids Health Dis. 2015, 14, 44. [Google Scholar] [CrossRef] [Green Version]
- Pona, A.; Haidari, W.; Kolli, S.S.; Feldman, S.R. Diet and psoriasis. Dermatol. Online J. 2019, 25, 13030/qt1p37435s. [Google Scholar] [CrossRef]
- Wu, A.G.; Weinberg, J.M. The impact of diet on psoriasis. Cutis 2019, 104, 7–10, Erratum in Cutis 2019, 104, 241. [Google Scholar]
- Garbicz, J.; Całyniuk, B.; Górski, M.; Buczkowska, M.; Piecuch, M.; Kulik, A.; Rozentryt, P. Nutritional Therapy in Persons Suffering from Psoriasis. Nutrients 2021, 14, 119. [Google Scholar] [CrossRef]
- Herbert, D.; Franz, S.; Popkova, Y.; Anderegg, U.; Schiller, J.; Schwede, K.; Lorz, A.; Simon, J.C.; Saalbach, A. High-Fat Diet Exacerbates Early Psoriatic Skin Inflammation Independent of Obesity: Saturated Fatty Acids as Key Players. J. Investig. Dermatol. 2018, 138, 1999–2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeda, K.; Morizane, S.; Akagi, T.; Hiramatsu-Asano, S.; Tachibana, K.; Yahagi, A.; Iseki, M.; Kaneto, H.; Wada, J.; Ishihara, K.; et al. Obesity and Dyslipidemia Synergistically Exacerbate Psoriatic Skin Inflammation. Int. J. Mol. Sci. 2022, 23, 4312. [Google Scholar] [CrossRef] [PubMed]
- Salehi-Abargouei, A.; Izadi, V.; Azadbakht, L. The effect of low calorie diet on adiponectin concentration: A systematic review and meta-analysis. Horm. Metab. Res. 2015, 47, 549–555. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Patients with Psoriasis n-53 | Control Group n-31 |
|---|---|---|
| Male | 29 | 17 |
| Female | 24 | 14 |
| Age [years] | 49.7 ± 17.6 | 48.5 ± 14.2 |
| Age of disease onset [years] | 34.03 ± 20.08 | - |
| Smoking | 19 | 12 |
| DLQI | 11.47 ± 8.19 | - |
| PASI | 11.28 ± 10.87 | - |
| BSA | 21.33 ± 21.18 | - |
| Adiponectin | Leptin | Resistin | ||||
|---|---|---|---|---|---|---|
| Parameter | Rs | p | Rs | p | Rs | p |
| Age | 0.28 | 0.03 | 0.02 | 0.83 | 0.2 | 0.14 |
| Age of disease onset | 0.05 | 0.71 | 0.05 | 0.67 | −0.06 | 0.62 |
| BMI | −0.33 | 0.14 | 0.56 | 0.01 | 0.24 | 0.29 |
| Leukocytes | 0.02 | 0.92 | 0.21 | 0.33 | 0.22 | 0.29 |
| ESR | 0.35 | 0.09 | 0.36 | 0.08 | 0.12 | 0.58 |
| CRP | 0.43 | 0.04 | 0.27 | 0.20 | 0.33 | 0.11 |
| AST | −0.22 | 0.29 | 0.12 | 0.58 | 0.10 | 0.62 |
| ALT | −0.44 | 0.03 | 0.17 | 0.41 | 0.10 | 0.64 |
| Creatinin | 0.03 | 0.98 | 0.45 | 0.03 | 0.09 | 0.66 |
| Sodium | 0.08 | 0.74 | 0.13 | 0.57 | 0.08 | 0.73 |
| Potassium | 0.26 | 0.27 | 0.19 | 0.41 | 0.06 | 0.79 |
| Cholesterol | −0.23 | 0.28 | 0.01 | 0.95 | 0.30 | 0.16 |
| LDL | −0.40 | 0.07 | 0.05 | 0.83 | 0.01 | 0.97 |
| Triglycerides | −0.02 | 0.94 | 0.29 | 0.19 | −0.01 | 0.97 |
| Glucose | −0.02 | 0.92 | 0.43 | 0.05 | 0.24 | 0.29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Słuczanowska-Głabowska, S.; Staniszewska, M.; Marchlewicz, M.; Duchnik, E.; Łuczkowska, K.; Safranow, K.; Machaliński, B.; Pawlik, A. Adiponectin, Leptin and Resistin in Patients with Psoriasis. J. Clin. Med. 2023, 12, 663. https://doi.org/10.3390/jcm12020663
Słuczanowska-Głabowska S, Staniszewska M, Marchlewicz M, Duchnik E, Łuczkowska K, Safranow K, Machaliński B, Pawlik A. Adiponectin, Leptin and Resistin in Patients with Psoriasis. Journal of Clinical Medicine. 2023; 12(2):663. https://doi.org/10.3390/jcm12020663
Chicago/Turabian StyleSłuczanowska-Głabowska, Sylwia, Marzena Staniszewska, Mariola Marchlewicz, Ewa Duchnik, Karolina Łuczkowska, Krzysztof Safranow, Bogusław Machaliński, and Andrzej Pawlik. 2023. "Adiponectin, Leptin and Resistin in Patients with Psoriasis" Journal of Clinical Medicine 12, no. 2: 663. https://doi.org/10.3390/jcm12020663