
Evaluation of Masticatory Muscles in Adult Patients with Maxillary Hypoplasia Treated with Surgically Assisted Rapid Maxillary Expansion (SARME): A Retrospective Study

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection and Inclusion Criteria
2.2. Surgical Procedure
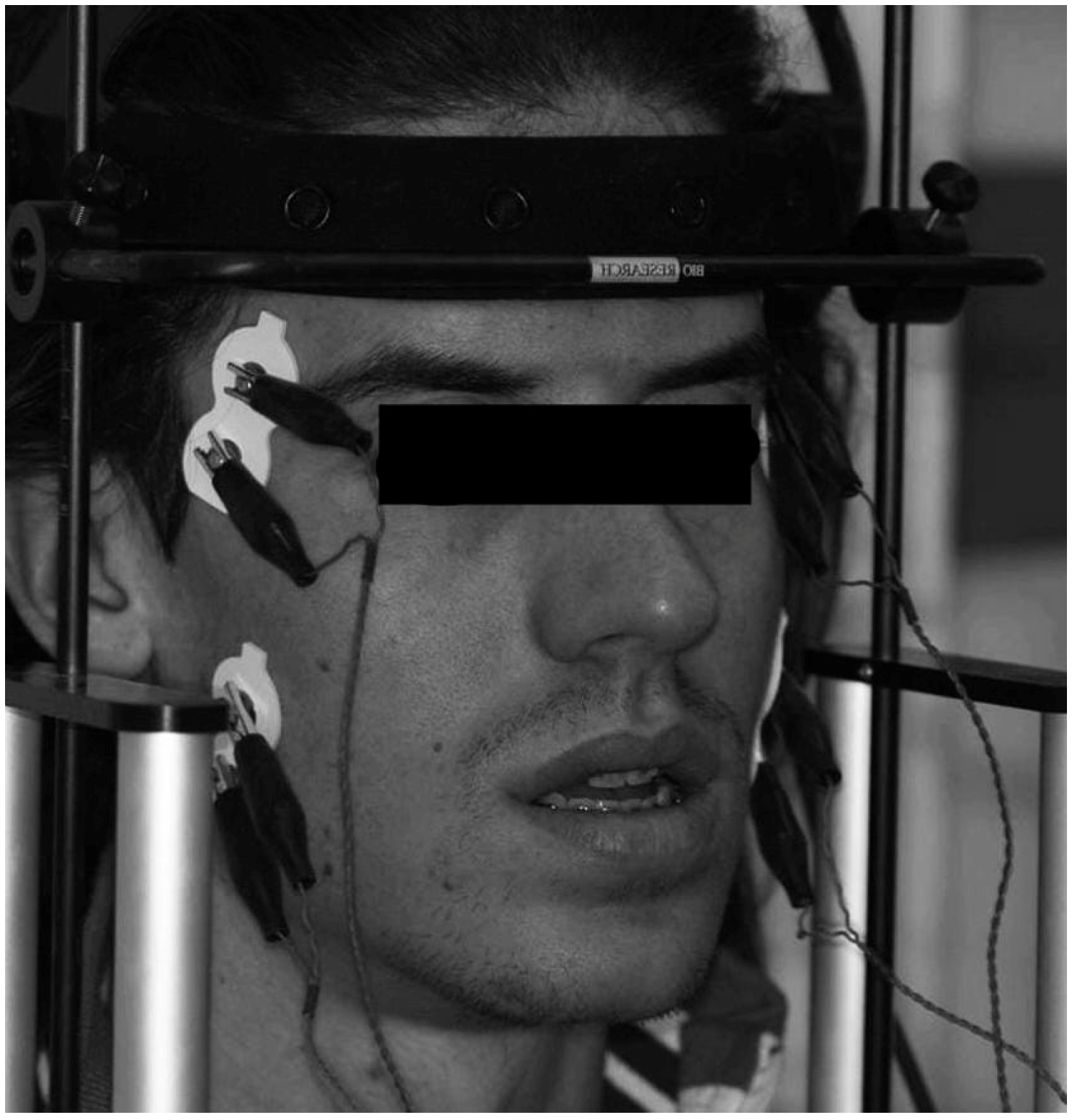
2.3. EMG Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caprioglio, A.; Meneghel, M.; Fastuca, R.; Zecca, P.A.; Nucera, R.; Nosetti, L. Rapid maxillary expansion in growing patients: Correspondence between 3-dimensional airway changes and polysomnography. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Di Carlo, G.; Cornelis, M.A.; Cattaneo, P.M. Three-dimensional analyses of short- and long-term effects of rapid maxillary expansion on nasal cavity and upper airway: A systematic review and meta-analysis. Orthod. Craniofac. Res. 2020, 23, 250–276. [Google Scholar] [CrossRef] [PubMed]
- Verstraaten, J.; Kuijpers-Jagtman, A.M.; Mommaerts, M.Y.; Bergé, S.J.; Nada, R.M.; Schols, J.G.J.H. A systematic review of the effects of bone-borne surgical assisted rapid maxillary expansion. J. Cranio-Maxillo-Facial Surg. 2010, 38, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Chamberland, S.; Proffit, W.R. Short-term and long-term stability of surgically assisted rapid palatal expansion revisited. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 815–822.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abate, A.; Cavagnetto, D.; Fama, A.; Matarese, M.; Lucarelli, D.; Assandri, F. Short term effects of rapid maxillary expansion on breathing function assessed with spirometry: A case-control study. Saudi Dent. J. 2020, 33, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Lanteri, V.; Cavagnetto, D.; Abate, A.; Mainardi, E.; Gaffuri, F.; Ugolini, A.; Maspero, C. Buccal Bone Changes Around First Permanent Molars and Second Primary Molars after Maxillary Expansion with a Low Compliance Ni-Ti Leaf Spring Expander. Int. J. Environ. Res. Public Health 2020, 17, 9104. [Google Scholar] [CrossRef]
- Abate, A.; Cavagnetto, D.; Rusconi, F.M.E.; Paolo, C.; Luca, E. Safety and Effects of the Rapid Maxillary Expander on Temporomandibular Joint in Subjects Affected by Juvenile Idiopathic Arthritis: A Retrospective Study. Children 2021, 8, 33. [Google Scholar] [CrossRef]
- Lindsten, R.; Ögaard, B.; Larsson, E.; Bjerklin, K. Transverse Dental and Dental Arch Depth Dimensions in the Mixed Dentition in a Skeletal Sample from the 14th to the 19th Century and Norwegian Children and Norwegian Sami Children of Today. Angle Orthod. 2002, 72, 439–448. [Google Scholar] [CrossRef]
- Lanteri, V.; Abate, A.; Cavagnetto, D.; Ugolini, A.; Gaffuri, F.; Gianolio, A.; Maspero, C. Cephalometric Changes Following Maxillary Expansion with Ni-Ti Leaf Springs Palatal Expander and Rapid Maxillary Expander: A Retrospective Study. Appl. Sci. 2021, 11, 5748. [Google Scholar] [CrossRef]
- Lehman, J.A.J.; Haas, A.J. Surgical-orthodontic correction of transverse maxillary deficiency. Clin. Plast. Surg. 1989, 16, 749–755. [Google Scholar] [CrossRef]
- Timms, D.J. An occlusal analysis of lateral maxillary expansion with midpalatal suture opening. Dent. Pract. Dent. Rec. 1968, 18, 435–441. [Google Scholar] [PubMed]
- Wertz, R.A. Skeletal and dental changes accompanying rapid midpalatal suture opening. Am. J. Orthod. 1970, 58, 41–66. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, K.; Quinn, P.D. Surgically-assisted rapid palatal expansion for management of transverse maxillary deficiency. J. Oral Maxillofac. Surg. 1997, 55, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.H.; Woo, A.; Zagarinsky, J.; Vanarsdall, R.L.; Fonseca, R.J. Maxillary sagittal and vertical displacement induced by surgically assisted rapid palatal expansion. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 144–148. [Google Scholar] [CrossRef]
- Vilani, G.N.L.; Mattos, C.T.; de Oliveira Ruellas, A.C.; Maia, L.C. Long-term dental and skeletal changes in patients submitted to surgically assisted rapid maxillary expansion: A meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 689–697. [Google Scholar] [CrossRef]
- Gurgel, J.A.; Tiago, C.M.; Normando, D. Transverse changes after surgically assisted rapid palatal expansion. Int. J. Oral Maxillofac. Surg. 2014, 43, 316–322. [Google Scholar] [CrossRef]
- Koudstaal, M.J.; Poort, L.J.; van der Wal, K.G.H.; Wolvius, E.B.; Prahl-Andersen, B.; Schulten, A.J.M. Surgically assisted rapid maxillary expansion (SARME): A review of the literature. Int. J. Oral Maxillofac. Surg. 2005, 34, 709–714. [Google Scholar] [CrossRef]
- Betts, N.J.; Vanarsdall, R.L.; Barber, H.D.; Higgins-Barber, K.; Fonseca, R.J. Diagnosis and treatment of transverse maxillary deficiency. Int. J. Adult Orthodon. Orthognath. Surg. 1995, 10, 75–96. [Google Scholar]
- Mortellaro, C.; Migliario, M.; Bologna, G.; Bello, L.; Lucchina, A.G.; Tetè, S. Rapid expansion of the palate with a new surgical technique. J. Craniofac. Surg. 2010, 21, 892–899. [Google Scholar] [CrossRef]
- Didier, H.; Assandri, F.; Gaffuri, F.; Cavagnetto, D.; Abate, A.; Villanova, M.; Maiorana, C. The Role of Dental Occlusion and Neuromuscular Behavior in Professional Ballet Dancers’ Performance: A Pilot Study. Healthcare 2021, 9, 251. [Google Scholar] [CrossRef]
- de Felício, C.M.; Freitas, R.L.R.G.; Vitti, M.; Regalo, S.C.H. Comparison of upper and lower lip muscle activity between stutterers and fluent speakers. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 1187–1192. [Google Scholar] [CrossRef] [PubMed]
- Foschi, D.; Abate, A.; Maspero, C.; Solimei, L.; Lanteri, C.; Lanteri, V. Method Presentation of a New Integrated Orthodontic-Conservative Approach for Minimally Invasive Full Mouth Rehabilitation: Speed Up Therapy. Biomedicines 2022, 10, 2536. [Google Scholar] [CrossRef] [PubMed]
- Galo, R.; Vitti, M.; da Glória Chiarello Mattos, M.; Regalo, S.C.H. Masticatory muscular activation in elderly individuals during chewing. Gerodontology 2007, 24, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Silva Andrade, A.; Gameiro, G.H.; Derossi, M.; Gavião, M.B.D. Posterior crossbite and functional changes. A systematic review. Angle Orthod. 2009, 79, 380–386. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Sforza, C.; Miani, A.J.; D’Addona, A.; Barbini, E. Electromyographic activity of human masticatory muscles in normal young people. Statistical evaluation of reference values for clinical applications. J. Oral Rehabil. 1993, 20, 271–280. [Google Scholar] [CrossRef]
- De Rossi, M.; De Rossi, A.; Hallak, J.E.C.; Vitti, M.; Regalo, S.C.H. Electromyographic evaluation in children having rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 355–360. [Google Scholar] [CrossRef]
- Michelotti, A.; Rongo, R.; Valentino, R.; D’Antò, V.; Bucci, R.; Danzi, G.; Cioffi, I. Evaluation of masticatory muscle activity in patients with unilateral posterior crossbite before and after rapid maxillary expansion. Eur. J. Orthod. 2019, 41, 46–53. [Google Scholar] [CrossRef]
- Steiner, C.C. Cephalometrics for you and me. Am. J. Orthod. 1953, 39, 729–755. [Google Scholar] [CrossRef]
- Bell, W.H.; Jacobs, J.D. Surgical-orthodontic correction of horizontal maxillary deficiency. J. Oral Surg. 1979, 37, 897–902. [Google Scholar]
- Ferrario, V.F.; Sforza, C.; Colombo, A.; Ciusa, V. An electromyographic investigation of masticatory muscles symmetry in normo-occlusion subjects. J. Oral Rehabil. 2000, 27, 33–40. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.F.; Tartaglia, G.M.; Galletta, A.; Grassi, G.P.; Sforza, C. The influence of occlusion on jaw and neck muscle activity: A surface EMG study in healthy young adults. J. Oral Rehabil. 2006, 33, 341–348. [Google Scholar] [CrossRef]
- Castroflorio, T.; Farina, D.; Bottin, A.; Piancino, M.G.; Bracco, P.; Merletti, R. Surface EMG of jaw elevator muscles: Effect of electrode location and inter-electrode distance. J. Oral Rehabil. 2005, 32, 411–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sverzut, C.E.; Martorelli, K.; Jabur, R.; Petri, A.D.; Trivellato, A.E.; Siéssere, S.; Regalo, S.C.H. Effect of surgically assisted rapid maxillary expansion on masticatory muscle activity: A pilot study. Ann. Maxillofac. Surg. 2011, 1, 32–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Palma, E.; Tepedino, M.; Chimenti, C.; Tartaglia, G.M.; Sforza, C. Longitudinal effects of rapid maxillary expansion on masticatory muscles activity. J. Clin. Exp. Dent. 2017, 9, e635–e640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abate, A.; Gaffuri, F.; Lanteri, V.; Fama, A.; Ugolini, A.; Mannina, L.; Maspero, C. A CBCT based analysis of the correlation between volumetric morphology of the frontal sinuses and the facial growth pattern in caucasian subjects. A cross-sectional study. Head Face Med. 2022, 18, 4. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Sforza, C.; Serrao, G. The influence of crossbite on the coordinated electromyographic activity of human masticatory muscles during mastication. J. Oral Rehabil. 1999, 26, 575–581. [Google Scholar] [CrossRef]
- Belser, U.C.; Hannam, A.G. The contribution of the deep fibers of the masseter muscle to selected tooth-clenching and chewing tasks. J. Prosthet. Dent. 1986, 56, 629–635. [Google Scholar] [CrossRef]
- Chaves, T.C.; Dos Santos Aguiar, A.; Felicio, L.R.; Greghi, S.M.; Hallak Regalo, S.C.; Bevilaqua-Grossi, D. Electromyographic ratio of masseter and anterior temporalis muscles in children with and without temporomandibular disorders. Int. J. Pediatr. Otorhinolaryngol. 2017, 97, 35–41. [Google Scholar] [CrossRef]
- Karkazis, H.C.; Kossioni, A.E. Re-examination of the surface EMG activity of the masseter muscle in young adults during chewing of two test foods. J. Oral Rehabil. 1997, 24, 216–223. [Google Scholar] [CrossRef]
- Bergamini, M.; Pierleoni, F.; Gizdulich, A.; Bergamini, C. Dental occlusion and body posture: A surface EMG study. Cranio 2008, 26, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, P.H.A.; Moura, L.B.; Trento, G.S.; Holzinger, D.; Gabrielli, M.A.C.; Gabrielli, M.F.R.; Pereira Filho, V.A. Surgically assisted rapid maxillary expansion: A systematic review of complications. Int. J. Oral Maxillofac. Surg. 2020, 49, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Galbiati, G.; Maspero, C.; Giannini, L.; Guenza, G.C.; Zanoni, F.; Farronato, G. Orthodontic-surgical treatment and respiratory function: Rhinomanometric assessment. Minerva Stomatol. 2017, 66, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Di Palma, E.; Gasparini, G.; Pelo, S.; Tartaglia, G.M.; Chimenti, C. Activities of masticatory muscles in patients after orthognathic surgery. J. Cranio-Maxillo-Facial Surg. 2009, 37, 417–420. [Google Scholar] [CrossRef]
- Farronato, G.; Maspero, C.; Giannini, L.; Farronato, D. Occlusal splint guides for presurgical orthodontic treatment. J. Clin. Orthod. 2008, 42, 508–512. [Google Scholar]
- Di Palma, E.; Tepedino, M.; Chimenti, C.; Tartaglia, G.M.; Sforza, C. Effects of the functional orthopaedic therapy on masticatory muscles activity. J. Clin. Exp. Dent. 2017, 9, e886–e891. [Google Scholar] [CrossRef] [Green Version]
- Arat, F.E.; Arat, Z.M.; Acar, M.; Beyazova, M.; Tompson, B. Muscular and condylar response to rapid maxillary expansion. Part 1: Electromyographic study of anterior temporal and superficial masseter muscles. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 815–822. [Google Scholar] [CrossRef]
- De Felício, C.M.; Mapelli, A.; Sidequersky, F.V.; Tartaglia, G.M.; Sforza, C. Mandibular kinematics and masticatory muscles EMG in patients with short lasting TMD of mild-moderate severity. J. Electromyogr. Kinesiol. 2013, 23, 627–633. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Indices | |
|---|---|
| Percentage overlapping coefficient (POC, unit: %) | An index of the symmetric distribution of muscular activity as determined by occlusion. Calculations were performed for each pair of muscles, resulting in a POC for the temporalis muscles (POCt) and a POC for the masseters (POCm). |
| Torque coefficient (TC, unit: %) | Index of the possible presence of a mandibular torque. |
| Activity Index (Ac, unit: %) | Index suggesting the prevailing area of occlusal contacts. |
| Standardized activity (unit: μV/μV s %) | The total standardized electric activity developed by the muscles investigated during the maximum voluntary clamping (MVC) was calculated as the average integrated areas of temporalis and masseter Superficial electromyographic (EMG) potentials over time. |
| Variable | T0 | T1 | Difference | p-Value | |
|---|---|---|---|---|---|
| POC t (%) | Mean | 86.52 | 85.52 | 1 | 0.317 |
| S.D | 3.75 | 5.73 | 3.38 | ||
| POC m (%) | Mean | 84.23 | 85.78 | −1.55 | 0.561 |
| S.D | 8.57 | 5.71 | 7.17 | ||
| TC (%) | Mean | 8.91 | 8.23 | 0.68 | 0.521 |
| S.D | 3.60 | 2.15 | 3.29 | ||
| Ac (%) | Mean | 2.35 | 4.81 | −2.46 | 0.533 |
| S.D | 12.28 | 10.62 | 14.22 | ||
| Standardized activity (μV/μV s %) | Mean | 133.69 | 132.87 | 0.82 | 0.925 |
| S.D | 43.89 | 50.4 | 36.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abate, A.; Lanteri, V.; Marcolongo, L.; Solimei, L.; Maspero, C. Evaluation of Masticatory Muscles in Adult Patients with Maxillary Hypoplasia Treated with Surgically Assisted Rapid Maxillary Expansion (SARME): A Retrospective Study. J. Clin. Med. 2023, 12, 607. https://doi.org/10.3390/jcm12020607
Abate A, Lanteri V, Marcolongo L, Solimei L, Maspero C. Evaluation of Masticatory Muscles in Adult Patients with Maxillary Hypoplasia Treated with Surgically Assisted Rapid Maxillary Expansion (SARME): A Retrospective Study. Journal of Clinical Medicine. 2023; 12(2):607. https://doi.org/10.3390/jcm12020607
Chicago/Turabian StyleAbate, Andrea, Valentina Lanteri, Loris Marcolongo, Luca Solimei, and Cinzia Maspero. 2023. "Evaluation of Masticatory Muscles in Adult Patients with Maxillary Hypoplasia Treated with Surgically Assisted Rapid Maxillary Expansion (SARME): A Retrospective Study" Journal of Clinical Medicine 12, no. 2: 607. https://doi.org/10.3390/jcm12020607