
Differentiated Effect of Smoking on Disease Activity and Quality of Life among Different Spondyloarthritis Phenotypes
 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
Statistical Analysis
3. Results
3.1. Summary of Study Population
Distribution of Cardiometabolic Factors between Both SpA Populations
3.2. Cardiometabolic Factors and Disease Outcomes
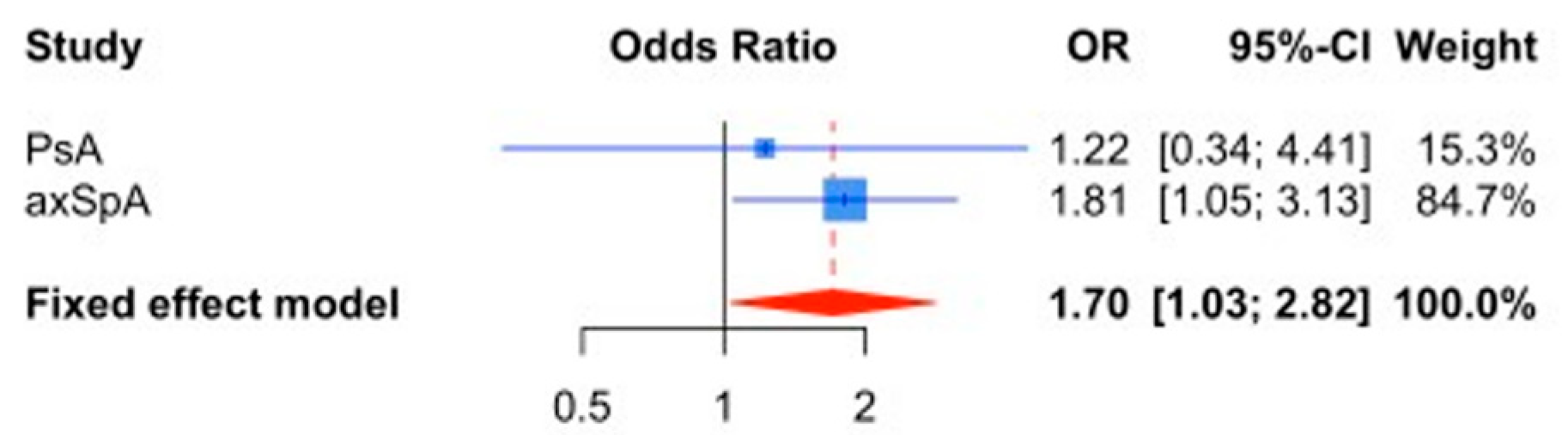
3.3. Meta-Analysis of the Tobacco Effect on Disease Activity
3.4. Impact of Cardiometabolic Risk Factors on Quality of Life
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dougados, M.; Baeten, D. Spondyloarthritis. Lancet 2011, 377, 2127–2137. [Google Scholar] [CrossRef]
- Gudu, T.; Gossec, L. Quality of life in psoriatic arthritis. Expert Rev. Clin. Immunol. 2018, 14, 405–417. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Cumbrera, M.; Poddubnyy, D.; Gossec, L.; Gálvez-Ruiz, D.; Bundy, C.; Mahapatra, R.; Makri, S.; Christen, L.; Delgado-Domínguez, C.J.; Sanz-Gómez, S.; et al. The European Map of Axial Spondyloarthritis: Capturing the Patient Perspective—An Analysis of 2846 Patients Across 13 Countries. Curr. Rheumatol. Rep. 2019, 21, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magrey, M.; Ritchlin, C. Measuring outcomes in ankylosing spondylitis: Pearls and pitfalls. Curr. Opin. Rheumatol. 2019, 31, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Desthieux, C.; Granger, B.; Balanescu, A.R.; Balint, P.; Braun, J.; Canete, J.D.; Heiberg, T.; Helliwell, P.S.; Kalyoncu, U.; Kvien, T.K.; et al. Determinants of Patient-Physician Discordance in Global Assessment in Psoriatic Arthritis: A Multicenter European Study. Arthritis Care Res. 2017, 69, 1606–1611. [Google Scholar] [CrossRef] [Green Version]
- Husni, M.E.; Merola, J.F.; Davin, S. The psychosocial burden of psoriatic arthritis. Semin. Arthritis Rheum. 2017, 47, 351–360. [Google Scholar] [CrossRef]
- Liew, J.W.; Ramiro, S.; Gensler, L.S. Cardiovascular morbidity and mortality in ankylosing spondylitis and psoriatic arthritis. Best Pract. Res. Clin. Rheumatol. 2018, 32, 369–389. [Google Scholar] [CrossRef]
- Kamata, M.; Tada, Y. Efficacy and Safety of Biologics for Psoriasis and Psoriatic Arthritis and Their Impact on Comorbidities: A Literature Review. Int. J. Mol. Sci. 2020, 21, 1690. [Google Scholar] [CrossRef] [Green Version]
- Molto, A.; Nikiphorou, E. Comorbidities in Spondyloarthritis. Front. Med. 2018, 5, 62. [Google Scholar] [CrossRef]
- Scriffignano, S.; Perrotta, F.M.; De Socio, A.; Lubrano, E. Role of comorbidities in spondyloarthritis including psoriatic arthritis. Clin. Rheumatol. 2019, 38, 3–10. [Google Scholar] [CrossRef]
- Zhao, S.S.; Goodson, N.J.; Robertson, S.; Gaffney, K. Smoking in spondyloarthritis: Unravelling the complexities. Rheumatology 2020, 59, 1472–1481. [Google Scholar] [CrossRef]
- Ciurea, A.; Scherer, A.; Weber, U.; Exer, P.; Bernhard, J.; Tamborrini, G.; Riek, M.; Müller, R.B.; Weiss, B.; Nissen, M.J.; et al. Impaired response to treatment with tumour necrosis factor α inhibitors in smokers with axial spondyloarthritis. Ann. Rheum. Dis. 2016, 75, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Castro, S.; Pardo, E.; Charca, L.; Pino, M.; Fernández, S.; Alperi, M.; Arboleya, L.; Queiro, R. Performance of the ASAS Health Index for the Evaluation of Spondyloarthritis in Daily Practice. J. Rheumatol. 2020, 47, 1483–1489. [Google Scholar] [CrossRef] [PubMed]
- Morante, I.; Aurrecoechea, E.; Villa, I.; Santos, M.; Riancho, L.; Queiro, R. Construct validity of the ASAS health index in psoriatic arthritis: A cross-sectional analysis. Rheumatology 2021, 60, 1465–1473. [Google Scholar] [CrossRef]
- García-Valle, A.; Llano, J.M.A.-D.; Fariña-González, A.J.; González-Benítez, R.D.; Queiro-Silva, R. Construct Validity of the Routine Assessment of Patient Index Data 3 (RAPID3) in the Evaluation of Axial Spondyloarthritis. J. Rheumatol. 2022, 49, 36–43. [Google Scholar] [CrossRef]
- Alonso, S.; Morante, I.; Alperi, M.; Queiro, R. The ASAS Health Index: A New Era for Health Impact Assessment in Spondyloar-thritis. J. Rheumatol. 2022, 49, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Gossec, L.; de Wit, M.; Kiltz, U.; Braun, J.; Kalyoncu, U.; Scrivo, R.; Maccarone, M.; Carton, L.; Otsa, K.; Sooäär, I.; et al. A patient-derived and patient-reported outcome measure for assessing psoriatic arthritis: Elaboration and preliminary validation of the Psoriatic Arthritis Impact of Disease (PsAID) questionnaire, a 13-country EULAR initiative. Ann. Rheum. Dis. 2014, 73, 1012–1019. [Google Scholar] [CrossRef] [Green Version]
- Pincus, T.; Askanase, A.D.; Swearingen, C.J. A Multi-dimensional Health Assessment Questionnaire (MDHAQ) and routine as-sessment of patient index data (RAPID3) scores are informative in patients with all rheumatic diseases. Rheum. Dis. Clin. N. Am. 2009, 35, 819–827. [Google Scholar] [CrossRef]
- Kaczynski, A.T.; Manske, S.R.; Mannell, R.C.; Grewal, K. Smoking and physical activity: A systematic review. Am. J. Health Behav. 2008, 32, 93–110. [Google Scholar] [CrossRef]
- Ramiro, S.; Landewé, R.; van Tubergen, A.; Boonen, A.; Stolwijk, C.; Dougados, M.; van den Bosch, F.; van der Heijde, D. Lifestyle factors may modify the effect of disease activity on radiographic progression in patients with ankylosing spondylitis: A longitudinal analysis. RMD Open 2015, 1, e000153. [Google Scholar] [CrossRef]
- Queiro, R.; Pardo, E.; Charca, L.; Alonso, S.; Arboleya, L.; Alperi, M. Analysis by Age Group of Disease Outcomes in Patients with Psoriatic Arthritis: A Cross-Sectional Multicentre Study. Drugs Aging 2020, 37, 99–104. [Google Scholar] [CrossRef]
- Garrido-Cumbrera, M.; Hillmann, O.; Mahapatra, R.; Trigos, D.; Zajc, P.; Weiss, L.; Bostynets, C.; Gossec, L.; Coates, L.C. Improving the management of psoriatic arthritis and axial spondy-loarthritis: Roundtable discussions with healthcare professionals and patients. Rheumatol. Ther. 2017, 4, 219–231. [Google Scholar] [CrossRef] [Green Version]
- Swinnen, T.W.; Westhovens, R.; Dankaerts, W.; De Vlam, K. Widespread pain in axial spondyloarthritis: Clinical importance and gender differences. Arthritis Res. Ther. 2018, 20, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Queiro, R.; Cañete, J.D. Impact of cardiovascular risk factors on the achievement of therapeutic goals in psoriatic arthritis: Is there any association? Clin. Rheumatol. 2018, 37, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Alonso, S.; Villa, I.; Fernández, S.; Martín, J.L.; Charca, L.; Pino, M.; Riancho, L.; Morante, I.; Santos, M.; Brandy, A.; et al. Multicenter Study of Secukinumab Survival and Safety in Spondyloarthritis and Psoriatic Arthritis: SEcukinumab in Cantabria and ASTURias Study. Front. Med. 2021, 8, 679009. [Google Scholar] [CrossRef] [PubMed]
- Almodóvar, R.; Zarco, P.; Otón, T.; Carmona, L. Effect of Weight Loss on Activity in Psoriatic Arthritis: A Systematic Review. Reumatol. Clín. (Engl. Ed.) 2018, 14, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Challoner, B.; Khattak, M.; Moots, R.J.; Goodson, N.J. Increasing smoking intensity is associated with increased disease activity in axial spondyloarthritis. Rheumatol. Int. 2017, 37, 239–244. [Google Scholar] [CrossRef]


{kind=link}
| Axial Spondyloarthritis | Psoriatic Arthritis |
|---|---|
| BASDAI 3.59 ± 2.40 | DAPSA 9.7 ± 7.8 |
| ASDAS-CRP 2.07 ± 0.83 | PsAID 2.8 ± 2.3 |
| ASAS-HI 5.4 ± 3.8 | ASAS HI 5.8 ± 4.3 |
| RAPID3 9.45 ± 6.7 | ASAS HI-PsAID correlation, r: 0.75, 95%CI: 0.64–0-83, p < 0.001. |
| CM Factor | PsA, n: 90 | axSpA, n: 242 | Total, n: 332 |
|---|---|---|---|
| Obesity, n (%) * | 21 (23) | 28 (12) | 49 (15) |
| Hypertension, n (%) * | 38 (42) | 38 (16) | 76 (23) |
| Diabetes, n (%) * | 14 (15) | 13 (5) | 27 (8) |
| Dyslipidemia, n (%) | 31 (34) | 56 (23) | 87 (26) |
| Smoking, n (%) * | 13 (14) | 81 (33) | 94 (28) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Castro, S.; García-Valle, A.; Morante-Bolado, I.; Braña, I.; Pardo, E.; Queiro, R. Differentiated Effect of Smoking on Disease Activity and Quality of Life among Different Spondyloarthritis Phenotypes. J. Clin. Med. 2023, 12, 551. https://doi.org/10.3390/jcm12020551
Alonso-Castro S, García-Valle A, Morante-Bolado I, Braña I, Pardo E, Queiro R. Differentiated Effect of Smoking on Disease Activity and Quality of Life among Different Spondyloarthritis Phenotypes. Journal of Clinical Medicine. 2023; 12(2):551. https://doi.org/10.3390/jcm12020551
Chicago/Turabian StyleAlonso-Castro, Sara, Andrea García-Valle, Isla Morante-Bolado, Ignacio Braña, Estefanía Pardo, and Rubén Queiro. 2023. "Differentiated Effect of Smoking on Disease Activity and Quality of Life among Different Spondyloarthritis Phenotypes" Journal of Clinical Medicine 12, no. 2: 551. https://doi.org/10.3390/jcm12020551