
Body Weight Reduction by Bariatric Surgery Reduces the Plasma Levels of the Novel Orexigenic Gut Hormone Insulin-like Peptide 5 in Patients with Severe Obesity

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Measurement of INSL5 Plasma Levels
2.3. Isolation of Human Adipose Tissue
2.4. RNA Isolation and Reverse Transcription PCR (RT-PCR) in Adipose Tissue
2.5. Western Blotting Analysis for INSL5 in Human Adipose Tissue
2.6. Statistical Analysis
3. Results
3.1. Clinical, Anthropometric, and Metabolic Characteristics of the Obese Patients before and after LSG
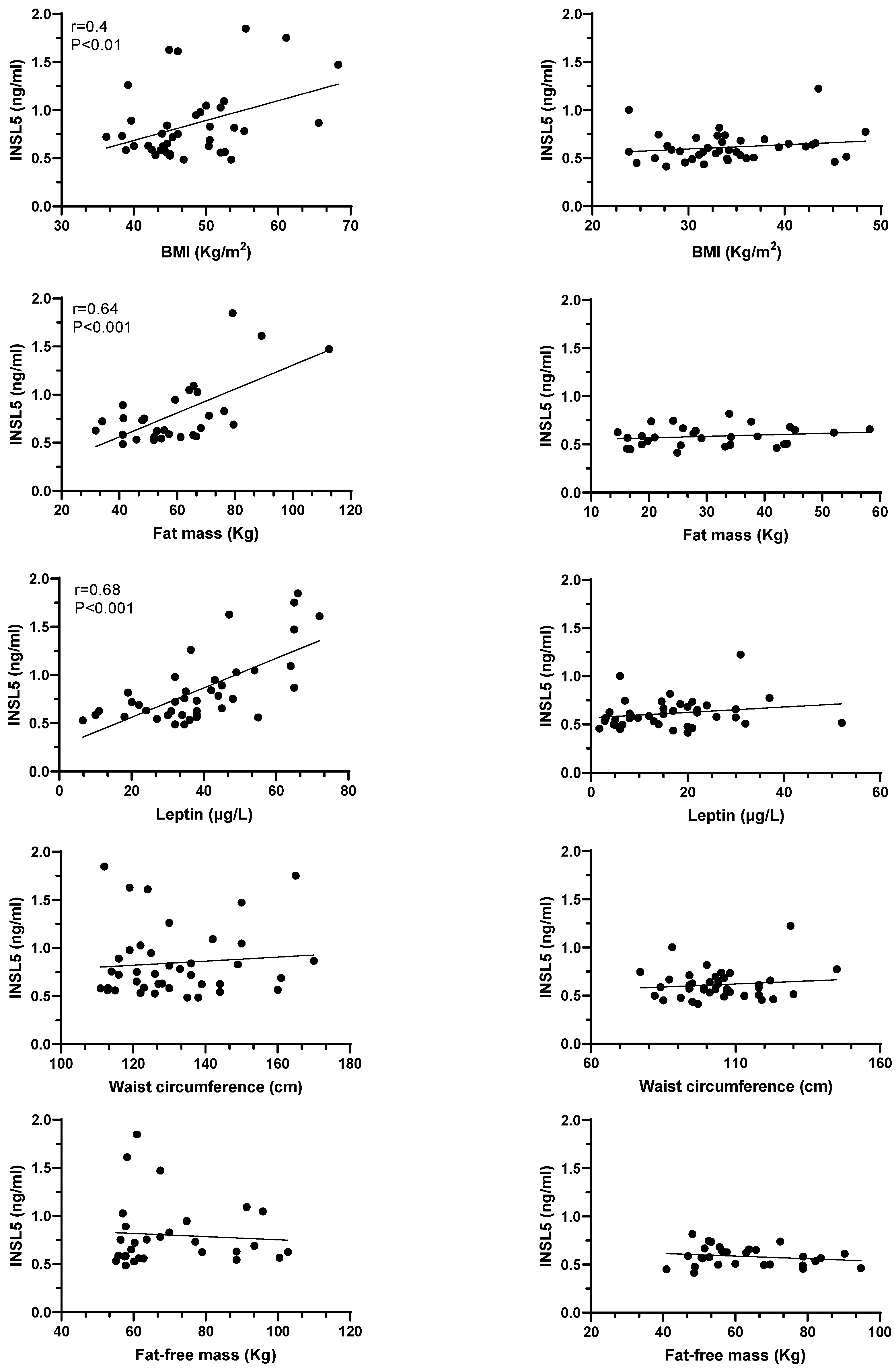
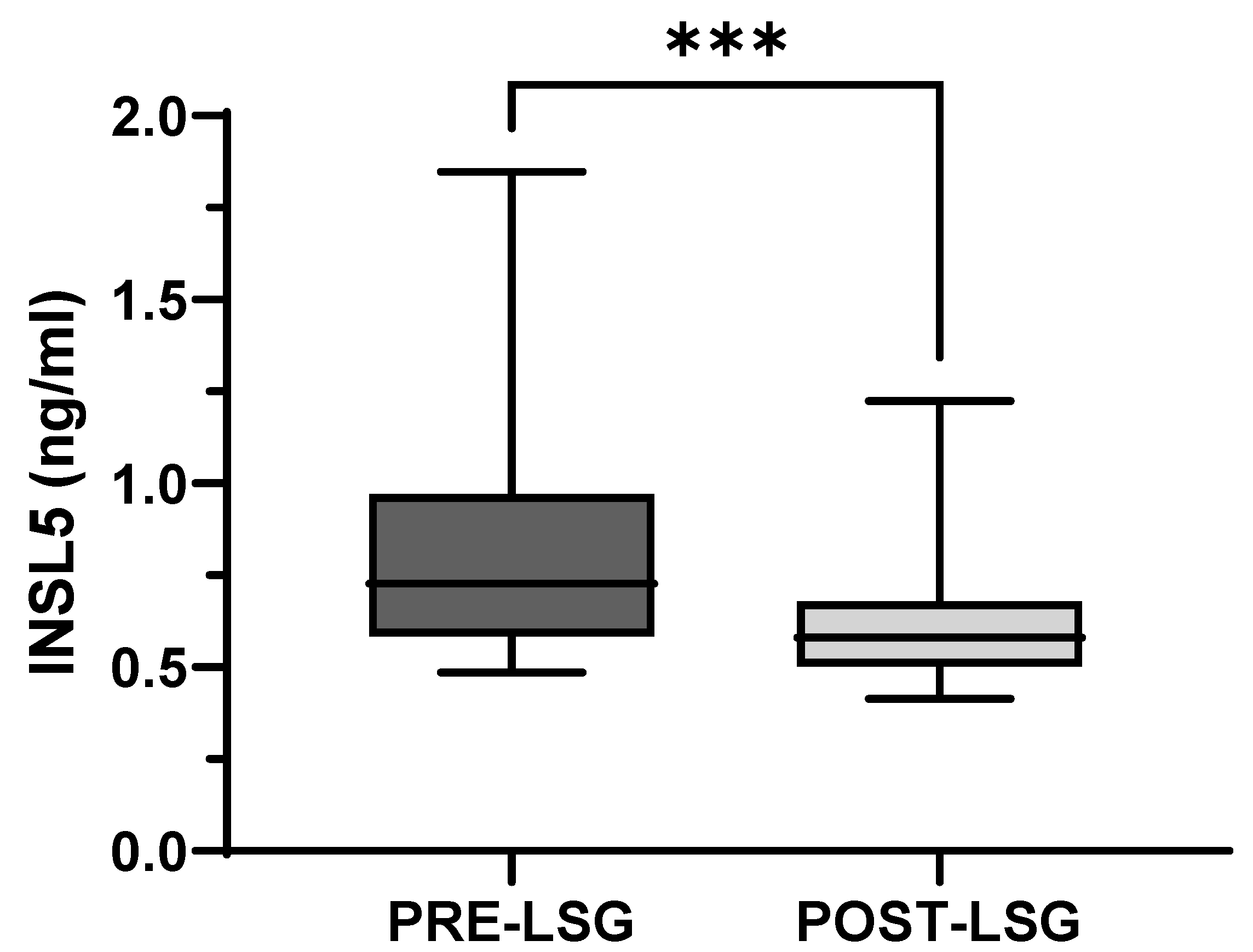
3.2. Plasma Levels of INSL5 before and after Laparoscopic Sleeve Gastrectomy
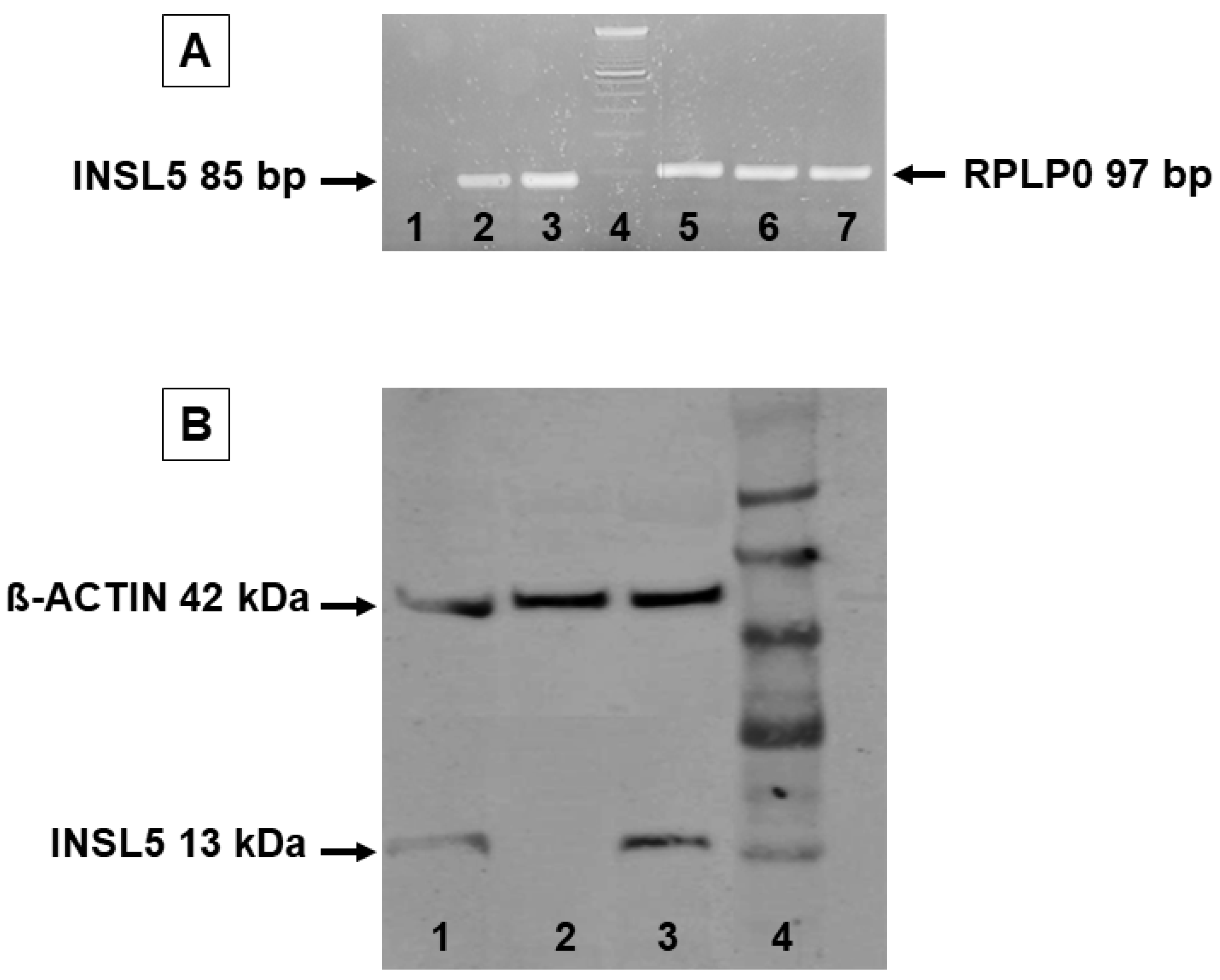
3.3. INSL5 mRNA and Protein Expression in Human White Adipose Tissue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, G.A.; Frühbeck, G.; Ryan, D.H.; Wilding, J.P. Management of obesity. Lancet 2016, 387, 1947–1956. [Google Scholar] [CrossRef] [PubMed]
- Whitlock, G.; Lewington, S.; Sherliker, P.; Clarke, R.; Emberson, J.; Halsey, J.; Qizilbash, N.; Collins, R.; Peto, R. Body-mass index and cause-specific mortality in 900,000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef] [PubMed]
- Sumithran, P.; Prendergast, L.A.; Delbridge, E.; Purcell, K.; Shulkes, A.; Kriketos, A.; Proietto, J. Long–term persistence of hormonal adaptation to weight loss. N. Engl. J. Med. 2011, 365, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.W.; Konz, E.C.; Frederich, R.C.; Wood, C.L. Long–term weight–loss mainteinance: A meta–analysis of US studies. Am. J. Clin. Nutr. 2001, 74, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Sjöström, L.; Peltonen, M.; Jacobson, P.; Sjöström, C.D.; Karason, K.; Wedel, H.; Ahlin, S.; Anveden, Å.; Bengtsson, C.; Bergmark, G.; et al. Bariatric surgery and long-term cardiovascular events. JAMA 2012, 307, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Goldstone, A.P.; Miras, A.D.; Scholtz, S.; Jackson, S.; Neff, K.J.; Pénicaud, L.; Geoghegan, J.; Chhina, N.; Durighel, G.; Bell, J.D.; et al. Link between increased satiety gut hormones and reduced food reward after gastric bypass surgery for obesity. J. Clin. Endocrinol. Metab. 2016, 101, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Benaiges, D.; Más-Lorenzo, A.; Goday, A.; Ramon, J.M.; Chillarón, J.J.; Pedro-Botet, J.; Flores-Le Roux, J.A. Laparoscopic sleeve gastrectomy: More than a restrictive bariatric surgery procedure? World J. Gastroenterol. 2015, 21, 11804–11814. [Google Scholar] [CrossRef] [PubMed]
- Grosse, J.; Heffron, H.; Burling, K.; Akhter-Hossain, M.; Habib, A.M.; Rogers, G.J.; Richards, P.; Larder, R.; Rimmington, D.; Adriaenssens, A.A.; et al. Insulin-like peptide 5 is an orexigenic gastrointestinal hormone. Proc. Natl. Acad. Sci. USA 2014, 111, 11133–11138. [Google Scholar] [CrossRef] [PubMed]
- Burnicka-Turek, O.; Mohamed, B.A.; Shirneshan, K.; Thanasupawat, T.; Hombach-Klonisch, S.; Klonisch, T.; Adham, I.M. INSL5-deficient mice display an alteration in glucose homeostasis and an impaired fertility. Endocrinology 2012, 153, 4655–4665. [Google Scholar] [CrossRef] [PubMed]
- Mashima, H.; Ohno, H.; Yamada, Y.; Sakai, T.; Ohnishi, H. INSL5 may be a unique marker of colorectal endocrine cells and neuroendocrine tumors. Biochem. Biophys. Res. Commun. 2013, 432, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Halls, M.L.; Bathgate, R.A.; Sutton, S.W.; Dschietzig, T.B.; Summers, R.J. International Union of Basic and Clinical Pharmacology. XCV. Recent advances in the understanding of the pharmacology and biological roles of relaxin family peptide receptors 1-4, the receptors for relaxin family peptides. Pharmacol. Rev. 2015, 67, 389–440. [Google Scholar] [CrossRef] [PubMed]
- Bathgate, R.A.D.; Halls, M.L.; Van der Westhuizen, E.T.; Callander, G.E.; Kocan, M.; Summers, R.J. Relaxin family peptides and their receptors. Physiol. Rev. 2013, 93, 405–480. [Google Scholar] [CrossRef] [PubMed]
- Rossato, M.; Granzotto, M.; Macchi, V.; Porzionato, A.; Petrelli, L.; Calcagno, A.; Vencato, J.; De Stefani, D.; Silvestrin, V.; Rizzuto, R.; et al. Human white adipocytes express the cold receptor TRPM8 which activation induces UCP1 expression, mitochondrial activation and heat production. Mol. Cell. Endocrinol. 2014, 383, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Editorial Office. Gastrointestinal Surgery for Severe Obesity. Obes. Surg. 1991, 1, 257–266. [Google Scholar]
- Belligoli, A.; Sanna, M.; Serra, R.; Fabris, R.; Dal Prà, C.; Conci, S.; Fioretto, P.; Prevedello, L.; Foletto, M.; Vettor, R.; et al. Incidence and predictors of hypoglycemia 1 year after laparoscopic sleeve gastrectomy. Obes. Surg. 2017, 27, 3179–3186. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Kuei, C.; Sutton, S.; Chen, J.; Bonaventure, P.; Wu, J.; Nepomuceno, D.; Kamme, F.; Tran, D.T.; Zhu, J.; et al. INSL5 is a high affinity specific agonist for GPCR142 (GPR100). J. Biol. Chem. 2005, 280, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Ricardo-Silgado, M.L.; McRae, A.; Acosta, A. Role of enteroendocrine hormones in appetite and glycemia. Obes. Med. 2021, 346, 100332. [Google Scholar] [CrossRef] [PubMed]
- Cummings, D.E.; Weigle, D.S.; Frayo, R.S.; Breen, P.A.; Ma, M.K.; Dellinger, E.P.; Purnell, J.Q. Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N. Engl. J. Med. 2002, 346, 1623–1630. [Google Scholar] [CrossRef] [PubMed]
- Ang, S.Y.; Hutchinson, D.S.; Evans, B.A.; Hossain, M.A.; Patil, N.; Bathgate, R.A.; Kocan, M.; Summers, R.J. The actions of relaxin family peptides on signal transduction pathways activated by the relaxin family peptide receptor RXFP4. Naunyn. Schmiedebergs. Arch. Pharmacol. 2017, 390, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Patil, N.A.; Rosengren, K.J.; Separovic, F.; Wade, J.D.; Bathgate, R.A.D.; Hossain, M.A. Relaxin family peptides: Structure-activity relationship studies. Br. J. Pharmacol. 2017, 174, 950–961. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Before-LSG | After-LSG | p | |
|---|---|---|---|
| Weight (Kg) | 133.2 ± 27.4 | 95.3 ± 23.1 | <0.0001 |
| BMI (Kg/m2) | 47.4 ± 7.0 | 33.8 ± 6.1 | <0.0001 |
| %Total body weight loss | - | 28.5 ± 8.8 | N.A. |
| Waist circumference (cm) | 131.4 ± 15.5 | 104.0 ± 14.6 | <0.0001 |
| Fat mass (Kg) | 59.4 ± 17.5 | 32.1 ± 13.4 | <0.0001 |
| Leptin (µg/L) | 38.0 ± 16.9 | 16.1 ± 13.5 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Vincenzo, A.; Crescenzi, M.; Granzotto, M.; Zancaner, S.; Fabris, R.; Foletto, M.; Prevedello, L.; Capone, F.; Vettor, R.; Rossato, M. Body Weight Reduction by Bariatric Surgery Reduces the Plasma Levels of the Novel Orexigenic Gut Hormone Insulin-like Peptide 5 in Patients with Severe Obesity. J. Clin. Med. 2023, 12, 3752. https://doi.org/10.3390/jcm12113752
Di Vincenzo A, Crescenzi M, Granzotto M, Zancaner S, Fabris R, Foletto M, Prevedello L, Capone F, Vettor R, Rossato M. Body Weight Reduction by Bariatric Surgery Reduces the Plasma Levels of the Novel Orexigenic Gut Hormone Insulin-like Peptide 5 in Patients with Severe Obesity. Journal of Clinical Medicine. 2023; 12(11):3752. https://doi.org/10.3390/jcm12113752
Chicago/Turabian StyleDi Vincenzo, Angelo, Marika Crescenzi, Marnie Granzotto, Sara Zancaner, Roberto Fabris, Mirto Foletto, Luca Prevedello, Federico Capone, Roberto Vettor, and Marco Rossato. 2023. "Body Weight Reduction by Bariatric Surgery Reduces the Plasma Levels of the Novel Orexigenic Gut Hormone Insulin-like Peptide 5 in Patients with Severe Obesity" Journal of Clinical Medicine 12, no. 11: 3752. https://doi.org/10.3390/jcm12113752