
Effects on Right Ventricular Function One Year after COVID-19-Related Pulmonary Embolism
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
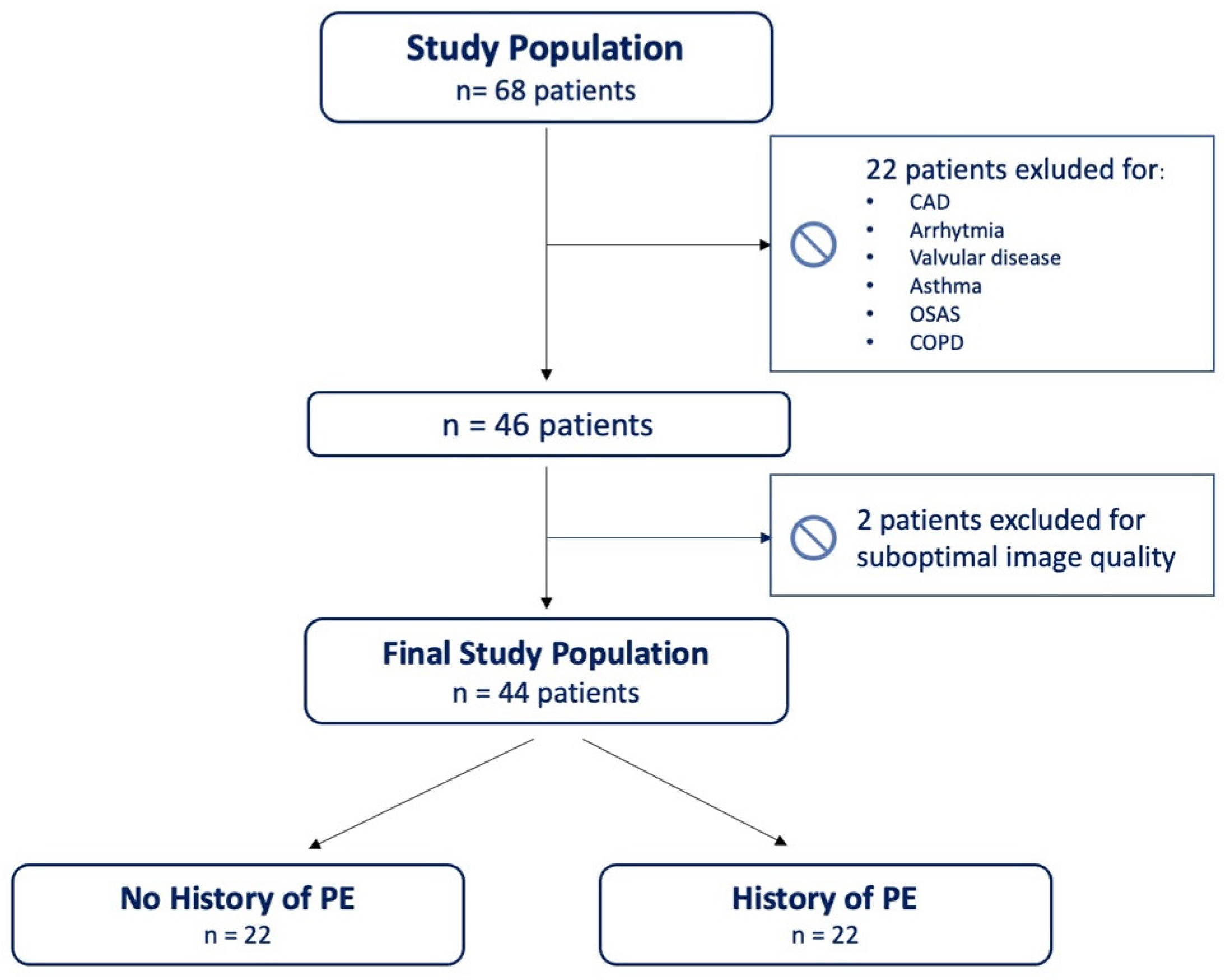
2.1. Patient Population and Data Collection
2.2. Echocardiographic Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Capone, V.; Cuomo, V.; Esposito, R.; Canonico, M.E.; Ilardi, F.; Prastaro, M.; Esposito, G.; Santoro, C. Epidemiology, Prognosis, and Clinical Manifestation of Cardiovascular Disease in COVID-19. Expert. Rev. Cardiovasc. Ther. 2020, 18, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Bonnemain, J.; Ltaief, Z.; Liaudet, L. The Right Ventricle in COVID-19. J. Clin. Med. 2021, 10, 2535. [Google Scholar] [CrossRef] [PubMed]
- Szekely, Y.; Lichter, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Gal Oz, A.; Rothschild, E.; Baruch, G.; Peri, Y.; et al. Spectrum of Cardiac Manifestations in COVID-19: A Systematic Echocardiographic Study. Circulation 2020, 142, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Volodarskiy, A.; Sultana, R.; Pollie, M.P.; Yum, B.; Nambiar, L.; Tafreshi, R.; Mitlak, H.W.; RoyChoudhury, A.; Horn, E.M.; et al. Prognostic Utility of Right Ventricular Remodeling Over Conventional Risk Stratification in Patients with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 1965–1977. [Google Scholar] [CrossRef]
- Li, Y.; Li, H.; Zhu, S.; Xie, Y.; Wang, B.; He, L.; Zhang, D.; Zhang, Y.; Yuan, H.; Wu, C.; et al. Prognostic Value of Right Ventricular Longitudinal Strain in Patients With COVID-19. JACC Cardiovasc. Imaging 2020, 13, 2287–2299. [Google Scholar] [CrossRef]
- WHO-2019-NCoV-Clinical-2020.4-Eng. Available online: https://apps.who.int/iris/bitstream/handle/10665/331446/WHO-2019-nCoV-clinical-2020.4-eng.pdf?sequence=1&isAllowed=y(accessed on 3 May 2023).
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT Imaging Features of 2019 Novel Coronavirus (2019-NCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.C.; Marino, P.N.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelista, A. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography. J. Am. Soc. Echocardiogr. 2009, 22, 107–133. [Google Scholar] [CrossRef]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography Endorsed by the European Association of Echocardiography, a Registered Branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713; quiz 786–788. [Google Scholar] [CrossRef]
- Ilardi, F.; Marchetta, S.; Martinez, C.; Sprynger, M.; Ancion, A.; Manganaro, R.; Sugimoto, T.; Tsugu, T.; Postolache, A.; Piette, C.; et al. Impact of Aortic Stenosis on Layer-Specific Longitudinal Strain: Relationship with Symptoms and Outcome. Eur. Heart J. Cardiovasc. Imaging 2019, 21, 408–416. [Google Scholar] [CrossRef]
- Sugimoto, T.; Dulgheru, R.; Bernard, A.; Ilardi, F.; Contu, L.; Addetia, K.; Caballero, L.; Akhaladze, N.; Athanassopoulos, G.D.; Barone, D.; et al. Echocardiographic Reference Ranges for Normal Left Ventricular 2D Strain: Results from the EACVI NORRE Study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Muraru, D.; Haugaa, K.; Donal, E.; Stankovic, I.; Voigt, J.U.; Petersen, S.E.; Popescu, B.A.; Marwick, T. Right Ventricular Longitudinal Strain in the Clinical Routine: A State-of-the-Art Review. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 898–912. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Scarafile, R.; Riegler, L.; Liccardo, B.; Crescibene, F.; Cocchia, R.; Bossone, E. Right Ventricular Function and Pulmonary Pressures as Independent Predictors of Survival in Patients With COVID-19 Pneumonia. JACC Cardiovasc. Imaging 2020, 13, 2467–2468. [Google Scholar] [CrossRef] [PubMed]
- Ghidini, S.; Gasperetti, A.; Winterton, D.; Vicenzi, M.; Busana, M.; Pedrazzini, G.; Biasco, L.; Tersalvi, G. Echocardiographic Assessment of the Right Ventricle in COVID-19: A Systematic Review. Int. J. Cardiovasc. Imaging 2021, 37, 3499–3512. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, C.; Annunziata, A.; Flora, M.; Mariniello, D.F.; Allocca, V.; Palma, M.I.; Coppola, A.; Meoli, I.; Pafundi, P.C.; Fiorentino, G. Three Month Follow-Up of Patients With COVID-19 Pneumonia Complicated by Pulmonary Embolism. Front. Mol. Biosci. 2022, 8, 809186. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Cante, L.; Palermi, S.; Carbone, A.; Ilardi, F.; Sabatella, F.; Crescibene, F.; Di Maio, M.; Giallauria, F.; Messalli, G.; et al. COVID-19 Myocarditis: Prognostic Role of Bedside Speckle-Tracking Echocardiography and Association with Total Scar Burden. Int. J. Environ. Res. Public. Health 2022, 19, 5898. [Google Scholar] [CrossRef]
- Carluccio, E.; Biagioli, P.; Alunni, G.; Murrone, A.; Zuchi, C.; Coiro, S.; Riccini, C.; Mengoni, A.; D’Antonio, A.; Ambrosio, G. Prognostic Value of Right Ventricular Dysfunction in Heart Failure With Reduced Ejection Fraction: Superiority of Longitudinal Strain Over Tricuspid Annular Plane Systolic Excursion. Circ. Cardiovasc. Imaging 2018, 11, e006894. [Google Scholar] [CrossRef] [PubMed]
- Buonauro, A.; Santoro, C.; Galderisi, M.; Canora, A.; Sorrentino, R.; Esposito, R.; Lembo, M.; Canonico, M.E.; Ilardi, F.; Fazio, V.; et al. Impaired Right and Left Ventricular Longitudinal Function in Patients with Fibrotic Interstitial Lung Diseases. J. Clin. Med. 2020, 9, 587. [Google Scholar] [CrossRef]
- Bieber, S.; Kraechan, A.; Hellmuth, J.C.; Muenchhoff, M.; Scherer, C.; Schroeder, I.; Irlbeck, M.; Kaeaeb, S.; Massberg, S.; Hausleiter, J.; et al. Left and Right Ventricular Dysfunction in Patients with COVID-19-Associated Myocardial Injury. Infection 2021, 49, 491–500. [Google Scholar] [CrossRef]
- Luchian, M.-L.; Motoc, A.; Lochy, S.; Magne, J.; Belsack, D.; De Mey, J.; Roosens, B.; Van den Bussche, K.; Boeckstaens, S.; Chameleva, H.; et al. Subclinical Myocardial Dysfunction in Patients with Persistent Dyspnea One Year after COVID-19. Diagnostics 2021, 12, 57. [Google Scholar] [CrossRef]
- Karagodin, I.; Singulane, C.C.; Descamps, T.; Woodward, G.M.; Xie, M.; Tucay, E.S.; Sarwar, R.; Vasquez-Ortiz, Z.Y.; Alizadehasl, A.; Monaghan, M.J.; et al. Ventricular Changes in Patients with Acute COVID-19 Infection: Follow-up of the World Alliance Societies of Echocardiography (WASE-COVID) Study. J. Am. Soc. Echocardiogr. 2022, 35, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Surkova, E.; Cosyns, B.; Gerber, B.; Gimelli, A.; La Gerche, A.; Ajmone Marsan, N. The Dysfunctional Right Ventricle: The Importance of Multi-Modality Imaging. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 885–897. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Overall (n = 44) | PE+ (n = 22) | PE− (n = 22) | p-Value |
|---|---|---|---|---|
| Age, years | 58.4 ± 13.3 | 58.7 ± 12.6 | 58 ± 14.3 | 0.859 |
| Male, gender n (%) | 31 (70) | 16 (73) | 15 (68) | 0.741 |
| Body-mass index, kg/m2 | 30.3 ± 6.3 | 30.9 ± 5.4 | 29.8 ± 7.1 | 0.572 |
| Body surface area, m2 | 2.0 ± 0.2 | 2.0 ± 0.2 | 2.0 ± 0.3 | 0.891 |
| Systolic blood pressure, mmHg | 131.7 ± 15.1 | 130.36 ± 17.7 | 133.53 ± 11 | 0.523 |
| Diastolic blood pressure, mmHg | 78.9 ± 10.8 | 77.27 ± 11.72 | 81.18 ± 9.44 | 0.270 |
| Obesity, n (%) | 19 (43) | 11 (50) | 8 (36) | 0.361 |
| Hypertension, n (%) | 29 (66) | 16 (73) | 13 (59) | 0.340 |
| Dyslipidemia, n (%) | 14 (32) | 9 (41) | 5 (23) | 0.195 |
| Diabetes mellitus, n (%) | 7 (16) | 4 (18) | 3 (14) | 0.680 |
Smoking, n (%)
| 0.834 | |||
| 33 (75) | 17 (77) | 16 (73) | ||
| 3 (7) | 1 (4) | 2 (9) | ||
| 8 (18) | 4 (18) | 4 (18) | ||
| Period of hospitalization, days | 24.1 ± 12.5 | 30.2 ± 10.3 | 17.7 ± 11.6 | 0.001 |
| Period of hospitalization in ICU, days | 0.7 ± 3.1 | 1.3 ± 4.3 | 0 | 0.175 |
| Mechanical ventilation, n (%) | 2 (4) | 2 (9) | 0 | 0.175 |
| Hemodynamic support, n (%) | 2 (4) | 2 (9) | 0 | 0.175 |
| Troponin I Hs, ng/mL | 12.9 ± 41.6 | 19.2 ± 53.9 | 3.9 ± 5.1 | 0.412 |
| D-dimer, μg/L | 417 (200–2053) | 620 (293–2898) | 340 (88–1099) | 0.025 |
| C reactive protein, mg/L | 11.3 ± 15.6 | 12.8 ± 19.8 | 9.5 ± 8.3 | 0.524 |
| IL-6 | 187 (40–467) | 279 (159–544) | 50 (29–365) | 0.017 |
| PaO2/FiO2 | 163.9 ± 71.3 | 169.2 ± 78.5 | 150.6 ± 51.0 | 0.569 |
| Lung total severity score | 9.3 ± 3.8 | 10.8 ± 3.1 | 7.3 ± 3.9 | 0.004 |
| Bilateral PE extension | 9 (41%) | |||
| No. of lobes affected by PE | ||||
| - 1 | 13 (59) | |||
| - ≥2 | 9 (41) |
| Variables | Overall (n = 44) | PE+ (n = 22) | PE− (n = 22) | p-Value |
|---|---|---|---|---|
| Interventricular septum, mm | 10.5 ± 1.3 | 10.7 ± 1.12 | 10.3 ± 1.5 | 0.316 |
| LV posterior wall, mm | 9.9 ± 1.3 | 10 ± 1.36 | 9.73 ± 1.32 | 0.435 |
| LV end-diastolic diameter, mm | 46.5 ± 4.6 | 47.3 ± 4.3 | 45.6 ± 4.9 | 0.221 |
| LV end-systolic diameter, mm | 28.6 ± 5.0 | 29.9 ± 5.2 | 27.2 ± 4.6 | 0.113 |
| LV mass indexed, g/m2 | 84.0 ± 20.9 | 87.6 ± 16.9 | 80.4 ± 24.2 | 0.263 |
| Relative wall thickness | 0.41 (0.38–0.46) | 0.40 (0.37–0.48) | 0.43 (0.41–0.46) | 0.444 |
| LV end-diastolic volume, mL | 89.2 ± 26.1 | 87.2 ± 20.3 | 91.2 ± 31.3 | 0.614 |
| LV end-systolic volume, mL | 36.7 ± 13.0 | 36.4 ± 10.7 | 37.1 ± 15.2 | 0.864 |
| LV ejection fraction, % | 60.1 ± 5.3 | 58.9 ± 5.62 | 61.4 ± 4.9 | 0.129 |
| LV GLS, % | 19.6 ± 3.2 | 19.1 ± 3.0 | 20 ± 3.32 | 0.320 |
| Indexed left atrial volume, mL/m2 | 22.5 (20.0–25.3) | 23.5 (19.8–26.1) | 21.7 (20.0–24.5) | 0.647 |
| Mitral E/A ratio, (m ± SD) | 0.88± 0.23 | 0.85 ± 0.28 | 0.90 ± 0.18 | 0.440 |
| Deceleration time, ms (m ± SD) | 231.6 ± 55.3 | 236.2 ± 50.2 | 227.1 ± 60.9 | 0.590 |
| E/e′, average (m ± SD) | 8.0 ± 2.5 | 9.3 ± 2.5 | 7.0 ± 2.0 | 0.015 |
| Variables | Overall (n = 44) | PE+ (n = 22) | PE− (n = 22) | p-Value |
|---|---|---|---|---|
| Indexed right atrial volume, mL/m2 | 16.8 ± 4.5 | 15.8 ± 4.13 | 17.98 ± 4.8 | 0.117 |
| RV basal diameter, mm | 35.1 ± 4.9 | 36.3 ± 5.3 | 34 ± 4.2 | 0.126 |
| RV FAC, % | 48.8 (40.6–54.5) | 50.6 (41.5–57.0) | 47.7 (40.4–54.5) | 0.390 |
| TAPSE, mm | 25.1 ± 4.1 | 25.5 ± 4.4 | 24.7 ± 3.9 | 0.565 |
| RV S′, cm/s | 13 (11–16) | 13 (11–15) | 12 (11–17) | 0.989 |
| Tricuspid valve velocity, m/s | 2.3 (1.9–2.6) | 2.4 (2.1–2.6) | 1.9 (1.8–2.5) | 0.089 |
| Tricuspid regurgitation gradient, mmHg | 22 (25–27) | 23.5 (17.5–27.2) | 15 (14–24) | 0.062 |
| sPAP, mmHg | 30 (23–33) | 32 (24–33) | 27 (23–32) | 0.467 |
| TAPSE/sPAP | 0.90 ± 0.25 | 0.85 ± 0.24 | 0.96 ± 0.26 | 0.308 |
| RV GLS, % | 19.0 ± 4.4 | 16.4 ± 2.9 | 21.6 ± 4.3 | <0.001 |
| RV-FWLS, % | 21.8 ± 5.4 | 18.9 ± 4 | 24.6 ± 5.12 | <0.001 |
| RVOT acceleration time, msec | 102.4 ± 23.3 | 95.9 ± 18.8 | 109.2 ± 26 | 0.074 |
| Main pulmonary artery diameter, mm | 21.9 ± 2.9 | 21.5 ± 2.9 | 22.3 ± 2.9 | 0.448 |
| Parameters | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Pulmonary thromboembolism | 23.8 (3.990–141.963) | 0.001 | 34.961 (3.241–377.091) | 0.003 |
| Obesity | 4.444 (1.118–17.668) | 0.034 | 10.341 (1.052–101.684) | 0.045 |
| Hypertension | 7 (1.277–38.358) | 0.025 | - | - |
| RVOT acceleration time | 0.970 (0.937–1.004) | 0.08 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilardi, F.; Crisci, M.; Calabrese, C.; Scognamiglio, A.; Arenga, F.; Manzo, R.; Mariniello, D.F.; Allocca, V.; Annunziata, A.; D’Andrea, A.; et al. Effects on Right Ventricular Function One Year after COVID-19-Related Pulmonary Embolism. J. Clin. Med. 2023, 12, 3611. https://doi.org/10.3390/jcm12113611
Ilardi F, Crisci M, Calabrese C, Scognamiglio A, Arenga F, Manzo R, Mariniello DF, Allocca V, Annunziata A, D’Andrea A, et al. Effects on Right Ventricular Function One Year after COVID-19-Related Pulmonary Embolism. Journal of Clinical Medicine. 2023; 12(11):3611. https://doi.org/10.3390/jcm12113611
Chicago/Turabian StyleIlardi, Federica, Mario Crisci, Cecilia Calabrese, Anna Scognamiglio, Fortunato Arenga, Rachele Manzo, Domenica F. Mariniello, Valentino Allocca, Anna Annunziata, Antonello D’Andrea, and et al. 2023. "Effects on Right Ventricular Function One Year after COVID-19-Related Pulmonary Embolism" Journal of Clinical Medicine 12, no. 11: 3611. https://doi.org/10.3390/jcm12113611