

Reporting of Drug-Induced Myopathies Associated with the Combination of Statins and Daptomycin: A Disproportionality Analysis Using the US Food and Drug Administration Adverse Event Reporting System


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source, Extraction, and Processing
2.2. Statistical Analysis
3. Results
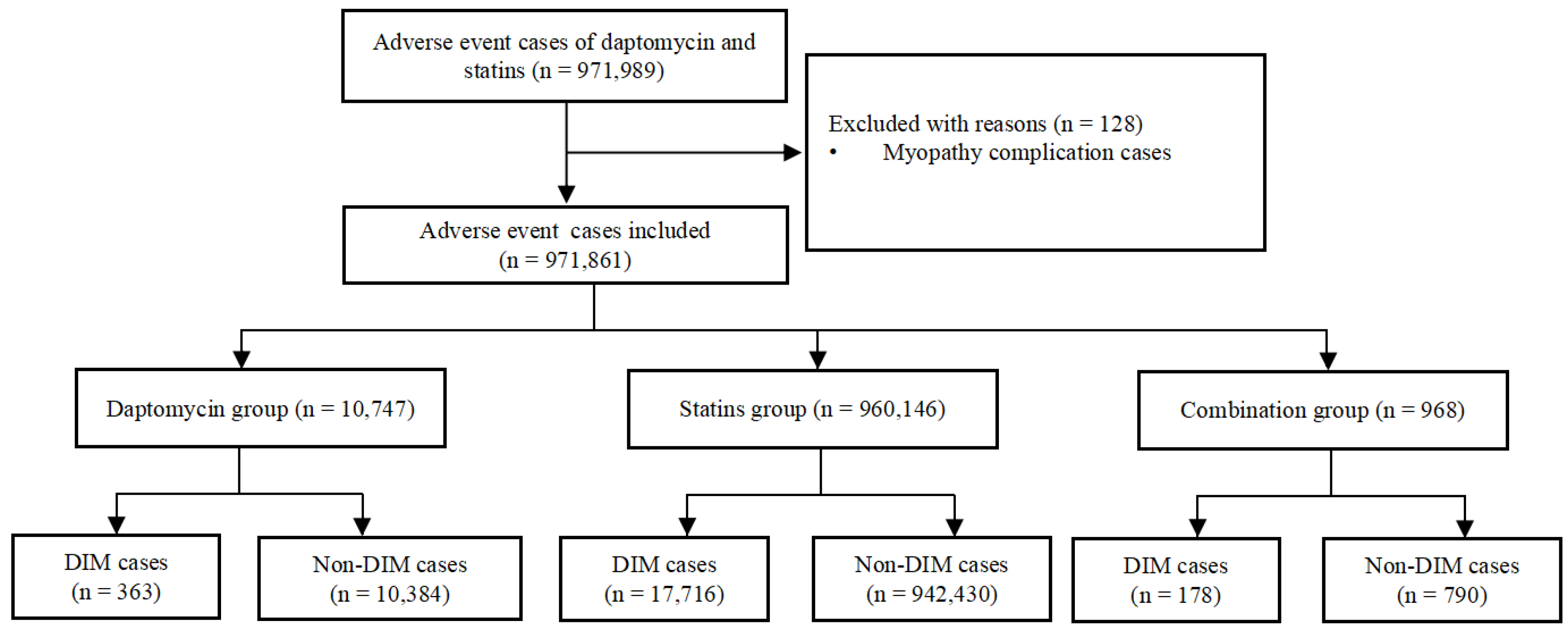
3.1. DIM Event Identification in the FAERS Database
3.2. Demographic Characteristics
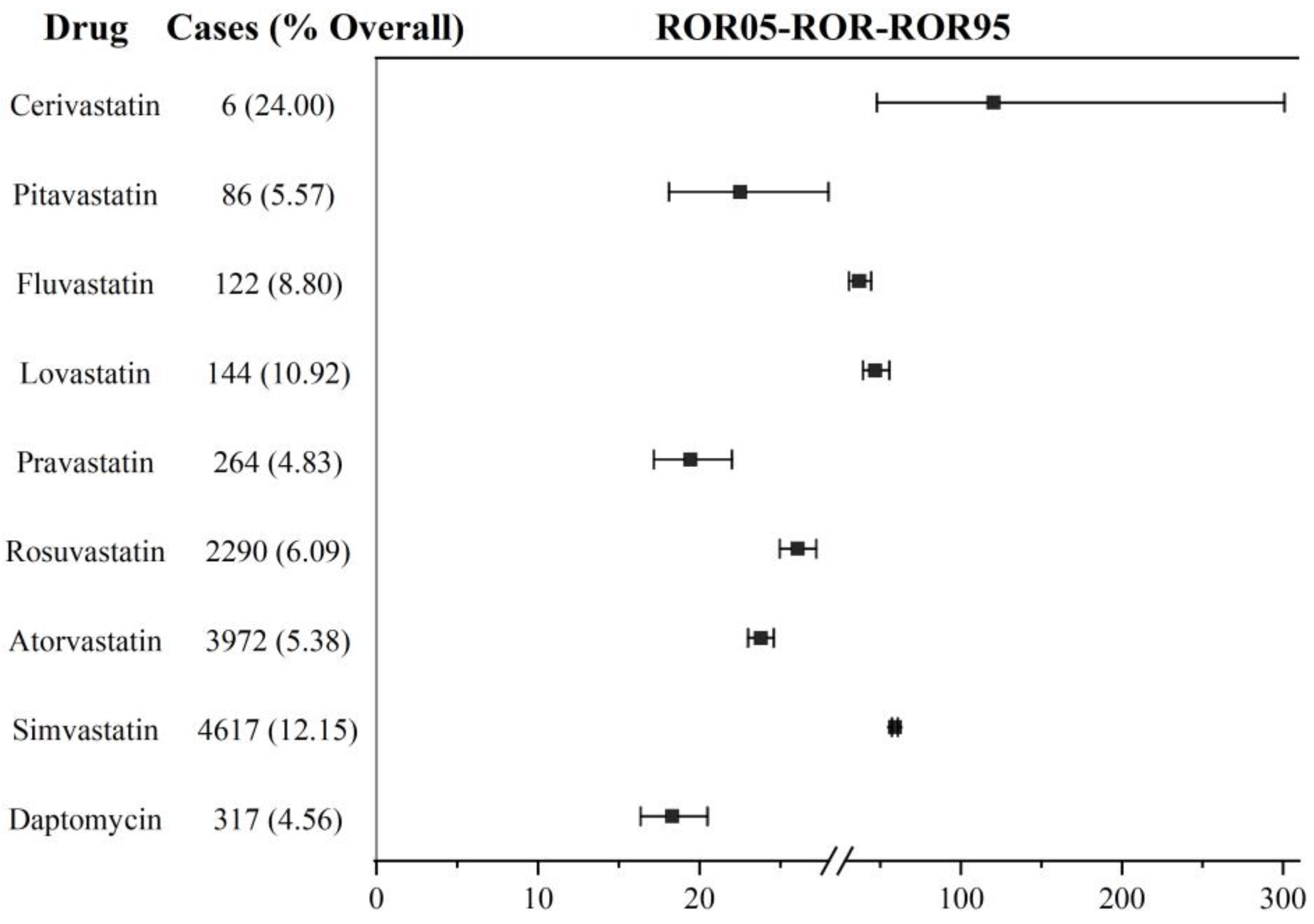
3.3. DIM Signal Detection in Daptomycin and Statins Based on the Primary Suspect
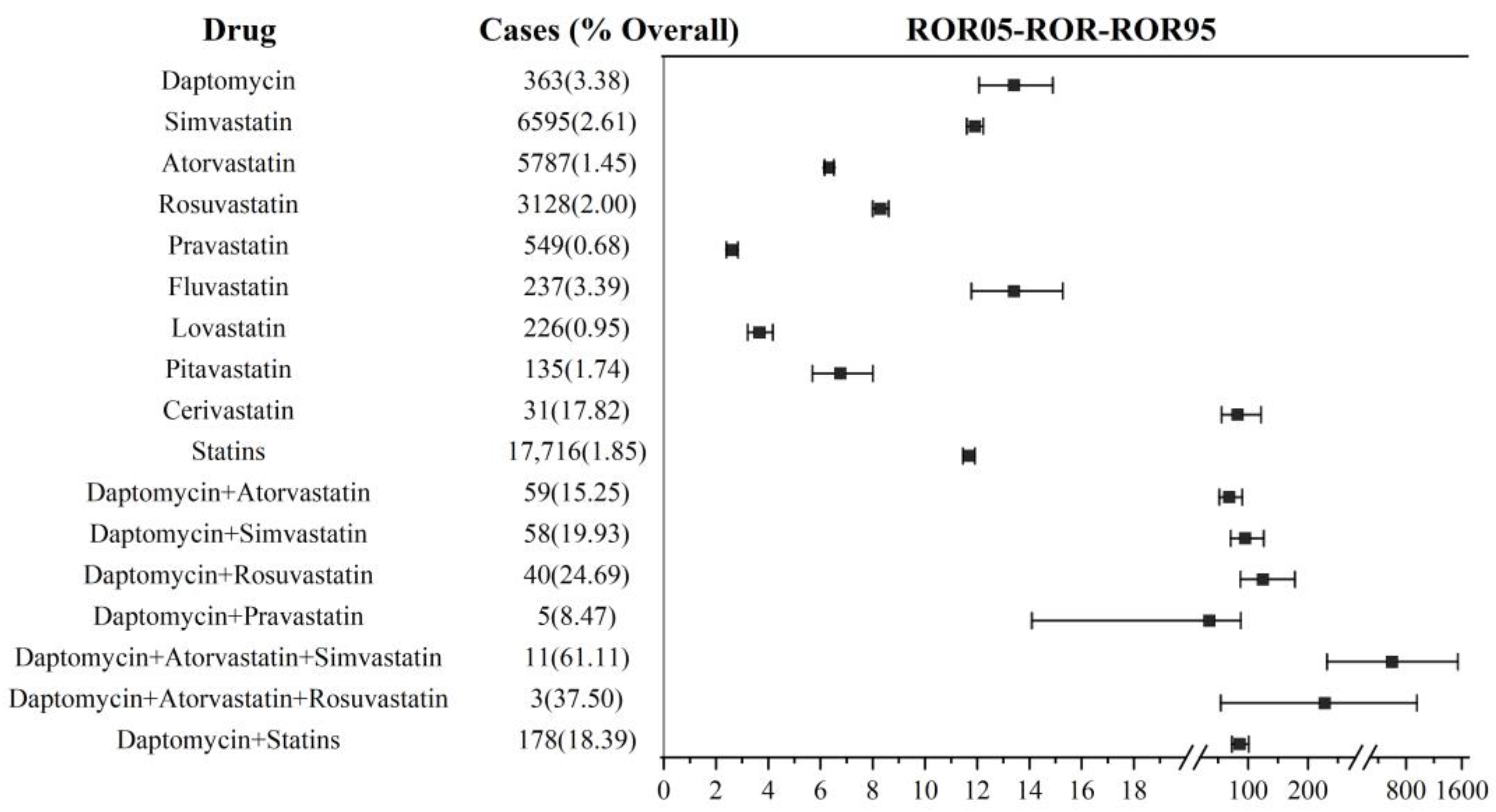
3.4. DIM Signal Detection in Daptomycin and Statin Co-Administration
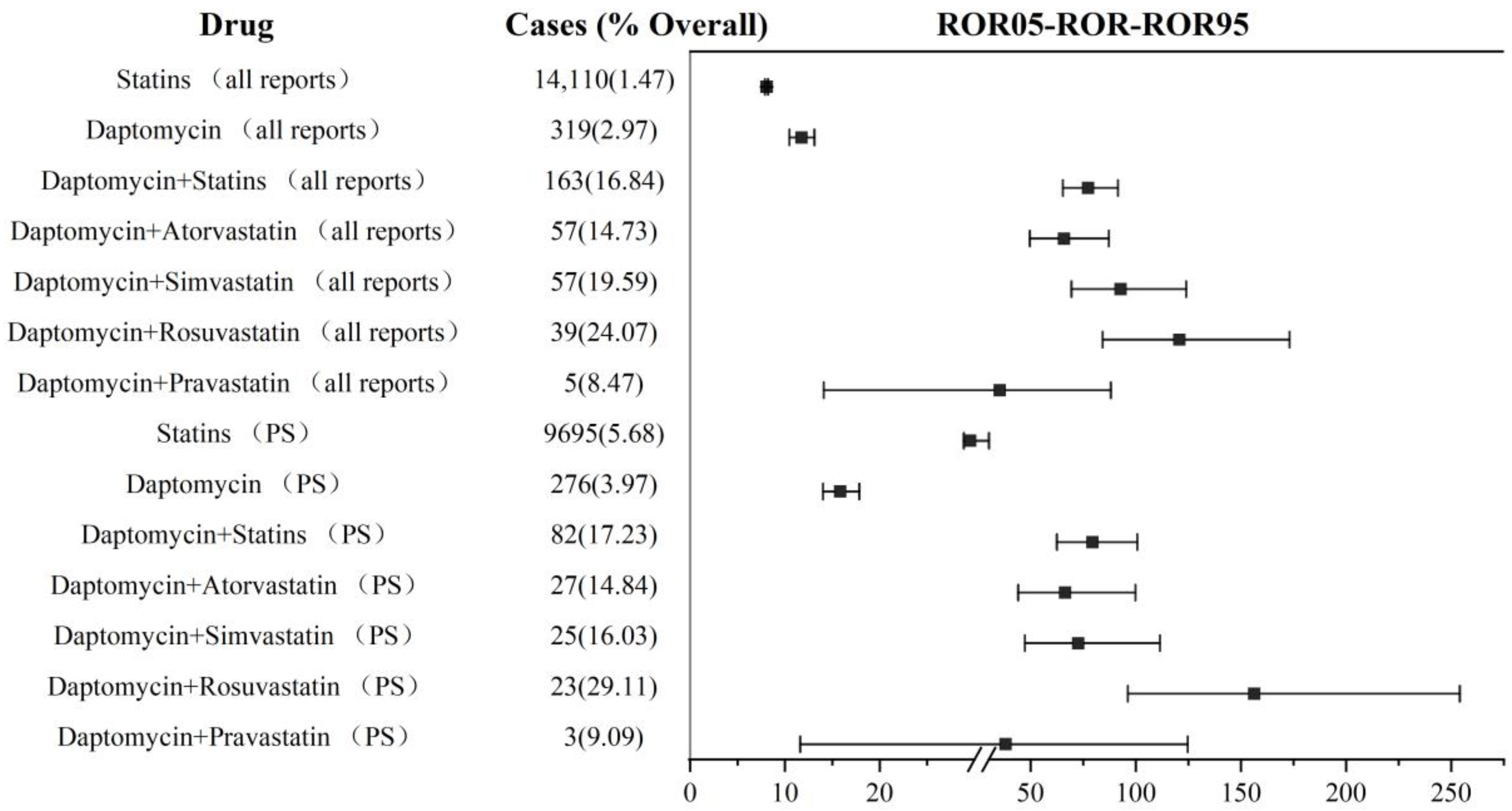
3.5. Rhabdomyolysis in Daptomycin and Statin Co-Administration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guemara, R.; Lazarou, I.; Guerne, I.A. Drug-induced myopathies. Rev. Med. Suisse 2017, 562, 1013–1017. [Google Scholar]
- Mastaglia, F.L. The changing spectrum of drug-induced myopathies. Acta Myol. 2020, 4, 283–288. [Google Scholar]
- Curry, S.C.; Chang, D.; Connor, D. Drug- and toxin-induced rhabdomyolysis. Ann. Emerg. Med. 1989, 10, 1068–1084. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.M.; De Carvalho, J.F. Glucocorticoid-induced myopathy. Jt. Bone Spine 2011, 1, 41–44. [Google Scholar] [CrossRef]
- Wu, K.; Michalski, A.; Cortes, D.; Rozenberg, D.; Mathur, S. Glucocorticoid-induced myopathy in people with asthma: A systematic review. J. Asthma 2022, 7, 1396–1409. [Google Scholar] [CrossRef]
- Abd, T.T.; Jacobson, T.A. Statin-induced myopathy: A review and update. Expert Opin. Drug Saf. 2011, 3, 373–387. [Google Scholar] [CrossRef]
- Lane, R.J.; Mastaglia, F.L. Drug-induced myopathies in man. Lancet 1978, 8089, 562–566. [Google Scholar] [CrossRef]
- Sieb, J.P.; Gillessen, T. Iatrogenic and toxic myopathies. Muscle Nerve 2003, 2, 142–156. [Google Scholar] [CrossRef]
- Dalakas, M.C. Toxic and drug-induced myopathies. J. Neurol. Neurosurg. Psychiatry 2009, 8, 832–838. [Google Scholar] [CrossRef]
- Saliba, W.R.; Elias, M. Myopathy from the combination of simvastatin and amiodarone. Eur. J. Intern. Med. 2006, 2, 148. [Google Scholar] [CrossRef]
- Roth, R.F.; Itabashi, H.; Louie, J.; Anderson, T.; Narahara, K.A. Amiodarone toxicity: Myopathy and neuropathy. Am. Heart J. 1990, 5, 1223–1225. [Google Scholar] [CrossRef] [PubMed]
- Humphries, R.M.; Pollett, S.; Sakoulas, G. A current perspective on daptomycin for the clinical microbiologist. Clin. Microbiol. Rev. 2013, 4, 759–780. [Google Scholar] [CrossRef] [PubMed]
- Araos, R.; García, P.; Chanqueo, L.; Labarca, J. Daptomycin: Pharmacological characteristics and its role in the treatment of gram positive infections. Rev. Chil. Infectol. 2012, 2, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Huo, X.C.; Wang, S.X.; Wang, F.; Zhao, Q. Data mining for adverse drug reaction signals of daptomycin based on real-world data: A disproportionality analysis of the US Food and Drug Administration adverse event reporting system. Int. J. Clin. Pharm. 2022, 6, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Dare, R.K.; Tewell, C.; Harris, B.; Wright, P.W.; Driest, S.V.; Farber-Eger, E.; Nelson, G.E.; Talbot, T.R. Effect of Statin Coadministration on the Risk of Daptomycin-Associated Myopathy. Clin. Infect. Dis. 2018, 9, 1356–1363. [Google Scholar] [CrossRef]
- Dvorchik, B.H.; Brazier, D.; Debruin, M.F.; Arbeit, R.D. Daptomycin pharmacokinetics and safety following administration of escalating doses once daily to healthy subjects. Antimicrob. Agents Chemother. 2003, 4, 1318–1323. [Google Scholar] [CrossRef]
- Papadopoulos, S.; Ball, A.M.; Liewer, S.E.; Martin, C.A.; Winstead, P.S.; Murphy, B.S. Rhabdomyolysis during therapy with daptomycin. Clin. Infect. Dis. 2006, 12, e108–e110. [Google Scholar] [CrossRef]
- Katz, D.E.; Lindfield, K.C.; Steenbergen, J.N.; Benziger, D.P.; Blackerby, K.J.; Knapp, A.G.; Martone, W.J. A pilot study of high-dose short duration daptomycin for the treatment of patients with complicated skin and skin structure infections caused by gram-positive bacteria. Int. J. Clin. Pract. 2008, 9, 1455–1464. [Google Scholar] [CrossRef]
- Pertel, P.E.; Eisenstein, B.I.; Link, A.S.; Donfrid, B.; Biermann, E.J.A.; Bernardo, P.; Martone, W.J. The efficacy and safety of daptomycin vs. vancomycin for the treatment of cellulitis and erysipelas. Int. J. Clin. Pract. 2009, 3, 368–375. [Google Scholar] [CrossRef]
- Tai, C.H.; Shao, C.H.; Chen, C.Y.; Lin, S.W.; Wu, C.C. Safety of high-dose daptomycin in patients with severe renal impairment. Ther. Clin. Risk Manag. 2018, 14, 493–499. [Google Scholar] [CrossRef]
- Pai, M.P.; Norenberg, J.P.; Anderson, T.; Goade, D.W.; Rodvold, K.A.; Telepak, R.A.; Mercier, R. Influence of morbid obesity on the single-dose pharmacokinetics of daptomycin. Antimicrob. Agents Chemother. 2007, 8, 2741–2747. [Google Scholar] [CrossRef] [PubMed]
- Bookstaver, P.B.; Bland, C.M.; Qureshi, Z.P.; Faulkner-Fennell, C.M.; Sheldon, M.A.; Caulder, C.R.; Hartis, C.; Investigators, S. Safety and effectiveness of daptomycin across a hospitalized obese population: Results of a multicenter investigation in the southeastern United States. Pharmacotherapy 2013, 12, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.N.; Smith, W.J.; Kupiec, K.E.; Harding, S.J.; Resman-Targoff, B.H.; Neely, S.B.; White, B.P.; Owens, R.E. Daptomycin dosing in obese patients: Analysis of the use of adjusted body weight versus actual body weight. Ther. Adv. Infect. Dis. 2019, 6, 2049936118820230. [Google Scholar] [CrossRef] [PubMed]
- Kido, K.; Oyen, A.A.; Beckmann, M.A.; Brouse, S.D. Musculoskeletal toxicities in patients receiving concomitant statin and daptomycin therapy. Am. J. Health Syst. Pharm. 2019, 4, 206–210. [Google Scholar] [CrossRef]
- Lehman, B.; Neuner, E.A.; Heh, V.; Isada, C. A Retrospective Multisite Case-Control Series of Concomitant Use of Daptomycin and Statins and the Effect on Creatine Phosphokinase. Open Forum Infect. Dis. 2019, 11, ofz444. [Google Scholar] [CrossRef] [PubMed]
- Bland, C.M.; Bookstaver, P.B.; Lu, Z.K.; Dunn, B.L.; Rumley, K.F. SERGE-45 Musculoskeletal safety outcomes of patients receiving daptomycin with HMG-CoA reductase inhibitors. Antimicrob. Agents Chemother. 2014, 10, 5726–5731. [Google Scholar] [CrossRef]
- Berg, M.L.; Estes, L.L.; Dierkhising, R.A.; Curran, B.; Enzler, M.J. Evaluation of impact of statin use on development of CPK elevation during daptomycin therapy. Ann. Pharmacother. 2014, 3, 320–327. [Google Scholar] [CrossRef]
- Tian, X.; Chen, L.; Gai, D.; He, S.; Jiang, X.; Zhang, N. Adverse Event Profiles of PARP Inhibitors: Analysis of Spontaneous Reports Submitted to FAERS. Front. Pharmacol. 2022, 13, 851246. [Google Scholar] [CrossRef]
- Wu, B.; Luo, M.; Wu, F.; He, Z.; Li, Y.; Xu, T. Acute Kidney Injury Associated with Remdesivir: A Comprehensive Pharmacovigilance Analysis of COVID-19 Reports in FAERS. Front. Pharmacol. 2022, 13, 692828. [Google Scholar] [CrossRef]
- Wu, B.; Hu, Q.; Tian, F.; Wu, F.; Li, Y.; Xu, T. A pharmacovigilance study of association between proton pump inhibitor and dementia event based on FDA adverse event reporting system data. Sci. Rep. 2021, 1, 10709. [Google Scholar] [CrossRef]
- Wu, L.; Ingle, T.; Liu, Z.; Wong, Z.A.; Harris, S.; Thakkar, S.; Zhou, G.; Yang, J.; Xu, J.; Mehta, D.; et al. Study of serious adverse drug reactions using FDA-approved drug labeling and MedDRA. BMC Bioinform. 2019, 20 (Suppl. 2), 97. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Xia, J.; Deng, J.; Jiang, J. A comparison of measures of disproportionality for signal detection on adverse drug reaction spontaneous reporting database of Guangdong province in China. Pharmacoepidemiol. Drug Saf. 2008, 6, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Zhang, J.; Yin, W.; Jiang, A.; Liu, Y.; Wu, B. A real-world pharmacovigilance study of severe cutaneous adverse reactions associated with antiepileptic drug combination therapy: Data mining of FDA adverse event reporting system. Expert Opin. Drug Saf. 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gluba-Brzozka, A.; Franczyk, B.; Toth, P.P.; Rysz, J.; Banach, M. Molecular mechanisms of statin intolerance. Arch. Med. Sci. 2016, 3, 645–658. [Google Scholar] [CrossRef]
- Ramachandran, R.; Wierzbicki, A.S. Statins, Muscle Disease and Mitochondria. J. Clin. Med. 2017, 6, 75. [Google Scholar] [CrossRef]
- Banach, M.; Stulc, T.; Dent, R.; Toch, P.P. Statin non-adherence and residual cardiovascular risk: There is need for substantial improvement. Int. J. Cardiol. 2016, 225, 184–196. [Google Scholar] [CrossRef]
- Dong, X.M.; Xu, N.N.; Yao, Y.Y.; Guan, Y.Y.; Li, Q.Y.; Zheng, F.; Chen, F.Z.; Wang, G. The Efficacy and Safety of High-dose Daptomycin in the Treatment of Complicated Skin and Soft Tissue Infections in Asians. Int. J. Infect. Dis. 2020, 95, 38–43. [Google Scholar] [CrossRef]
- Parra-Ruiz, J.; Dueñas-Gutiérrez, C.; Tomás-Jiménez, C.; Linares-Palomino, J.P.; Garrido-Gomez, J.; Hernández-Quero, J. Safety analysis of high dose (>6 mg/kg/day) daptomycin in patients with concomitant statin therapy. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 8, 1771–1774. [Google Scholar] [CrossRef]
- Chuma, M.; Nakamoto, A.; Bando, T.; Niimura, T.; Kondo, Y.; Hamano, H.; Okada, N.; Asada, M.; Zamami, Y.; Takechi, K.; et al. Association Between Statin Use and Daptomycin-related Musculoskeletal Adverse Events: A Mixed Approach Combining a Meta-analysis and a Disproportionality Analysis. Clin. Infect. Dis. 2022, 8, 1416–1422. [Google Scholar] [CrossRef]
- Yamada, T.; Mitsuboshi, S.; Suzuki, K.; Nishihara, M.; Uchiyama, K. Risk of muscle toxicity events for daptomycin with and without statins: Analysis of the Japanese Adverse Event Report database. Basic Clin. Pharmacol. Toxicol. 2021, 3, 268–272. [Google Scholar] [CrossRef]
- Skilving, I.; Eriksson, M.; Rane, A.; Ovesjö, M.L. Statin-induced myopathy in a usual care setting-a prospective observational study of gender differences. Eur. J. Clin. Pharmacol. 2016, 10, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Barilla, D.; Prasad, P.; Hubert, M.; Gumbhir-Shah, K. Steady-state pharmacokinetics of fluvastatin in healthy subjects following a new extended release fluvastatin tablet, Lescol XL. Biopharm. Drug Dispos. 2004, 2, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Catapano, A.L. Statin-induced myotoxicity: Pharmacokinetic differences among statins and the risk of rhabdomyolysis, with particular reference to pitavastatin. Curr. Vasc. Pharmacol. 2012, 2, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, M.A.; Keech, A.; Sacks, F.M.; Cobbe, S.M.; Tonkin, A.; Byington, R.P.; Davis, B.R.; Friedman, C.P.; Braunwald, E. Safety and tolerability of pravastatin in long-term clinical trials: Prospective Pravastatin Pooling (PPP) Project. Circulation 2002, 20, 2341–2346. [Google Scholar] [CrossRef]
- Diaconu, C.C.; Iorga, R.A.; Furtunescu, F.; Katsiki, N.; Stoian, A.P.; Rizzo, M. Statin intolerance: New data and further options for treatment. Curr. Opin. Cardiol. 2021, 4, 487–493. [Google Scholar] [CrossRef]
- Karlson, B.W.; Palmer, M.K.; Nicholls, S.J.; Lundman, P.; Barter, P.J. Doses of rosuvastatin, atorvastatin and simvastatin that induce equal reductions in LDL-C and non-HDL-C: Results from the VOYAGER meta-analysis. Eur. J. Prev. Cardiol. 2016, 7, 744–747. [Google Scholar] [CrossRef]
- Jones, P.H.; Davidson, M.H.; Stein, E.A.; Bays, H.E.; Mckenney, J.M.; Miller, E.; Cain, V.A.; Blasetto, J.W.; STELLAR Study Group. Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR* Trial). Am. J. Cardiol. 2003, 2, 152–160. [Google Scholar] [CrossRef]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 21, 2195–2207. [Google Scholar] [CrossRef]
- Hodel, C. Myopathy and rhabdomyolysis with lipid-lowering drugs. Toxicol. Lett. 2002, 1–3, 159–168. [Google Scholar] [CrossRef]
- Cabral, B.M.I.; Edding, S.N.; Portocarrero, J.P.; Lerma, E.V. Rhabdomyolysis. Dis. Mon. 2020, 8, 101015. [Google Scholar] [CrossRef]
- Chatzizisis, Y.S.; Misirli, G.; Hatzitolios, A.I.; Giannoglou, G.D. The syndrome of rhabdomyolysis: Complications and treatment. Eur. J. Intern. Med. 2008, 8, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Vinci, P.; Panizon, E.; Tosoni, L.M.; Cerrato, C.; Pellicori, F.; Mearelli, F.; Biasinutto, C.; Fiotti, N.; Girolamo, F.G.D.; Biolo, G. Statin-Associated Myopathy: Emphasis on Mechanisms and Targeted Therapy. Int. J. Mol. Sci. 2021, 22, 11687. [Google Scholar] [CrossRef] [PubMed]
- Phillips, P.S.; Haas, R.H.; Bannykh, S.; Hathaway, S.; Gray, N.L.; Kimura, B.J.; Vladutiu, G.D.; England, J.D.F. Scripps Mercy Clinical Research Center Statin-associated myopathy with normal creatine kinase levels. Ann. Intern. Med. 2002, 7, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, K.; Kimura, J. Mechanism of statin-induced rhabdomyolysis. J. Pharmacol. Sci. 2013, 4, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Sakai, Y.; Murakami, E.; Kato, H.; Ohyama, K.; Esaka, Y.; Yamamoto, T.; Hagihara, M.; Mikamo, H.; Uno, B. Feasibility of Trypsin Digestion as a Sample Preparation for Daptomycin Quantification in Murine Skeletal Muscles. Biol. Pharm. Bull. 2019, 5, 751–757. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DIM Group | Non-DIM Group | Total | |||
|---|---|---|---|---|---|
| Number (n) | Proportion (%) | Number (n) | Proportion (%) | Number (n) | |
| Gender | |||||
| Female | 6495 | 35.58 | 462,610 | 48.51 | 469,105 |
| Male | 10,164 | 55.67 | 435,023 | 45.62 | 445,187 |
| Unknown | 1598 | 8.75 | 55,971 | 5.87 | 57,569 |
| Age (year) | |||||
| <18 | 55 | 0.30 | 1532 | 0.16 | 1587 |
| 18–65 | 6060 | 33.19 | 288,139 | 30.22 | 294,199 |
| ≥65 | 8883 | 48.66 | 420,630 | 44.11 | 429,513 |
| Unknown | 3259 | 17.85 | 243,303 | 25.51 | 246,562 |
| Identity of reporter | |||||
| Health professional | 15,128 | 82.86 | 488,562 | 51.23 | 503,690 |
| Non-health professional | 1709 | 9.36 | 388,956 | 40.79 | 390,665 |
| Unknown | 1420 | 7.78 | 76,086 | 7.98 | 77,506 |
| Europe | 7684 | 42.09 | 214,147 | 22.46 | 221,831 |
| North America | 6640 | 36.37 | 613,283 | 64.31 | 619,923 |
| Asian | 1497 | 8.20 | 38,068 | 3.99 | 39,565 |
| Oceania | 509 | 2.79 | 8806 | 0.92 | 9315 |
| South America | 77 | 0.42 | 18,802 | 1.97 | 18,879 |
| Africa | 33 | 0.18 | 2712 | 0.28 | 2745 |
| Unknown | 1817 | 9.95 | 57,786 | 6.06 | 59,603 |
| Report year | |||||
| 2004–2008 | 4470 | 24.48 | 101,399 | 10.64 | 105,869 |
| 2009–2013 | 4665 | 25.55 | 211,535 | 22.18 | 216,200 |
| 2014–2018 | 4195 | 22.98 | 336,073 | 35.24 | 340,268 |
| 2019–2022 | 4927 | 26.99 | 304,597 | 31.94 | 309,524 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, C.; Yin, W.; He, Z.; Wu, B. Reporting of Drug-Induced Myopathies Associated with the Combination of Statins and Daptomycin: A Disproportionality Analysis Using the US Food and Drug Administration Adverse Event Reporting System. J. Clin. Med. 2023, 12, 3548. https://doi.org/10.3390/jcm12103548
Wei C, Yin W, He Z, Wu B. Reporting of Drug-Induced Myopathies Associated with the Combination of Statins and Daptomycin: A Disproportionality Analysis Using the US Food and Drug Administration Adverse Event Reporting System. Journal of Clinical Medicine. 2023; 12(10):3548. https://doi.org/10.3390/jcm12103548
Chicago/Turabian StyleWei, Chunyan, Wanhong Yin, Zhiyao He, and Bin Wu. 2023. "Reporting of Drug-Induced Myopathies Associated with the Combination of Statins and Daptomycin: A Disproportionality Analysis Using the US Food and Drug Administration Adverse Event Reporting System" Journal of Clinical Medicine 12, no. 10: 3548. https://doi.org/10.3390/jcm12103548