
Getting It Right in Restrictive Lung Disease
Abstract
:1. Introduction
A Typical Patient’s Clinical Journey
2. Methods: Literature Review
3. Results
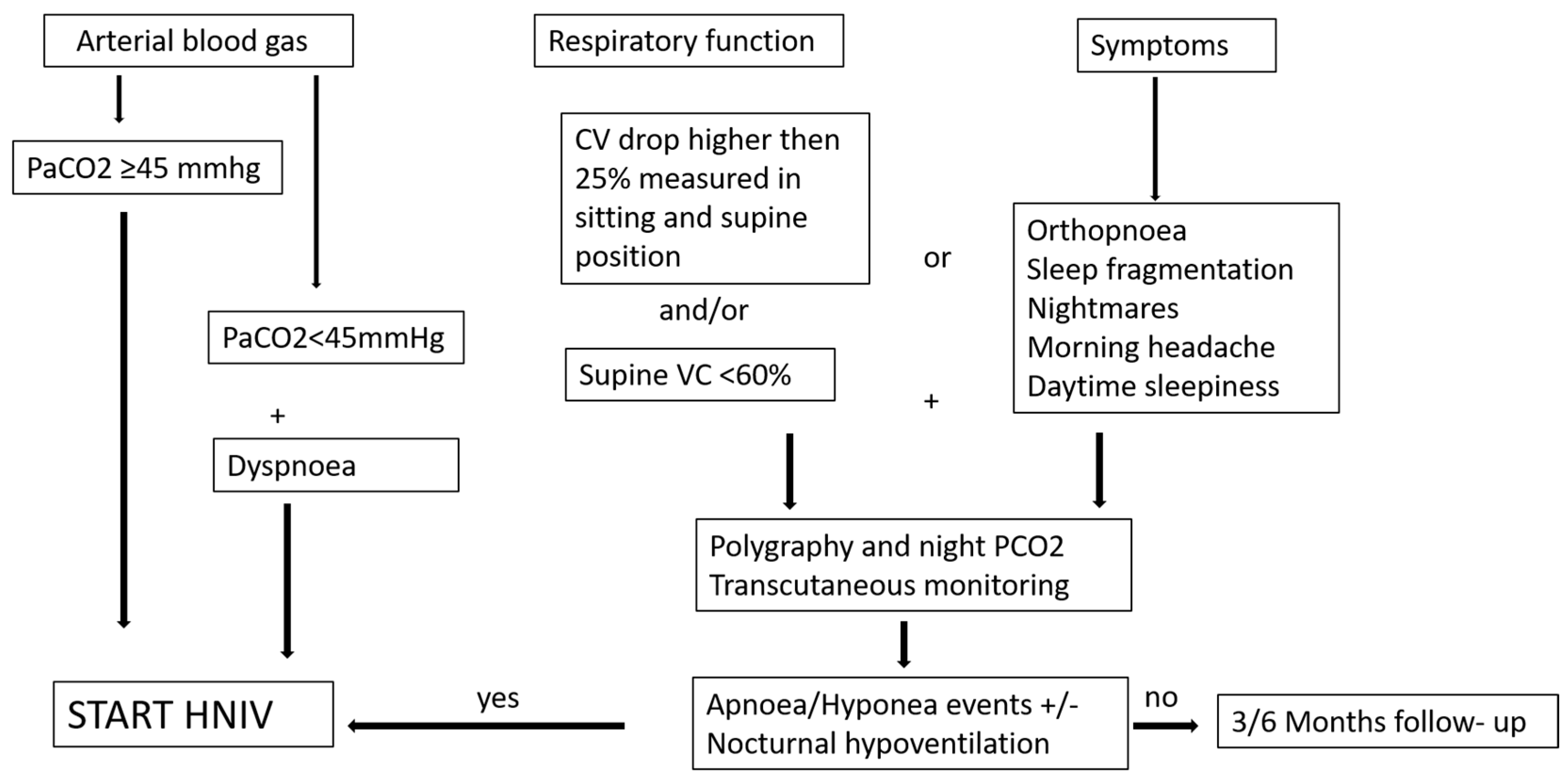
3.1. When Is the Right Time to Start Home NIV?
3.2. Back to Our Patient Case and Their Journey
3.3. How to Ventilate: Settings and Objective Measures of Successful Ventilation
3.4. How to Set a Ventilator
3.5. Mouth-Piece Ventilation (MPV)
3.6. Beyond HNIV
4. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Crimi, C.; Pierucci, P.; Carlucci, A.; Cortegiani, A.; Gregoretti, C. Long-Term Ventilation in Neuromuscular Patients: Review of Concerns, Beliefs, and Ethical Dilemmas. Respiration 2019, 97, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Bergosky, E.H. Respiratory failure in disorders of the thoracic cage. Am. Rev. Respir. Dis. 1979, 119, 643–669. [Google Scholar]
- Annane, D.; Orlikowski, D.; Chevret, S. Nocturnal mechanical ventilation for chronic hypoventilation in patients with neuromuscular and chest wall disorders. Cochrane Database Syst. Rev. 2014, 13, CD001941. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, T.; Franklin, K.A.; Midgren, B.; Pehrsson, K.; Ranstam, J.; Ström, K. Survival of patients with kyphoscoliosis receiving mechanical ventilation or oxygen at home. Chest 2006, 130, 1828–1833. [Google Scholar] [CrossRef]
- Wolfe, L.F.; Benditt, J.O.; Aboussouan, L.; Hess, D.R.; Coleman, J.M., III; ONMAP Technical Expert Panel. Optimal NIV Medicare Access Promotion: Patients with Thoracic Restrictive Disorders: A Technical Expert Panel Report From the American College of Chest Physicians, the American Association for Respiratory Care, the American Academy of Sleep Medicine, and the American Thoracic Society. Chest 2021, 160, e399–e408. [Google Scholar] [CrossRef]
- Raphael, J.C.; Chevret, S.; Chastang, C.; Bouvet, F. Randomised trial of preventive nasal ventilation in Duchenne muscular dystrophy. French Multicentre Cooperative Group on Home Mechanical Ventilation Assistance in Duchenne de Boulogne Muscular Dystrophy. Lancet 1994, 343, 1600–1604. [Google Scholar] [CrossRef]
- Jacobs, T.L.; Brown, D.L.; Baek, J.; Migda, E.M.; Funckes, T.; Gruis, K.L. Trial of early noninvasive ventilation for ALS: A pilot placebocontrolled study. Neurology 2016, 87, 1878–1883. [Google Scholar] [CrossRef]
- Ward, S.; Chatwin, M.; Heather, S.; Simonds, A.K. Randomised controlled trial of non-invasive ventilation (NIV) for nocturnal hypoventilation in neuromuscular and chest wall disease patients with daytime normocapnia. Thorax 2005, 60, 1019–1024. [Google Scholar] [CrossRef]
- Ragette, R.; Mellies, U.; Schwake, C.; Voit, T.; Teschler, H. Patterns and predictors of sleep disordered breathing in primary myopathies. Thorax 2002, 57, 724–728. [Google Scholar] [CrossRef]
- Fromageot, C.; Lofaso, F.; Annane, D.; Falaize, L.; Lejaille, M.; Clair, B.; Gajdos, P.; Raphaël, J.C. Supine fall in lung volumes in the assessment of diaphragmatic weakness in neuromuscular disorders. Arch. Phys. Med. Rehabil. 2001, 82, 123–128. [Google Scholar] [CrossRef]
- Morelot-Panzini, C.; Bruneteau, G.; Gonzalez-Bermejo, J. NIV in amyotrophic lateral sclerosis: The ‘when’ and ‘how’ of the matter. Respirology 2019, 24, 521–530. [Google Scholar] [CrossRef]
- Gonzalez-Bermejo, J.; Morelot-Panzini, C.; Arnol, N.; Meininger, V.; Kraoua, S.; Salachas, F.; Similowski, T. Prognostic value of efficiently correcting nocturnal desaturations after one month of noninvasive ventilation in amyotrophic lateral sclerosis: A retrospective monocentre observational cohort study. Amyotroph. Lateral Scler. Front. Degener. 2013, 14, 373–379. [Google Scholar] [CrossRef]
- Ogna, A.; Quera Salva, M.A.; Prigent, H.; Mroue, G.; Vaugier, I.; Annane, D.; Lofaso, F.; Orlikowski, D. Nocturnal hypoventilation in neuromuscular disease: Prevalence according to different definitions issued from the literature. Sleep Breath. 2016, 20, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef]
- Orlikowski, D.; Prigent, H.; Quera Salva, M.A.; Heming, N.; Chaffaut, C.; Chevret, S.; Annane, D.; Lofaso, F.; Ogna, A. Prognostic value of nocturnal hypoventilation in neuromuscular patients. Neuromuscul. Disord. 2017, 27, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Lanini, B.; Misuri, G.; Gigliotti, F.; Iandelli, I.; Pizzi, A.; Romagnoli, I.; Scano, G. Perception of dyspnea in patients with neuromuscular disease. Chest 2001, 120, 402–408. [Google Scholar] [CrossRef]
- Gonzalez-Bermejo, J.; Perrin, C.; Janssens, J.P.; Pepin, J.L.; Mroue, G.; Léger, P.; Langevin, B.; Rouault, S.; Rabec, C.; Rodenstein, D.; et al. Proposal for a systematic analysis of polygraphy or polysomnography for identifying and scoring abnormal events occurring during non-invasive ventilation. Thorax 2012, 67, 546–552. [Google Scholar] [CrossRef]
- Pierucci, P.; Crimi, C.; Carlucci, A.; Carpagnano, G.E.; Janssens, J.P.; Lujan, M.; Noto, A.; Wijkstra, P.J.; Windisch, W.; Scala, R. REINVENT: ERS International survey on REstrictive thoracic diseases IN long term home noninvasive VENTilation. ERJ Open Res. 2021, 7, 00911–02020. [Google Scholar] [CrossRef] [PubMed]
- Arellano-Maric, M.P.; Gregoretti, C.; Duiverman, M.; Windisch, W. Long-term volume-targeted pressure-controlled ventilation: Sense or nonsense? Eur. Respir. J. 2017, 49, 1602193. [Google Scholar] [CrossRef]
- Sancho, J.; Servera, E.; Morelot-Panzini, C.; Salachas, F.; Similowski, T.; Gonzalez-Bermejo, J. Non-invasive ventilation effectiveness and the effect of ventilatory mode on survival in ALS patients. Amyotroph. Lateral Scler. Front. Degener. 2014, 15, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Carlucci, A.; Schreiber, A.; Mattei, A.; Malovini, A.; Bellinati, J.; Ceriana, P.; Gregoretti, C. The configuration of bi-level ventilator circuits may affect compensation for non-intentional leaks during volume targeted ventilation. Intensive Care Med. 2013, 39, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Georges, M.; Rabec, C.; Monin, E.; Aho, S.; Beltramo, G.; Janssens, J.P.; Bonniaud, P. Monitoring of noninvasive ventilation: Comparative analysis of different strategies. Respir. Res. 2020, 21, 324. [Google Scholar] [CrossRef] [PubMed]
- Ogna, A.; Nardi, J.; Prigent, H.; Quera Salva, M.A.; Chaffaut, C.; Lamothe, L.; Chevret, S.; Annane, D.; Orlikowski, D.; Lofaso, F. Prognostic Value of Initial Assessment of Residual Hypoventilation Using Nocturnal Capnography in Mechanically Ventilated Neuromuscular Patients: A 5-Year Follow-up Study. Front. Med. 2016, 3, 40. [Google Scholar] [CrossRef] [PubMed]
- Léotard, A.; Delorme, M.; Hartley, S.; Khouri, C.; Lebret, M.; Lofaso, F.; Pepin, J.L.; Borel, J.C. Non-invasive ventilation in neuromuscular diseases: Should we use higher levels of ventilatory support? Sleep Breath. 2022, 20. [Google Scholar] [CrossRef]
- Gonzalez-Bermejo, J.; Janssens, J.P.; Rabec, C.; Perrin, C.; Lofaso, F.; Langevin, B.; Carlucci, A.; Lujan, M.; SomnoNIV group. Framework for patient-ventilator asynchrony during long-term non-invasive ventilation. Thorax 2019, 74, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Janssens, J.P.; Cantero, C.; Pasquina, P.; Georges, M.; Rabec, C. Monitoring Long Term Noninvasive Ventilation: Benefits, Caveats and Perspectives. Front. Med. 2022, 9, 874523. [Google Scholar] [CrossRef]
- Sayas Catalán, J.; Jiménez Huerta, I.; Benavides Mañas, P.; Luján, M.; López-Padilla, D.; Arias Arias, E.; Hernández Voth, A.; Rabec, C. Videolaryngoscopy with Noninvasive Ventilation in Subjects with Upper-Airway Obstruction. Respir. Care 2017, 62, 222–230. [Google Scholar] [CrossRef]
- Vrijsen, B.; Buyse, B.; Belge, C.; Vanpee, G.; Van Damme, P.; Testelmans, D. Randomized cross-over trial of ventilator modes during non-invasive ventilation titration in amyotrophic lateral sclerosis. Respirology 2021, 22, 1212–1218. [Google Scholar] [CrossRef]
- Toussaint, M.; Chatwin, M.; Gonzalez, J.; Berlowitz, D.J.; the ENMC Respiratory Therapy Consortium. Airway clearance techniques in neuromuscular disorders. Neuromuscul. Disord. 2018, 28, 289–298. [Google Scholar] [CrossRef]
- Carlucci, A.; Mattei, A.; Rossi, V.; Paracchini, E.; Raineri, S.M.; Gregoretti, C. Ventilator Settings to Avoid Nuisance Alarms During Mouthpiece Ventilation. Respir. Care 2016, 61, 462–467. [Google Scholar] [CrossRef]
- Chatwin, M.; Toussaint, M.; Gonçalves, M.R.; Sheers, N.; Mellies, U.; Gonzales-Bermejo, J.; Sancho, J.; Fauroux, B.; Andersen, T.; Hov, B.; et al. Airway clearance techniques in neuromuscular disorders: A state of the art review. Respir. Med. 2018, 136, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Veldhoen, E.S.; van der Wal, R.; Verweij-van den Oudenrijn, L.P.; Wösten-van Asperen, R.M.; Gaytant, M.A.; van der Ent, C.K.; van der Pol, W.L.; Hulzebos, E.H. Evidence for Beneficial Effect of Daily Use of Mechanical Insufflation-Exsufflation in Patients With Neuromuscular Diseases. Respir. Care 2023, 68, 531–546. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ventilator Parameter | Setting | Objective | Possible Problems |
|---|---|---|---|
| Pressure Support (cmH2O) | Starting from 8 (normally no need for high PS level) | Improve diurnal pCO2 and nocturnal PtCO2; treat hypopnea | Too high value may induce glottic closure and/or leaks |
| Pressurization Rate | Medium value according to the patient’s tolerance | Best tolerated | Too high value may induce glottic closure; too low value may not allow PS to be reached |
| Inspiratory Trigger | Highest sensitivity that avoid auto-trigger | Avoid ineffective effort | Auto-triggering (specially in presence of leaks) |
| Cycling criteria | Starting from 50% to lower value | Inspiratory/Expiratory ratio 1:1.5–1:2 | Too short inspiratory time |
| EPAP (cmH2O) | 4–12 | Treat obstruction with active drive | Leaks; reactive glottic closure |
| Respiratory Rate (breath/min) | 12–16 | Improve gas exchanges and efficiency of sleep | Asynchronies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlucci, A.; Fusar Poli, B. Getting It Right in Restrictive Lung Disease. J. Clin. Med. 2023, 12, 3353. https://doi.org/10.3390/jcm12103353
Carlucci A, Fusar Poli B. Getting It Right in Restrictive Lung Disease. Journal of Clinical Medicine. 2023; 12(10):3353. https://doi.org/10.3390/jcm12103353
Chicago/Turabian StyleCarlucci, Annalisa, and Barbara Fusar Poli. 2023. "Getting It Right in Restrictive Lung Disease" Journal of Clinical Medicine 12, no. 10: 3353. https://doi.org/10.3390/jcm12103353