
Clinicopathologic Profile, Management and Outcome of Sinonasal Ameloblastoma—A Systematic Review

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question
2.1.1. Inclusion Criteria
- CR and CS reporting sinonasal ameloblastoma.
2.1.2. Exclusion Criteria
- Gnathic ameloblastomas were excluded.
- Secondary sinonasal ameloblastomas were excluded.
- Pre-clinical studies, letters to the editor, commentaries and reviews were excluded.
2.2. Literature Search
2.3. Data Extraction
2.4. Quality Assessment
3. Results
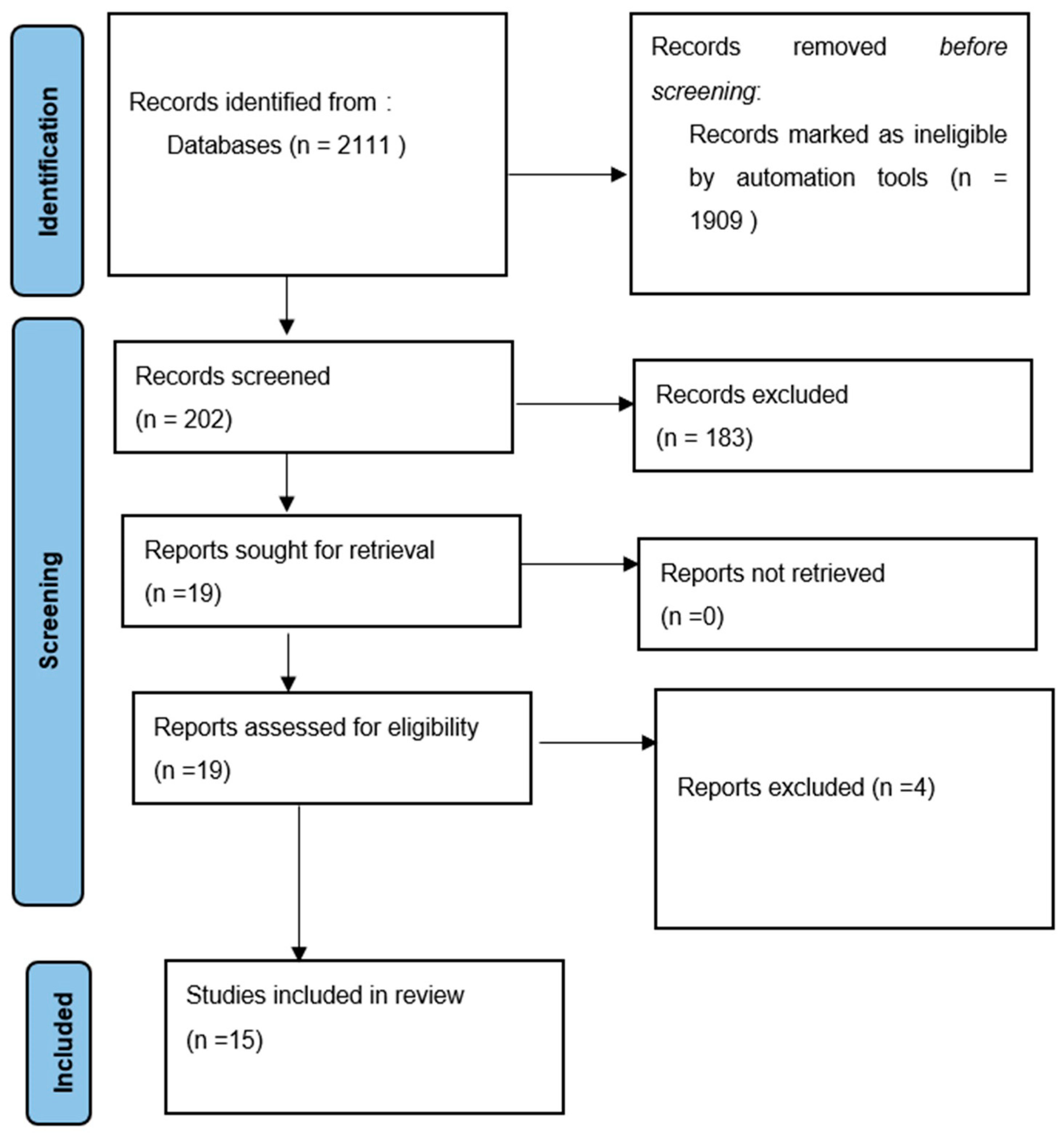
3.1. Literature Search
3.2. General Characteristics of Included Studies
3.3. Management, Recurrence Rate and Post-Op Complications
3.4. Results of the Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Da Silva, L.A.M.; Filho, S.R.C.; Saraiva, M.J.D.; Maia, C.R.; Santos, C.; Santos, P.P.A. Clinical, Radiographic and Histopathological Analysis of Craniopharyngiomas and Ameloblastomas: A Systematic Review. Head Neck Pathol. 2022, 16, 1195–1222. [Google Scholar] [CrossRef] [PubMed]
- Boffano, P.; Cavarra, F.; Tricarico, G.; Masu, L.; Brucoli, M.; Ruslin, M.; Forouzanfar, T.; Ridwan-Pramana, A.; Rodríguez-Santamarta, T.; Ranz, M.R.; et al. The epidemiology and management of ameloblastomas: A European multicenter study. J. Craniomaxillofac. Surg. 2021, 49, 1107–1112. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, G.; Padhiary, S.K.; Nayak, T.K.; Mishra, N. Rehabilitation using implants in free fibula flap of a patient with ameloblastoma: Case report with 4-year follow-up. Natl. J. Maxillofac. Surg. 2022, 13, 194–198. [Google Scholar]
- Pitak-Arnnop, P.; Subbalekha, K.; Sirintawat, N.; Meningaud, J.-P.; Tangmanee, C.; Auychai, P.; Neff, A. A retrospective cohort study on predictors associated with skull base invasion of maxillary ameloblastomas. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e439–e447. [Google Scholar] [CrossRef] [PubMed]
- Nwoga, M.C. Recurrent tumors of ameloblastoma: Clinicopathologic features and diagnostic outcome. Niger. J. Clin. Pract. 2022, 25, 1771–1777. [Google Scholar] [CrossRef] [PubMed]
- Schafer, D.R.; Thompson, L.D.R.; Smith, B.C.; Wenig, B.M. Primary ameloblastoma of the sinonasal tract: A clinicopathologic study of 24 cases. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1998, 82, 667–674. [Google Scholar] [CrossRef]
- Tranchina, M.G.; Amico, P.; Galia, A.; Emmanuele, C.; Saita, V.; Fraggetta, F. Ameloblastoma of the sinonasal tract: Report of a case with clinicopathologic considerations. Case Rep. Pathol. 2012, 2012, 218156. [Google Scholar] [CrossRef] [Green Version]
- Karp, J.; Xiong, W.; Derikvand, S.; Javer, A. Maxillary sinus ameloblastoma: Transnasal endoscopic management. Ear Nose Throat J. 2021, 100 (Suppl. S10), 908S–912S. [Google Scholar] [CrossRef]
- Barrena, B.G.; Phillips, B.J.; Moran, K.J.; Betz, S.J. Sinonasal ameloblastoma. Head Neck Pathol. 2019, 13, 247–250. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Riley, D.S.; Barber, M.S.; Kienle, G.S.; Aronson, J.; von Schoen-Angerer, T.; Tugwell, P.; Keine, H.; Helfand, M.; Altman, D.; Sox, H.; et al. CARE 2013 explanations and elaborations: Reporting guidelines for case reports. J. Clin. Epidemiol. 2017, 89, 218–235. [Google Scholar] [CrossRef] [PubMed]
- Stephen, N.; Srinivas, B.H.; Ravi, S.; Ganesh, R.N.; A Badhe, B.; Toi, P.; Jinkala, S.; Sekar, R.; Alexander, A.; Narendhar; et al. Neuroectodermal tumours of the sino-nasal tract: A clinicopathological study of 18 cases with a newly proposed revised classification and a brief review of literature. Eur. Arch. Oto-Rhino-Laryngol. 2021, 279, 1181–1191. [Google Scholar] [CrossRef]
- Vanoven, B.J.; Parker, N.P.; Petruzzelli, G.J. Peripheral ameloblastoma of the maxilla: A case report and literature review. Am. J. Otolaryngol. 2008, 29, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Alexiev, B.A.; Tumer, Y.; Bishop, J.A. Sinonasal adamantinoma-like Ewing sarcoma: A case report. Pathol. Res. Pract. 2017, 213, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Scheer, M.; Drebber, U.; Kübler, A.; Zöller, J.E. Der interessante Fall Nr. 52. Laryngorhinootologie 2002, 81, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Guilemany, J.M.; Ballesteros, F.; Alos, L.; Alobid, I.; Prades, E.; Menéndez, L.M.; Cardesa, A. Plexiform ameloblastoma presenting as a sinonasal tumor. Eur. Arch. Oto-Rhino-Laryngol. Head Neck 2004, 261, 304–306. [Google Scholar] [CrossRef]
- Ereno, C.; Etxegarai, L.; Corral, M.; Basurko, J.M.; Bilbao, F.J.; López, J.I. Primary sinonasal ameloblastoma: Case report. APMIS 2005, 113, 148–150. [Google Scholar] [CrossRef]
- Koscielny, S.; Stebel, S. Das Ameloblastom als Differenzialdiagnose von Tumoren der Nasennebenhöhlen. Laryngorhinootologie 2010, 89, 367–368. [Google Scholar] [CrossRef]
- Leong, S.C.; Karkos, P.D.; Krajacevic, J.; Islam, R.; Kent, S.E. Ameloblastoma of the sinonasal tract: A case report. Ear Nose Throat J. 2010, 89, 70–71. [Google Scholar] [CrossRef] [Green Version]
- Morrison, E.J.; Wei, B.P.; Galloway, S.; De Alwis, N.; Lyons, B.; Baker, T. A rare case of sinonasal ameloblastoma presenting with complete nasal obstruction. ANZ J. Surg. 2011, 81, 931–932. [Google Scholar] [CrossRef]
- Shahidi, S.H.; Bronoosh, P.; Daneshbod, Y. Follicular ameloblastoma presenting as a sinonasal tumor. Iran. Red Crescent Med. J. 2012, 14, 113. [Google Scholar] [PubMed]
- Temporale, H.; Zatoński, T.; Roszkowska, A.; Kręcicki, T. Ameloblastoma of the nasal septum origin: A case report. Case Rep. Otolaryngol. 2013, 2013, 280509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiedler, L.S.; Wunsch, A. Ameloblastoma of the maxillary sinus: Conservative surgical management considering high recurrence risk potential. BMJ Case Rep. CP 2021, 14, e241487. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.-J.; Liu, Z.-P.; Xu, C.-Y.; Zhang, X.-L.; Liu, X.-W.; Wang, J.-Y.; Guo, Y.-F. Endoscopic Management of Recurrent Maxillary Sinus Ameloblastoma in a Child With Autism Spectrum Disorder: A Case Report. Ear Nose Throat J. 2022; ahead of print. [Google Scholar]
- Harada, H.; Kimura, S.; Kimura, Y.; Higaki, K.; Kurose, A. Sinonasal ameloblastoma: A case report focusing on histogenesis and related morphological characteristics. Oral Maxillofac. Surg. Cases 2020, 6, 100201. [Google Scholar] [CrossRef]
- London, S.D.; Schlosser, R.J.; Gross, C.W. Endoscopic management of benign sinonasal tumors: A decade of experience. Am. J. Rhinol. 2002, 16, 221–227. [Google Scholar] [CrossRef]
- Karp, J.; Bryk, J.; Menke, E.; McTigue, D. The complete endodontic obturation of an avulsed immature permanent incisor with mineral trioxide aggregate: A case report. Pediatr. Dent. 2006, 28, 273–278. [Google Scholar]
- Ajila, V.; Hegde, S. Ameloblastomas vs recurrent ameloblastomas: A systematic review. J. Oral Med. Oral Surg. 2022, 28, 11. [Google Scholar] [CrossRef]
- Philipsen, H.P.; Reichart, P.A.; Nikai, H.; Takata, T.; Kudo, Y. Peripheral ameloblastoma: Biological profile based on 160 cases from the literature. Oral Oncol. 2001, 37, 17–27. [Google Scholar] [CrossRef]
- Patsa, S.; Jadav, R.B.; Halder, G.C.; Ray, J.G.; Datta, S.; Deb, T. Demographic and histopathological variation of ameloblastoma: A hospital-based study. J. Oral Maxillofac. Pathol. JOMFP 2016, 20, 230. [Google Scholar]
- Chawla, R.; Ramalingam, K.; Sarkar, A.; Muddiah, S. Ninety-one cases of ameloblastoma in an Indian population: A comprehensive review. J. Nat. Sci. Biol. Med. 2013, 4, 310–315. [Google Scholar] [CrossRef]


{kind=link}
| Study (Author(s), Year) | Country | Ethnicity | Participants/Cases with SNA (n) | SNA (n) | Age (Mean/Median, Range; Years) | Gender (n) | Features/Presentation | Deaths Due to Ameloblastoma | Follow-up (Mean & Range, Years) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Histological | Radiographic | Clinical | |||||||||
| Schafer et al., 1998 [6] | USA | NA | 24 | 24 | Mean 59.7; Range: 43–81 years | M: 19; F: 5 | Peripheral palisaded columnar cells with reverse polarity | Solid masses or opacities in nasal cavity, maxillary sinus, or both Plexiform pattern Surface epithelial derivation | Enlarging mass (n = 24) Sinusitis (n = 9) Epistaxis (n = 8) | 0 | 9.5; 1–44 |
| London et al., 2002 [26] | USA | NA | 1 (out of 18) | 1 | NR | NR | NR | NR | NR | 0 | 4 years |
| Guilemany et al., 2004 [16] | Spain | NA | 1 | 1 | 68 years | M: 1 | Long anastomosing strands of odontogenic epithelium | Bony erosion of lateral sinus and orbital floor | Headache, maxillary pain, facial paresthesia, nasal obstruction, rhinorrhea | 0 | 50 months |
| Ereno et al., 2005 [17] | Spain | NA | 1 | 1 | 66 years | M: 1 | Anastomosing epithelial cords within a hyaline fibrous stroma; arising from surface epithelium of maxillary sinus | Opaque mass in the nasal cavity, and maxillary and ethmoidal sinuses with loss of integrity of alveolar area | Nasal obstruction and bleeding | 0 | 9 months |
| Koscielny et al., 2020 [18] | Germany | NA | 1 | 1 | 56 years | NR | Epithelial-mesenchymal tumor, mimicking primitive tooth formation | Mass obstructing right nasal cavity. | Progressive hearing loss and nasal obstruction for one year | 0 | 1 year |
| Leong et al., 2010 [19] | UK | NA | 1 | 1 | 61 years | M: 1 | Respiratory mucosa infiltrated by interconnecting strands and cords of epithelium in loose, vascular sparsely cellular connective tissue stroma indicating | Complete obstruction of nasal cavity with deviated nasal septum to the other side. Middle turbinate obliterated. | Nasal obstruction, blood-stained mucus. Lesion: lobulated, vascular. | 0 | 12 months |
| Morrisson et al., 2011 [20] | Australia | NA | 1 | 1 | 73 years | F: 1 | Follicular pattern; cords of tumor within a hyalinized fossa | Expansive, erosive mass obstructing nasal cavity and nasopharyngeal air space | Complete nasal obstruction; polypoid mass. | 0 | NR |
| Shahidi et al., 2012 [21] | Iran | NA | 1 | 1 | 74 years | M: 1 | Follicular islands of odontogenic epithelium presenting follicular ameloblastoma | Erosion of alveolar process and left premolar and molar region. Loss of borders of maxillary sinus and lateral wall of nasal fossa. Massive expansile lesion invading the entire affected maxillary sinus | Yellowish-white necrotized tissue surrounded by an erythemic rim and mucosal hyperplasia. Bony swelling in the premolar and molar region | 0 | 4 years |
| Temporale et al., 2013 [22] | Poland | NA | 1 | 1 | 35 years | M: 1 | Ameloblastoma | Soft tissue mass involving nasopharynx, ethmoid and sphenoid sinus | Nasal obstruction occurred 2 months after removal of nasal cyst noted after septoplasty | 0 | NR |
| Barrena et al., 2019 [9] | USA | NA | 1 | 1 | 34 years | M: 1 | Ameloblastic islands: hyperchromatic columnar cells with reverse polarity. | Pain and selling in left maxillary for 2–3 weeks | Well-demarcated, soft tissue mass in left maxillofacial region. Complete obstruction of left maxillary sinus, nasal cavity, and ethmoid sinus. Extension to alveolar process, body of zygoma and floor of orbit. Involvement as far as posterior portion of body of sphenoid. | 0 | 12 days |
| Harada et al., 2020 [25] | Japan | Japanese | 1 | 1 | 80 years | M: 1 | Basaloid cells with cystic structures; columnar or cuboidal epithelial cells. | Mass initially diagnosed as a polyp and misdiagnosed as a salivary gland tumor. | MRI revealed lesion in right nasal cavity and right maxillary sinus. | 0 | 2 years |
| Fiedler et al., 2021 [23] | Germany | NA | 1 | 1 | 38 years | M: 1 | NA | Nasal obstruction | Completely obstructed right maxillary sinus and distortion of middle and inferior conchae. | 0 | 4 months |
| Karp et al., 2021 [8] | Not clear | Caucasian | 1 | 1 | 64 years | M: 1 | Cyst-like; columnar epithelial cells. | Inferomedially to the root of the upper left third molar | Diagnosis of SNA made during repeat endoscopic sinus surgery. | 0 | 15 months |
| Tranchina et al., 2021 [7] | Italy | NA | 1 | 1 | 74 years | M: 1 | Cords and follicular islands of odontogenic epithelium; columnar cells with reverse polarity. | Lytic, expansile, solid lesion; from nasopharynx to lateral pharyngeal space, laterally to the parotid. Erosion of bone in the middle cranial fossa | 2 months of progressive right-side obstruction, rhinorrhea and sinusitis | 0 | 12 months |
| Wu et al., 2022 [24] | China | NA | 1 | 1 | 14 years | M: 1 | Capsule wall-like substance composed of fibrous tissue lined with odontogenic epithelium and epithelial nests and calcium deposits | Expansive bone destruction of the maxillary sinus | Swelling noted on left cheek one month after a cold | 0 | 16 months |
| Study (Author(s), Year) | Treatment | Recurrence (n (%), Time Post Treatment) | Post Treatment Complications |
|---|---|---|---|
| Schafer et al., 1998 [6] | Surgical excision (n = 23) Maxillectomy + radiotherapy (n = 1) | 5 (21%), 1–13 years | None |
| London et al., 2002 [26] | Computer assisted endoscopy | NR | None |
| Guilemany et al., 2004 [16] | Resection; paralateral rhinotomy; radiotherapy | 0 | None |
| Ereno et al., 2005 [17] | Radical right maxillectomy with radiotherapy | 0 | None |
| Koscielny et al., 2020 [18] | Maxillary resection through lateral rhinotomy | 0 | None |
| Leong et al., 2010 [19] | Endoscopic resection | 0 | None |
| Morrisson et al., 2011 [20] | Right total maxillectomy and ethmoidectomy, with clearance of right infratemporal fossa. Reconstruction with a vertical rectus abdominis mycocutaneous flap | 0 | None |
| Shahidi et al., 2012 [21] | Radical left maxillectomy | 0 | None |
| Temporale et al., 2013 [22] | Radical surgery—access through eversion of face coverings (removal of front and medial call of right maxillary sinus wall | 0 | None |
| Barrena et al., 2019 [9] | Unilateral total ethmoidectomy, frontal sinusotomy, sphenoid sinusotomy with left infratemporal dissection. Free flap reconstruction and orbital reconstruction | NR | None |
| Harada et al., 2020 [25] | Surgical excision | After 2 years | Not available–recurrent mass left untreated |
| Fiedler et al., 2021 [23] | Transnasal functional endoscopic sinus surgery | 0 | None |
| Karp et al., 2021 [8] | Endoscopic (transnasal) turbinectomy and medical maxillectomy | 1 (6 months post-op) | Numbness of tooth 27—extracted. |
| Tranchina et al., 2021 [7] | Endoscopic excision | 0 | 0 |
| Wu et al., 2022 [24] | Left uncinate process resected endoscopically and maxillary sinus was opened for access (two surgeries required due to recurrence) | 1 (10 months) | None |
| Topic | Schafer et al., 1998 [6] | London et al., 2002 [26] | Guilemany et al., 2004 [16] | Ereno et al., 2005 [17] | Koscielny et al., 2020 [18] | Leong et al., 2010 [19] | Morrisson et al., 2011 [20] | Shahidi et al., 2012 [21] | Temporale et al., 2013 [22] | Barrena et al., 2019 [9] | Harada et al., 2020 [25] | Karp et al., 2021 [8] | Fiedler et al., 2021 [23] | Tranchina et al., 2021 [7] | Wu et al., 2022 [24] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Title (mentioning case report) | Yes | No | No | No | No | Yes | Yes | No | Yes | No | Yes | No | No | Yes | Yes |
| Key words (with ‘case report’) | No | No | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Abstract | |||||||||||||||
| Background | Yes | No | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Main findings | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Conclusion | Yes | Yes | Yes | Yes | No | Yes | No | No | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Adequate introduction | Yes | No | Yes | No | No | No | Yes | Yes | Yes | No | No | Yes | No | No | No |
| Patient information | |||||||||||||||
| De-identified information | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Concerns and symptoms | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | No | Yes | No | Yes |
| Medical, family, psychosocial genetic history | No | No | No | No | Yes | No | No | Yes | No | No | Partially | No | No | No | Yes |
| Past interventions and outcomes | No | No | No | No | No | No | No | Yes | Yes | No | Yes | Yes | No | No | Yes |
| Physical examination and clinical findings | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Timeline | No | No | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Diagnostic assessment | |||||||||||||||
| Testing | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Partial | Yes | Yes | Yes | Yes |
| Challenges | No | No | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Diagnosis | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Prognosis/staging | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Intervention | |||||||||||||||
| Type of intervention stated | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Dosage/level/details of intervention | Yes | Yes | No | No | Yes | No | No | No | Yes | Yes | No | Yes | Yes | No | Yes |
| Changes/modifications | No | No | Yes | No | No | No | No | No | No | No | No | No | No | No | Yes |
| Follow-up/outcome details reported | |||||||||||||||
| Clinician-/patient-reported outcomes | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Follow-up diagnostic tests | No | No | Yes | No | Yes | No | No | No | No | No | Yes | Yes | Yes | No | Yes |
| Adherence and tolerability to follow-up tests | Yes | Yes | No | No | No | No | No | No | No | No | No | No | No | No | Yes |
| Adverse effects reported | No | No | No | No | No | No | No | No | No | No | No | Yes | No | No | No |
| Discussion | |||||||||||||||
| Strengths and limitations | No | No | No | No | No | No | No | Yes | No | No | No | No | No | No | No |
| Discussion of relevant literature | Yes | Yes | Yes | Yes | Partially | No | No | Yes | Yes | Yes | Yes | Yes | Partially | Yes | Yes |
| Rationale for conclusions | Yes | Yes | Yes | Yes | No | No | No | No | Yes | No | Yes | Yes | Yes | No | Yes |
| Take-away lessons/recommendations | Yes | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | No | No | Yes |
| Patient perspective | Yes | No | No | No | No | No | No | No | Yes | No | No | No | No | No | No |
| Informed consent/ethical approval | No | No | No | No | No | No | No | No | No | Yes | No | No | No | No | Yes |
| Overall quality | Moderate | Low | Low | Low | Low | Low | Low | Low | High | Low | Low | Moderate | Low | Low | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mehta, V.; Sarode, G.S.; Obulareddy, V.T.; Sharma, T.; Kokane, S.; Cicciù, M.; Minervini, G. Clinicopathologic Profile, Management and Outcome of Sinonasal Ameloblastoma—A Systematic Review. J. Clin. Med. 2023, 12, 381. https://doi.org/10.3390/jcm12010381
Mehta V, Sarode GS, Obulareddy VT, Sharma T, Kokane S, Cicciù M, Minervini G. Clinicopathologic Profile, Management and Outcome of Sinonasal Ameloblastoma—A Systematic Review. Journal of Clinical Medicine. 2023; 12(1):381. https://doi.org/10.3390/jcm12010381
Chicago/Turabian StyleMehta, Vini, Gargi S. Sarode, Vishnu Teja Obulareddy, Tanvi Sharma, Shruti Kokane, Marco Cicciù, and Giuseppe Minervini. 2023. "Clinicopathologic Profile, Management and Outcome of Sinonasal Ameloblastoma—A Systematic Review" Journal of Clinical Medicine 12, no. 1: 381. https://doi.org/10.3390/jcm12010381