
Arrhythmia and Heart Rate Variability during Long Interdialytic Periods in Patients on Maintenance Hemodialysis: Prospective Observational Cohort Study
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Continuous ECG Monitoring by a Wearable Patch
2.3. Discrimination of Arrhythmias
2.4. HRV Measurements
2.5. Clinical Covariates
2.6. Statistical Analysis
3. Results
3.1. Participants
3.2. Arrhythmia during the Interdialytic Period
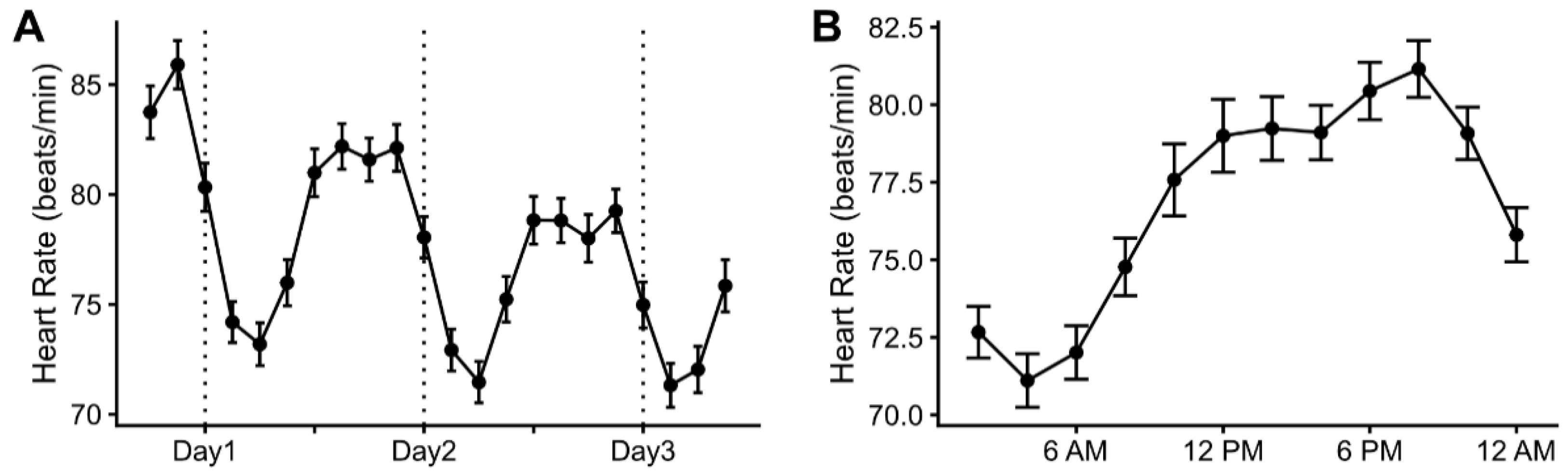
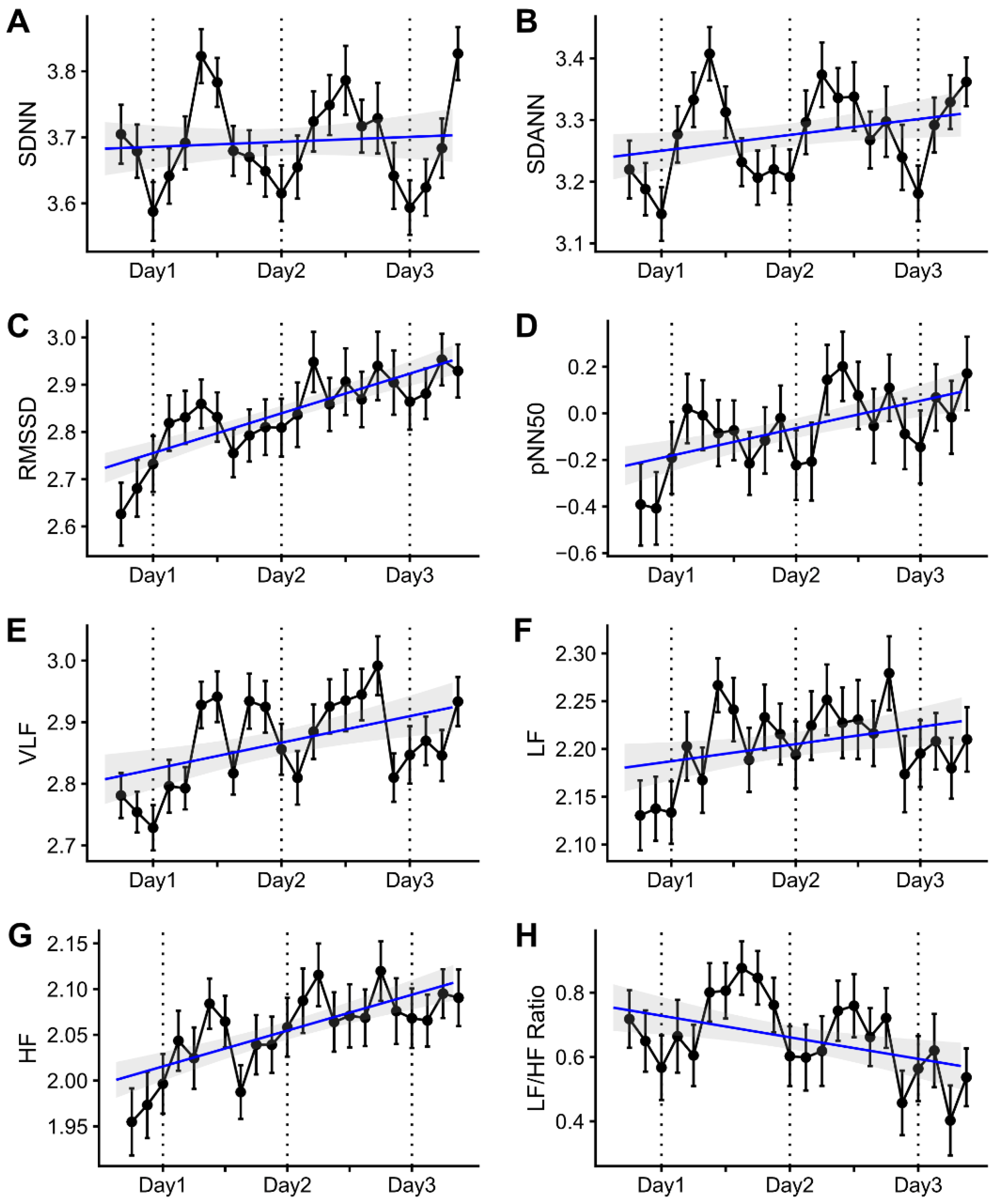
3.3. Heart Rate Variability during the Interdialytic Period
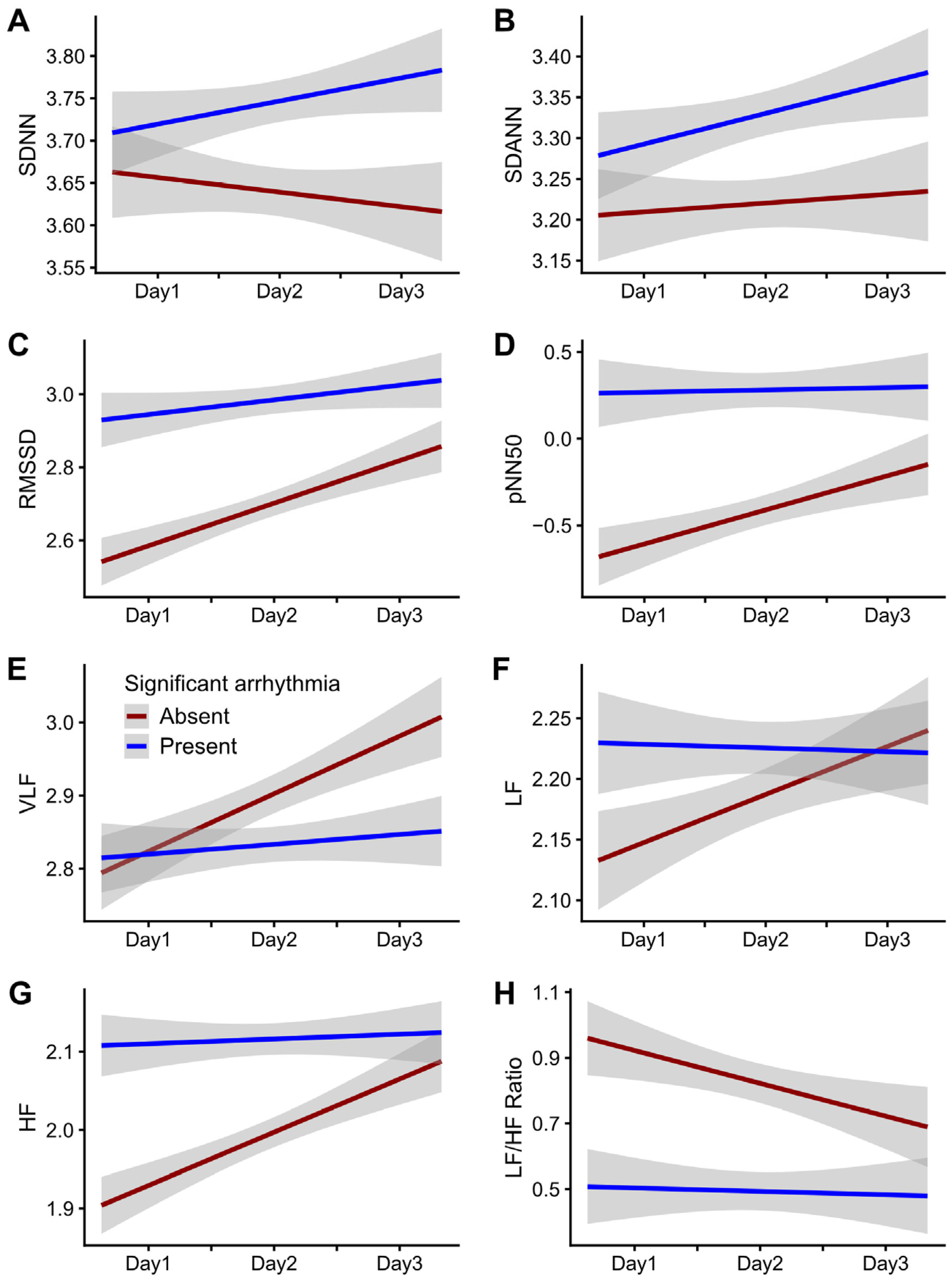
3.4. Temporal Trends in HRV Parameters According to the Presence of Arrhythmia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Makar, M.S.; Pun, P.H. Sudden Cardiac Death Among Hemodialysis Patients. Am. J. Kidney Dis. 2017, 69, 684–695. [Google Scholar] [CrossRef] [Green Version]
- Jadoul, M.; Thumma, J.; Fuller, D.S.; Tentori, F.; Li, Y.; Morgenstern, H.; Mendelssohn, D.; Tomo, T.; Ethier, J.; Port, F.; et al. Modifiable practices associated with sudden death among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study. Clin. J. Am. Soc. Nephrol. 2012, 7, 765–774. [Google Scholar] [CrossRef] [Green Version]
- Tereshchenko, L.G.; Kim, E.D.; Oehler, A.; Meoni, L.A.; Ghafoori, E.; Rami, T.; Maly, M.; Kabir, M.; Hawkins, L.; Tomaselli, G.F.; et al. Electrophysiologic Substrate and Risk of Mortality in Incident Hemodialysis. J. Am. Soc. Nephrol. 2016, 27, 3413–3420. [Google Scholar] [CrossRef] [Green Version]
- Bleyer, A.J.; Hartman, J.; Brannon, P.C.; Reeves-Daniel, A.; Satko, S.G.; Russell, G. Characteristics of sudden death in hemodialysis patients. Kidney Int. 2006, 69, 2268–2273. [Google Scholar] [CrossRef] [Green Version]
- Foley, R.N.; Gilbertson, D.T.; Murray, T.; Collins, A.J. Long interdialytic interval and mortality among patients receiving hemodialysis. N. Engl. J. Med. 2011, 365, 1099–1107. [Google Scholar] [CrossRef]
- Perl, J.; Chan, C.T. Timing of sudden death relative to the hemodialysis procedure. Nat. Clin. Pract. Nephrol. 2006, 2, 668–669. [Google Scholar] [CrossRef]
- Wong, M.C.; Kalman, J.M.; Pedagogos, E.; Toussaint, N.; Vohra, J.K.; Sparks, P.B.; Sanders, P.; Kistler, P.M.; Halloran, K.; Lee, G.; et al. Temporal distribution of arrhythmic events in chronic kidney disease: Highest incidence in the long interdialytic period. Heart Rhythm 2015, 12, 2047–2055. [Google Scholar] [CrossRef]
- Roy-Chaudhury, P.; Tumlin, J.A.; Koplan, B.A.; Costea, A.I.; Kher, V.; Williamson, D.; Pokhariyal, S.; Charytan, D.M. Primary outcomes of the Monitoring in Dialysis Study indicate that clinically significant arrhythmias are common in hemodialysis patients and related to dialytic cycle. Kidney Int. 2018, 93, 941–951. [Google Scholar] [CrossRef]
- Rogovoy, N.M.; Howell, S.J.; Lee, T.L.; Hamilton, C.; Perez-Alday, E.A.; Kabir, M.M.; Zhang, Y.; Kim, E.D.; Fitzpatrick, J.; Monroy-Trujillo, J.M.; et al. Hemodialysis Procedure-Associated Autonomic Imbalance and Cardiac Arrhythmias: Insights From Continuous 14-Day ECG Monitoring. J. Am. Heart Assoc. 2019, 8, e013748. [Google Scholar] [CrossRef] [Green Version]
- Noppakun, K.; Putchagarn, P.; Phrommintikul, A.; Wongcharoen, W. Effects of interdialytic interval on heart rate variability in chronic hemodialysis patients: A cross-sectional study. Sci. Rep. 2021, 11, 20944. [Google Scholar] [CrossRef]
- Okólska, M.; Łach, J.; Matusik, P.T.; Pająk, J.; Mroczek, T.; Podolec, P.; Tomkiewicz-Pająk, L. Heart Rate Variability and Its Associations with Organ Complications in Adults after Fontan Operation. J. Clin. Med. 2021, 10, 4492. [Google Scholar] [CrossRef] [PubMed]
- Vuoti, A.O.; Tulppo, M.P.; Ukkola, O.H.; Junttila, M.J.; Huikuri, H.V.; Kiviniemi, A.M.; Perkiömäki, J.S. Prognostic value of heart rate variability in patients with coronary artery disease in the current treatment era. PLoS ONE 2021, 16, e0254107. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.T.; Chang, Y.M.; Chen, I.L.; Yang, C.L.; Leu, S.C.; Su, H.L.; Kao, J.L.; Tsai, S.C.; Jhen, R.N.; Tang, W.R.; et al. Heart rate variability during hemodialysis is an indicator for long-term vascular access survival in uremic patients. PLoS ONE 2017, 12, e0172212. [Google Scholar] [CrossRef] [Green Version]
- Kida, N.; Tsubakihara, Y.; Kida, H.; Ageta, S.; Arai, M.; Hamada, Y.; Matsuura, N. Usefulness of measurement of heart rate variability by holter ECG in hemodialysis patients. BMC Nephrol. 2017, 18, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanna, T.; Diener, H.C.; Passman, R.S.; Di Lazzaro, V.; Bernstein, R.A.; Morillo, C.A.; Rymer, M.M.; Thijs, V.; Rogers, T.; Beckers, F.; et al. Cryptogenic stroke and underlying atrial fibrillation. N. Engl. J. Med. 2014, 370, 2478–2486. [Google Scholar] [CrossRef] [Green Version]
- Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [CrossRef] [Green Version]
- Zhu, H.; Pan, Y.; Wu, F.; Huan, R. Optimized Electrode Locations for Wearable Single-Lead ECG Monitoring Devices: A Case Study Using WFEES Modules Based on the LANS Method. Sensors 2019, 19, 4458. [Google Scholar] [CrossRef] [Green Version]
- Kwon, S.; Lee, S.R.; Choi, E.K.; Ahn, H.J.; Song, H.S.; Lee, Y.S.; Oh, S. Validation of Adhesive Single-Lead ECG Device Compared with Holter Monitoring among Non-Atrial Fibrillation Patients. Sensors 2021, 21, 3122. [Google Scholar] [CrossRef]
- Buccelletti, E.; Gilardi, E.; Scaini, E.; Galiuto, L.; Persiani, R.; Biondi, A.; Basile, F.; Silveri, N.G. Heart rate variability and myocardial infarction: Systematic literature review and metanalysis. Eur. Rev. Med. Pharmacol. Sci. 2009, 13, 299–307. [Google Scholar]
- Saran, R.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.; Albertus, P.; Ayanian, J.; Balkrishnan, R.; Bragg-Gresham, J.; Cao, J.; Chen, J.L. US renal data system 2016 annual data report: Epidemiology of kidney disease in the United States. Am. J. Kidney Dis. 2017, 69, A7–A8. [Google Scholar] [CrossRef] [Green Version]
- Herzog, C.A.; Mangrum, J.M.; Passman, R. Sudden cardiac death and dialysis patients. Semin. Dial. 2008, 21, 300–307. [Google Scholar] [CrossRef]
- Rantanen, J.M.; Riahi, S.; Schmidt, E.B.; Johansen, M.B.; Søgaard, P.; Christensen, J.H. Arrhythmias in Patients on Maintenance Dialysis: A Cross-sectional Study. Am. J. Kidney Dis. 2020, 75, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Moak, J.P.; Goldstein, D.S.; Eldadah, B.A.; Saleem, A.; Holmes, C.; Pechnik, S.; Sharabi, Y. Supine low-frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation. Heart Rhythm 2007, 4, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Karemaker, J.M. The multibranched nerve: Vagal function beyond heart rate variability. Biol. Psychol. 2022, 172, 108378. [Google Scholar] [CrossRef]
- Fukuta, H.; Hayano, J.; Ishihara, S.; Sakata, S.; Mukai, S.; Ohte, N.; Ojika, K.; Yagi, K.; Matsumoto, H.; Sohmiya, S.; et al. Prognostic value of heart rate variability in patients with end-stage renal disease on chronic haemodialysis. Nephrol. Dial. Transplant 2003, 18, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Oikawa, K.; Ishihara, R.; Maeda, T.; Yamaguchi, K.; Koike, A.; Kawaguchi, H.; Tabata, Y.; Murotani, N.; Itoh, H. Prognostic value of heart rate variability in patients with renal failure on hemodialysis. Int. J. Cardiol. 2009, 131, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Hiroshi, T.; Aoyama, T.; Tanaka, M.; Ishii, H.; Kisohara, M.; Iizuka, N.; Murohara, T.; Hayano, J. Nonlinear measures of heart rate variability and mortality risk in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2012, 7, 1454–1460. [Google Scholar] [CrossRef] [Green Version]
- Seibert, E.; Zohles, K.; Ulrich, C.; Kluttig, A.; Nuding, S.; Kors, J.A.; Swenne, C.A.; Werdan, K.; Fiedler, R.; Girndt, M. Association between autonomic nervous dysfunction and cellular inflammation in end-stage renal disease. BMC Cardiovasc. Disord. 2016, 16, 210. [Google Scholar] [CrossRef] [Green Version]
- Kersh, E.S.; Kronfield, S.J.; Unger, A.; Popper, R.W.; Cantor, S.; Cohn, K. Autonomic insufficiency in uremia as a cause of hemodialysis-induced hypotension. N. Engl. J. Med. 1974, 290, 650–653. [Google Scholar] [CrossRef]
- Kamga, P.; Mostafa, R.; Zafar, S. The Use of Wearable ECG Devices in the Clinical Setting: A Review. Curr. Emerg. Hosp. Med. Rep. 2022, 10, 67–72. [Google Scholar] [CrossRef]
- Wieringa, F.P.; Broers, N.J.H.; Kooman, J.P.; Van Der Sande, F.M.; Van Hoof, C. Wearable sensors: Can they benefit patients with chronic kidney disease? Expert Rev. Med. Devices 2017, 14, 505–519. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.Y.; Wong, L.S. Uremic Pruritus: From Diagnosis to Treatment. Diagnostics 2022, 12, 1108. [Google Scholar] [CrossRef] [PubMed]
- Winkelmayer, W.C.; Patrick, A.R.; Liu, J.; Brookhart, M.A.; Setoguchi, S. The increasing prevalence of atrial fibrillation among hemodialysis patients. J. Am. Soc. Nephrol. 2011, 22, 349–357. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Participants (n = 49) | Significant Arrhythmia | ||
|---|---|---|---|---|
| Absent (n = 26) | Present (n = 23) | p-Value | ||
| Age, years | 55.2 ± 10.3 | 51.9 ± 9.3 | 59.0 ± 10.2 | 0.014 |
| Male, n (%) | 25 (51.0) | 12 (46.2) | 13 (56.5) | 0.661 |
| Post-hemodialysis weight, kg | 62.5 ± 12.6 | 62.1 ± 13.5 | 63.0 ± 11.7 | 0.813 |
| Comorbidity, n (%) | ||||
| Diabetes | 26 (53.1) | 13 (50.0) | 13 (56.5) | 0.865 |
| Hypertension | 48 (98.0) | 26 (100.0) | 22 (95.7) | 0.469 |
| Coronary artery disease | 8 (16.3) | 3 (11.5) | 5 (21.7) | 0.448 |
| Cerebrovascular accident | 1 (2.0) | 1 (3.8) | 0 (0.0) | 1.000 |
| Cause of ESRD, n (%) | 0.918 | |||
| Diabetic nephropathy | 23 (46.9) | 12 (46.2) | 11 (47.8) | |
| Hypertensive | 12 (24.5) | 7 (26.9) | 5 (21.7) | |
| Glomerulonephritis | 11 (22.4) | 6 (23.1) | 5 (21.7) | |
| Other | 3 (6.1) | 1 (3.8) | 2 (8.7) | |
| HD duration, months | 71.9 (26.7, 143.3) | 66.7 (22.9, 94.6) | 89.7 (27.1, 165.3) | 0.131 |
| Beta-blocker use, n (%) | 16 (32.7) | 10 (38.5) | 6 (26.1) | 0.537 |
| Hemoglobin, g/dL | 10.4 ± 1.3 | 10.7 ± 1.3 | 10.2 ± 1.3 | 0.196 |
| Ferritin, ng/mL | 275 (199, 420) | 287 (182, 427) | 260 (217, 386) | 0.581 |
| Transferrin saturation, % | 31.2 (26.8, 42.2) | 30.3 (27.7, 40.2) | 35.6 (23.6, 43.4) | 0.942 |
| Albumin, g/dL | 4.10 (3.80, 4.30) | 4.10 (3.82, 4.27) | 4.10 (3.85, 4.25) | 0.793 |
| Potassium, mmol/L | 4.58 ± 0.72 | 4.58 ± 0.70 | 4.58 ± 0.76 | 0.978 |
| Total calcium, mg/dL | 8.96 ± 0.65 | 8.75 ± 0.68 | 9.19 ± 0.53 | 0.015 |
| Phosphorus, mg/dL | 4.63 ± 1.41 | 4.67 ± 1.48 | 4.58 ± 1.36 | 0.833 |
| Intact PTH, pg/mL | 206 (123, 346) | 219 (160, 321) | 157 (111, 360) | 0.302 |
| Unadjusted Models | Multivariable Models | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline Difference | Difference in Mean Change per Day | Baseline Difference | Difference in Mean Change per Day | |||||||||
| β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | |
| SDNN | 0.040 | 0.109 | 0.717 | 0.035 | 0.018 | 0.055 | 0.085 | 0.109 | 0.439 | 0.039 | 0.020 | 0.056 |
| SDANN | 0.072 | 0.129 | 0.581 | 0.024 | 0.017 | 0.151 | 0.143 | 0.127 | 0.266 | 0.029 | 0.018 | 0.117 |
| RMSSD | 0.465 | 0.158 | 0.005 | −0.093 | 0.022 | <0.001 | 0.446 | 0.160 | 0.007 | −0.078 | 0.024 | 0.001 |
| pNN50 | 1.159 | 0.394 | 0.005 | −0.231 | 0.057 | <0.001 | 1.222 | 0.389 | 0.003 | −0.237 | 0.062 | <0.001 |
| VLF | 0.049 | 0.079 | 0.541 | −0.054 | 0.021 | 0.009 | 0.059 | 0.086 | 0.491 | −0.044 | 0.023 | 0.055 |
| LF | 0.133 | 0.085 | 0.126 | −0.043 | 0.015 | 0.003 | 0.158 | 0.085 | 0.070 | −0.030 | 0.016 | 0.057 |
| HF | 0.248 | 0.080 | 0.003 | −0.067 | 0.013 | <0.001 | 0.243 | 0.082 | 0.005 | −0.061 | 0.014 | <0.001 |
| LF/HF ratio | −0.487 | 0.223 | 0.033 | 0.103 | 0.042 | 0.015 | −0.386 | 0.203 | 0.062 | 0.144 | 0.046 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.Y.; Cho, N.-J.; Park, S.; Lee, H.; Hong, M.; Lee, E.Y.; Gil, H.-W. Arrhythmia and Heart Rate Variability during Long Interdialytic Periods in Patients on Maintenance Hemodialysis: Prospective Observational Cohort Study. J. Clin. Med. 2023, 12, 265. https://doi.org/10.3390/jcm12010265
Choi HY, Cho N-J, Park S, Lee H, Hong M, Lee EY, Gil H-W. Arrhythmia and Heart Rate Variability during Long Interdialytic Periods in Patients on Maintenance Hemodialysis: Prospective Observational Cohort Study. Journal of Clinical Medicine. 2023; 12(1):265. https://doi.org/10.3390/jcm12010265
Chicago/Turabian StyleChoi, Ha Young, Nam-Jun Cho, Samel Park, Hwamin Lee, Min Hong, Eun Young Lee, and Hyo-Wook Gil. 2023. "Arrhythmia and Heart Rate Variability during Long Interdialytic Periods in Patients on Maintenance Hemodialysis: Prospective Observational Cohort Study" Journal of Clinical Medicine 12, no. 1: 265. https://doi.org/10.3390/jcm12010265