
Prone Position Facilitates Creation of Ulnar-Basilic Arteriovenous Fistula

 , , , ,
, , , ,  , and
, and 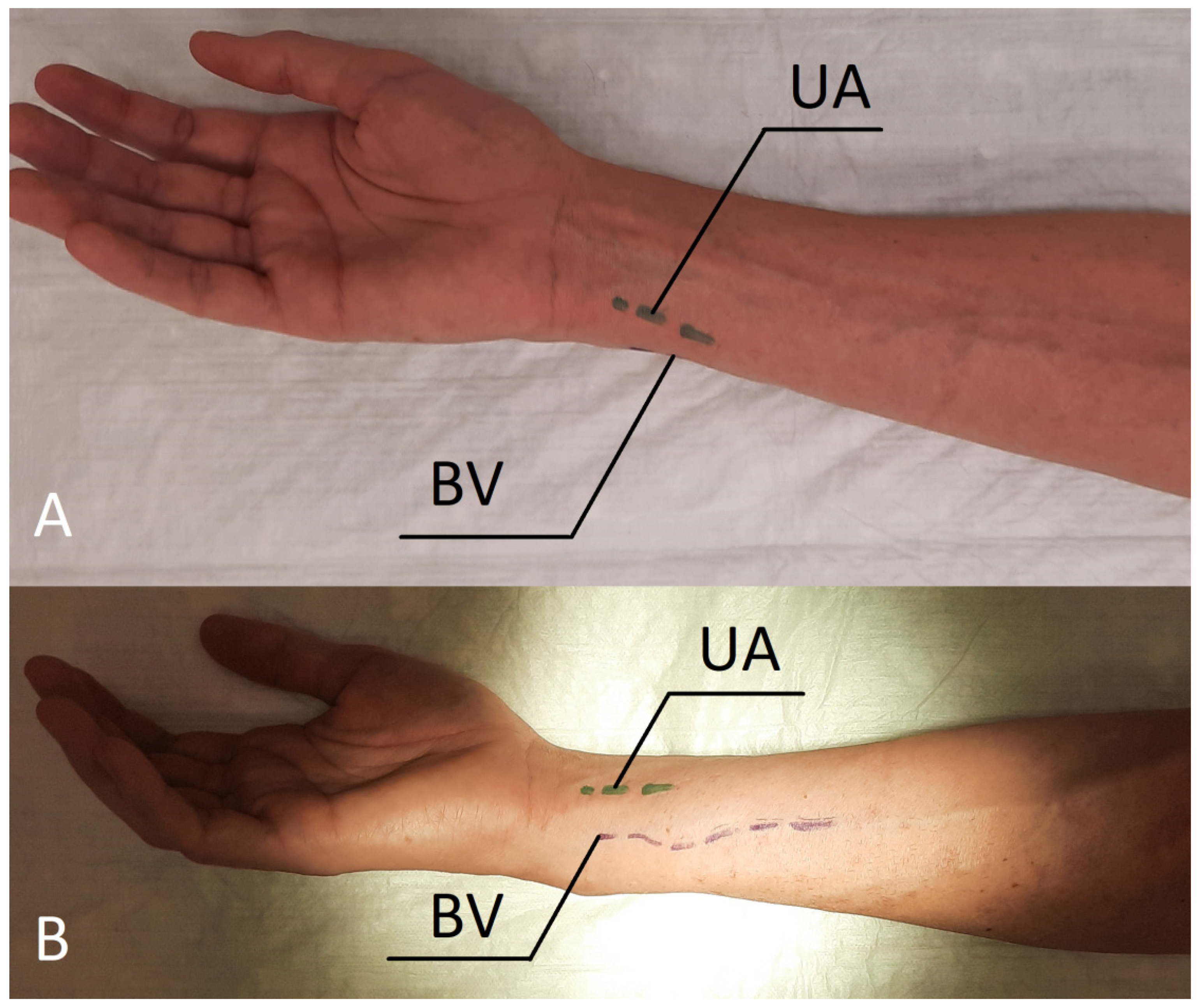{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Description
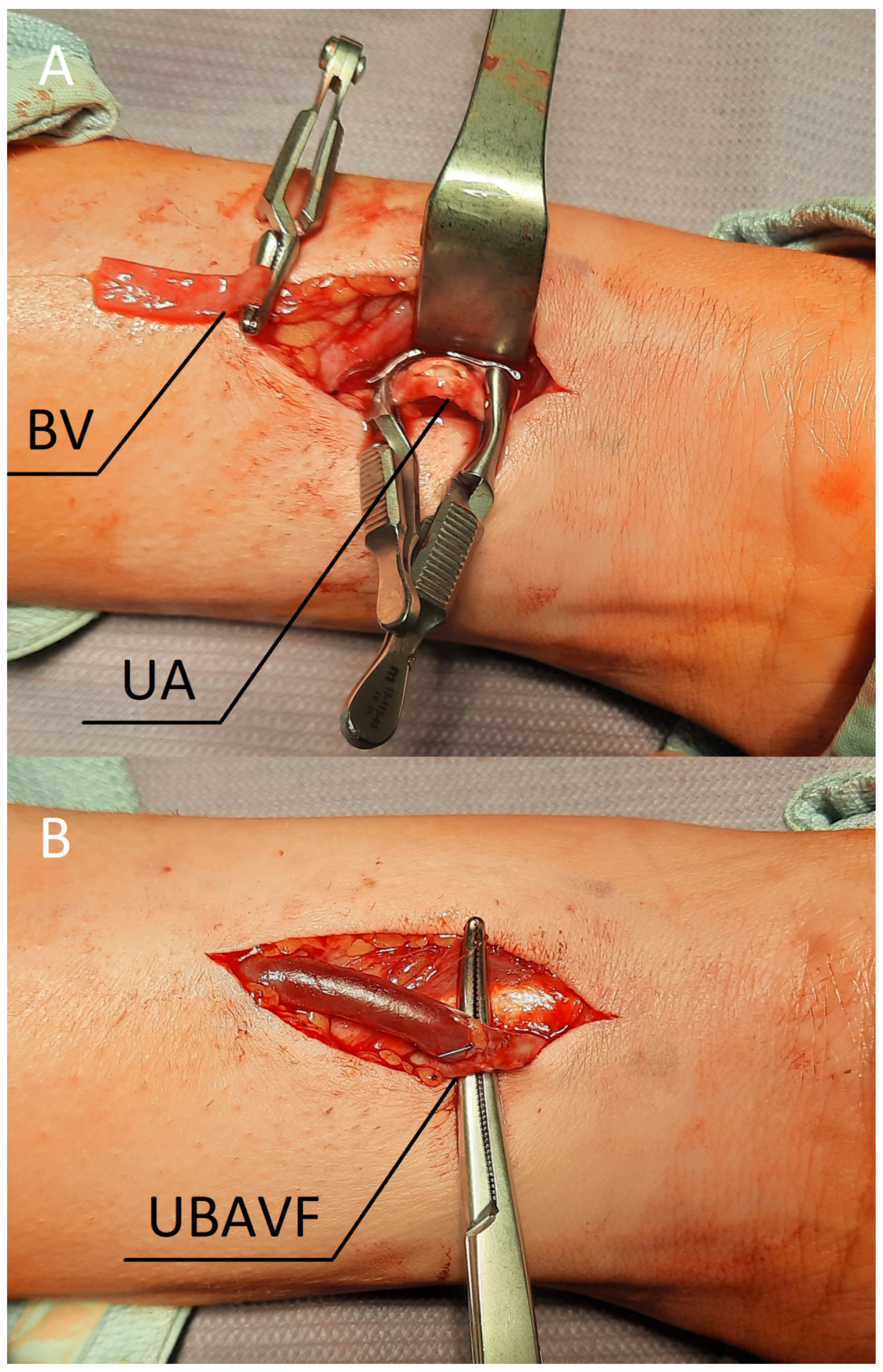
3. Procedure Description
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, C.T.; Blankestijn, P.J.; Dember, L.M.; Gallieni, M.; Harris, D.C.; Lok, C.; Mehrotra, R.; Stevens, P.E.; Wang, A.Y.-M.; Cheung, M.; et al. Dialysis initiation, modality choice, access, and prescription: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019, 96, 37–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson, J.S.; Carmody, M.; Keogh, B.; O’Dwyer, W.F. Access to circulation by permanent arteriovenous fistula in regular dialysis treatment. BMJ 1967, 4, 586–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinnaert, P.; Vereerstraeten, P.; Toussaint, C.; Van Geertruyden, J. Nine years’ experience with internal arteriovenous fistulas for haemodialysis: A study of some factors influencing the results. Br. J. Surg. 2005, 64, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Bourquelot, P.; Cussenot, O.; Corbi, P.; Pillion, G.; Gagnadoux, M.-F.; Bensman, A.; Loirat, C.; Broyer, M. Microsurgical creation and follow-up of arteriovenous fistulae for chronic haemodialysis in children. Pediatr. Nephrol. 1990, 4, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Schmidli, J.; Widmer, M.K.; Basile, C.; de Donato, G.; Gallieni, M.; Gibbons, C.P.; Haage, P.; Hamilton, G.; Hedin, U.; Kamper, L.; et al. Editor’s Choice–Vascular Access: 2018 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2018, 55, 757–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibeas, J.; Roca-Tey, R.; Vallespín, J.; Moreno, T.; Moñux, G.; Martí-Monrós, A.; Del Pozo, J.L.; Gruss, E.; De Arellano, M.R.; Fontseré, N.; et al. Spanish Clinical Guidelines on Vascular Access for Haemodialysis. Nefrologia 2017, 37 (Suppl. S1), 1–177. [Google Scholar] [CrossRef] [PubMed]
- Brescia, M.J.; Cimino, J.E.; Appel, K.; Hurwich, B.J. Chronic Hemodialysis Using Venipuncture and a Surgically Created Arteriovenous Fistula. N. Engl. J. Med. 1966, 275, 1089–1092. [Google Scholar] [CrossRef] [PubMed]
- Weyde, W.; Letachowicz, W.; Krajewska, M.K.; Letachowicz, K.; Watorek, E.; Kusztal, M.; Porazko, T.; Gołebiowski, T.; Madziarska, K.; Klinger, M. Native forearm fistulas utilizing the basilic vein: An underused type of vascular access. J. Nephrol. 2008, 21, 363–367. [Google Scholar] [PubMed]
- Zhen, Y.; Liu, P.; Ye, Z.; Zheng, X.; Ma, B.; Fan, G.; Yang, Y. Long-Term Results of Ulnar-Basilic Fistula Versus Radiocephalic Fistula for Maintenance Hemodialysis Access. Vasc. Endovasc. Surg. 2017, 51, 466–469. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Bera, S.; Goyal, V.D.; Gupta, V.; Bisht, N. Ulnar-Basilic Arteriovenous Fistula for Hemodialysis Access: Utility as the “Second Procedure” after Radio Cephalic Fistula. Ann. Vasc. Dis. 2021, 14, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Salgado, O.J.; Chacon, R.E.; Henriquez, C. Ulnar-basilic Fistula: Indications, Surgical Aspects, Puncture Technique, and Results. Artif. Organs 2004, 28, 634–638. [Google Scholar] [CrossRef]
- Bourquelot, P.; Van-Laere, O.; Baaklini, G.; Turmel-Rodrigues, L.; Franco, G.; Gaudric, J.; Raynaud, A. Placement of wrist ulnar-basilic autogenous arteriovenous access for hemodialysis in adults and children using microsurgery. J. Vasc. Surg. 2011, 53, 1298–1302. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gołębiowski, T.; Jerzak, P.; Letachowicz, K.; Konieczny, A.; Kusztal, M.; Gołębiowski, M.; Banasik, M.; Sznajder, K.; Krajewska, M. Prone Position Facilitates Creation of Ulnar-Basilic Arteriovenous Fistula. J. Clin. Med. 2022, 11, 2610. https://doi.org/10.3390/jcm11092610
Gołębiowski T, Jerzak P, Letachowicz K, Konieczny A, Kusztal M, Gołębiowski M, Banasik M, Sznajder K, Krajewska M. Prone Position Facilitates Creation of Ulnar-Basilic Arteriovenous Fistula. Journal of Clinical Medicine. 2022; 11(9):2610. https://doi.org/10.3390/jcm11092610
Chicago/Turabian StyleGołębiowski, Tomasz, Patryk Jerzak, Krzysztof Letachowicz, Andrzej Konieczny, Mariusz Kusztal, Maciej Gołębiowski, Mirosław Banasik, Katarzyna Sznajder, and Magdalena Krajewska. 2022. "Prone Position Facilitates Creation of Ulnar-Basilic Arteriovenous Fistula" Journal of Clinical Medicine 11, no. 9: 2610. https://doi.org/10.3390/jcm11092610