
Effectiveness of an Active and Continuous Surveillance Program for Intensive Care Units Infections Based on the EPIC III (Extended Prevalence of Infection in Intensive Care) Approach

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Context
2.3. Data Collection
2.4. Operative Definitions
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Prevalence of Infections
3.2. Antibiotic Therapy
3.3. Clinical Outcomes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sakr, Y.; Jaschinski, U.; Wittebole, X.; Szakmany, T.; Lipman, J.; Ñamendys-Silva, S.A.; Martin-Loeches, I.; Leone, M.; Lupu, M.-N.; Vincent, J.-L.; et al. Sepsis in Intensive Care Unit Patients: Worldwide Data from the Intensive Care over Nations Audit. Open Forum Infect. Dis. 2018, 5, ofy313. [Google Scholar] [CrossRef] [PubMed]
- SepNet Critical Care Trials Group. Incidence of severe sepsis and septic shock in German intensive care units: The prospective, multicentre INSEP study. Intensive Care Med. 2016, 42, 1980–1989. [Google Scholar] [CrossRef] [PubMed]
- Baykara, N.; Sepsis Study Group; Akalın, H.; Arslantaş, M.K.; Hancı, V.; Çağlayan, Ç.; Kahveci, F.; Demirağ, K.; Baydemir, C.; Ünal, N. Epidemiology of sepsis in intensive care units in Turkey: A multicenter, point-prevalence study. Crit. Care 2018, 22, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Qian, C.; Zhao, M.; Yu, X.; Kang, Y.; Ma, X.; Ai, Y.; Xu, Y.; Liu, D.; An, Y.; et al. Epidemiology and outcome of severe sepsis and septic shock in intensive care units in mainland China. PLoS ONE 2014, 9, e107181. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.; Dalfior, L., Jr.; Fernandes Hda, S.; Moreno, R.; Vincent, J.L. Prevalence and outcomes of infections in Brazilian ICUs: A subanalysis of EPIC II study. Prevalência e desfechos clínicos de infecções em UTIs brasileiras: Subanálise do estudo EPIC II. Rev. Bras. Ter. Intensiva 2012, 24, 143–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agodi, A.; Barchitta, M.; Auxilia, F. Epidemiology of intensive care unit-acquired sepsis in Italy: Results of the SPIN-UTI network. Ann. Ig. 2018, 30 (Suppl. 2), 15–21. [Google Scholar] [CrossRef]
- Migliara, G.; Di Paolo, C.; Barbato, D. Multimodal surveillance of healthcare associated infections in an intensive care unit of a large teaching hospital. Ann. Ig. 2019, 31, 399–413. [Google Scholar] [CrossRef]
- Reinhart, K.; Daniels, R.; Kissoon, N.; Machado, F.R.; Schachter, R.D.; Finfer, S. Recognizing Sepsis as a Global Health Priority—A WHO Resolution. N. Engl. J. Med. 2017, 377, 414–417. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Sakr, Y.; Singer, M.; Martin-Loeches, I.; Machado, F.R.; Marshall, J.C.; Finfer, S.; Pelosi, P.; Brazzi, L.; Aditianingsih, D.; et al. Prevalence and Outcomes of Infection Among Patients in Intensive Care Units in 2017. JAMA 2020, 323, 1478–1487. [Google Scholar] [CrossRef]
- Li, Z.-J.; Wang, K.-W.; Liu, B.; Zang, F.; Zhang, Y.; Zhang, W.-H.; Zhou, S.-M.; Zhang, Y.-X. The Distribution and Source of MRDOs Infection: A Retrospective Study in 8 ICUs, 2013–2019. Infect. Drug Resist. 2021, 14, 4983–4991. [Google Scholar] [CrossRef]
- Saito, H.; Kilpatrick, C.; Pittet, D. The 2018 World Health Organization SAVE LIVES: Clean Your Hands Campaign targets sepsis in health care. Intensive Care Med. 2018, 44, 499–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markwart, R.; Saito, H.; Harder, T.; Tomczyk, S.; Cassini, A.; Fleischmann-Struzek, C.; Reichert, F.; Eckmanns, T.; Allegranzi, B. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: A systematic review and meta-analysis. Intensive Care Med. 2020, 46, 1536–1551. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/bitstream/handle/10665/80135/9789241501507_eng.pdf (accessed on 16 March 2022).
- Suetens, C.; Latour, K.; Kärki, T.; Ricchizzi, E.; Kinross, P.; Moro, M.L.; Jans, B.; Hopkins, S.; Hansen, S.; Lyytikäinen, O.; et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: Results from two European point prevalence surveys, 2016 to 2017. Euro Surveill. 2018, 23, 1800516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreiber, P.W.; Sax, H.; Wolfensberger, A.; Clack, L.; Kuster, S.P. The preventable proportion of healthcare-associated infections 2005-2016: Systematic review and meta-analysis. Infect. Control Hosp. Epidemiol. 2018, 39, 1277–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann, M.C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K.; International Forum of Acute Care Trialists. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef]
- Finazzi, S.; Paci, G.; Antiga, L.; Brissy, O.; Carrara, G.; Crespi, D.; Csato, G.; Csomos, A.; Duek, O.; Facchinetti, S.; et al. PROSAFE: A European endeavor to improve quality of critical care medicine in seven countries. Minerva Anestesiol. 2020, 86, 1305–1320. [Google Scholar] [CrossRef]
- Weist, K.; Högberg, L.D. ECDC publishes 2015 surveillance data on antimicrobial resistance and antimicrobial consumption in Europe. Eurosurveillance 2016, 21, 30401. [Google Scholar] [CrossRef]
- Serra-Burriel, M.; Campillo-Artero, C.; Agodi, A.; Barchitta, M.; López-Casasnovas, G. Association between antibiotic resistance in intensive care unit (ICU)-acquired infections and excess resource utilization: Evidence from Spain, Italy, and Portugal. Infect. Control Hosp. Epidemiol. 2021. [Google Scholar] [CrossRef]
- Plachouras, D.; Lepape, A.; Suetens, C. ECDC definitions and methods for the surveillance of healthcare-associated infections in intensive care units. Intensive Care Med. 2018, 44, 2216–2218. [Google Scholar] [CrossRef] [Green Version]
- Yin, M.; Tambyah, P.A.; Perencevich, E.N. Infection, Antibiotics, and Patient Outcomes in the Intensive Care Unit. JAMA 2020, 323, 1451–1452. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.-L.; Bihari, D.J.; Suter, P.M.; Bruining, H.A.; White, J.; Nicolas-Chanoin, M.-H.; Wolff, M.; Spencer, R.C.; Hemmer, M. The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. EPIC International Advisory Committee. JAMA 1995, 274, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Rello, J.; Marshall, J.K.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Antimicrobial consumption. In ECDC Annual Epidemiological Report for 2017; ECDC: Stockholm, Sweden, 2018; Available online: http://ecdc.europa.eu/sites/portal/files/documents/AER_for_2017-antimicrobial-consumption.pdf (accessed on 16 March 2022).
- Secondo Studio di Prevalenza Italiano Sulle Infezioni Correlate All’assistenza e Sull’Uso di Antibiotici Negli Ospedali per Acuti—Protocollo ECDC. Dipartimento Scienze Della Salute Pubblica e Pediatriche Università di Torino. 2018. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2791_allegato.pdf (accessed on 16 March 2022).
- Antonioli, P.; Bolognesi, N.; Valpiani, G.; Morotti, C.; Bernardini, D.; Bravi, F.; Di Ruscio, E.; Stefanati, A.; Gabutti, G. A 2-year point-prevalence surveillance of healthcare-associated infections and antimicrobial use in Ferrara University Hospital, Italy. BMC Infect. Dis. 2020, 20, 75. [Google Scholar] [CrossRef]
- Metsini, A.; Vazquez, M.; Sommerstein, R.; Marschall, J.; Voide, C.; Troillet, N.; Gardiol, C.; Pittet, D.; Zingg, W. Point prevalence of healthcare-associated infections and antibiotic use in three large Swiss acute-care hospitals. Swiss Med. Wkly. 2018, 148, w14617. [Google Scholar] [CrossRef] [Green Version]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Montrucchio, G.; Sales, G.; Corcione, S.; De Rosa, F.G.; Brazzi, L. Choosing wisely: What is the actual role of antimicrobial stewardship in Intensive Care Units? Minerva Anestesiol. 2019, 85, 71–82. [Google Scholar] [CrossRef]
- De Rosa, F.G.; Corcione, S.; Montrucchio, G.; Brazzi, L.; Di Perri, G. Antifungal Treatment Strategies in the ICU: Beyond Meta-analysis. Turk. J. Anaesthesiol. Reanim. 2016, 44, 283–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rosa, F.G.; Corcione, S.; Montrucchio, G.; Brazzi, L.; Di Perri, G. Appropriate Treatment of Invasive Candidiasis in ICU: Timing, Colonization Index, Candida Score & Biomarkers, Towards de-Escalation? Turk. J. Anaesthesiol. Reanim. 2016, 44, 279–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timsit, J.-F.; Bassetti, M.; Cremer, O.; Daikos, G.; De Waele, J.; Kallil, A.; Kipnis, E.; Kollef, M.; Laupland, K.; Paiva, J.-A.; et al. Rationalizing antimicrobial therapy in the ICU: A narrative review. Intensive Care Med. 2019, 45, 172–189. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Shorr, A.F.; Bassetti, M.; Timsit, J.-F.; Micek, S.T.; Michelson, A.P.; Garnacho-Montero, J. Timing of antibiotic therapy in the ICU. Crit. Care 2021, 25, 360. [Google Scholar] [CrossRef] [PubMed]
- Tabah, A.; Bassetti, M.; Kollef, M.H.; Zahar, J.-R.; Paiva, J.-A.; Timsit, J.-F.; Roberts, J.A.; Schouten, J.; Giamarellou, H.; Rello, J.; et al. Antimicrobial de-escalation in critically ill patients: A position statement from a task force of the European Society of Intensive Care Medicine (ESICM) and European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Critically Ill Patients Study Group (ESGCIP). Intensive Care Med. 2020, 46, 245–265. [Google Scholar] [CrossRef]


{kind=link}
| All Patients (n = 435) | Infection | p Value | |||
|---|---|---|---|---|---|
| No (n = 251) | Yes (n = 184) | ||||
| Age, year, mean (SD) | 57.5 (20.6) | 58 (21.2) | 57 (19.7) | 0.4069 | |
| Male, n (%) | 261 (60.0) | 141 (56.2) | 120 (65.2) | 0.0572 | |
| ICU, n (%) | General | 186 (42.8) | 108 (43.0) | 78 (42.4) | 0.9465 |
| Specialist | 219 (50.3) | 125 (49.8) | 94 (51.1) | ||
| Pediatric | 30 (6.9) | 18 (7.2) | 12 (6.5) | ||
| Type of admission, n (%) | Medical | 120 (27.6) | 46 (18.3) | 74 (40.2) | <0.001 * |
| Elective surgery | 158 (36.3) | 114 (45.4) | 44 (23.9) | ||
| Emergency surgery | 105 (24.1) | 59 (23.5) | 46 (25.0) | ||
| Trauma | 52 (12.0) | 32 (12.7) | 20 (10.9) | ||
| Reason for admission, n (%) | Respiratory | 57 (13.1) | 13 (5.2) | 44 (23.9) | <0.001 |
| Cardiovascular | 55 (12.6) | 19 (7.6) | 36 (19.6) | ||
| Neurological | 80 (18.4) | 46 (18.3) | 34 (18.5) | ||
| Trauma | 57 (13.1) | 32 (12.7) | 25 (13.6) | ||
| Surveillance | 154 (35.4) | 125 (49.8) | 29 (15.8) | ||
| Other | 32 (7.4) | 16 (6.4) | 16 (8.7) | ||
| Comorbidities, yes, n (%) | 274 (63.0) | 159 (63.3) | 115 (62.5) | 0.8566 | |
| Comorbidities, n (%) | Solid cancer | 100 (23.0) | 68 (15.6) | 32 (7.4) | 0.0175 * |
| Hematologic cancer | 7 (1.6) | 1 (0.4) | 6 (3.3) | 0.0452 * | |
| Diabetes Mellitus | 64 (14.7) | 42 (16.7) | 22 (12.0) | 0.1647 | |
| COPD | 54 12.4) | 21 (8.4) | 33 (17.9) | 0.0028 * | |
| Heart Failure, NYHA III/IV | 66 (15.2) | 36 (14.6) | 30 (16.3) | 0.5731 | |
| Previous cardiac disease | 73 (16.8) | 40 (15.9) | 33 (17.9) | 0.5816 | |
| Chronic kidney failure | 55 (12.6) | 29 (11.6) | 26 (14.1) | 0.4244 | |
| Immunosuppression | 38 (8.7) | 25 (10.0) | 13 (7.1) | 0.2908 | |
| Solid organ transplant | 39 (9.0) | 26 (10.4) | 13 (7.1) | 0.2349 | |
| SOFA, mean (SD) a | 5.5 (4.1) | 4.0 (3.2) | 7.4 (4.5) | <0.001 * | |
| Invasive ventilation, n (%) | 217 (49.9) | 96 (38.2) | 121 (65.8) | <0.001* | |
| Non-invasive ventilation, n (%) | 35 (8.0) | 21 (8.5) | 14 (7.7) | 0.7741 | |
| Tracheostomy, n (%) | 114 (26.2) | 51 (20.6) | 63 (34.2) | 0.0014 * | |
| Vasopressor use, yes, n (%) | 114 (26.2) | 50 (19.9) | 64 (34.8) | <0.001* | |
| CVC, n (%) | 372 (85.5) | 206 (83.4) | 166 (90.7) | 0.0171 * | |
| Urinary catheter, n (%) | 407 (93.6) | 234 (94.7) | 173 (95.1) | 0.7386 | |
| Renal replacement therapy, n (%) | 39 (9.0) | 11 (4.4) | 28 (15.2) | <0.001 * | |
| ECMO, n (%) | 8 (1.8) | 0 (0) | 8 (4.4) | <0.001 * | |
| Septic shock, n (%) | 69 (15.9) | 24 (9.6) | 45 (24.5) | <0.001 * | |
| Hyperlactacidemia, n (%) | 77 (17.7) | 37 (14.7) | 40 (21.7) | 0.0589 | |
| Antibiotic prophylaxis, n (%) | 149 (34.3) | 147 (58.6) | 2 (1.1) | <0.001 * | |
| Gastrointestinal decontamination, n (%) a | 25 (5.9) | 12 (4.9) | 13 (7.3) | 0.2934 | |
| Chlorhexidine, n (%) a | 175 (41.6) | 104 (42.4) | 71 (40.3) | 0.6651 | |
| ICU length of stay, days, median (IQR) a | 14 (4–36) | 4 (1–12) | 20 (10–33) | <0.001 * | |
| Hospital length of stay, median (IQR) a | 29 (15–54) | 11 (6–21) | 50 (22–65) | <0.001 * | |
| Mortality at 60 days, n (%) a | 52 (12.9) | 19 (7.9) | 33 (20.1) | <0.001 * | |
| Mode of Acquisition | |||||
|---|---|---|---|---|---|
| Infected Patients (n = 184) | Community-Acquired (n = 36) | Hospital-Acquired/Health Care-Associated (n = 41) | ICU-Acquired (n = 117) | ||
| Evidence of infection, n (%) | Certain | 108 (58.7) | 25 (69.4) | 22 (53.7) | 74 (63.2) |
| Probable | 44 (23.9) | 10 (27.8) | 8 (19.5) | 30 (25.6) | |
| Feasible | 52 (28.3) | 5 (13.9) | 20 (48.8) | 32 (27.4) | |
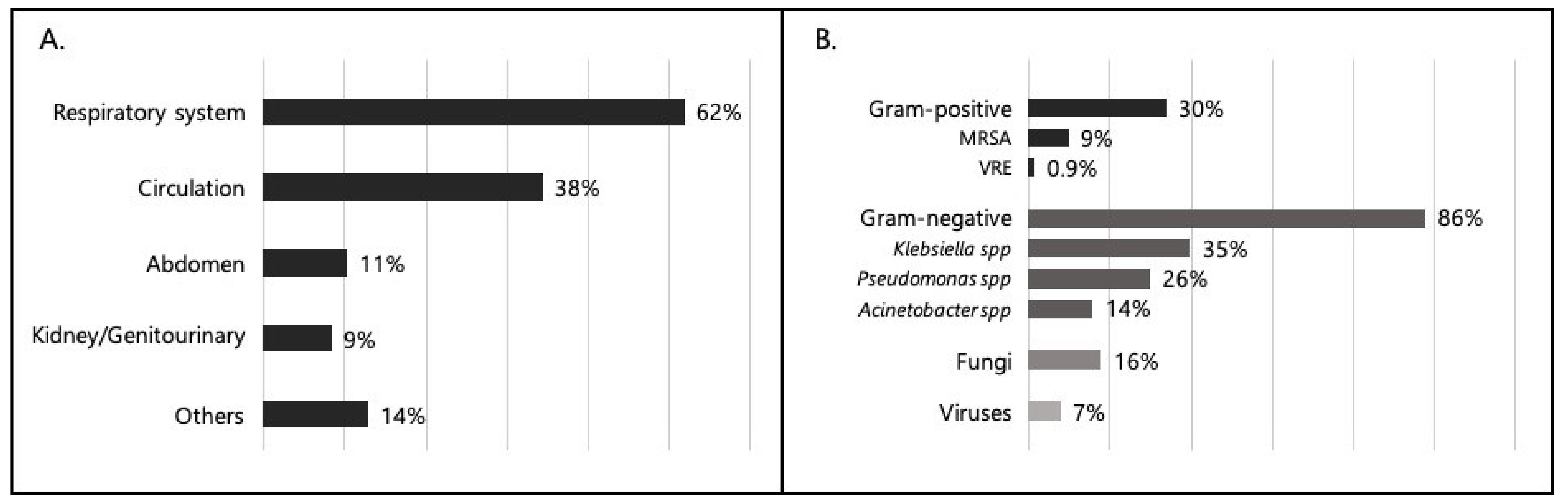
| Site of infection, n (%) | Respiratory system | 114 (62.0) | 23 (63.9) | 25 (61.0) | 77 (65.8) |
| Abdomen | 21 (11.4) | 3 (8.3) | 9 (22.0) | 10 (8.5) | |
| Circulation | 69 (37.5) | 11 (30.6) | 12 (29.3) | 56 (47.9) | |
| Kidney/genitourinary | 17 (9.2) | 2 (5.6) | 3 (7.3) | 14 (12.0) | |
| Others | 26 (14.1) | 6 (16.7) | 6 (14.6) | 14 (12.0) | |
| Colture-Positive Patients (n = 114) | Community-Acquired (n = 16) | Hospital-Acquired/Health Care-Associated (n = 23) | ICU-Acquired (n = 85) | ||
| Positive isolates, n (%) | Gram-positive | 34 (29.8) | 6 (37.5) | 8 (34.8) | 24 (28.2) |
| Gram-positive MS | 19 (16.7) | 5 (31.3) | 5 (21.7) | 12 (14.1) | |
| Gram-positive MDR | 17 (14.9) | 1 (6.3) | 5 (21.7) | 14 (16.5) | |
| Gram-negative | 98 (86.0) | 10 (62.5) | 17 (73.9) | 78 (91.8) | |
| Gram-negative MS | 69 (60.5) | 9 (56.3) | 9 (39.1) | 56 (65.9) | |
| Gram-negative MDR | 47 (41.2) | 2 (12.5) | 10 (43.5) | 39 (45.9) | |
| All MDR bacteria | 59 (51.8) | 3 (18.8) | 14 (60.9) | 48 (56.5) | |
| Fungi | 19 (16.7) | 5 (31.3) | 3 (13.0) | 14 (16.5) | |
| Viruses | 8 (7.0) | 5 (31.3) | 1 (4.3) | 4 (4.7) | |
| Klebsiella | 40 (35.1) | 3 (18.8) | 10 (43.5) | 30 (35.3) | |
| Pseudomonas | 30 (26.3) | 1 (6.3) | 2 (8.7) | 28 (32.9) | |
| Acinetobacter | 16 (14.0) | 0 (0) | 2 (8.7) | 15 (17.6) | |
| Bacteria resistant to Carbapenems | 36 (31.6) | 1 (6.3) | 8 (34.8) | 30 (35.3) | |
| All Patients (n = 403) | Mortality at 60 Days | p Value | |||
|---|---|---|---|---|---|
| Alive (n = 351) | Dead (n = 52) | ||||
| Antibiotic prophylaxis, n (%) | 141 (35.2) | 131 (37.4) | 10 (19.6) | 0.0107 * | |
| Positive isolates, n (%) | Gram-positive | 33 (8.2) | 30 (8.5) | 3 (5.8) | 0.7852 |
| Gram-positive MS | 19 (4.7) | 18 (5.1) | 1 (1.9) | 0.4891 | |
| Gram-positive MDR | 16 (4.0) | 14 (4.0) | 2 (3.8) | 1.0000 | |
| Gram-negative | 87 (21.6) | 76 (21.7) | 11 (21.2) | 0.9350 | |
| Gram-negative MS | 60 (14.9) | 52 (14.8) | 8 (15.4) | 0.9142 | |
| Gram-negative MDR | 42 (10.4) | 37 (10.5) | 5 (9.6) | 0.8384 | |
| All MDR bacteria | 54 (13.4) | 47 (13.4) | 7 (13.5) | 0.9888 | |
| Fungi | 16 (4.0) | 9 (2.6) | 7 (13.5) | 0.0018 * | |
| Viruses | 6 (1.5) | 5 (1.4) | 1 (1.9) | 0.5659 | |
| Klebsiella | 36 (8.9) | 35 (10.0) | 1 (1.9) | 0.0664 | |
| Pseudomonas | 28 (6.9) | 25 (7.1) | 3 (5.8) | 1.0000 | |
| Acinetobacter | 15 (3.7) | 13 (3.7) | 2 (3.8) | 1.0000 | |
| Bacteria resistant to Carbapenems | 32 (7.9) | 28 (8.0) | 4 (7.7) | 1.0000 | |
| Site of infection, n (%) | Respiratory system | 102 (25.3) | 80 (22.8) | 22 (42.3) | 0.0025 * |
| Abdomen | 16 (4.0) | 13 (3.7) | 3 (5.8) | 0.4460 | |
| Circulation | 56 (13.9) | 40 (11.4) | 16 (30.8) | 0.0002 * | |
| Kidney/genitourinary | 16 (4.0) | 13 (3.7) | 3 (5.8) | 0.4460 | |
| Others | 24 (6.0) | 21 (6.0) | 3 (5.8) | 1.0000 | |
| Acquisition mode, n (%) | Community-acquired | 30 (7.4) | 20 (5.7) | 10 (19.2) | 0.0022 * |
| Hospital-acquired /Health Care-associated | 36 (8.9) | 27 (7.7) | 9 (17.3) | 0.0344 * | |
| ICU-acquired | 106 (26.3) | 87 (24.8) | 19 (36.5) | 0.0724 | |
| (A) | |||
|---|---|---|---|
| Univariate | Multivariate | ||
| Variable | OR (95% CI) | OR (95% CI) | |
| Age | 1.00 (0.99–1.01) | 1.00 (0.99–1.01) | |
| Gender | Male | 1 (reference) | 1 (reference) |
| Female | 0.69 (0.47–1.02) | 0.92 (0.57–1.48)) | |
| Reason for admission | Respiratory | 1 (reference) | 1 (reference) |
| Cardiovascular | 0.56 (0.24–1.29) | 0.37 (0.15–0.92) | |
| Neurological | 0.22 (0.10–0.47) | 0.23 (0.10–0.53) | |
| Trauma | 0.23 (0.10–0.52) | 0.29 (0.12–0.68) | |
| Surveillance | 0.07 (0.03–0.15) | 0.07 (0.03–0.15) | |
| Other | 0.30 (0.12–0.75) | 0.25 (0.09–0.69) | |
| Invasive ventilation | 3.13 (2.11–4.66) | 2.14 (1.29–3.53) | |
| Vasopressor use | 2.19 (1.42–3.38) | 1.53 (0.86–2.73) | |
| CVC | 1.97 (1.10–3.54) | 1.37 (0.68–2.74) | |
| Renal replacement therapy | 3.90 (1.89–8.06) | 2.78 (1.30–5.96) | |
| COPD | 2.38 (1.33–4.28) | 2.15 (1.06–4.35) | |
| (B) | |||
| Variable | OR (95% CI) | OR (95% CI) | |
| Age | 1.04 (1.02–1.07) | 1.05 (1.02–1.08) | |
| Gender | Male | 1 (reference) | 1 (reference) |
| Female | 1.20 (0.66–2.16) | 2.20 (1.07–4.53) | |
| Source of admission | Operating room/Surgical department | 1 (reference) | 1 (reference) |
| Emergency department | 1.13 (0.51–2.48) | 1.03 (0.38–2.78) | |
| Medical department | 3.56 (1.53–8.26) | 3.69 (1.39–9.78) | |
| Other hospital | 0.86 (0.27–2.69) | 0.59 (0.15–2.35) | |
| Other ICUs | 2.01 (0.76–5.29) | 3.86 (1.16–12.84) | |
| Comorbidities | 11.53 (3.52–37.73) | 12.77 (2.91–56.02) | |
| Invasive ventilation | 4.71 (2.34–9.48) | 4.22 (1.91–9.30) | |
| Site of infection | Circulation | 3.56 (1.81–7.00) | 3.43 (1.48–7.97) |
| Acquisition mode | Community-acquired | 4.04 (1.77–9.22) | 9.90 (3.07–31.92) |
| All Patients (n = 403) | Mortality at 60 Days | p Value | |||
|---|---|---|---|---|---|
| Alive (n = 351) | Dead (n = 52) | ||||
| Age, year, mean (SD) | 57.5 (20.6) | 56.5 (22.9) | 66.6 (15.0) | <0.001 * | |
| Male, n (%) | 236 (58.6) | 208 (59.3) | 28 (53.8) | 0.4596 | |
| ICU, n (%) | General | 173 (42.9) | 146 (41.6) | 27 (51.9) | <0.001 * |
| Specialist | 203 (50.4) | 180 (51.3) | 23 (44.2) | ||
| Pediatric | 27 (6.7) | 25 (7.1) | 11 (3.8) | ||
| Type of admission, n (%) | Medical | 109 (27.0) | 87 (24.8) | 22 (42.3) | 0.0122 * |
| Surgical election | 151 (37.5) | 135 (38.5) | 16 (30.8) | ||
| Surgical emergency | 95 (23.6) | 82 (23.4) | 13 (25.0) | ||
| Trauma | 48 (11.9) | 47 (13.4) | 1 (21.9) | ||
| Reason for admission, n (%) | Respiratory | 52 (13.0) | 41 (11.7) | 11 (21.2) | <0.001 * |
| Cardiovascular | 50 (12.4) | 36 (10.3) | 14 (26.9) | ||
| Neurological | 72 (17.9) | 64 (18.2) | 8 (15.4) | ||
| Trauma | 53 (13.2) | 52 (14.8) | 1 (1.9) | ||
| Surveillance | 147 (36.2) | 134 (37.8) | 13 (25.0) | ||
| Other | 29 (7.2) | 24 (6.8) | 5 (17.2) | ||
| Comorbidities, yes, n (%) | 252 (62.5) | 204 (58.1) | 48 (92.3) | <0.001 * | |
| Comorbidities, n (%) | Solid cancer | 94 (23.3) | 77 (19.1) | 17 (4.2) | 0.0870 |
| Hematologic cancer | 6 (1.5) | 3 (0.9) | 3 (5.8) | 0.0306 * | |
| Diabetes Mellitus | 60 (14.9) | 50 (14.2) | 10 (19.2) | 0.3459 | |
| COPD | 50 (12.4) | 35 (10.0) | 15 (28.8) | <0.001 * | |
| Heart Failure, NYHA III/IV | 59 (14.6) | 46 (13.1) | 13 (25.0) | 0.0236 * | |
| Previous cardiac disease | 68 (16.9) | 47 (13.4) | 21 (40.4) | <0.001 * | |
| Chronic kidney failure | 48 (11.9) | 36 (10.3) | 12 (23.1) | 0.0077 * | |
| Immunosuppression | 36 (8.9) | 30 (8.5) | 6 (11.5) | 0.4405 | |
| Solid-organ transplant | 36 (8.9) | 31 (8.8) | 5 (9.6) | 0.7965 | |
| SOFA, mean (SD) a | 5.5 (4.1) | 4.5 (3.6) | 9.6 (4.1) | <0.001* | |
| Invasive ventilation, n (%) | 194 (48.1) | 153 (43.6) | 41 (78.8) | <0.001 * | |
| Non-invasive ventilation, n (%) | 33 (8.3) | 28 (8.1) | 5 (9.6) | 0.5971 | |
| Tracheostomy, n (%) | 101 (25.3) | 87 (25.0) | 14 (26.9) | 0.7401 | |
| Vasopressor use, yes, n (%) | 101 (25.1) | 75 (21.4) | 26 (50.0) | <0.001 * | |
| CVC, n (%) | 343 (86.0) | 294 (84.7) | 49 (94.2) | 0.0478 * | |
| Urinary catheter, n (%) | 376 (94.7) | 325 (94.2) | 51 (98.1) | 0.2300 | |
| Renal replacement therapy, n (%) | 36 (8.9) | 23 (6.6) | 13 (25.0) | <0.001 * | |
| ECMO, n (%) | 7 (1.8) | 6 (1.7) | 1 (1.9) | 1.0000 | |
| Septic shock, n (%) | 58 (14.4) | 42 (12.0) | 16 (30.8) | <0.001 * | |
| Hyperlactacidemia, n (%) | 64 (15.9) | 47 (13.4) | 17 (32.7) | <0.001 * | |
| ICU length of stay, days, median (IQR) a | 14 (4–35) | 14 (3–34) | 14 (8–45) | 0.2494 | |
| Hospital length of stay, median (IQR) a | 29 (16–54) | 28 (16–52) | 39 (14–68) | 0.4315 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montrucchio, G.; Sales, G.; Catozzi, G.; Bosso, S.; Scanu, M.; Vignola, T.V.; Costamagna, A.; Corcione, S.; Urbino, R.; Filippini, C.; et al. Effectiveness of an Active and Continuous Surveillance Program for Intensive Care Units Infections Based on the EPIC III (Extended Prevalence of Infection in Intensive Care) Approach. J. Clin. Med. 2022, 11, 2482. https://doi.org/10.3390/jcm11092482
Montrucchio G, Sales G, Catozzi G, Bosso S, Scanu M, Vignola TV, Costamagna A, Corcione S, Urbino R, Filippini C, et al. Effectiveness of an Active and Continuous Surveillance Program for Intensive Care Units Infections Based on the EPIC III (Extended Prevalence of Infection in Intensive Care) Approach. Journal of Clinical Medicine. 2022; 11(9):2482. https://doi.org/10.3390/jcm11092482
Chicago/Turabian StyleMontrucchio, Giorgia, Gabriele Sales, Giulia Catozzi, Stefano Bosso, Martina Scanu, Titty Vita Vignola, Andrea Costamagna, Silvia Corcione, Rosario Urbino, Claudia Filippini, and et al. 2022. "Effectiveness of an Active and Continuous Surveillance Program for Intensive Care Units Infections Based on the EPIC III (Extended Prevalence of Infection in Intensive Care) Approach" Journal of Clinical Medicine 11, no. 9: 2482. https://doi.org/10.3390/jcm11092482