
Cerebral Hypoperfusion Intensity Ratio Is Linked to Progressive Early Edema Formation

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
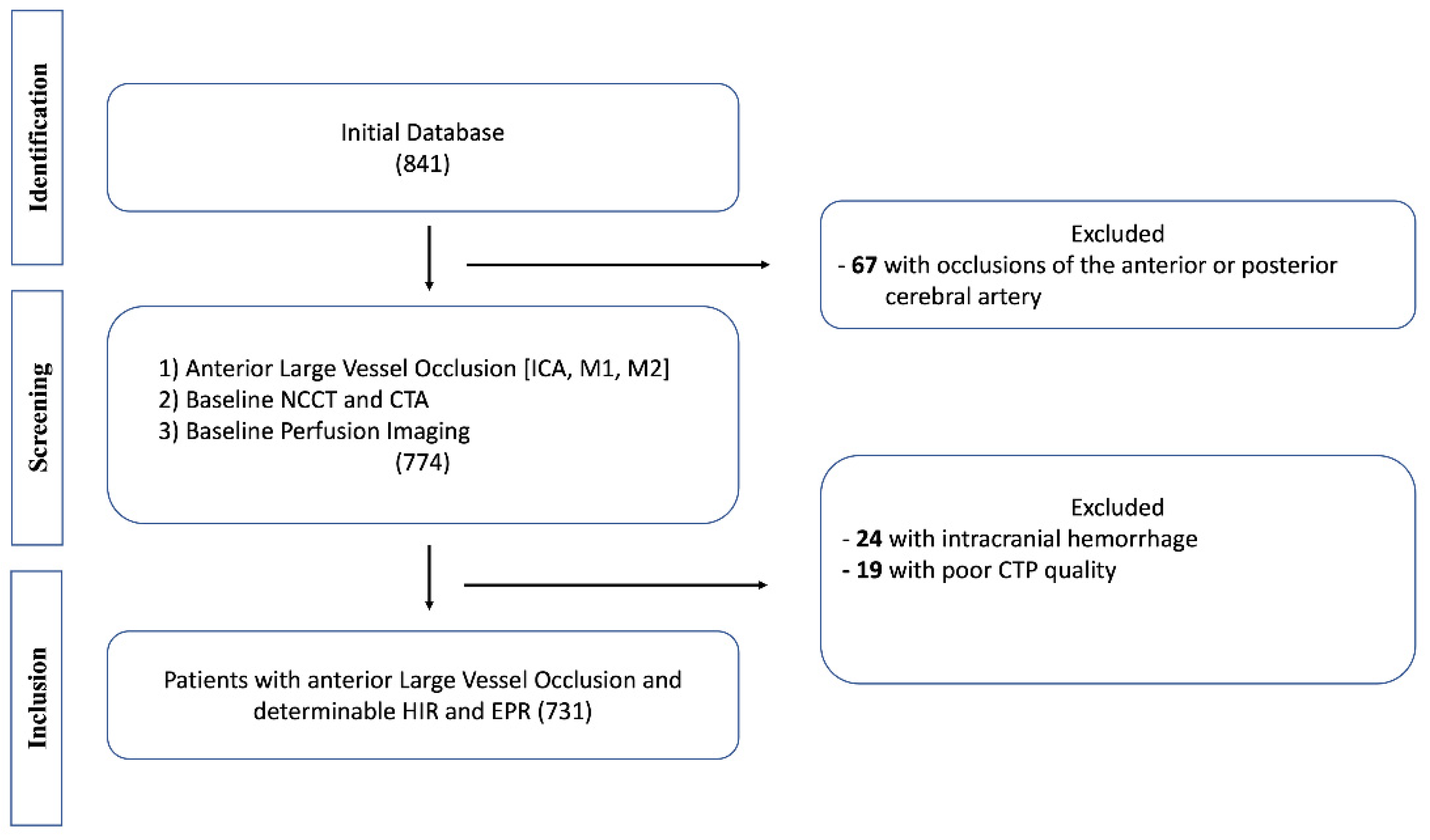
2.1. Study Design
2.2. Patient Inclusion, Population, and Clinical Data
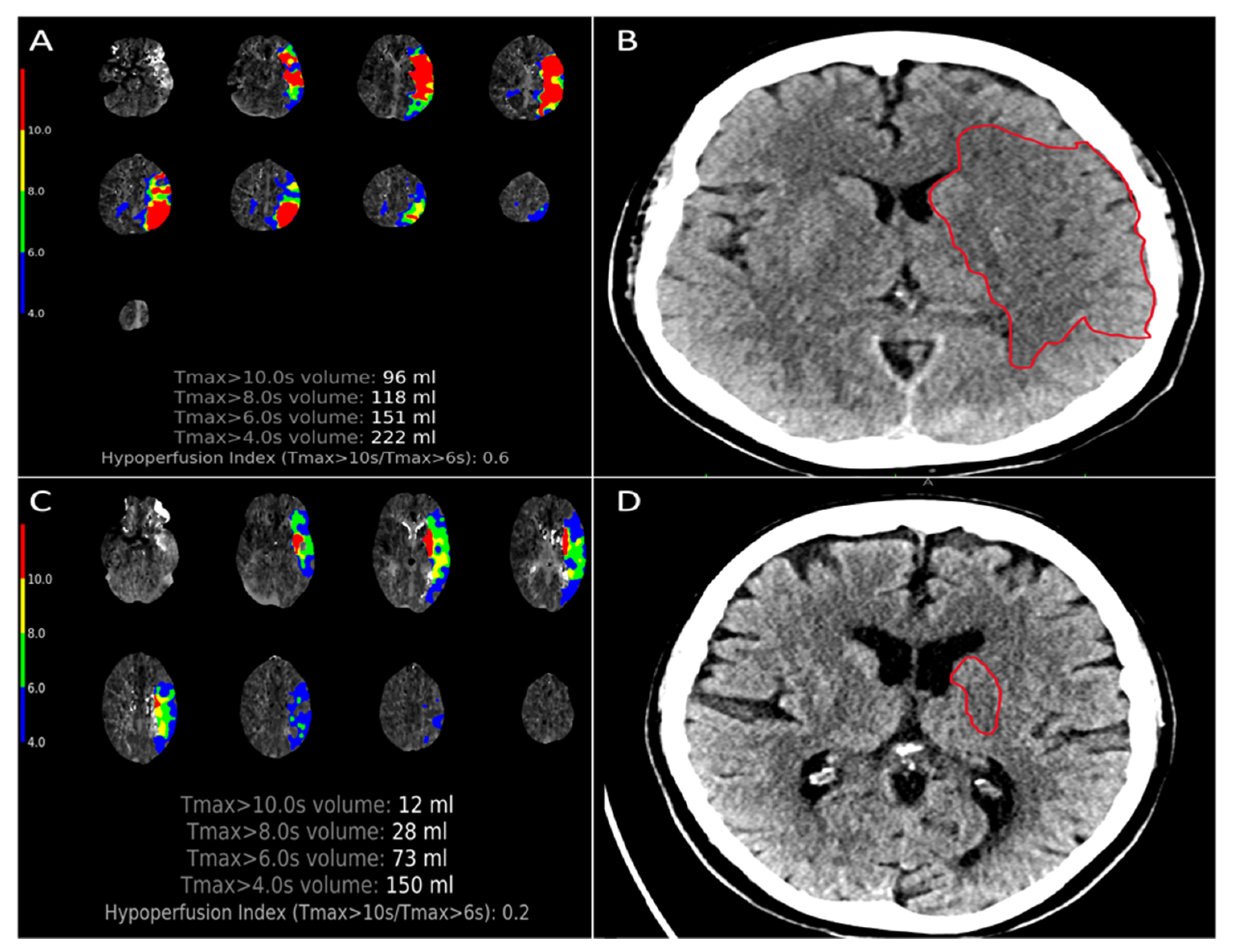
2.3. Imaging Analysis
2.4. Outcome Measures
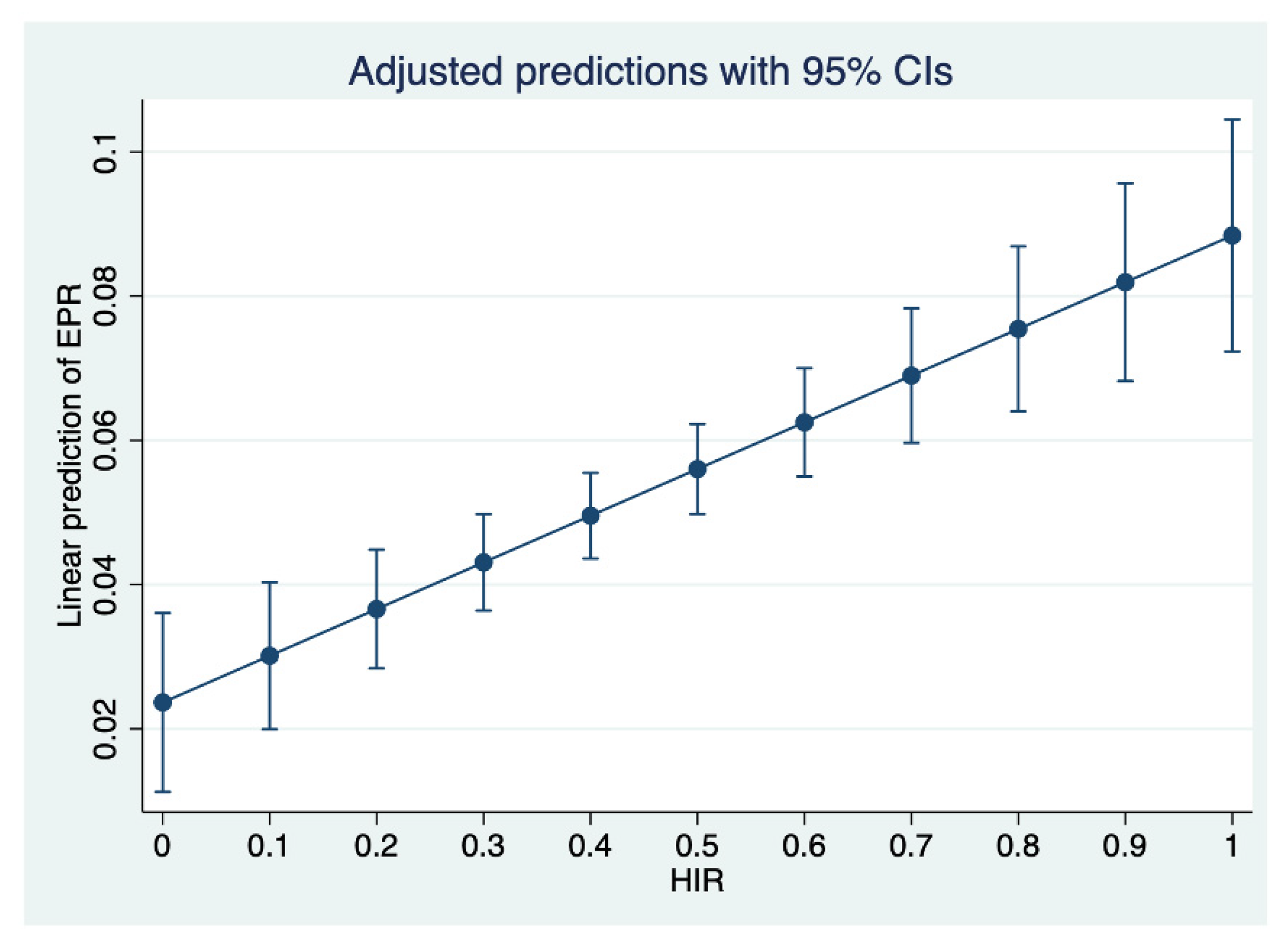
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Broocks, G.; Hanning, U.; Flottmann, F.; Schönfeld, M.; Faizy, T.D.; Sporns, P.B.; Baumgart, M.; Leischner, H.; Schön, G.; Minnerup, J.; et al. Clinical benefit of thrombectomy in stroke patients with low ASPECTS is mediated by oedema reduction. Brain 2019, 142, 1399–1407. [Google Scholar] [CrossRef] [PubMed]
- Broocks, G.; Flottmann, F.; Ernst, M.; Faizy, T.D.; Minnerup, J.; Siemonsen, S.; Fiehler, J.; Kemmling, A. Computed Tomography-Based Imaging of Voxel-Wise Lesion Water Uptake in Ischemic Brain: Relationship between Density and Direct Volumetry. Investig. Radiol. 2018, 53, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Broocks, G.; Flottmann, F.; Scheibel, A.; Aigner, A.; Faizy, T.D.; Hanning, U.; Leischner, H.; Broocks, S.I.; Fiehler, J.; Gellissen, S.; et al. Quantitative Lesion Water Uptake in Acute Stroke Computed Tomography Is a Predictor of Malignant Infarction. Stroke 2018, 49, 1906–1912. [Google Scholar] [CrossRef] [PubMed]
- Broocks, G.; Kniep, H.; Schramm, P.; Hanning, U.; Flottmann, F.; Faizy, T.; Schönfeld, M.; Meyer, L.; Schön, G.; Aulmann, L.; et al. Patients with low Alberta Stroke Program Early CT Score (ASPECTS) but good collaterals benefit from endovascular recanalization. J. Neurointerv. Surg. 2020, 12, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Nawabi, J.; Flottmann, F.; Hanning, U.; Bechstein, M.; Schön, G.; Kemmling, A.; Fiehler, J.; Broocks, G. Futile Recanalization with Poor Clinical Outcome Is Associated with Increased Edema Volume after Ischemic Stroke. Investig. Radiol. 2019, 54, 282–287. [Google Scholar] [CrossRef]
- Olivot, J.M.; Mlynash, M.; Inoue, M.; Marks, M.P.; Wheeler, H.M.; Kemp, S.; Straka, M.; Zaharchuk, G.; Bammer, R.; Lansberg, M.; et al. Hypoperfusion Intensity Ratio Predicts Infarct Progression and Functional Outcome in the DEFUSE 2 Cohort. Stroke 2014, 45, 1018–1023. [Google Scholar] [CrossRef] [Green Version]
- Faizy, T.D.; Kabiri, R.; Christensen, S.; Mlynash, M.; Kuraitis, G.; Broocks, G.; Hanning, U.; Nawabi, J.; Lansberg, M.G.; Marks, M.P.; et al. Perfusion imaging-based tissue-level collaterals predict ischemic lesion net water uptake in patients with acute ischemic stroke and large vessel occlusion. J. Cereb. Blood Flow Metab. 2021, 41, 2067–2075. [Google Scholar] [CrossRef]
- Guenego, A.; Fahed, R.; Albers, G.W.; Kuraitis, G.; Sussman, E.S.; Martin, B.W.; Marcellus, D.G.; Olivot, J.; Marks, M.P.; Lansberg, M.G.; et al. Hypoperfusion intensity ratio correlates with angiographic collaterals in acute ischaemic stroke with M1 occlusion. Eur. J. Neurol. 2020, 27, 864–870. [Google Scholar] [CrossRef]
- Guenego, A.; Marcellus, D.G.; Martin, B.W.; Christensen, S.; Albers, G.W.; Lansberg, M.G.; Marks, M.P.; Wintermark, M.; Heit, J.J. Hypoperfusion Intensity Ratio Is Correlated with Patient Eligibility for Thrombectomy. Stroke 2019, 50, 917–922. [Google Scholar] [CrossRef]
- Heit, J.J.; Mlynash, M.; Christensen, S.; Kemp, S.M.; Lansberg, M.G.; Marks, M.P.; Olivot, J.M.; Gregory, A.W. What predicts poor outcome after successful thrombectomy in late time windows? J. Neurointerv. Surg. 2021, 13, 421–425. [Google Scholar] [CrossRef]
- Guenego, A.; Mlynash, M.; Christensen, S.; Bs, S.K.; Heit, J.J.; Lansberg, M.G.; Albers, G.W. Hypoperfusion ratio predicts infarct growth during transfer for thrombectomy. Ann. Neurol. 2018, 84, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Faizy, T.D.; Kabiri, R.; Christensen, S.; Mlynash, M.; Kuraitis, G.M.; Broocks, G.; Flottmann, F.; Marks, M.P.; Lansberg, M.G.; Albers, G.W.; et al. Favorable Venous Outflow Profiles Correlate with Favorable Tissue-Level Collaterals and Clinical Outcome. Stroke 2021, 52, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Pexman, J.H.W.; Barber, P.A.; Hill, M.D.; Sevick, R.J.; Demchuk, A.M.; Hudon, M.E.; Hu, W.Y.; Buchan, A.M. Use of the Alberta Stroke Program Early CT Score (ASPECTS) for Assessing CT Scans in Patients with Acute Stroke. Am. J. Neuroradiol. 2001, 22, 1534–1542. [Google Scholar] [PubMed]
- Yeo, L.; Paliwal, P.; Teoh, H.; Seet, R.; Chan, B.; Ting, E.; Venketasubramanian, N.; Leow, W.; Wakerley, B.; Kusama, Y.; et al. Assessment of Intracranial Collaterals on CT Angiography in Anterior Circulation Acute Ischemic Stroke. Am. J. Neuroradiol. 2015, 36, 289–294. [Google Scholar] [CrossRef] [Green Version]
- Minnerup, J.; Broocks, G.; Kalkoffen, J.; Langner, S.; Knauth, M.; Psychogios, M.N.; Wersching, H.; Teuber, A.; Heindel, W.; Eckert, B.; et al. Computed tomography-based quantification of lesion water uptake identifies patients within 4.5 h of stroke onset: A multicenter observational study. Ann. Neurol. 2016, 80, 924–934. [Google Scholar] [CrossRef]
- Broocks, G.; Kemmling, A.; Meyer, L.; Nawabi, J.; Schön, G.; Fiehler, J.; Kniep, H.; Hanning, U. Computed Tomography Angiography Collateral Profile Is Directly Linked to Early Edema Progression Rate in Acute Ischemic Stroke. Stroke 2019, 50, 3424–3430. [Google Scholar] [CrossRef]
- Tan, J.C.; Dillon, W.P.; Liu, S.; Adler, F.; Smith, W.S.; Wintermark, M. Systematic comparison of perfusion-CT and CT-angiography in acute stroke patients. Ann. Neurol. 2007, 61, 533–543. [Google Scholar] [CrossRef]
- Faizy, T.D.; Heit, J.J. Rethinking the Collateral Vasculature Assessment in Acute Ischemic Stroke: The Comprehensive Collateral Cascade. Top. Magn. Reson. Imaging 2021, 30, 181–186. [Google Scholar] [CrossRef]
- Jansen, I.G.H.; van Vuuren, A.B.; van Zwam, W.H.; van den Wijngaard, I.R.; Berkhemer, O.A.; Lingsma, H.F.; Slump, C.H.; van Oostenbrugge, R.J.; Treurniet, K.M.; Dippel, D.W.J.; et al. Absence of Cortical Vein Opacification is Associated with Lack of Intra-arterial Therapy Benefit in Stroke. Radiology 2018, 286, 731. [Google Scholar] [CrossRef]
- Liebeskind, D.S. Imaging the collaterome: A stroke renaissance. Curr. Opin. Neurol. 2015, 28, 1–3. [Google Scholar] [CrossRef]
- Sheth, S.A.; Liebeskind, D.S. Collaterals in endovascular therapy for stroke. Curr. Opin. Neurol. 2015, 28, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Bang, O.Y.; Saver, J.L.; Buck, B.H.; Alger, J.R.; Starkman, S.; Ovbiagele, B.; Kim, D.; Jahan, R.; Duckwiler, G.R.; Yoon, S.R.; et al. Impact of collateral flow on tissue fate in acute ischaemic stroke. J. Neurol. Neurosurg. Psychiatry 2008, 79, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Liebeskind, D.S. Collaterals in Acute Stroke: Beyond the Clot. Neuroimaging Clin. N. Am. 2005, 15, 553–573. [Google Scholar] [CrossRef] [PubMed]
- Liebeskind, D.S. Collateral circulation. Stroke 2003, 34, 2279–2284. [Google Scholar] [CrossRef]
- Baek, J.H. Low Hypoperfusion Intensity Ratio Is Associated with a Favorable Outcome even in Large Ischemic Core and Delayed Recanalization Time. J. Clin. Med. 2021, 10, 1869. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| HIR+ (n = 381) | HIR− (n = 350) | p-Value | |
|---|---|---|---|
| Age (years), median (IQR) | 75 (64–82) | 76 (64–84) | 0.562 |
| Female | 200 (52.2) | 176 (50.3) | 0.551 |
| Medical History | |||
| Arterial Fibrillation | 146 (38.1) | 141 (40.3) | 0.645 |
| Hypertension | 248 (64.8) | 256 (73.1) | 0.024 |
| Blood Glucose, median (IQR) | 120 (105–146) | 123 (104–148) | 0.657 |
| Diabetes Mellitus | 66 (18.9) | 85 (22.2) | 0.235 |
| Smoking | |||
| Current Smoker | 42 (11) | 41 (11.7) | 0.997 |
| Never Smoked | 245 (64) | 246 (70.3) | 0.571 |
| Prior Smoker | 61 (15.9) | 53 15.1) | 0.494 |
| Unknown Smoking Status | 33 (8.7) | 10 (2.9) | |
| Stroke Presentation Details | |||
| Presentation NIHSS, median (IQR) | 12 (7–17) | 17 (13–20) | <0.001 |
| Time from Symptom Onset to i.v. tPA in min, median (IQR) | 95 (73–164) | 108 (66–150) | 0.838 |
| Time from Symptom Onset to imaging, min, median (IQR) | 197 (100–396) | 160 (86–335) | 0.61 |
| Treatment Details | |||
| Intravenous tPA Details | |||
| i.v. tPA Administration | 198 (51.7) | 168 (48) | 0.343 |
| Endovascular Treatment Details | |||
| Treated by endovascular thrombectomy | 342 (89.8) | 348 (99.4) | 0.58 |
| Recanalization after thrombectomy (TICI 2b-3) | 287 (83.9) | 270 (77.5) | 0.01 |
| Vessel Recanalization by tPA, Thrombectomy or Spontaneous | 305 (79.6) | 248 (70.9) | 0.001 |
| HIR+ (n = 381) | HIR− (n = 350) | p Value | |
|---|---|---|---|
| ASPECTS, median (IQR) | 8 (7–10) | 7 (6–8) | <0.001 |
| Baseline Infarct Core Volume [CBF < 30%] (mL), median (IQR) | 0 (0–10) | 31 (13–64) | <0.001 |
| Penumbra Tmax > 6 s volume (mL), median (IQR) | 90.5 (54.5–140) | 145 (88–197) | <0.001 |
| Penumbra Tmax > 10 s volume (mL), median (IQR) | 20.8 (8–45.2) | 89.6 (49.7–126) | <0.001 |
| NWU on admission (%), median (IQR) | 4 (2.1–7.6) | 8.2 (6–10.4) | <0.001 |
| Early Edema Progression Rate, (%/h), median (IQR) | 0.96 (0.42–2.4) | 2.64 (1.26–5.34) | <0.001 |
| Hypoperfusion intensity ratio (HIR), median (IQR) | 0.2 (0.1–0.3) | 0.6 (0.5–0.7) | <0.001 |
| Favorable CTA collaterals (TAN) | 304 (79.4) | 195 (55.7) | <0.001 |
| Vessel occlusion localization on CTA | |||
| Internal carotid artery | 60 (15.7) | 87 (24.9) | 0.004 |
| Proximal MCA 1 segment occlusion | 119 (31.1) | 153 (43.7) | <0.001 |
| Distal MCA 1 segment occlusion | 103 (26.9) | 59 (16.9) | 0.001 |
| MCA 2 segment occlusion | 96 (25.1) | 51 (14.6) | 0.001 |
| Long-term clinical outcome | |||
| Modified Ranking Scale after 90 days, median (IQR) | 2 (1–5) | 4 (3–6) | <0.001 |
| Unknown | 19 (5) | 8 (2.3) |
| Early Edema Progression Rate | |||
|---|---|---|---|
| Predictors | β | SE | p-Value |
| Favorable HIR | 0.53 | 0.017 | 0.003 |
| Presentation NIHSS | 0.2 | 0.0006 | 0.001 |
| Baseline ASPECTS | −0.11 | 0.002 | 0.551 |
| Favorable TAN collaterals | −0.46 | 0.0083 | 0.579 |
| Proximal vessel occlusion | 0.03 | 0.0034 | 0.349 |
| Blood glucose | 0.00036 | 0 | 0.62 |
| Age | 0.0013 | 0.0002 | 0.604 |
| Sex | −0.0084 | 0.007 | 0.229 |
| Observations n = 701 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Horn, N.; Broocks, G.; Kabiri, R.; Kraemer, M.C.; Christensen, S.; Mlynash, M.; Meyer, L.; Lansberg, M.G.; Albers, G.W.; Sporns, P.; et al. Cerebral Hypoperfusion Intensity Ratio Is Linked to Progressive Early Edema Formation. J. Clin. Med. 2022, 11, 2373. https://doi.org/10.3390/jcm11092373
van Horn N, Broocks G, Kabiri R, Kraemer MC, Christensen S, Mlynash M, Meyer L, Lansberg MG, Albers GW, Sporns P, et al. Cerebral Hypoperfusion Intensity Ratio Is Linked to Progressive Early Edema Formation. Journal of Clinical Medicine. 2022; 11(9):2373. https://doi.org/10.3390/jcm11092373
Chicago/Turabian Stylevan Horn, Noel, Gabriel Broocks, Reza Kabiri, Michel C. Kraemer, Soren Christensen, Michael Mlynash, Lukas Meyer, Maarten G. Lansberg, Gregory W. Albers, Peter Sporns, and et al. 2022. "Cerebral Hypoperfusion Intensity Ratio Is Linked to Progressive Early Edema Formation" Journal of Clinical Medicine 11, no. 9: 2373. https://doi.org/10.3390/jcm11092373