
Co-Sleeping as a Protector against Malocclusion in the Primary Dentition: A Cross-Sectional Study

 , ,
, ,
Abstract
:1. Introduction
- -
- To assess whether the practice of co-sleeping is influenced by sociodemographic variables;
- -
- To analyze whether the practice of co-sleeping has an impact on non-nutritive sucking habits, their duration and frequency;
- -
- To study whether the coincidence between the onset of these habits and the time of weaning is greater in subjects who do not co-sleep;
- -
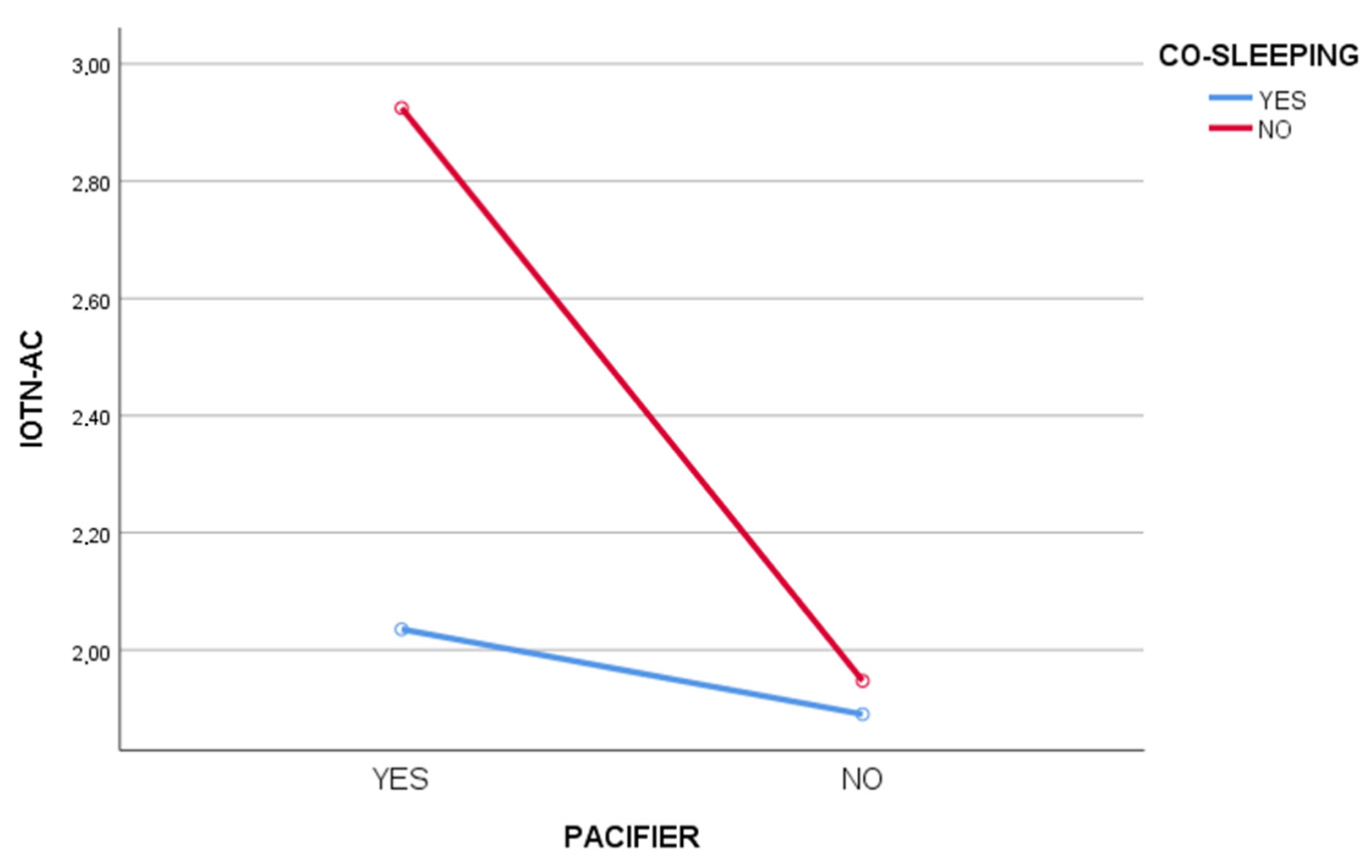
- To investigate whether co-sleeping alters the relationship between non-nutritive sucking habits and malocclusion in children who are weaned early.
2. Materials and Methods
2.1. Study Design and Setting
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Analysis
3.2. Co-Sleeping and Habits
3.3. Breastfeeding and Malocclusion
4. Discussion
5. Conclusions
- -
- Co-sleeping is not influenced by sociodemographic variables.
- -
- Children who practice co-sleeping appear to have a lower frequency and duration of non-nutritive sucking habits.
- -
- In addition, co-sleeping may contribute to a reduced development of malocclusions.
- -
- Co-sleeping appears to act as a moderator in the relationship between non-nutritive sucking habits and malocclusion.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Academy of Pediatric Dentistry. Management of the developing dentition and occlusion in pediatric dentistry. In The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2019; pp. 362–378. [Google Scholar]
- Stahl, F.; Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. Longitudinal growth changes in untreated subjects with Class II Division 1 malocclusion. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Klocke, A.; Nanda, R.S.; Kahl-Nieke, B. Anterior open bite in the deciduous dentition: Longitudinal follow-up and craniofacial growth considerations. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Peres, K.G.; Barros, A.J.D.; Peres, M.A.; Victora, C.G. Effects of breastfeeding and sucking habits on malocclusion in a birth cohort study. Rev. Saúde. Pública. 2007, 41, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.T.; Marquezan, M.; Verma, S.K.; Maheshwari, S.; Zahid, S.N.; Chaudhary, P.K. Neuromuscular dentistry: Occlusal diseases and posture. J. Oral Biol. Craniofacial Res. 2013, 3, 146–150. [Google Scholar] [CrossRef] [Green Version]
- Marquezan, M.; Faraco-Junior, I.M.; Feldens, C.A.; Kramer, P.F.; Ferreira, S.H. Association between occlusal anomalies and dental caries in 3- to 5 year-old Brazilian children. J. Orthod. 2011, 38, 8–14. [Google Scholar] [CrossRef]
- Tristão, S.K.P.C.; Magno, M.B.; Pintor, A.V.B.; Christovam, I.F.O.; Ferreira, D.M.T.P.; Maia, L.C.; De Souza, I.P.R. Is there a relationship between malocclusion and bullying? A systematic review. Prog. Orthod. 2020, 21, 26. [Google Scholar] [CrossRef]
- Dimberg, L.; Arnrup, K.; Bondemark, L. The impact of malocclusion on the quality of life among children and adolescents: A systematic review of quantitative studies. Eur. J. Orthod. 2014, 37, 238–247. [Google Scholar] [CrossRef]
- Lombardo, G.; Vena, F.; Negri, P.; Pagano, S.; Barilotti, C.; Paglia, L.; Colombo, S.; Orso, M.; Cianetti, S. Worldwide prevalence of malocclusion in the different stages of dentition: A systematic review and meta-analysis. Eur. J. Paediatr. Dent. 2020, 21, 115–123. [Google Scholar] [CrossRef]
- Pegoraro, N.A.; dos Santos, C.M.; Colvara, B.C.; Rech, R.S.; Faustino-Silva, D.D.; Hugo, F.N.; Hilgert, J.B. Prevalence of malocclusion in early childhood and its associated factors in a primary care service in Brazil. CoDAS 2022, 34, e20210007. [Google Scholar] [CrossRef]
- Zina, L.; Saliba, N.A.; Saliba, O.; Suzely, A.M. Association between breast-feeding practices and sucking habits: A cross-sectional study of children in their first year of life. J. Indian Soc. Pedod. Prev. Dent. 2008, 26, 102–106. [Google Scholar] [CrossRef]
- Kasparaviciene, K.; Sidlauskas, A.; Zasciurinskiene, E.; Vasiliauskas, A.; Juodzbalys, G.; Mantas Sidlauskas, M.; Marmaite, U. The prevalence of malocclusion and oral habits among 5–7-year-old children. Med Sci. Monit. 2014, 20, 2036–2042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero, C.C.; Scavone-Junior, H.; Garib, D.G.; Cotrim-Ferreira, F.A.; Ferreira, R.I. Breastfeeding and non-nutritive sucking patterns related to the prevalence of anterior open bite in primary dentition. J. Appl. Oral Sci. 2011, 19, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Molins, M.; Grau, J.C.; Lischeid, C.G.; Ustrell, J.T. Comparative study of the craniofacial growth depending on the type of lactation received. Eur. J. Paediatr. Dent. 2010, 11, 87–92. [Google Scholar]
- Luz, C.L.; Garib, D.G.; Arouca, R. Association between breastfeeding duration and mandibular retrusion: A cross-sectional study of children in the mixed dentition. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 531–534. [Google Scholar] [CrossRef]
- Kobayashi, H.M.; Scavone, H.; Ferreira, R.I.; Garib, D. Relationship between breastfeeding duration and prevalence of posterior crossbite in the deciduous dentition. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 54–58. [Google Scholar] [CrossRef]
- Peres, K.G.; Cascaes, A.M.; Peres, M.A.; Demarco, F.F.; Santos, I.S.; Matijasevich, A.; Barros, A.J. Exclusive Breastfeeding and Risk of Dental Malocclusion. Pediatrics 2015, 136, e60–e67. [Google Scholar] [CrossRef] [Green Version]
- Abreu, L.G.; Paiva, S.M.; Pordeus, I.A.; Martins, C.C. Breastfeeding, bottle feeding and risk of malocclusion in mixed and permanent dentitions: A systematic review. Braz. Oral Res. 2016, 30, S1806-83242016000100401. [Google Scholar] [CrossRef] [Green Version]
- D’Onofrio, L. Oral dysfunction as a cause of malocclusion. Orthod. Craniofacial Res. 2019, 22 (Suppl. S1), 43–48. [Google Scholar] [CrossRef]
- Al-Haj Ali, S.N.; Alsineedi, F.; Alsamari, N.; Alduhayan, G.; BaniHani, A.; Farah, R.I. Risk factors of early childhood caries among preschool children in eastern Saudi Arabia. Sci. Prog. 2021, 104, 2. [Google Scholar] [CrossRef]
- Thomaz, E.B.A.F.; Cangussu, M.C.T.; Assis, A.M.O. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: A multivariate analysis. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 500–506. [Google Scholar] [CrossRef]
- Peres, K.; Chaffee, B.; Feldens, C.A.; Flores-Mir, C.; Moynihan, P.; Rugg-Gunn, A. Breastfeeding and oral health: Evidence and methodological challenges. J. Dent. Res. 2017, 97, 251–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes-Freire, G.M.; Cárdenas, A.B.C.; De Deza, J.E.E.S.; Ustrell-Torrent, J.M.; Oliveira, L.B.; Quesada, J.R. Exploring the association between feeding habits, non-nutritive sucking habits, and malocclusions in the deciduous dentition. Prog. Orthod. 2015, 16, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, S.S.; Nehra, K.; Sharma, M.; Jayan, B.; Poonia, A.; Bhattal, H. Association between breastfeeding duration, non-nutritive sucking habits and dental arch dimensions in deciduous dentition: A cross-sectional study. Prog. Orthod. 2014, 15, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crittenden, A.N.; Samson, D.R.; Herlosky, K.N.; Mabulla, I.A.; Mabulla, A.Z.; McKenna, J.J. Infant co-sleeping patterns and maternal sleep quality among Hadza hunter-gatherers. Sleep Health 2018, 4, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Ward, T.C.S. Reasons for mother–infant bed-sharing: A systematic narrative synthesis of the literature and implications for future research. Matern. Child Health J. 2014, 19, 675–690. [Google Scholar] [CrossRef]
- Barry, E.S. Co-sleeping as a proximal context for infant development: The importance of physical touch. Infant Behav. Dev. 2019, 57, 101385. [Google Scholar] [CrossRef] [PubMed]
- Beijers, R.; Riksen-Walraven, J.M.; De Weerth, C. Cortisol regulation in 12-month-old human infants: Associations with the infants’ early history of breastfeeding and co-sleeping. Stress 2012, 16, 267–277. [Google Scholar] [CrossRef]
- Da Costa, C.T.; Shqair, A.Q.; Azevedo, M.S.; Goettems, M.L.; Bonow, M.L.M.; Romano, A.R. Pacifier use modifies the association between breastfeeding and malocclusion: A cross-sectional study. Braz. Oral Res. 2018, 32, e101. [Google Scholar] [CrossRef]
- Rochelle, I.M.F.; da Silva, E.P.; Pereira, A.C.; Meneghim, M.C.; Nóbilo, K.A.; Bovi, G.M. Breastfeeding, deleterious oral habits and malocclusion in 5-year-old children in São Pedro, SP, Brazil. Dent. Press J. Orthod. 2010, 15, 71–81. [Google Scholar] [CrossRef] [Green Version]
- Brook, P.H.; Shaw, W.C. The development of an index of orthodontic treatment priority. Eur. J. Orthod. 1989, 11, 309–320. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Xia, B.; Ge, L. Effects of breast-feeding duration, bottle-feeding duration and non-nutritive sucking habits on the occlusal characteristics of primary dentition. BMC Pediatr. 2015, 15, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warren, J.J.; Bishara, S.E. Duration of nutritive and nonnutritive sucking behaviors and their effects on the dental arches in the primary dentition. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 347–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, H.T.B.; Sum, F.H.K.M.H.; Zhang, L.; Yeung, C.P.W.; Li, K.Y.; Wong, H.M.; Yang, Y. The association between nutritive, non-nutritive sucking habits and primary dental occlusion. BMC Oral Health 2018, 18, 145. [Google Scholar] [CrossRef] [PubMed]
- Jabbar, N.S.A.; Bueno, A.B.M.; Da Silva, P.E.; Scavone-Junior, H.; Ferreira, R.I. Bottle feeding, increased overjet and Class 2 primary canine relationship: Is there any association? Braz. Oral Res. 2011, 25, 331–337. [Google Scholar] [CrossRef] [Green Version]
- Paolantonio, E.G.; Ludovici, N.; Saccomanno, S.; La Torre, G.; Grippaudo, C. Association between oral habits, mouth breathing and malocclusion in Italian preschoolers. Eur. J. Paediatr. Dent. 2019, 20, 204–208. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Co-Sleeping | Non-Co-Sleeping | n (%) |
|---|---|---|---|
| Gender | |||
| Male | 69 | 49 | 118 (53.4%) |
| Female | 61 | 42 | 103 (46.6%) |
| Total n (%) | 130 | 91 | 221 (100%) |
| Children’s age | |||
| 2 years | 4 | 5 | 9 (4.1%) |
| 3 years | 45 | 25 | 70 (31.7%) |
| 4 years | 42 | 34 | 76 (34.4%) |
| 5 years | 39 | 27 | 66 (29.9%) |
| Total n (%) | 130 | 91 | 221 (100%) |
| Mother’s age range | |||
| ≤30 | 40 | 28 | 68 (30.8%) |
| >31 | 90 | 63 | 153 (69.2%) |
| Total n (%) | 130 | 91 | 221 (100%) |
| Mother’s educational level | |||
| No studies or primary | 27 | 27 | 54 (24.4%) |
| Secondary and higher education | 103 | 64 | 167 (75.6%) |
| Total n (%) | 130 | 91 | 221 (100%) |
| Mother’s work | |||
| Employee | 85 | 64 | 149 (67.4%) |
| Unemployed | 45 | 27 | 72 (32.6%) |
| Total n (%) | 130 | 91 | 221 (100%) |
| Socioeconomic level | |||
| Low | 16 | 17 | 33 (14.9%) |
| Low-medium | 34 | 17 | 51 (23.1%) |
| Medium | 40 | 30 | 70 (31.7%) |
| Medium-high | 30 | 18 | 48 (21.7%) |
| High | 10 | 9 | 19 (8.6%) |
| Total n (%) | 130 | 91 | 221 (100%) |
| Variables | Co-Sleeping M (SD) | Non-Co-Sleeping M (SD) | p-Value | D Cohen |
|---|---|---|---|---|
| Pacifier sucking | ||||
| Daily frequency (hours in a day) | 5.94 (5.69) | 8.77 (6.40) | 0.016 * | 0.46 |
| Duration (months) | 18.91 (10.88) | 24.86 (9.82) | 0.043 * | 0.57 |
| Digital sucking | ||||
| Daily frequency (hours in a day) | 2.90 (1.44) | 3.92 (1.61) | 0.029 * | 0.66 |
| Duration (months) | 17.25 (12.75) | 25.11 (12.79) | 0.003 ** | 0.61 |
| 1 | 2 | 3 | 4 | 5 | 6 | ||
|---|---|---|---|---|---|---|---|
| Daily frequency of pacifier use (hours) | r | 0.210 | 0.147 | 0.000 | 0.194 | 0.230 | |
| p | 0.006 | 0.246 | 0.998 | 0.012 | 0.003 | ||
| n | 168 | 64 | 64 | 168 | 168 | ||
| Pacifier duration (months) | r | −0.041 | 0.129 | 0.210 | 0.290 | ||
| p | 0.750 | 0.311 | 0.006 | 0.000 | |||
| n | 64 | 64 | 168 | 168 | |||
| Daily frequency of digital sucking (hours) | r | 0.362 | 0.157 | 0.045 | |||
| p | 0.001 | 0.147 | 0.682 | ||||
| n | 87 | 87 | 87 | ||||
| Duration of digital sucking (months) | r | 0.146 | 0.061 | ||||
| p | 0.176 | 0.572 | |||||
| n | 87 | 87 | |||||
| IOTN-AC | r | 0.573 | |||||
| p | 0.000 | ||||||
| n | 221 | ||||||
| WHO INDEX | r | ||||||
| p | |||||||
| n |
| Variables | Co-Sleeping M (SD) | Non-Co-Sleeping M (SD) | p-Value | D Cohen |
|---|---|---|---|---|
| WHO | 1.81 (0.71) | 2.27 (0.76) | 0.000 * | 0.62 |
| IOTN-AC | 1.95 (1.04) | 2.38 (1.45) | 0.011 ** | 0.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrillo-Díaz, M.; Ruiz-Guillén, A.; Moya, M.; Romero-Maroto, M.; González-Olmo, M.J. Co-Sleeping as a Protector against Malocclusion in the Primary Dentition: A Cross-Sectional Study. J. Clin. Med. 2022, 11, 2338. https://doi.org/10.3390/jcm11092338
Carrillo-Díaz M, Ruiz-Guillén A, Moya M, Romero-Maroto M, González-Olmo MJ. Co-Sleeping as a Protector against Malocclusion in the Primary Dentition: A Cross-Sectional Study. Journal of Clinical Medicine. 2022; 11(9):2338. https://doi.org/10.3390/jcm11092338
Chicago/Turabian StyleCarrillo-Díaz, María, Ana Ruiz-Guillén, María Moya, Martín Romero-Maroto, and María José González-Olmo. 2022. "Co-Sleeping as a Protector against Malocclusion in the Primary Dentition: A Cross-Sectional Study" Journal of Clinical Medicine 11, no. 9: 2338. https://doi.org/10.3390/jcm11092338