
Endoscopic-Assisted Keyhole Middle Cranial Fossa Approach for Small Vestibular Schwannomas

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
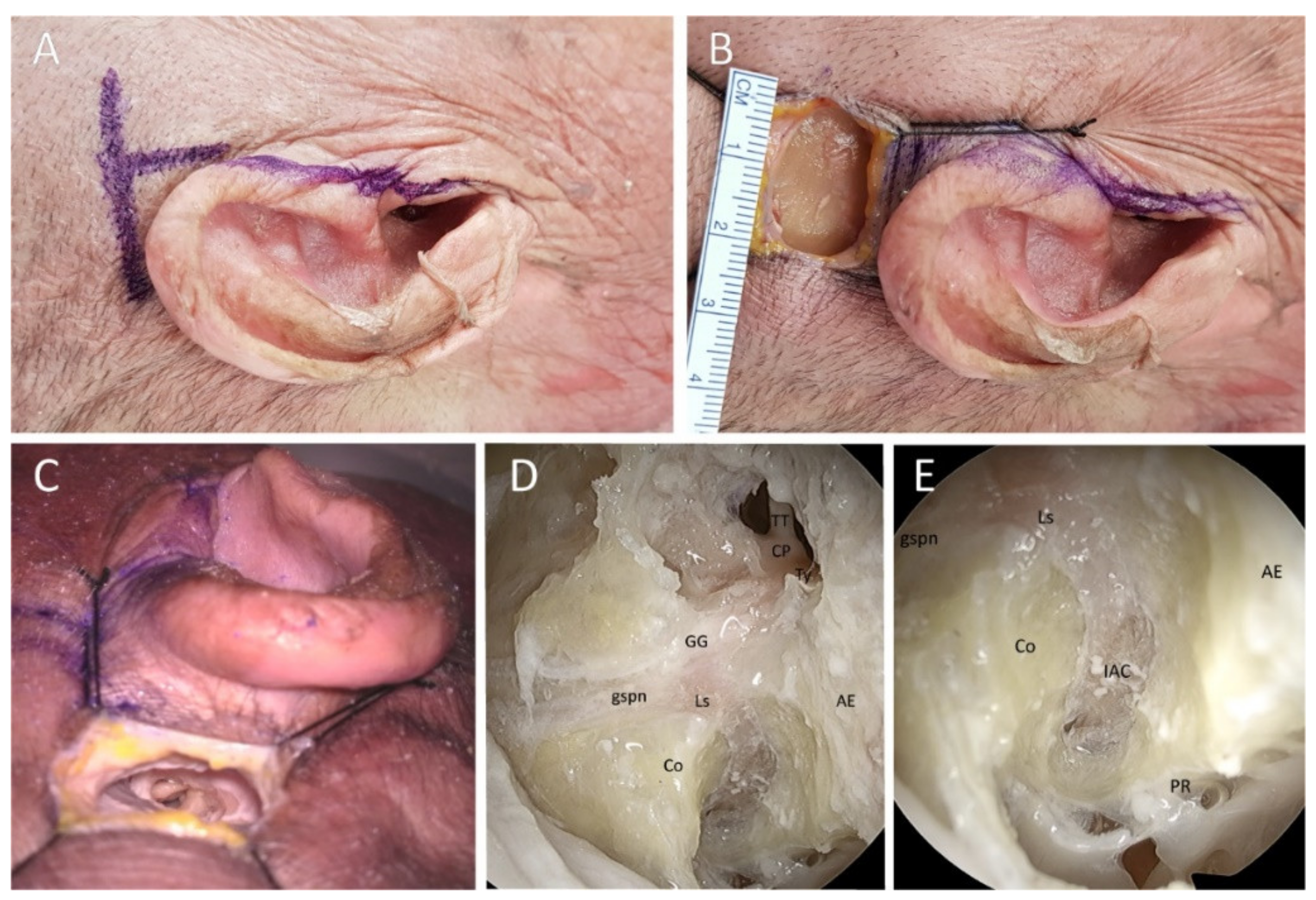
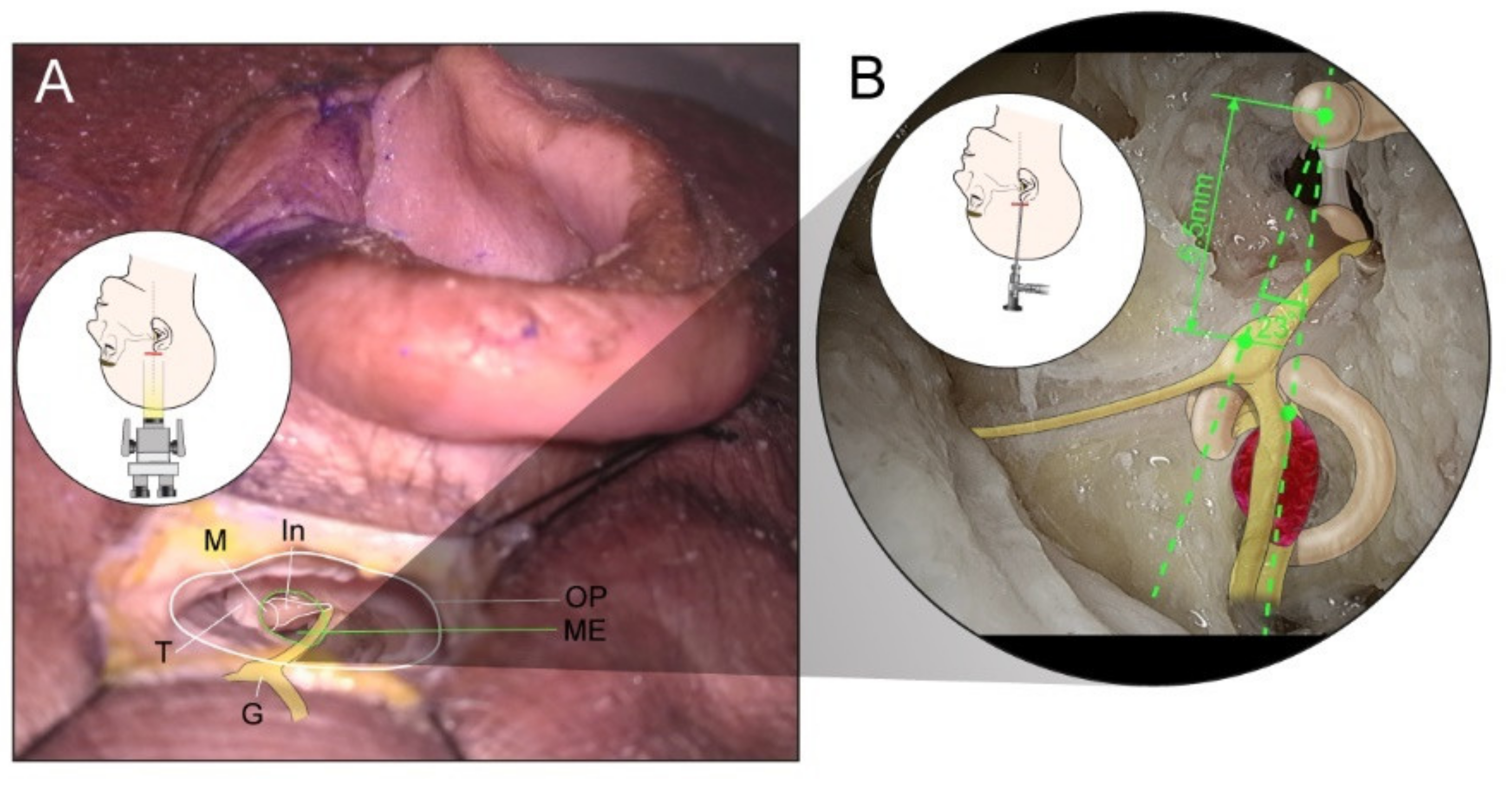
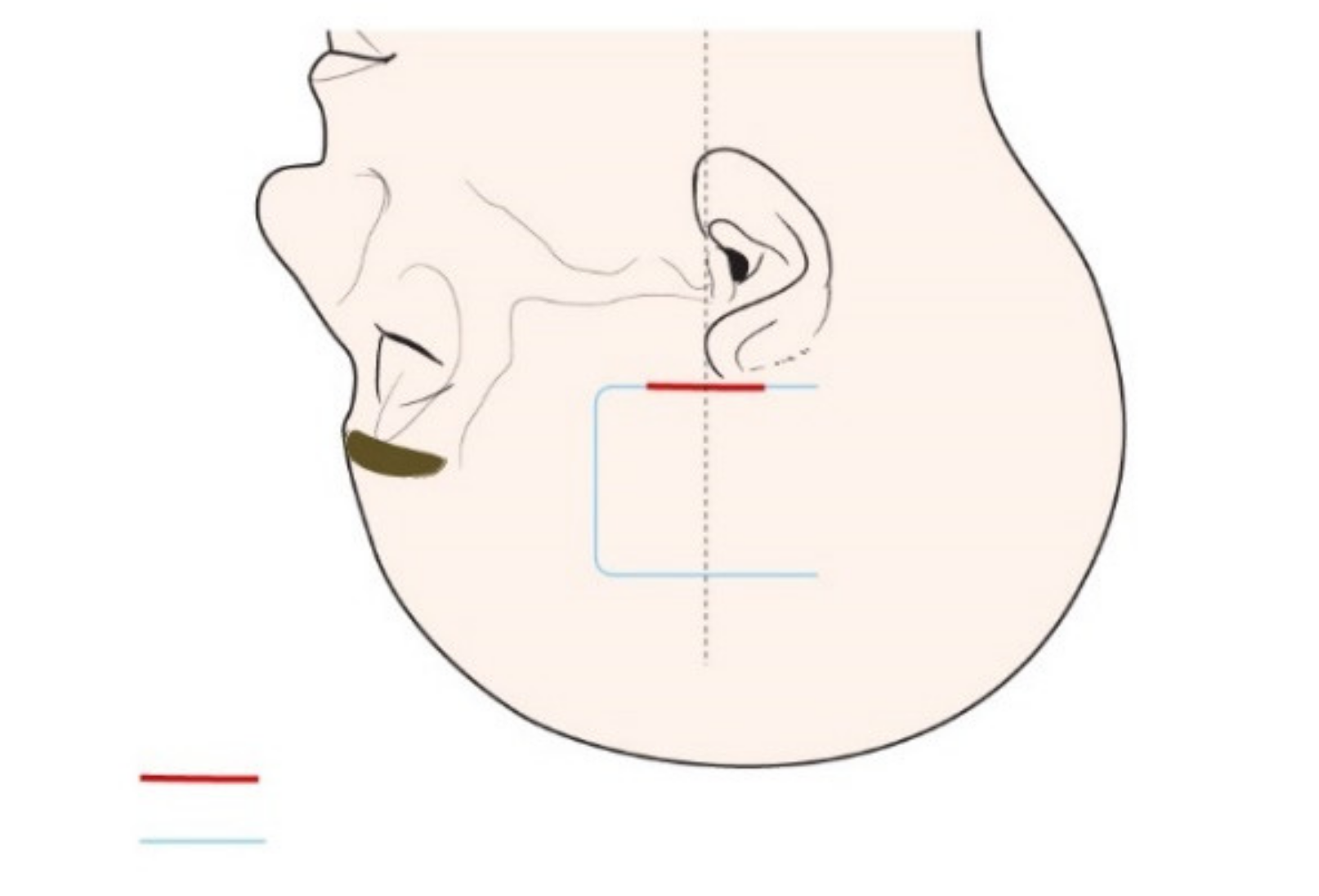
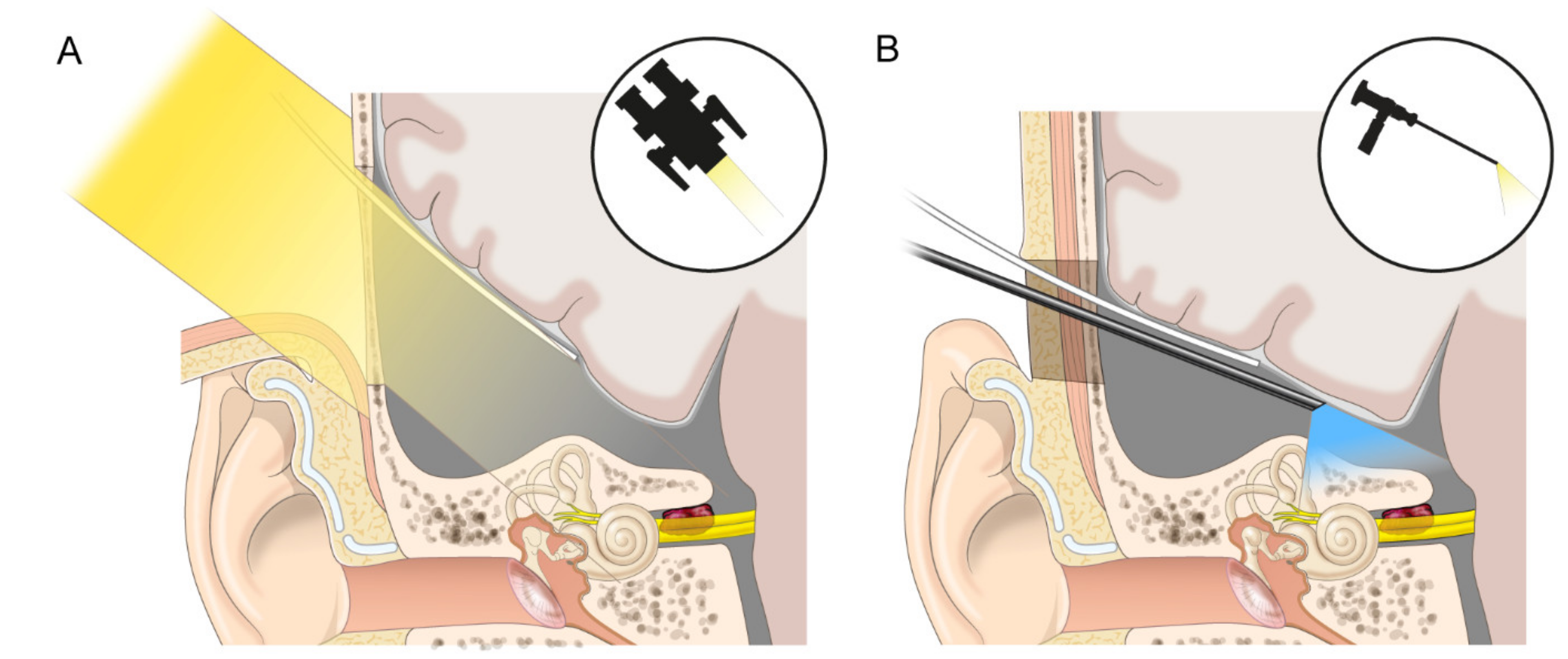
2.1. Cadaveric Demonstration
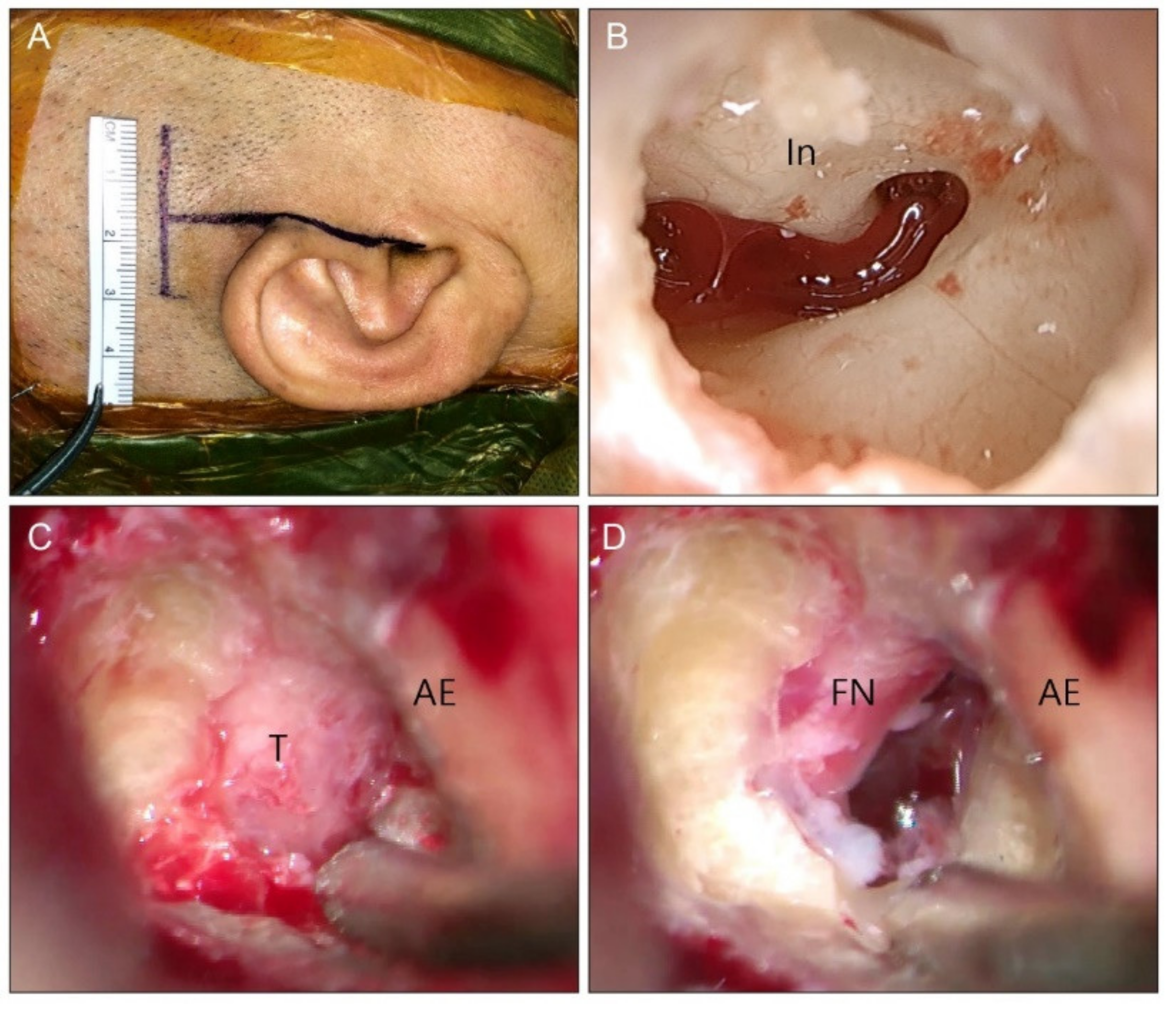
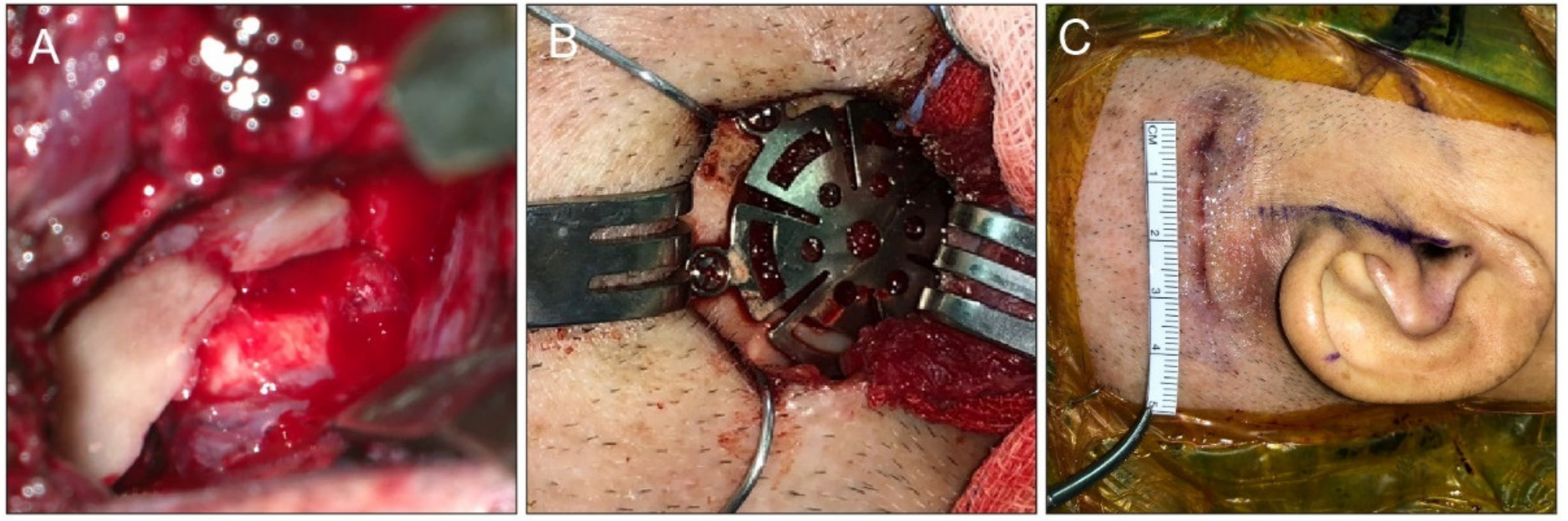
2.2. Clinical Cases
2.3. Outcome Evaluation
2.4. Statistical Analyses
3. Results
3.1. Cadaveric Demonstration
3.2. Clinical Cases
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- House, W.F. Surgical exposure of the internal auditory canal and its contents through the middle, cranial fossa. Laryngoscope 1961, 71, 1363–1385. [Google Scholar] [CrossRef] [PubMed]
- Kutz, J.W., Jr.; Johnson, A.K.; Wick, C.C. Surgical management of spontaneous cerebrospinal fistulas and encephaloceles of the temporal bone. Laryngoscope 2018, 128, 2170–2177. [Google Scholar] [CrossRef] [PubMed]
- Arts, H.A.; Telian, S.A.; El-Kashlan, H.; Thompson, B.G. Hearing preservation and facial nerve outcomes in vestibular schwannoma surgery: Results using the middle cranial fossa approach. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2006, 27, 234–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannon, R.B.; Gurgel, R.K.; Warren, F.M.; Shelton, C. Facial nerve outcomes after middle fossa decompression for bell’s palsy. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2015, 36, 513–518. [Google Scholar] [CrossRef]
- Rabelo de Freitas, M.; Russo, A.; Sequino, G.; Piccirillo, E.; Sanna, M. Analysis of hearing preservation and facial nerve function for patients undergoing vestibular schwannoma surgery: The middle cranial fossa approach versus the retrosigmoid approach--personal experience and literature review. Audiol. Neuro-Otol. 2012, 17, 71–81. [Google Scholar] [CrossRef]
- Ung, N.; Chung, L.K.; Lagman, C.; Bhatt, N.S.; Barnette, N.E.; Ong, V.; Gopen, Q.; Yang, I. Outcomes of middle fossa craniotomy for the repair of superior semicircular canal dehiscence. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2017, 43, 103–107. [Google Scholar] [CrossRef]
- Fisch, U. Transtemporal supralabyrinthine (middle cranial fossa) vestibular neurectomy: A review of the last 100 cases. Skull Base Surg. 1996, 6, 221–225. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Ibanez, E.; Garcia-Ibanez, J.L. Middle fossa vestibular neurectomy: A report of 373 cases. Otolaryngol. -Head Neck Surg. Off. J. Am. Acad. Otolaryngol. -Head Neck Surg. 1980, 88, 486–490. [Google Scholar] [CrossRef]
- Sanna, M.; Hamada, M. Atlas of Acoustic Neurinoma Microsurgery; Thieme: Stuttgart, Germany, 2011. [Google Scholar]
- Kutz, J.W., Jr.; Scoresby, T.; Isaacson, B.; Mickey, B.E.; Madden, C.J.; Barnett, S.L.; Coimbra, C.; Hynan, L.S.; Roland, P.S. Hearing preservation using the middle fossa approach for the treatment of vestibular schwannoma. Neurosurgery 2012, 70, 334–340, discussion 340–31. [Google Scholar] [CrossRef]
- Komatsu, F.; Imai, M.; Hirayama, A.; Hayashi, N.; Oda, S.; Shimoda, M.; Matsumae, M. Endoscopic middle cranial fossa reconstruction with a subtemporal keyhole. World Neurosurg. 2017, 108, 157–162. [Google Scholar] [CrossRef]
- Kozin, E.D.; Lee, D.J. Minimally invasive middle fossa craniotomy approach with endoscopic repair of superior canal dehiscence. Oper. Tech. Otolaryngol. -Head Neck Surg. 2017, 28, 50–56. [Google Scholar] [CrossRef]
- Trieu, V.; Pelargos, P.E.; Spasic, M.; Chung, L.K.; Voth, B.; Ung, N.; Gopen, Q.; Yang, I. Minimally invasive middle fossa keyhole craniectomy for repair of superior semicircular canal dehiscence. Oper. Neurosurg. (Hagerstown) 2017, 13, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.K.; Shinners, M.; Wong, R.H. Minimally invasive repair of tegmen defects through keyhole middle fossa approach to reduce hospitalization. World Neurosurg. 2020, 133, e683–e689. [Google Scholar] [CrossRef]
- Liming, B.J.; Westbrook, B.; Bakken, H.; Crawford, J.V. Cadaveric study of an endoscopic keyhole middle fossa craniotomy approach to the superior semicircular canal. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2016, 37, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Mourgela, S.; Sakellaropoulos, A.; Anagnostopoulou, S. Middle cranial fossa endoscopy using a rigid endoscope. Minim Invasive Ther. Allied. Technol. 2007, 16, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.J.; Eden, A.R. An external reference to identify the internal auditory canal in middle fossa surgery. Otolaryngol. -Head Neck Surg. Off. J. Am. Acad. Otolaryngol.—Head Neck Surg. 1993, 108, 111–116. [Google Scholar] [CrossRef]
- Lee, H.K.; Lee, W.S. Microsurgical anatomy of the perigeniculate ganglion area as seen from the middle cranial fossa approach. Ann. Otol. Rhinol. Laryngol. 2003, 112, 531–533. [Google Scholar] [CrossRef]
- Han, T.; Park, C. A study on standardization of korean pb word list for speech audiometry. Korean J. Otorhinolaryngol. Head Neck Surg. 1981, 24, 265–272. [Google Scholar]
- Gurgel, R.K.; Jackler, R.K.; Dobie, R.A.; Popelka, G.R. A new standardized format for reporting hearing outcome in clinical trials. Otolaryngol. -Head Neck Surg. Off. J. Am. Acad. Otolaryngol. -Head Neck Surg. 2012, 147, 803–807. [Google Scholar] [CrossRef]
- Hecht, C.S.; Honrubia, V.F.; Wiet, R.J.; Sims, H.S. Hearing preservation after acoustic neuroma resection with tumor size used as a clinical prognosticator. Laryngoscope 1997, 107, 1122–1126. [Google Scholar] [CrossRef]
- Nadol, J.B., Jr.; Chiong, C.M.; Ojemann, R.G.; McKenna, M.J.; Martuza, R.L.; Montgomery, W.W.; Levine, R.A.; Ronner, S.F.; Glynn, R.J. Preservation of hearing and facial nerve function in resection of acoustic neuroma. Laryngoscope 1992, 102, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Staecker, H.; Nadol, J.B., Jr.; Ojeman, R.; Ronner, S.; McKenna, M.J. Hearing preservation in acoustic neuroma surgery: Middle fossa versus retrosigmoid approach. Am. J. Otol. 2000, 21, 399–404. [Google Scholar] [CrossRef]
- Niranjan, A.; Mathieu, D.; Flickinger, J.C.; Kondziolka, D.; Lunsford, L.D. Hearing preservation after intracanalicular vestibular schwannoma radiosurgery. Neurosurgery 2008, 63, 1054–1062, discussion 1062–1053. [Google Scholar] [CrossRef] [PubMed]
- Gerosa, M.; Mesiano, N.; Longhi, M.; De Simone, A.; Foroni, R.; Verlicchi, A.; Zanotti, B.; Nicolato, A. Gamma knife surgery in vestibular schwannomas: Impact on the anterior and posterior labyrinth. J. Neurosurg. 2010, 113, 128–135. [Google Scholar] [CrossRef]
- Combs, S.E.; Thilmann, C.; Debus, J.; Schulz-Ertner, D. Long-term outcome of stereotactic radiosurgery (srs) in patients with acoustic neuromas. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 1341–1347. [Google Scholar] [CrossRef]
- Chopra, R.; Kondziolka, D.; Niranjan, A.; Lunsford, L.D.; Flickinger, J.C. Long-term follow-up of acoustic schwannoma radiosurgery with marginal tumor doses of 12 to 13 gy. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 845–851. [Google Scholar] [CrossRef]
- Ismail, O.; Sobhy, O.; Assal, S.; Sanghera, P.; Begg, P.; Irving, R. Comparing hearing outcomes in irradiated and conservatively managed vestibular schwannoma. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2022, 43, e374–e381. [Google Scholar] [CrossRef]
- Jean, W.C.; Mueller, K.; Kim, H.J. Middle fossa approach for resection of an intracanalicular vestibular schwannoma. J. Neurol. Surg. B Skull Base 2019, 80, S287. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.; Skilbeck, C.; Saeed, S.; Bradford, R. Expectant management of vestibular schwannoma: A retrospective multivariate analysis of tumor growth and outcome. Skull Base Off. J. N. Am. Skull Base Soc. 2011, 21, 295–302. [Google Scholar]
- Hajioff, D.; Raut, V.V.; Walsh, R.M.; Bath, A.P.; Bance, M.L.; Guha, A.; Tator, C.H.; Rutka, J.A. Conservative management of vestibular schwannomas: Third review of a 10-year prospective study. Clin. Otolaryngol. Off. J. ENT-UK Off. J. Neth. Soc. Oto-Rhino-Laryngol. Cervico-Facial Surg. 2008, 33, 255–259. [Google Scholar] [CrossRef]
- Banerjee, R.; Moriarty, J.P.; Foote, R.L.; Pollock, B.E. Comparison of the surgical and follow-up costs associated with microsurgical resection and stereotactic radiosurgery for vestibular schwannoma. J. Neurosurg. 2008, 108, 1220–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangham, C.A., Jr. Retrosigmoid versus middle fossa surgery for small vestibular schwannomas. Laryngoscope 2004, 114, 1455–1461. [Google Scholar] [CrossRef] [PubMed]
- Quesnel, A.M.; McKenna, M.J. Current strategies in management of intracanalicular vestibular schwannoma. Curr. Opin. Otolaryngol. Head Neck Surg. 2011, 19, 335–340. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgery | Patient | Sex | Age (Years) | Site | Tumor Size (mm) | Tumor Growth Rate (mm/year) | Intractable Vertigo | Preoperative Hearing Threshold (dB HL) | Preoperative Word Recognition Score (%) | Hearing Deterioration Rate (dB/6 Months) | Surgical Outcome | Postoperative Complications | Operation Time (Minutes) | Hospital Stay (Days) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| KMCFA | 1 | Male | 40 | Left | 8 × 5 | Not available | No | 68 | 58 | 29 | Total | None | 312 | 6 |
| KMCFA | 2 | Female | 60 | Left | 11 × 8 | 2 | Yes | 26 | 90 | 2 | Total | None | 345 | 7 |
| KMCFA | 3 | Female | 77 | Left | 7 × 3 | 2 | No | 61 | 26 | 5 | Total | None | 263 | 10 |
| KMCFA | 4 | Female | 49 | Right | 4 × 5 | <1 | Yes | 8 | 96 | None | Total | None | 501 | 7 |
| KMCFA | 5 | Male | 59 | Left | 9 × 5 | Not available | No | 56 | 70 | 2 | Total | None | 320 | 7 |
| MCFA | 6 | Male | 49 | Left | 7 × 4 | 1 | Yes | 10 | 94 | None | Total | Facial palsy, headache | 427 | 9 |
| MCFA | 7 | Male | 59 | Right | 13 × 8 | Not available | Yes | 24 | 90 | Not available | Subtotal | None | 637 | 9 |
| MCFA | 8 | Female | 37 | Left | 8 × 5 | Not available | Yes | 10 | Not available | Not available | Subtotal | None | 681 | 9 |
| MCFA | 9 | Male | 44 | Left | 6 × 4 | <1 | No | 60 | 52 | 3 | Subtotal | None | 555 | 11 |
| MCFA | 10 | Female | 51 | Left | 6 × 2 | Not available | No | 33 | 88 | Not available | Total | None | 430 | 15 |
| MCFA | 11 | Female | 38 | Left | 5 × 4 | No growth | No | 58 | 70 | Not available | Total | CSF leakage | 405 | 12 |
| MCFA | 12 | Female | 66 | Left | 3 × 2 | Not available | No | 8 | 98 | Not available | Total | None | 460 | 12 |
| MCFA | 13 | Male | 17 | Right | 5 × 3 | No growth | No | 21 | 98 | Not available | Total | None | 300 | 11 |
| KMCFA | Classical MCFA | p-Value | |
|---|---|---|---|
| Sex (male:female) | 2:3 | 4:4 | |
| Site (left:right) | 4:1 | 6:2 | |
| Age (years) | 57 ± 6.19 | 45.1 ± 5.32 | 0.18 |
| Tumor size (mm) | 8 ± 1.00 | 6.8 ± 1.04 | 0.45 |
| Tumor growth rate † (mm/6 months) | 2 | 0.3 | |
| Intractable vertigo rate (%) | 40 (2/5) | 37.5 (3/8) | |
| Preoperative hearing threshold (dB HL) | 40 ± 10.0 | 28 ± 7.4 | 0.35 |
| Surgical outcome (rate of total removal, %) | 100 (5/5) | 62.5 (5/8) | 0.23 |
| Major complication ‡ rate (%) | 0 (0/5) | 25 (2/8) | 0.49 |
| Surgical time (minutes) | 348.2 ± 40.45 | 486.9 ± 45.13 | 0.06 |
| Hospital stay § (days) | 7.4 (6.5–8.5) | 11 (9–12) | 0.0054 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, I.S.; Choi, I.S.; Shin, S.H.; Yang, S.; Jung, Y.; Na, G. Endoscopic-Assisted Keyhole Middle Cranial Fossa Approach for Small Vestibular Schwannomas. J. Clin. Med. 2022, 11, 2324. https://doi.org/10.3390/jcm11092324
Moon IS, Choi IS, Shin SH, Yang S, Jung Y, Na G. Endoscopic-Assisted Keyhole Middle Cranial Fossa Approach for Small Vestibular Schwannomas. Journal of Clinical Medicine. 2022; 11(9):2324. https://doi.org/10.3390/jcm11092324
Chicago/Turabian StyleMoon, In Seok, Ick Soo Choi, Seung Ho Shin, Seungjoon Yang, Youngrak Jung, and Gina Na. 2022. "Endoscopic-Assisted Keyhole Middle Cranial Fossa Approach for Small Vestibular Schwannomas" Journal of Clinical Medicine 11, no. 9: 2324. https://doi.org/10.3390/jcm11092324