
New Analytical Approach for the Alignment of Different HE4 Automated Immunometric Systems: An Italian Multicentric Study

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Reference Calibration Curve
2.3. Sample Size Calculation
2.4. Database Population
- (a)
- Healthy women: Healthy Blood donors without gynecological diseases have been recruited from the Transfusional Unit of the Policlinico Umberto I of Rome. Healthy women were recruited according to the criteria and physical requirements for the selection of blood and blood-components donors following “the disposition related to the quality requirements and safety of blood and its components”, published in Gazzetta Ufficiale no.69 (2 November 2015).
- (b)
- Benign gynecological diseases: Ovarian cyst, endometriosis, uterine and vaginal fibroma, hemorrhagic corpus luteum, endometrial hyperplasia, endometrial polyp, salpingitis, chronic cervicitis, Brenner’s tumor, cystadenoma of the ovary, vesicular mola. All patients included in this group had imaging and histological confirmation of these clinical status.
- (c)
- Malignant gynecological diseases: Ovarian cancer. All patients, following surgery, have had confirmation of the malignancy of the neoplasm and relative staging.
2.5. Serum Sample
2.6. HE4 Immunoassay
- LUMIPULSE G1200II and G600II (CLEIA) chemiluminescence. The HE4 Lumipulse G Fujirebio assay uses a chemiluminescent competitive enzyme immunoassay (CLEIA), conducted on the LUMIPULSE G 1200 II analyzer and LUMIPULSE G600II. It is a two-step sandwich test that uses two monoclonal antibodies, 2H5 MAb, which coats paramagnetic microparticles and 12A2 MAb, labeled with alkaline phosphatase. All necessary components are packaged in a single ready-to-use cartridge.The manufacturer declares a total coefficient of variation (CV) ≤ 3.2%.Internal Controls → Three different internal controls (Level1 48.3–89.8; Level2 398–738; specimen pool) were processed to test the correct functionality of the analyzer.Calibration → A two-point master curve with a range between 0 and 1500 pmol/L was used for calibration.LoD 3.5 pmol/L, LoQ 3.5 pmol/L and linearity was between 20.0 and 1500 pmol/L.
- COBAS E601 (Roche Diagnostics, Manheim, Germany) Electrochemiluminescence (ECLIA). The Elecsys HE4 test is an electrochemiluminescence immunoassay performed on Cobas E601. The development of ECL immunoassays is based on the use of a ruthenium and tripropylamine (TPA) complex. IT is based on a one-step sandwich principle, using a biotinylated 2H5 MAb and the 12A2 MAb labeled with a ruthenium complex for sandwich detection. The latter MAb binds the amino terminal domain of the whey acidic four-disulphide core (WFDC) of the HE4 protein. The chemiluminescence reaction for detecting the reaction complex is initiated by applying a voltage to the sample solution, which results in a precisely controlled reaction.The manufacturer declares a CV ≤ 10%.Internal Controls → Three different internal controls (high, medium and low concentration levels) were processed to test the correct functionality of the analyzer.Calibration → A two-point master curve with a range between 0 and 1500 pmol/L was used for calibration.LoD 5.00 pmol/L, LoQ 20.0 pmol/L and linearity was between 15.0 and 1500 pmol/L.
- ARCHITECT (Abbott Diagnostics, North Chicago, IL, USA) (CMIA) chemiluminescence. The assay HE4 is a microparticle capture chemiluminescent immunoassay (CMIA), performed on the Architect i2000 platform. It is a two-step non-competitive assay performed using two monoclonal antibodies (MAb) directed against two different epitopes of the carboxy terminal domain of the whey acidic four-disulphide core (C-WFDC) of the HE4 protein, 2H5 MAb, capture antibody and 3D8 MAb detection antibody. The chemiluminescent reaction is detected as a relative light unit (RLU). The amount of He4 in the sample and the detected RLUs are directly related parameters.The manufacturer declares a CV ≤ 10%.Internal Controls → Three different internal controls (high, medium and low concentration levels) are processed to test the correct functionality of the analyzer.Calibration → A six-point calibration with a range between 0 and 1500 pmol/L was used for calibration. The calibrators for the assay (in liquid form ready to use lot n.88K10514) were made volumetrically.LoD < 15.0 pmol/L, LoQ < 20.0 pmol/L and linearity was between 20.0 and 1500 pmol/L.
- ALINITY I (LAB4) (Abbott Laboratories, IL, USA) (CMIA) chemiluminescence: The HE4 test is a microparticle capture chemiluminescent immunoassay (CMIA), performed on the Anility I analyzer.The sample and the paramagnetic microparticles coated with antibodies anti-HE4 2H5 are dispensed together and incubated. The HE4 antigen in the sample binds to microparticles coated with anti-HE4 antibodies. The mixture is washed. Acridinium-labeled anti-HE4 3D8 antibody conjugate is added to form a mixture reaction, which is then incubated. After a wash cycle, pre-trigger and trigger solutions are added. The resulting chemiluminescent reaction is measured in relative light units (RLUs). There is a direct link between the amount of HE4 antigen in the sample and the RLUs measured by the optical system.The manufacturer declares a total CV ≤ 4.9%. Two different internal controls (low and medium) were processed in order to test the correct functionality of the test and analyzer: low control ranged from 35–65 pmol/L and medium control was between 122.5–227.5 pmol/L.Calibration of HE4 assay was performed with six calibrators, with a concentration ranging between 0 and 1500 pmol/L.LoD 0.5 pmol/L and LoQ 2.0 pmol/L. Linearity of the assay was between 20.0 and 1500.0 pmol/L.
2.7. Ca125 Immunoassay
- LUMIPULSE G1200II and G600II (CLEIA) chemiluminescence. The Ca125 Lumipulse G Fujirebio assay uses a CLEIA Chemiluminescent Competitive Enzyme Immunoassay, conducted on the LUMIPULSE G 1200 II analyzer and LUMIPULSE G600II. It is a two-step sandwich test that uses two monoclonal antibodies, OC125 MAb, which coats paramagnetic microparticles and M11 MAb, labeled with alkaline phosphatase. All necessary components are packaged in a single ready-to-use cartridge. The manufacturer declares a total CV ≤ 4%.Internal Controls → Three different internal controls were processed to test the correct functionality of the analyzer.Calibration → A two-point master curve with a range between 0 and 1000 U/mL was used for calibration.LoD 0.657 U/mL, LoQ 0.657 U/mL and linearity was between 13.9 and 1000 U/mL.
- COBAS E601 (Roche Diagnostics, Manheim, Germany) Electrochemiluminescence (ECLIA). The Elecsys Ca125 test is an electrochemiluminescence immunoassay performed on Cobas E601. The development of ECL immunoassays is based on the use of a ruthenium and tripropylamine (TPA) complex. IT is based on a one-step sandwich principle, using a biotinylated M11 MAb and the OC125 MAb labeled with a ruthenium complex for sandwich detection. The chemiluminescence reaction for detecting the reaction complex is initiated by applying a voltage to the sample solution, which results in a precisely controlled reaction. The manufacturer declares a CV ≤ 6.5%.Internal Controls → Three different internal controls (high, medium and low concentration levels) were processed to test the correct functionality of the analyzer.Calibration → A two-point master curve with a range between 0 and 5000 U/mL was used for calibration.LoD 1.2 U/mL, LoQ 2.0 U/mL and linearity was between 0.6–5000 U/mL.
- ARCHITECT (Abbott Diagnostics, North Chicago, IL, USA) (CMIA) chemiluminescence. The Assay Ca125 is a microparticle capture chemiluminescent immunoassay (CMIA), performed on the Architect i2000 platform. In the first step, the sample and OC 125 MAb coated paramagnetic microparticles are combined. OC 125 defined antigen present in the sample binds to the OC 125 coated microparticles. After washing, M11 MAb acridinium-labeled conjugate is added in the second step. The chemiluminescent reaction is detected as a relative light unit (RLU). The amount of Ca125 in the sample and the detected RLUs are directly related parameters. The manufacturer declares a CV ≤ 10%.Internal Controls → Three different internal controls (high, medium and low concentration levels) were processed to test the correct functionality of the analyzer.Calibration → A six-point calibration with a range between 0 and 1000 U/mL was used for calibration.LoD ≤ 1.0 U/mL, LoQ ≤ 1.0 U/mL and linearity was between 1.0 and 1000 U/mL.
- ALINITY I (LAB4) (Abbott Laboratories, IL, USA) (CMIA) chemiluminescence. The Ca125 test is a microparticle capture chemiluminescent immunoassay (CMIA), performed on the Anility I analyzer. The assay uses paramagnetic microparticles coated with OC 125 monoclonal antibody to bind the molecules containing the antigen OC 125. These antigens are quantified using acridinium-labeled M11 antibody. The resulting chemiluminescent reaction is measured in relative light units (RLUs). There is a direct link between the amount of Ca125 antigen in the sample and the RLUs measured by the optical system. The manufacturer declares a total CV ≤ 4.8%.Internal controls (low and medium) were processed in order to test the correct functionality of the test and analyzer.Calibration of Ca125 assay was performed with six calibrators with a concentration range between 0 and 1000 U/mL.LoD 0.3 U/mL and LoQ 0.6 U/mL. Linearity of the assay was between 1.1 and 1000.0 U/mL.
2.8. Statistical Analisys
3. Results
3.1. Systematic Biases in HE4 Measurement
3.2. Analysis of Factors Influencing HE4 Accuracy
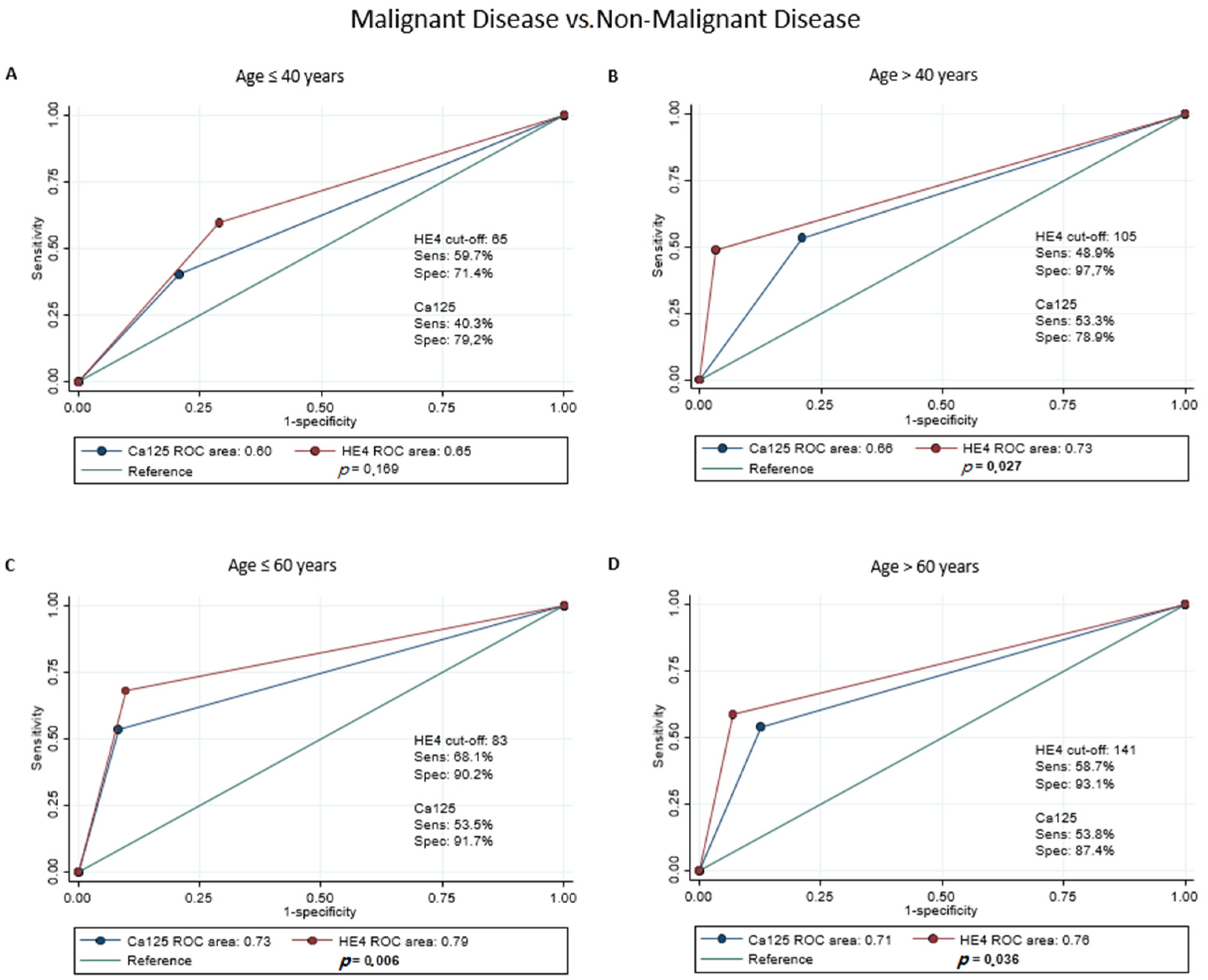
3.3. Accuracy of Dichotomous HE4
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Suneja, G.; Viswanathan, A. Gynecologic Malignancies. Hematol. Oncol. Clin. N. Am. 2020, 34, 71–89. [Google Scholar] [CrossRef] [PubMed]
- Ledford, L.R.C.; Lockwood, S. Scope and Epidemiology of Gynecologic Cancers: An Overview. Semin. Oncol. Nurs. 2019, 35, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Momenimovahed, Z.; Tiznobaik, A.; Taheri, S.; Salehiniya, H. Ovarian cancer in the world: Epidemiology and risk factors. Int. J. Womens Health 2019, 11, 287–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernooij, F.; Heintz, A.P.; Coebergh, J.W.; Massuger, L.F.; Witteveen, P.O.; van der Graaf, Y. Specialized and high-volume care leads to better outcomes of ovarian cancer treatment in the Netherlands. Gynecol. Oncol. 2009, 112, 455–461. [Google Scholar] [CrossRef]
- Goff, B.A.; Matthews, B.J.; Larson, E.H.; Andrilla, C.H.; Wynn, M.; Lishner, D.M.; Baldwin, L.M. Predictors of comprehensive surgical treatment in patients with ovarian cancer. Cancer 2007, 109, 2031–2042. [Google Scholar] [CrossRef]
- Aune, G.; Torp, S.H.; Syversen, U.; Hagen, B.; Tingulstad, S. Ten years’ experience with centralized surgery of ovarian cancer in one health region in Norway. Int. J. Gynecol. Cancer 2012, 22, 226–231. [Google Scholar] [CrossRef]
- Dochez, V.; Caillon, H.; Vaucel, E.; Dimet, J.; Winer, N.; Ducarme, G. Biomarkers and algorithms for diagnosis of ovarian cancer: CA125, HE4, RMI and ROMA, a review. J. Ovarian. Res. 2019, 12, 28. [Google Scholar] [CrossRef] [Green Version]
- Funston, G.; Hamilton, W.; Abel, G.; Crosbie, E.J.; Rous, B.; Walter, F.M. The diagnostic performance of CA125 for the detection of ovarian and non-ovarian cancer in primary care: A population-based cohort study. PLoS Med. 2020, 17, e1003295. [Google Scholar] [CrossRef]
- Anastasi, E.; Granato, T.; Marchei, G.G.; Viggiani, V.; Colaprisca, B.; Complo, J.S.; Reale, M.G.; Frati, L.; Midulla, C. Ovarian tumor marker HE4 is differently expressed during the phases of the menstrual cycle in healthy young women. Tumour Biol. 2010, 31, 411–415. [Google Scholar] [CrossRef]
- Granato, T.; Porpora, M.G.; Longo, F.; Angeloni, A.; Manganaro, L.; Anastasi, E. HE4 in the differential diagnosis of ovarian masses. Clin. Chim. Acta. 2015, 446, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Moore, R.G.; Brown, A.K.; Miller, M.C.; Skates, S.; Allard, W.J.; Verch, T.; Steinhoff, M.; Messerlian, G.; DiSilvestro, P.; Granai, C.O.; et al. The use of multiple novel tumor biomarkers for the detection of ovarian carcinoma in patients with a pelvic mass. Gynecol. Oncol. 2008, 108, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.G.; McMeekin, D.S.; Brown, A.K.; DiSilvestro, P.; Miller, M.C.; Allard, W.J.; Gajewski, W.; Kurman, R.; Bast, R.C., Jr.; Skates, S.J. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol. Oncol. 2009, 112, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, R.G.; Miller, M.C.; Disilvestro, P.; Landrum, L.M.; Gajewski, W.; Ball, J.J.; Skates, S.J. Evaluation of the diagnostic accuracy of the risk of ovarian malignancy algorithm in women with a pelvic mass. Obstet. Gynecol. 2011, 118, 280–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahlou, N.; Brun, J.L. Marqueurs sériques et tumoraux ovariens dans le diagnostic des tumeurs ovariennes présumées bénignes [Ovarian tumor markers of presumed benign ovarian tumors]. J. Gynecol. Obstet. Biol. Reprod. 2013, 42, 752–759. [Google Scholar] [CrossRef]
- Barr, C.E.; Funston, G.; Mounce, L.T.A.; Pemberton, P.W.; Howe, J.D.; Crosbie, E.J. Comparison of two immunoassays for the measurement of serum HE4 for ovarian cancer. Pract. Lab. Med. 2021, 26, e00235. [Google Scholar] [CrossRef]
- Lippi, G.; Da Rin, G. Advantages and limitations of total laboratory automation: A personal overview. Clin. Chem. Lab. Med. 2019, 57, 802–811. [Google Scholar] [CrossRef]
- Ferraro, S.; Borille, S.; Carnevale, A.; Frusciante, E.; Bassani, N.; Panteghini, M. Verification of the harmonization of human epididymis protein 4 assays. Clin. Chem. Lab. Med. 2016, 54, 1635–1643. [Google Scholar] [CrossRef]
- Guo, Y.; Zhao, B.; Zhou, S.; Wen, L.; Liu, J.; Fu, Y.; Xu, F.; Liu, M. A comparison of the diagnostic performance of the O-RADS, RMI4, IOTA LR2, and IOTA SR systems by senior and junior doctors. Ultrasonography 2022. [Google Scholar] [CrossRef]
- Ludbrook, J. Linear regression analysis for comparing two measurers or methods of measurement: But which regression? Clin. Exp. Pharmacol. Physiol. 2010, 37, 692–699. [Google Scholar] [CrossRef]
- Pepe, M.; Longton, G.; Janes, H. Estimation and Comparison of Receiver Operating Characteristic Curves. Stata J. 2009, 9, 1. [Google Scholar] [CrossRef] [Green Version]
- Plebani, M.; HE4 Study Group. HE4 in gynecological cancers: Report of a European investigators and experts meeting. Clin. Chem. Lab. Med. 2012, 50, 2127–2136. [Google Scholar] [CrossRef] [PubMed]
- Abu Hassaan, S.O. Monitoring ovarian cancer patients during chemotherapy and follow-up with the serum tumor marker CA125. Dan. Med. J. 2018, 65, B5463. [Google Scholar] [PubMed]
- Olsen, M.; Lof, P.; Stiekema, A.; van den Broek, D.; Wilthagen, E.A.; Bossuyt, P.M.; Lok, C. The diagnostic accuracy of human epididymis protein 4 (HE4) for discriminating between benign and malignant pelvic masses: A systematic review and meta-analysis. Acta Obstet. Et Gynecol. Scand. 2021, 100, 1788–1799. [Google Scholar] [CrossRef]
- Jiang, S.W.; Chen, H.; Dowdy, S.; Fu, A.; Attewell, J.; Kalogera, E.; Drapkin, R.; Podratz, K.; Broaddus, R.; Li, J. HE4 transcription- and splice variants-specific expression in endometrial cancer and correlation with patient survival. Int. J. Mol. Sci. 2013, 14, 22655–22677. [Google Scholar] [CrossRef] [Green Version]
- Romagnolo, C.; Leon, A.E.; Fabricio, A.S.C.; Taborelli, M.; Polesel, J.; Del Pup, L.; Steffan, A.; Cervo, S.; Ravaggi, A.; Zanotti, L.; et al. HE4, CA125 and risk of ovarian malignancy algorithm (ROMA) as diagnostic tools for ovarian cancer in patients with a pelvic mass: An Italian multicenter study. Gynecol. Oncol. 2016, 141, 303–311. [Google Scholar] [CrossRef]
- Chen, X.; Zhou, H.; Chen, R.; He, J.; Wang, Y.; Huang, L.; Sun, L.; Duan, C.; Luo, X.; Yan, H. Development of a multimarker assay for differential diagnosis of benign and malignant pelvic masses. Clin. Chim. Acta. 2015, 440, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Peiretti, M.; Congiu, F.; Ricciardi, E.; Maniglio, P.; Mais, V.; Angioni, S. Conservative treatment for well-differentiated endometrial cancer: When and why it should be considered in young women. Ecancermedicalscience 2019, 13, 892. [Google Scholar] [CrossRef] [PubMed]
- Candotti, G.; Peiretti, M.; Mangili, G.; Bergamini, A.; Candiani, M.; Cioffi, R.; Mais, V.; Rabaiotti, E.; Bocciolone, L. What women want: Fertility sparing surgery in Borderline ovarian tumours patients and pregnancy outcome. Eur. J. Surg. Oncol. 2020, 46, 888–892. [Google Scholar] [CrossRef]
- Suri, A.; Perumal, V.; Ammalli, P.; Suryan, V.; Bansal, S.K. Diagnostic measures comparison for ovarian malignancy risk in Epithelial ovarian cancer patients: A meta-analysis. Sci. Rep. 2021, 11, 17308. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Malignant Disease Patients N = 627 (41.6) | Non-Malignant Disease Patients N = 583 (38.6) | Healthy Women N = 299 (19.8) | |
|---|---|---|---|
| Age (years), n (%) | 59.4 (13.8) | 47.3 (13.9) | 46.6 (13.0) |
| Post-Menopausal Status, n (%) | 473 (75.4) | 220 (37.7) | 144 (48.2) |
| Smokers (n = 1232), n (%) | 124 (26.6) | 140 (28.6) | 47 (17.1) |
| Non-Caucasian Ethnicity, n (%) | 12 (1.9) | 19 (3.3) | 5 (1.7) |
| HE4 (pmol/L), mean (SD) | 474.1 (1207.0) | 59.7 (62.1) | 45.7 (14.7) |
| Adjusted HE4 (pmol/L), mean (SD) | 499.62 (1245.6) | 68.0 (61.7) | 56.3 (14.6) |
| CA125 (IU/mL), mean (SD) | 610.4 (7.9) | 30.1 (65.9) | 15.4 (11.9) |
| Creatinine, mean (SD) | 0.8 (0.2) | 0.7 (0.2) | 0.7 (0.1) |
| Lab1 | Lab2 | Lab3 | Lab4 | Lab5 | Lab6 | |
|---|---|---|---|---|---|---|
| Sample A | 1074.4 | 981.4 | 927.1 | 1008.6 | 1049.0 | 1027.7 |
| Sample B | 574.9 | 497.3 | 492.5 | 513.2 | 501.5 | 532.1 |
| Sample C | 384.1 | 326.4 | 282.4 | 347.8 | 314.4 | 349.7 |
| Sample D | 322.4 | 266.4 | 244.5 | 293.8 | 248.5 | 239.7 |
| Sample E | 219.6 | 183.3 | 163.4 | 209.6 | 174.4 | 202.3 |
| Sample F | 186.5 | 155.9 | 148.3 | 175.7 | 143 | 169.4 |
| Sample G | 121.9 | 105.2 | 88.8 | 115.0 | 95.6 | 112.7 |
| Sample H | 88.9 | 74.55 | 64.2 | 82.7 | 68.7 | 82.9 |
| Sample I | 68.0 | 56.55 | 51.7 | 65.4 | 53.2 | 60.5 |
| Sample J | 30.3 | 25.8 | 26.4 | 26.4 | 28.1 | 26.8 |
| Fixed Bias, α (95% CI) | Ref. | 13.9 (2.3–25.6) | 21.2 (3.4–39.0) | 1.88 (−7.64–11.4) | 33.3 (9.05–57.6) | 13.88 (−7.42–34.96) |
| Proportional Bias, β (95% CI) | Ref. | 1.09 (1.07–1.13) | 1.15 (1.10–1.20) | 1.08 (1.05–1.10) | 1.02 (0.96–1.08) | 1.04 (0.99–1.10) |
| Control Model (Linear Model, n = 882, Dependent Variable: Adjusted HE4) | ROC Model (Generalized Linear Model with Probit Link, n = 1509, 50 Bootstrap Replications) | ||
|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | |
| Creatinine | 112.05 (−28.95; 253.05) | 0.097 | −1.02 (−1.74; −0.29) |
| Menopausal State (yes) | 6.91 (−2.67; 16.49) | 0.123 | 0.52 (0.31; 0.73) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angeloni, A.; De Vito, C.; Farina, A.; Terracciano, D.; Cennamo, M.; Passerini, R.; Bottari, F.; Schirinzi, A.; Vettori, R.; Steffan, A.; et al. New Analytical Approach for the Alignment of Different HE4 Automated Immunometric Systems: An Italian Multicentric Study. J. Clin. Med. 2022, 11, 1994. https://doi.org/10.3390/jcm11071994
Angeloni A, De Vito C, Farina A, Terracciano D, Cennamo M, Passerini R, Bottari F, Schirinzi A, Vettori R, Steffan A, et al. New Analytical Approach for the Alignment of Different HE4 Automated Immunometric Systems: An Italian Multicentric Study. Journal of Clinical Medicine. 2022; 11(7):1994. https://doi.org/10.3390/jcm11071994
Chicago/Turabian StyleAngeloni, Antonio, Corrado De Vito, Antonella Farina, Daniela Terracciano, Michele Cennamo, Rita Passerini, Fabio Bottari, Annalisa Schirinzi, Roberto Vettori, Agostino Steffan, and et al. 2022. "New Analytical Approach for the Alignment of Different HE4 Automated Immunometric Systems: An Italian Multicentric Study" Journal of Clinical Medicine 11, no. 7: 1994. https://doi.org/10.3390/jcm11071994