
Outcomes of Frail Patients While Waiting for Kidney Transplantation: Differences between Physical Frailty Phenotype and FRAIL Scale

 , , , ,
on behalf of the FRAIL-MAR Study Group
, , , ,
on behalf of the FRAIL-MAR Study Group
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethics
2.3. Frailty Assessment
2.4. Study Variables
2.5. Statistics
3. Results
3.1. Comparisons among Candidates Who Received a KT during the Study Period and Those Who Remained Non-Transplanted
3.2. Clinical Outcomes of Frail Patients While Waiting for Transplantation
3.3. Mortality of Frail Patients While Waiting for Transplantation
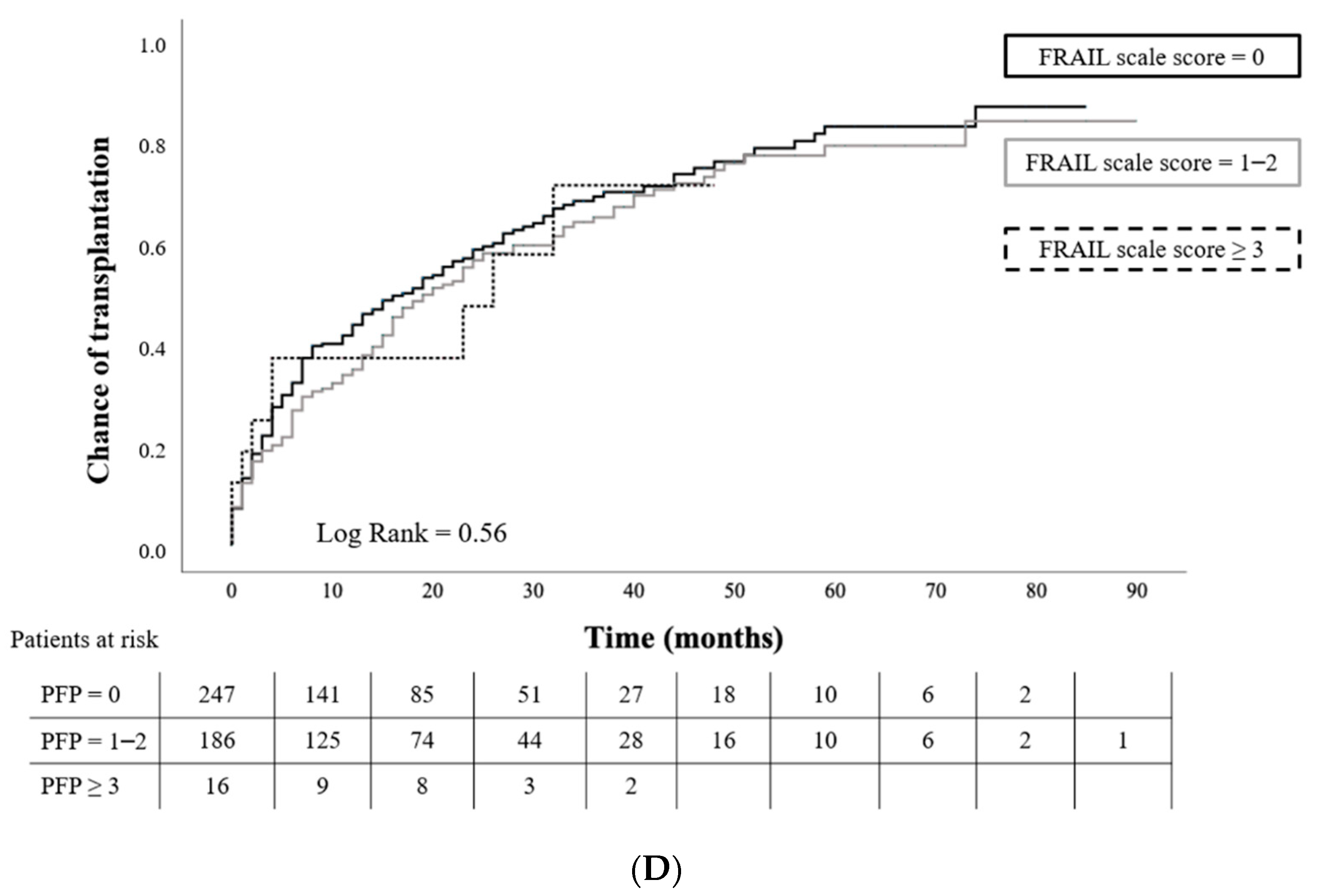
3.4. Chance of Transplantation among KT Candidates and Its Relationship with Frailty Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chowdhury, R.; Peel, N.; Krosch, M.; Hubbard, R. Frailty and chronic kidney disease: A systematic review. Arch. Gerontol. Geriatr. 2017, 68, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Harhay, M.N.; Rao, M.K.; Woodside, K.J.; Johansen, K.L.; Lentine, K.L.; Tullius, S.G.; Parsons, R.F.; Alhamad, T.; Berger, J.; Cheng, X.S.; et al. An overview of frailty in kidney transplantation: Measurement, management and future considerations. Nephrol. Dial. Transplant. 2020, 35, 1099–1112. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Cesari, M.; Gambassi, G.; van Kan, G.A.; Vellas, B. The frailty phenotype and the frailty index: Different instruments for different purposes. Age Ageing 2013, 43, 10–12. [Google Scholar] [CrossRef] [Green Version]
- Oviedo-Briones, M.; Laso, R.; Carnicero, J.A.; Cesari, M.; Grodzicki, T.; Gryglewska, B.; Sinclair, A.; Landi, F.; Vellas, B.; Checa-López, M.; et al. A Comparison of Frailty Assessment Instruments in Different Clinical and Social Care Settings: The Frailtools Project. J. Am. Med. Dir. Assoc. 2020, 22, 607.e7–607.e12. [Google Scholar] [CrossRef]
- Lim, Y.J.; Ng, Y.-S.; Sultana, R.; Tay, E.L.; Mah, S.M.; Chan, C.H.N.; Latib, A.B.; Abu-Bakar, H.M.; Ho, J.C.Y.; Kwek, T.H.H.; et al. Frailty Assessment in Community-Dwelling Older Adults: A Comparison of 3 Diagnostic Instruments. J. Nutr. Health Aging 2020, 24, 582–590. [Google Scholar] [CrossRef]
- Ibrahim, K.; Howson, F.F.A.; Culliford, D.J.; Sayer, A.A.; Roberts, H.C. The feasibility of assessing frailty and sarcopenia in hospitalised older people: A comparison of commonly used tools. BMC Geriatr. 2019, 19, 42. [Google Scholar] [CrossRef]
- Van Loon, I.N.; Goto, N.A.; Boereboom, F.T.; Bots, M.L.; Verhaar, M.C.; Hamaker, M.E. Frailty screening tools for elderly patients incident to dialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1480–1488. [Google Scholar] [CrossRef] [Green Version]
- Kittiskulnam, P.; Chertow, G.M.; Carrero, J.J.; Delgado, C.; Kaysen, G.A.; Johansen, K.L. Sarcopenia and its individual criteria are associated, in part, with mortality among patients on hemodialysis. Kidney Int. 2017, 92, 238–247. [Google Scholar] [CrossRef]
- Fernández, M.P.; Miguel, P.M.; Ying, H.; Haugen, C.E.; Chu, N.; Puyol, D.M.R.; Rodríguez-Mañas, L.; Norman, S.P.; Walston, J.D.; Segev, D.L.; et al. Comorbidity, Frailty, and Waitlist Mortality among Kidney Transplant Candidates of All Ages. Am. J. Nephrol. 2019, 49, 103–110. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Ying, H.; Thomas, A.; Warsame, F.; Shaffer, A.; Haugen, C.E.; Garonzik-Wang, J.M.; Desai, N.M.; Varadhan, R.; Walston, J.; et al. Frailty, Inflammatory Markers, and Waitlist Mortality Among Patients with End-stage Renal Disease in a Prospective Cohort Study. Transplantation 2018, 102, 1740–1746. [Google Scholar] [CrossRef]
- Lorenz, E.C.; Cosio, F.G.; Bernard, S.L.; Bogard, S.D.; Bjerke, B.R.; Geissler, E.N.; Hanna, S.W.; Kremers, W.K.; Cheng, Y.; Stegall, M.D.; et al. The Relationship between Frailty and Decreased Physical Performance with Death on the Kidney Transplant Waiting List. Prog. Transplant. 2019, 29, 108–114. [Google Scholar] [CrossRef]
- Haugen, C.E.; Chu, N.; Ying, H.; Warsame, F.; Holscher, C.M.; Desai, N.M.; Jones, M.R.; Norman, S.P.; Brennan, D.C.; Garonzik-Wang, J.; et al. Frailty and Access to Kidney Transplantation. Clin. J. Am. Soc. Nephrol. 2019, 14, 576–582. [Google Scholar] [CrossRef]
- Harhay, M.N.; Reese, P.P. Frailty and cognitive deficits limit access to kidney transplantation unfair or unavoidable? Clin. J. Am. Soc. Nephrol. 2019, 14, 493–495. [Google Scholar] [CrossRef] [Green Version]
- McAdams-DeMarco, M.A.; Chu, N.M.; Segev, D.L. Frailty and Long-Term Post-Kidney Transplant Outcomes. Curr. Transplant. Rep. 2019, 6, 45–51. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.; Law, A.; King, E.; Orandi, B.; Salter, M.; Gupta, N.; Chow, E.; Alachkar, N.; Desai, N.; Varadhan, R.; et al. Frailty and Mortality in Kidney Transplant Recipients. Am. J. Transplant. 2014, 15, 149–154. [Google Scholar] [CrossRef] [Green Version]
- Quint, E.E.; Zogaj, D.; Banning, L.B.; Benjamens, S.; Annema, C.; Bakker, S.J.; Nieuwenhuijs-Moeke, G.J.; Segev, D.L.; McAdams-DeMarco, M.A.; Pol, R.A. Frailty and Kidney Transplantation: A Systematic Review and Meta-analysis. Transplant. Direct 2021, 7, e701. [Google Scholar] [CrossRef]
- Morley, J.E.; Malmstrom, T.K.; Miller, D.K. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J. Nutr. Health Aging 2012, 16, 601–608. [Google Scholar] [CrossRef] [Green Version]
- McAdams-DeMarco, M.; Law, A.; Tan, J.; Delp, C.; King, E.A.; Orandi, B.; Salter, M.; Alachkar, N.; Desai, N.; Grams, M.; et al. Frailty, Mycophenolate Reduction, and Graft Loss in Kidney Transplant Recipients. Transplantation 2015, 99, 805–810. [Google Scholar] [CrossRef] [Green Version]
- McAdams-DeMarco, M.A.; Olorundare, I.O.; Ying, H.; Warsame, F.; Haugen, C.E.; Hall, R.; Garonzik-Wang, J.M.; Desai, N.M.; Walston, J.D.; Norman, S.P.; et al. Frailty and Postkidney Transplant Health-Related Quality of Life. Transplantation 2018, 102, 291–299. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontology 1969, 9, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Haugen, C.E.; Thomas, A.G.; Chu, N.; Shaffer, A.A.; Norman, S.P.; Bingaman, A.W.; Segev, D.L.; McAdams-DeMarco, M. Prevalence of frailty among kidney transplant candidates and recipients in the United States: Estimates from a National Registry and Multicenter Cohort Study. Am. J. Transplant. 2019, 20, 1170–1180. [Google Scholar] [CrossRef]
- Lynch, R.J.; Zhang, R.; Patzer, R.E.; Larsen, C.P.; Adams, A.B. First-Year Waitlist Hospitalization and Subsequent Waitlist and Transplant Outcome. Am. J. Transplant. 2016, 17, 1031–1041. [Google Scholar] [CrossRef]
- Lynch, R.J.; Zhang, R.; Patzer, R.E.; Larsen, C.P.; Adams, A.B. Waitlist Hospital Admissions Predict Resource Utilization and Survival after Renal Transplantation. Ann. Surg. 2016, 264, 1168–1173. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Law, A.; Salter, M.L.; Boyarsky, B.; Gimenez, L.; Jaar, B.G.; Walston, J.D.; Segev, D.L. Frailty as a novel predictor of mortality and hospitalization in individuals of all ages under-going hemodialysis. J. Am. Geriatr. Soc. 2013, 61, 896–901. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 449) | WL 1 (n = 153) | KT (n = 296) | p-Value a | |
|---|---|---|---|---|
| Sociodemographics | ||||
| Age (years, mean ± sd) | 60.4 ± 14.1 | 61.5 ± 13.5 | 59.8 ± 14.3 | 0.20 |
| Sex (female, n (%)) | 141 (31.4) | 50 (23.7) | 91 (30.7) | 0.67 |
| Ethnicity (Caucasian, n (%)) | 420 (93.5) | 141 (92.2) | 279 (94.3) | 0.21 |
| BMI (Kg/m2, mean ± sd) | 27.9 ± 5.2 | 28.5 ± 5.2 | 27.7 ± 5.1 | 0.17 |
| Education (no/primary, n (%)) | 282 (62.8) | 99 (64.7) | 183 (61.8) | 0.54 |
| Deficient family support, n (%) | 64 (14.2) | 19 (12.4) | 45 (15.3) | 0.41 |
| Socioeconomic status (non-regular incomes, n (%)) | 41 (9.1) | 23 (15) | 18 (6.1) | 0.002 |
| Comorbidities | ||||
| Hypertension, n (%) | 432 (96.2) | 148 (96.7) | 284 (96.3) | 0.80 |
| Diabetes mellitus, n (%) | 164 (36.5) | 63 (41.2) | 101 (34.2) | 0.15 |
| Heart failure, n (%) | 26 (5.8) | 16 (10.5) | 10 (3.4) | 0.002 |
| Ischemic coronary disease, n (%) | 73 (16.3) | 32 (20.9) | 41 (13.9) | 0.055 |
| Peripheral vasculopathy, n (%) | 41 (9.1) | 16 (10.5) | 25 (8.4) | 0.48 |
| Cerebral vasculopathy, n (%) | 35 (7.8) | 13 (8.5) | 22 (7.4) | 0.69 |
| Chronic obstructive pulmonary disease, n (%) | 34 (7.6) | 15 (9.8) | 19 (6.4) | 0.19 |
| RRT modality, n (%) | ||||
| Hemodialysis | 295 (65.7) | 107 (69.9) | 188 (63.5) | |
| Peritoneal dialysis | 93 (20.7) | 22 (14.4) | 71 (24) | 0.06 |
| Low clearance | 61 (13.6) | 24 (17.5) | 37 (12.5) | |
| Dialysis vintage (months, median [IQR]) | 7 (0–14) | 6 (−2–13.5) | 7 (1–14) | 0.19 |
| Disabilities | ||||
| Disability for activities of daily living *, n (%) | 35 (8.7) | 16 (12.3) | 19 (7) | 0.077 |
| Disability for instrumental activities of daily living #, n (%) | 88 (22) | 33 (26) | 55 (20.1) | 0.19 |
| Physical Frailty Phenotype | ||||
| Shrinking, n (%) | 77 (17.1) | 27 (17.6) | 50 (16.9) | 0.84 |
| Exhaustion, n (%) | 108 (24.1) | 43 (28.1) | 65 (22) | 0.14 |
| Low physical activity, n (%) | 25 (5.6) | 12 (7.8) | 13 (4.4) | 0.13 |
| Slowness, n (%) | 61 (13.6) | 29 (19) | 32 (10.8) | 0.02 |
| Weakness, n (%) | 243 (54.1) | 90 (58.8) | 153 (51.7) | 0.15 |
| Hand grip (Kg, mean ± sd) | 26.8 (9.4) | 26.3 (9.8) | 27.1 (9.2) | 0.30 |
| PFP 3 categories (0, 1–2, and ≥3) | ||||
| 0 | 129 (28.7) | 39 (25.5) | 90 (30.4) | |
| 1–2 | 273 (60.8) | 89 (58.2) | 184 (62.2) | 0.013 |
| ≥3 | 47 (10.5) | 25 (16.3) | 22 (7.4) | |
| PFP 2 categories (0 and ≥1) | ||||
| 0 | 129 (28.7) | 39 (25.5) | 90 (30.4) | 0.27 |
| ≥1 | 320 (71.3) | 114 (74.5) | 206 (69.6) | |
| FRAIL scale | ||||
| Fatigue, n (%) | 108 (24.1) | 43 (28.1) | 65 (22) | 0.14 |
| Resistance, n (%) | 42 (9.4) | 24 (15.7) | 18 (6.1) | <0.001 |
| Ambulation, n (%) | 20 (4.5) | 10 (6.5) | 10 (3.4) | 0.12 |
| Illness, n (%) | 55 (12.2) | 18 (11.8) | 37 (12.5) | 0.82 |
| Loss of weight, n (%) | 86 (19.2) | 31 (20.3) | 55 (18.6) | 0.66 |
| FRAIL 3 categories (0, 1–2, and ≥3) | ||||
| 0 | 247 (55) | 82 (53.6) | 165 (55.7) | |
| 1–2 | 186 (41.4) | 64 (41.8) | 122 (41.2) | 0.68 |
| ≥3 | 16 (3.6) | 7 (4.6) | 9 (3) | |
| FRAIL 2 categories (0 and ≥1) | ||||
| 0 | 247 (55) | 82 (53.6) | 165 (55.7) | 0.66 |
| ≥1 | 202 (45) | 71 (46.4) | 131 (44.3) | |
| PFP | |||
|---|---|---|---|
| 0 (n = 72) | ≥1 (n = 205) | p-Value | |
| Hospitalization requirement during 1st year on the WL, n (%) | 15 (20.8) | 89 (43.4) | <0.001 |
| Number of hospitalizations, n (%) | 0.09 | ||
| 0 | 56 (77.8) | 115 (56.1) | |
| 1 | 9 (12.5) | 56 (27.3) | |
| 2 | 2 (2.8) | 22 (10.7) | |
| 3 | 3 (4.2) | 9 (4.4) | |
| >3 | 2 (2.8) | 3 (3) | |
| FRAIL Scale | |||
| 0 (n = 144) | ≥1 (n = 133) | p-Value | |
| Hospitalization requirement during 1st year on the WL, n (%) | 39 (27.1) | 65 (48.9) | <0.001 |
| Number of hospitalizations, n (%) | <0.001 | ||
| 0 | 104 (72.2) | 67 (50.4) | |
| 1 | 29 (20.1) | 36 (27.1) | |
| 2 | 4 (2.8) | 20 (15) | |
| 3 | 4 (2.8) | 8 (6) | |
| >3 | 3 (2.1) | 2 (1.5) | |
| PFP | |||
|---|---|---|---|
| 0 (n = 39) | ≥1 (n = 114) | p-Value | |
| Cardiovascular event, n (%) | 10 (25.6) | 48 (42.1) | 0.07 |
| Major infection event, n (%) | 7 (17.9) | 40 (35.1) | 0.04 |
| Neoplasia, n (%) | 2 (5.1) | 13 (11.4) | 0.25 |
| Dialysis access problem, n (%) | 4 (10.3) | 22 (19.3) | 0.19 |
| Any event, n (%) | 10 (25.6) | 59 (51.9) | 0.005 |
| Number of events > 1, n (%) | 5 (12.8) | 29 (25.4) | 0.10 |
| WL exclusion during the follow-up, n (%) | 9 (23.1) | 65 (57) | <0.001 |
| FRAIL scale | |||
| 0 (n = 82) | ≥1 (n = 71) | p-Value | |
| Cardiovascular event, n (%) | 23 (28) | 35 (49.3) | 0.007 |
| Major infection event, n (%) | 22 (26.8) | 25 (35.2) | 0.26 |
| Neoplasia, n (%) | 8 (9.8) | 7 (9.9) | 0.98 |
| Dialysis access problem, n (%) | 9 (11) | 17 (23.9) | 0.033 |
| Any event, n (%) | 31 (37.8) | 38 (53.1) | 0.05 |
| Number of events > 1, n (%) | 13 (15.9) | 21 (29.6) | 0.03 |
| WL exclusion during the follow-up, n (%) | 29 (35.4) | 45 (63.4) | <0.001 |
| Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|
| HR | CI 95% | p-Value | HR | CI 95% | p-Value | |
| Age (per year) | 1.008 | 1.003–1.013 | 0.03 | 1.098 | 1.003–1.015 | 0.003 |
| Sex (ref: male) | 0.637 | 0.309–1.316 | 0.22 | |||
| Race (ref: Caucasian) | 3.30 | 1.13–9.61 | 0.03 | 1.35 | 0.19 | |
| Hypertension | 20.99 | 0.02–228.17 | 0.51 | |||
| Diabetes mellitus | 1.32 | 0.67–2.60 | 0.43 | |||
| Any cardiovascular disease | 2.37 | 1.20–4.68 | 0.01 | 3.43 | 1.35–8.66 | 0.009 |
| Chronic obstructive pulmonary disease | 1.57 | 0.61–4.06 | 0.35 | |||
| Hemodialysis as RRT modality (ref: HD) | 0.72 | 0.27–1.87 | 0.50 | |||
| Dialysis vintage (per month) | 1.004 | 0.99–1.01 | 0.43 | |||
| PFP (ref: 0) | ||||||
| ≥1 | 3.24 | 0.99–10.61 | 0.05 | 4.07 | 0.78–21.15 | 0.09 |
| PFP (ref: 0) | ||||||
| 1–2 | 2.87 | 0.71–11.4 | 0.13 | 4.05 | 0.77–21.19 | 0.09 |
| ≥3 | 3.35 | 1.01–11.10 | 0.04 | 4.37 | 0.64–29.14 | 0.13 |
| FRAIL scale (ref: 0) | ||||||
| ≥1 | 1.83 | 0.90–3.70 | 0.09 | 1.51 | 0.62–3.70 | 0.35 |
| FRAIL scale (ref: 0) | ||||||
| 1–2 | 1.81 | 0.88–3.70 | 0.15 | 1.51 | 0.66–3.47 | 0.32 |
| ≥3 | 2.06 | 0.46–9.27 | 0.43 | 1.95 | 0.38–9.98 | 0.41 |
| Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|
| HR | CI 95% | p-Value | HR | CI 95% | p-Value | |
| Age (per year) | 0.99 | 0.98–1.01 | 0.64 | |||
| Sex (ref: male) | 0.80 | 0.62–1.02 | 0.08 | 0.81 | 0.62–1.06 | 0.14 |
| Hypertension | 1.01 | 0.55–1.84 | 0.97 | |||
| Diabetes mellitus | 0.83 | 0.65–1.06 | 0.14 | |||
| Any cardiovascular disease | 0.72 | 0.55–0.94 | 0.01 | 0.72 | 0.54–0.95 | 0.02 |
| Chronic obstructive pulmonary disease | 0.82 | 0.51–1.30 | 0.40 | |||
| Hemodialysis as RRT modality (ref: HD) | 0.94 | 0.63–1.41 | 0.78 | |||
| Dialysis vintage (per month) | 1.005 | 1.001–1.008 | 0.01 | 1.005 | 1.001–1.009 | 0.007 |
| PFP (ref: 0) | ||||||
| ≥1 | 0.76 | 0.60–0.98 | 0.03 | 0.78 | 0.59–1.03 | 0.08 |
| PFP (ref: 0) | ||||||
| 1–2 | 0.82 | 0.64–1.06 | 0.13 | 0.83 | 0.63–1.09 | 0.19 |
| ≥3 | 0.49 | 0.30–0.78 | 0.003 | 0.45 | 0.26–0.77 | 0.004 |
| FRAIL scale (ref: 0) | ||||||
| ≥1 | 0.88 | 0.70–1.11 | 0.29 | 0.84 | 0.65–1.08 | 0.19 |
| FRAIL scale (ref: 0) | ||||||
| 1–2 | 0.88 | 0.70–1.11 | 0.30 | 0.85 | 0.66–1.10 | 0.23 |
| ≥3 | 0.87 | 0.44–0.71 | 0.70 | 0.70 | 0.32–1.51 | 0.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Sáez, M.J.; Redondo-Pachón, D.; Arias-Cabrales, C.E.; Faura, A.; Bach, A.; Buxeda, A.; Burballa, C.; Junyent, E.; Crespo, M.; Marco, E.; et al. Outcomes of Frail Patients While Waiting for Kidney Transplantation: Differences between Physical Frailty Phenotype and FRAIL Scale. J. Clin. Med. 2022, 11, 672. https://doi.org/10.3390/jcm11030672
Pérez-Sáez MJ, Redondo-Pachón D, Arias-Cabrales CE, Faura A, Bach A, Buxeda A, Burballa C, Junyent E, Crespo M, Marco E, et al. Outcomes of Frail Patients While Waiting for Kidney Transplantation: Differences between Physical Frailty Phenotype and FRAIL Scale. Journal of Clinical Medicine. 2022; 11(3):672. https://doi.org/10.3390/jcm11030672
Chicago/Turabian StylePérez-Sáez, María José, Dolores Redondo-Pachón, Carlos E. Arias-Cabrales, Anna Faura, Anna Bach, Anna Buxeda, Carla Burballa, Ernestina Junyent, Marta Crespo, Ester Marco, and et al. 2022. "Outcomes of Frail Patients While Waiting for Kidney Transplantation: Differences between Physical Frailty Phenotype and FRAIL Scale" Journal of Clinical Medicine 11, no. 3: 672. https://doi.org/10.3390/jcm11030672