


Exploring the Importance of Corticalization Occurring in Alveolar Bone Surrounding a Dental Implant


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chęcińska, K.; Chęciński, M.; Sikora, M.; Nowak, Z.; Karwan, S.; Chlubek, D. The Effect of Zirconium Dioxide (ZrO2) Nanoparticles Addition on the Mechanical Parameters of Polymethyl Methacrylate (PMMA): A Systematic Review and Meta-Analysis of Experimental Studies. Polymers 2022, 14, 1047. [Google Scholar] [CrossRef] [PubMed]
- Pokrowiecki, R.; Szałaj, U.; Fudala, D.; Zaręba, T.; Wojnarowicz, J.; Łojkowski, W.; Tyski, S.; Dowgierd, K.; Mielczarek, A. Dental Implant Healing Screws as Temporary Oral Drug Delivery Systems for Decrease of Infections in the Area of the Head and Neck. Int. J. Nanomed. 2022, 17, 1679–1693. [Google Scholar] [CrossRef]
- Hadzik, J.; Kubasiewicz-Ross, P.; Simka, W.; Gębarowski, T.; Barg, E.; Cieśla-Niechwiadowicz, A.; Szajna, A.T.; Szajna, E.; Gedrange, T.; Kozakiewicz, M.; et al. Fractal Dimension and Texture Analysis in the Assessment of Experimental Laser-Induced Periodic Surface Structures (LIPSS) Dental Implant Surface—In Vitro Study Preliminary Report. Materials 2022, 15, 2713. [Google Scholar] [CrossRef] [PubMed]
- Wach, T.; Kozakiewicz, M. Comparison of Two Clinical Procedures in Patient Affected with Bone Deficit in Posterior Mandible. Dent. Med. Probl. 2016, 53, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Dowgierd, K.; Borowiec, M.; Kozakiewicz, M. Bone changes on lateral cephalograms and CBCT during treatment of maxillary narrowing using palatal osteodistraction with bone-anchored appliances. J. Cranio-Maxillofac. Surg. 2018, 46, 2069–2081. [Google Scholar] [CrossRef] [PubMed]
- Dowgierd, K.; Lipowicz, A.; Kulesa-Mrowiecka, M.; Wolański, W.; Linek, P.; Myśliwiec, A. Efficacy of immediate physiotherapy after surgical release of zygomatico-coronoid ankylosis in a young child: A case report. Physiother. Theory Pract. 2022, 38, 3187–3193. [Google Scholar] [CrossRef] [PubMed]
- Dowgierd, K.; Pokrowiecki, R.; Borowiec, M.; Sokolowska, Z.; Dowgierd, M.; Wos, J.; Kozakiewicz, M.; Krakowczyk, Ł. Protocol and Evaluation of 3D-Planned Microsurgical and Dental Implant Reconstruction of Maxillary Cleft Critical Size Defects in Adolescents and Young Adults. J. Clin. Med. 2021, 10, 2267. [Google Scholar] [CrossRef] [PubMed]
- Michalak, P.; Wyszyńska-Pawelec, G.; Szuta, M.; Hajto-Bryk, J.; Zapała, J.; Zarzecka, J.K. Fractures of the Craniofacial Skeleton in the Elderly: Retrospective Studies. Int. J. Environ. Res. Public Health 2021, 18, 11219. [Google Scholar] [CrossRef]
- Iezzi, G.; Pecora, G.; Scarano, A.; Perrotti, V.; Piattelli, A. Immediately loaded screw implant retrieved after a 12-year loading period: A histologic and histomorphometric case report. J. Osseointegration 2009, 1, 54–59. [Google Scholar] [CrossRef]
- Tumedei, M.; Piattelli, A.; Degidi, M.; Mangano, C.; Iezzi, G. A Narrative Review of the Histological and Histomorphometrical Evaluation of the Peri-Implant Bone in Loaded and Unloaded Dental Implants. A 30-Year Experience (1988–2018). Int. J. Environ. Res. Public Health 2020, 17, 2088. [Google Scholar] [CrossRef]
- Yonezawa, D.; Piattelli, A.; Favero, R.; Ferri, M.; Iezzi, G.; Botticelli, D. Bone Healing at Functionally Loaded and Unloaded Screw-Shaped Implants Supporting Single Crowns: A Histomorphometric Study in Humans. Int. J. Oral Maxillofac. Implant. 2018, 33, 181–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, F.G.; Pires, J.T.; Shibli, J.A.; Mijiritsky, E.; Iezzi, G.; Piattelli, A.; Mangano, C. Early Bone Response to Dual Acid-Etched and Machined Dental Implants Placed in the Posterior Maxilla: A Histologic and Histomorphometric Human Study. Implant Dent. 2017, 26, 24–29. [Google Scholar] [CrossRef]
- Mangano, C.; Piattelli, A.; Mortellaro, C.; Mangano, F.; Perrotti, V.; Iezzi, G. Evaluation of Peri-Implant Bone Response in Implants Retrieved for Fracture After More Than 20 Years of Loading: A Case Series. J. Oral Implantol. 2015, 41, 414–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traini, T.; Mangano, C.; Perrotti, V.; Caputi, S.; Coelho, P.; Piattelli, A.; Iezzi, G. Human bone reactions around implants with adverse interfacial bone strain over 20 years. J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 1342–1352. [Google Scholar] [CrossRef]
- Piattelli, A.; Artese, L.; Penitente, E.; Iaculli, F.; Degidi, M.; Mangano, C.; Shibli, J.A.; Coelho, P.G.; Perrotti, V.; Iezzi, G. Osteocyte density in the peri-implant bone of implants retrieved after different time periods (4 weeks to 27 years). J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Iezzi, G.; Piattelli, A.; Mangano, C.; Shibli, J.A.; Vantaggiato, G.; Frosecchi, M.; Di Chiara, C.; Perrotti, V. Peri-implant bone tissues around retrieved human implants after time periods longer than 5 years: A retrospective histologic and histomorphometric evaluation of 8 cases. Odontology 2014, 102, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Mangano, C.; Piattelli, A.; Mangano, F.; Rustichelli, F.; Shibli, J.A.; Iezzi, G.; Giuliani, A. Histological and synchrotron radiation-based computed microtomography study of 2 human-retrieved direct laser metal formed titanium implants. Implant Dent. 2013, 22, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Mangano, C.; Perrotti, V.; Raspanti, M.; Mangano, F.; Luongo, G.; Piattelli, A.; Iezzi, G. Human Dental Implants with a Sandblasted, Acid-Etched Surface Retrieved After 5 and 10 Years: A Light and Scanning Electron Microscopy Evaluation of Two Cases. Int. J. Oral Maxillofac. Implant. 2013, 28, 917–920. [Google Scholar] [CrossRef] [Green Version]
- Iezzi, G.; Degidi, M.; Shibli, J.; Vantaggiato, G.; Piattelli, A.; Perrotti, V. Bone Response to Dental Implants After a 3- to 10-Year Loading Period: A Histologic and Histomorphometric Report of Four Cases. Int. J. Periodontics Restor. Dent. 2013, 33, 755–761. [Google Scholar] [CrossRef] [Green Version]
- Iezzi, G.; Degidi, M.; Piattelli, A.; Shibli, J.A.; Perrotti, V. A Histological and Histomorphometrical Evaluation of Retrieved Human Implants with a Wettable, Highly Hydrophilic, Hierarchically Microstructured Surface: A retrospective analysis of 14 implants. Implant Dent. 2013, 22, 138–142. [Google Scholar] [CrossRef]
- Iezzi, G.; Vantaggiato, G.; Shibli, J.A.; Fiera, E.; Falco, A.; Piattelli, A.; Perrotti, V. Machined and sandblasted human dental implants retrieved after 5 years: A histologic and histomorphometric analysis of three cases. Quintessence Int. 2012, 43, 287–292. [Google Scholar] [PubMed]
- Degidi, M.; Perrotti, V.; Piattelli, A.; Iezzi, G. Mineralized bone-implant contact and implant stability quotient in 16 human implants retrieved after early healing periods: A histologic and histomorphometric evaluation. Int. J. Oral Maxillofac. Implant. 2010, 25, 45–48. [Google Scholar]
- Shibli, J.A.; Mangano, C.; D’Avila, S.; Piattelli, A.; Pecora, G.E.; Mangano, F.; Onuma, T.; Cardoso, L.A.; Ferrari, D.S.; Aguiar, K.C.; et al. Influence of direct laser fabrication implant topography on type IV bone: A histomorphometric study in humans. J. Biomed. Mater. Res. Part A 2010, 93, 607–614. [Google Scholar] [CrossRef]
- Shibli, J.A.; Grassi, S.; Piattelli, A.; Pecora, G.E.; Ferrari, D.S.; Onuma, T.; D’Avila, S.; Coelho, P.G.; Barros, R.; Iezzi, G. Histomorphometric Evaluation of Bioceramic Molecular Impregnated and Dual Acid-Etched Implant Surfaces in the Human Posterior Maxilla. Clin. Implant Dent. Relat. Res. 2010, 12, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Vantaggiato, G.; Iezzi, G.; Fiera, E.; Perrotti, V.; Piattelli, A. Histologic and Histomorphometric Report of Three Immediately Loaded Screw Implants Retrieved from Man After a Three-Year Loading Period. Implant Dent. 2008, 17, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, D.; Iezzi, G.; Scarano, A.; Perrotti, V.; Piattelli, A. Immediately Loaded Blade Implant Retrieved from a Man After a 20-year Loading Period: A Histologic and Histomorphometric Case Report. J. Oral Implantol. 2006, 32, 171–176. [Google Scholar] [CrossRef]
- Romanos, G.E.; Testori, T.; Degidi, M.; Piattelli, A. Histologic and Histomorphometric Findings from Retrieved, Immediately Occlusally Loaded Implants in Humans. J. Periodontol. 2005, 76, 1823–1832. [Google Scholar] [CrossRef]
- Degidi, M.; Scarano, A.; Iezzi, G.; Piattelli, A. Histologic and Histomorphometric Analysis of an Immediately Loaded Implant Retrieved from Man after 14 Months of Loading. J. Long-Term Eff. Med. Implant. 2005, 15, 489–498. [Google Scholar] [CrossRef]
- Degidi, M.; Petrone, G.; Iezzi, G.; Piattelli, A. Histologic evaluation of a human immediately loaded titanium implant with a porous anodized surface. Clin. Implant Dent. Relat. Res. 2002, 4, 110–114. [Google Scholar] [CrossRef]
- Piattelli, A.; Scarano, A.; Piattelli, M.; Bertolai, R.; Panzoni, E. Histologic Aspects of the Bone and Soft Tissues Surrounding Three Titanium Non-Submerged Plasma-Sprayed Implants Retrieved at Autopsy: A Case Report. J. Periodontol. 1997, 68, 694–700. [Google Scholar] [CrossRef]
- Trisi, P.; Quaranta, M.; Emanuelli, M.; Piattelli, A. A Light Microscopy, Scanning Electron Microscopy, and Laser Scanning Microscopy Analysis of Retrieved Blade Implants After 7 to 20 Years of Clinical Function. A Report of 3 Cases. J. Periodontol. 1993, 64, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Shibli, J.A.; Mangano, C.; Mangano, F.; Rodrigues, J.A.; Cassoni, A.; Bechara, K.; Ferreia, J.D.B.; Dottore, A.M.; Iezzi, G.; Piattelli, A. Bone-to-Implant Contact Around Immediately Loaded Direct Laser Metal-Forming Transitional Implants in Human Posterior Maxilla. J. Periodontol. 2013, 84, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Piattelli, A.; Shibli, J.A.; Perrotti, V.; Iezzi, G. Early bone formation around immediately restored implants with and without occlusal contact: A human histologic and histomorphometric evaluation. Case report. Int. J. Oral Maxillofac. Implant. 2009, 24, 734–739. [Google Scholar]
- Degidi, M.; Piattelli, A.; Shibli, J.A.; Perrotti, V.; Iezzi, G. Bone formation around immediately loaded and submerged dental implants with a modified sandblasted and acid-etched surface after 4 and 8 weeks: A human histologic and histomorphometric analysis. Int. J. Oral Maxillofac. Implant. 2009, 24, 896–901. [Google Scholar]
- Degidi, M.; Scarano, A.; Petrone, G.; Piattelli, A. Histologic Analysis of Clinically Retrieved Immediately Loaded Titanium Implants: A Report of 11 Cases. Clin. Implant Dent. Relat. Res. 2003, 5, 89–94. [Google Scholar] [CrossRef]
- Piattelli, A.; Trisi, P.; Romasco, N.; Emanuelli, M. Histologic analysis of a screw implant retrieved from man: Influence of early loading and primary stability. J. Oral Implantol. 1993, 19, 303–306. [Google Scholar]
- Rasperini, G.; Siciliano, V.I.; Cafiero, C.; Salvi, G.E.; Blasi, A.; Aglietta, M. Crestal Bone Changes at Teeth and Implants in Periodontally Healthy and Periodontally Compromised Patients. A 10-Year Comparative Case-Series Study. J. Periodontol. 2014, 85, e152–e159. [Google Scholar] [CrossRef]
- Degidi, M.; Scarano, A.; Iezzi, G.; Piattelli, A. Histologic Analysis of an Immediately Loaded Implant Retrieved after 2 Months. J. Oral Implantol. 2005, 31, 247–254. [Google Scholar] [CrossRef]
- Traini, T.; Pecora, G.; Iezzi, G.; Piattelli, A. Preferred Collagen Fiber Orientation in Human Peri-implant Bone After a Short- and Long-term Loading Period: A Case Report. J. Oral Implantol. 2006, 32, 177–181. [Google Scholar] [CrossRef]
- Traini, T.; Degidi, M.; Caputi, S.; Strocchi, R.; Di Iorio, D.; Piattelli, A. Collagen Fiber Orientation in Human Peri-Implant Bone Around Immediately Loaded and Unloaded Titanium Dental Implants. J. Periodontol. 2005, 76, 83–89. [Google Scholar] [CrossRef]
- Traini, T.; Degidi, M.; Iezzi, G.; Artese, L.; Piattelli, A. Comparative evaluation of the peri-implant bone tissue mineral density around unloaded titanium dental implants. J. Dent. 2007, 35, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Zamparini, F.; Iezzi, G.; Degidi, M.; Botticelli, D.; Piattelli, A.; Prati, C. Microchemical and Micromorphologic ESEM-EDX Analysis of Bone Mineralization at the Thread Interface in Human Dental Implants Retrieved for Mechanical Complications after 2 Months to 17 Years. Int. J. Periodontics Restor. Dent. 2018, 38, 431–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, C.; Harrison, J.; Reed, R.; Cruickshank, B. Bone apposition rate as an index of bone metabolism. Metabolism 1978, 27, 143–150. [Google Scholar] [CrossRef]
- Pazzaglia, U.E.; Congiu, T.; Marchese, M.; Spagnuolo, F.; Quacci, D. Morphometry and Patterns of Lamellar Bone in Human Haversian Systems. Anat. Rec. Adv. Integr. Anat. Evol. Biol. 2012, 295, 1421–1429. [Google Scholar] [CrossRef]
- Kungsadalpipob, K.; Supanimitkul, K.; Manopattanasoontorn, S.; Sophon, N.; Tangsathian, T.; Arunyanak, S.P. The lack of keratinized mucosa is associated with poor peri-implant tissue health: A cross-sectional study. Int. J. Implant Dent. 2020, 6, 28. [Google Scholar] [CrossRef]
- Albrektsson, T.; Brånemark, P.-I.; Hansson, H.-A.; Lindström, J. Osseointegrated Titanium Implants: Requirements for Ensuring a Long-Lasting, Direct Bone-to-Implant Anchorage in Man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brånemark, P.; Adell, R.; Albrektsson, T.; Lekholm, U.; Lundkvist, S.; Rockler, B. Osseointegrated titanium fixtures in the treatment of edentulousness. Biomaterials 1983, 4, 25–28. [Google Scholar] [CrossRef]
- Linkevicius, T.; Puisys, A.; Linkeviciene, L.; Peciuliene, V.; Schlee, M. Crestal Bone Stability around Implants with Horizontally Matching Connection after Soft Tissue Thickening: A Prospective Clinical Trial. Clin. Implant Dent. Relat. Res. 2015, 17, 497–508. [Google Scholar] [CrossRef]
- Vlachodimou, E.; Fragkioudakis, I.; Vouros, I. Is There an Association between the Gingival Phenotype and the Width of Keratinized Gingiva? A Systematic Review. Dent. J. 2021, 9, 34. [Google Scholar] [CrossRef]
- Baer, R.A.; Nölken, R.; Colic, S.; Heydecke, G.; Mirzakhanian, C.; Behneke, A.; Behneke, N.; Gottesman, E.; Ottria, L.; Pozzi, A.; et al. Immediately provisionalized tapered conical connection implants for single-tooth restorations in the maxillary esthetic zone: A 5-year prospective single-cohort multicenter analysis. Clin. Oral Investig. 2022, 26, 3593–3604. [Google Scholar] [CrossRef]
- Kinaia, B.M.; Shah, M.; Neely, A.L.; Goodis, H.E. Crestal Bone Level Changes Around Immediately Placed Implants: A Systematic Review and Meta-Analyses With at Least 12 Months’ Follow-Up After Functional Loading. J. Periodontol. 2014, 85, 1537–1548. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Linkevicius, R.; Gineviciute, E.; Alkimavicius, J.; Mazeikiene, A.; Linkeviciene, L. The influence of new immediate tissue level abutment on crestal bone stability of subcrestally placed implants: A 1-year randomized controlled clinical trial. Clin. Implant Dent. Relat. Res. 2021, 23, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Puisys, A.; Linkevicius, R.; Alkimavicius, J.; Gineviciute, E.; Linkeviciene, L. The influence of submerged healing abutment or subcrestal implant placement on soft tissue thickness and crestal bone stability. A 2-year randomized clinical trial. Clin. Implant Dent. Relat. Res. 2020, 22, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Kołaciński, M.; Kozakiewicz, M.; Materka, A. Textural entropy as a potential feature for quantitative assessment of jaw bone healing process. Arch. Med. Sci. 2015, 11, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Dewan, H.; Robaian, A.; Divakar, D.D.; Hegde, S.M.R.; Shankar, S.M.; Poojari, B. Levels of peri-implant sulcular fluid levels of soluble urokinase plasminogen activator receptor and TNF-α among cigarette smokers and non-smokers with peri-implantitis. Technol. Health Care 2022. epub ahead of print. [Google Scholar] [CrossRef]
- Naveau, A.; Shinmyouzu, K.; Moore, C.; Avivi-Arber, L.; Jokerst, J.; Koka, S. Etiology and Measurement of Peri-Implant Crestal Bone Loss (CBL). J. Clin. Med. 2019, 8, 166. [Google Scholar] [CrossRef] [Green Version]
- Bohner, L.; Tortamano, P.; Meier, N.; Gremse, F.; Kleinheinz, J.; Hanisch, M. Trabecular Bone Assessment Using Magnetic-Resonance Imaging: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 9282. [Google Scholar] [CrossRef]
- Guenoun, D.; Fouré, A.; Pithioux, M.; Guis, S.; Le Corroller, T.; Mattei, J.-P.; Pauly, V.; Guye, M.; Bernard, M.; Chabrand, P.; et al. Correlative Analysis of Vertebral Trabecular Bone Microarchitecture and Mechanical Properties: A Combined Ultra-High Field (7 Tesla) MRI and Biomechanical Investigation. Spine 2017, 42, E1165–E1172. [Google Scholar] [CrossRef]
- Hadrowicz, J.; Hadrowicz, P.; Gesing, A.; Kozakiewicz, M. Age dependent alteration in bone surrounding dental implant. Dent. Med. Probl. 2014, 51, 27–34. [Google Scholar]
- Hadrowicz, P.; Hadrowicz, J.; Kozakiewicz, M.; Gesing, A. Assessment of Parathyroid Hormone Serum Level as a Predictor for Bone Condition Around Dental Implants. Int. J. Oral Maxillofac. Implant. 2017, 32, e207–e212. [Google Scholar] [CrossRef]
- Kozakiewicz, M.; Szyszkowski, A. Evaluation of selected prognostic factors in dental implant treatment–two-year follow-up. Dent. Med. Probl. 2014, 51, 439–447. [Google Scholar]
- Rózyło-Kalinowska, I. Digital radiography density measurements in differentiation between periapical granulomas and radicular cysts. Med. Sci. Monit. 2007, 13 (Suppl. 1), 129–136. [Google Scholar] [PubMed]
- Szyszkowski, A.; Kozakiewicz, M. Effect of Implant-Abutment Connection Type on Bone Around Dental Implants in Long-Term Observation: Internal cone versus internal hex. Implant Dent. 2019, 28, 430–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wach, T.; Kozakiewicz, M. Are recent available blended collagen-calcium phosphate better than collagen alone or crystalline calcium phosphate? Radiotextural analysis of a 1-year clinical trial. Clin. Oral Investig. 2021, 25, 3711–3718. [Google Scholar] [CrossRef] [PubMed]
- Grocholewicz, K.; Janiszewska-Olszowska, J.; Aniko-Włodarczyk, M.; Preuss, O.; Trybek, G.; Sobolewska, E.; Lipski, M. Panoramic radiographs and quantitative ultrasound of the radius and phalanx III to assess bone mineral status in postmenopausal women. BMC Oral Health 2018, 18, 127. [Google Scholar] [CrossRef] [PubMed]
- Bayrakdar, I.S.; Orhan, K.; Çelik, Ö.; Bilgir, E.; Sağlam, H.; Kaplan, F.A.; Görür, S.A.; Odabaş, A.; Aslan, A.F.; Różyło-Kalinowska, I. A U-Net Approach to Apical Lesion Segmentation on Panoramic Radiographs. BioMed Res. Int. 2022, 2022, 7035367. [Google Scholar] [CrossRef] [PubMed]
- Bilgir, E.; Bayrakdar, I.; Çelik, Ö.; Orhan, K.; Akkoca, F.; Sağlam, H.; Odabaş, A.; Aslan, A.F.; Ozcetin, C.; Kıllı, M.; et al. An artificial intelligence approach to automatic tooth detection and numbering in panoramic radiographs. BMC Med. Imaging 2021, 21, 124. [Google Scholar] [CrossRef] [PubMed]
- Srebrzyńska-Witek, A.; Koszowski, R.; Różyło-Kalinowska, I. Relationship between anterior mandibular bone thickness and the angulation of incisors and canines—A CBCT study. Clin. Oral Investig. 2018, 22, 1567–1578. [Google Scholar] [CrossRef]
- Moshfeghi, M.; Safi, Y.; Różyło-Kalinowska, I.; Gandomi, S. Does the size of an object containing dental implant affect the expression of artifacts in cone beam computed tomography imaging? Head Face Med. 2022, 18, 20. [Google Scholar] [CrossRef]
- Bohner, L.; Hanisch, M.; Sesma, N.; Blanck-Lubarsch, M.; Kleinheinz, J. Artifacts in magnetic resonance imaging caused by dental materials: A systematic review. Dentomaxillofacial Radiol. 2022, 51, 20210450. [Google Scholar] [CrossRef]
- Chang, G.; Honig, S.; Liu, Y.; Chen, C.; Chu, K.K.; Rajapakse, C.S.; Egol, K.; Xia, D.; Saha, P.K.; Regatte, R.R. 7 Tesla MRI of bone microarchitecture discriminates between women without and with fragility fractures who do not differ by bone mineral density. J. Bone Miner. Metab. 2015, 33, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Guenoun, D.; Pithioux, M.; Souplet, J.-C.; Guis, S.; Le Corroller, T.; Fouré, A.; Pauly, V.; Mattei, J.-P.; Bernard, M.; Guye, M.; et al. Assessment of proximal femur microarchitecture using ultra-high field MRI at 7 Tesla. Diagn. Interv. Imaging 2020, 101, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Krug, R.; Carballido-Gamio, J.; Banerjee, S.; Burghardt, A.J.; Link, T.M.; Majumdar, S. In vivo ultra-high-field magnetic resonance imaging of trabecular bone microarchitecture at 7 T. J. Magn. Reson. Imaging 2008, 27, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Rajapakse, C.S.; Magland, J.; Zhang, X.H.; Liu, X.S.; Wehrli, S.L.; Guo, X.E.; Wehrli, F.W. Implications of noise and resolution on mechanical properties of trabecular bone estimated by image-based finite-element analysis. J. Orthop. Res. 2009, 27, 1263–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajapakse, C.S.; Kobe, E.; Batzdorf, A.S.; Hast, M.W.; Wehrli, F.W. Accuracy of MRI-based finite element assessment of distal tibia compared to mechanical testing. Bone 2018, 108, 71–78. [Google Scholar] [CrossRef]
- Seifert, A.C.; Wehrli, F.W. Solid-State Quantitative 1H and 31P MRI of Cortical Bone in Humans. Curr. Osteoporos. Rep. 2016, 14, 77–86. [Google Scholar] [CrossRef]
- Dudek, D.; Kozakiewicz, M. Szerokość beleczek kostnych w szczęce i żuchwie człowieka na podstawie cyfrowych radiologicznych zdjęć wewnąrzustnych [Bone trabecula width in the human maxilla and mandible based on digital intraoral radiographs]. Mag. Stomatol. 2012, 236, 77–80. [Google Scholar]
- Rózyło-Kalinowska, I.; Michalska, A.; Burdan, F. Optimization of analysis of skeletal ossification of laboratory animals by means of digital radiography software options. Ann. Univ. Mariae Curie-Sklodowska 2003, 58, 95–100. [Google Scholar]
- Kozakiewicz, M.; Skorupska, M.; Wach, T. What Does Bone Corticalization around Dental Implants Mean in Light of Ten Years of Follow-Up? J. Clin. Med. 2022, 11, 3545. [Google Scholar] [CrossRef]
- Kozakiewicz, M. Measures of Corticalization. J. Clin. Med. 2022, 11, 5463. [Google Scholar] [CrossRef]
- Kozakiewicz, M.; Wilamski, M. Technika standaryzacji wewnątrzustnych zdjęć rentgenowskich [Standardization technique for intraoral radiographs]. Czas. Stomatol. 1999, 52, 673–677. [Google Scholar]
- Szczypiński, P.M.; Strzelecki, M.; Materka, A.; Klepaczko, A. MaZda–The Software Package for Textural Analysis of Biomedical Images. In Computers in Medical Activity; Advances in Intelligent and Soft Computing; Springer: Berlin/Heidelberg, Germany, 2009; Volume 65, pp. 73–84. [Google Scholar]
- Kozakiewicz, M.; Bogusiak, K.; Hanclik, M.; Denkowski, M.; Arkuszewski, P. Noise in subtraction images made from pairs of intraoral radiographs: A comparison between four methods of geometric alignment. Dentomaxillofacial Radiol. 2008, 37, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Kozakiewicz, M.; Szymor, P.; Wach, T. Influence of General Mineral Condition on Collagen-Guided Alveolar Crest Augmentation. Materials 2020, 13, 3649. [Google Scholar] [CrossRef] [PubMed]
- Kozakiewicz, M.; Wach, T. New Oral Surgery Materials for Bone Reconstruction—A Comparison of Five Bone Substitute Materials for Dentoalveolar Augmentation. Materials 2020, 13, 2935. [Google Scholar] [CrossRef]
- Wach, T.; Kozakiewicz, M. Fast-Versus Slow-Resorbable Calcium Phosphate Bone Substitute Materials—Texture Analysis after 12 Months of Observation. Materials 2020, 13, 3854. [Google Scholar] [CrossRef]
- Haralick, R.M. Statistical and structural approaches to texture. Proc. IEEE 1979, 67, 786–804. [Google Scholar] [CrossRef]
- Materka, A.; Strzelecki, M. Texture Analysis Methods–A Review, COST B11 Report. Presented at MC Meeting and Workshop, Brussels, Belgium, 25 June 1998; Technical University of Lodz: Lodz, Poland, 1998. [Google Scholar]
- Eriksson, R.A.; Albrektsson, T.; Magnusson, B. Assessment of Bone Viability After Heat Trauma: A Histological, Histochemical and Vital Microscopic Study in the Rabbit. Scand. J. Plast. Reconstr. Surg. 1984, 18, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Dahlin, C.; Jemt, T.; Sennerby, L.; Turri, A.; Wennerberg, A. Is Marginal Bone Loss around Oral Implants the Result of a Provoked Foreign Body Reaction? Clin. Implant. Dent. Relat. Res. 2014, 16, 155–165. [Google Scholar] [CrossRef]
- Buser, D.; Janner, S.F.M.; Wittneben, J.-G.; Brägger, U.; Ramseier, C.A.; Salvi, G.E. 10-Year Survival and Success Rates of 511 Titanium Implants with a Sandblasted and Acid-Etched Surface: A Retrospective Study in 303 Partially Edentulous Patients. Clin. Implant. Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar] [CrossRef]
- Szczypinski, P.M.; Klepaczko, A.; Kociolek, M. QMaZda—Software tools for image analysis and pattern recognition. In Proceedings of the 2017 Signal Processing: Algorithms, Architectures, Arrangements, and Applications (SPA), Poznan, Poland, 20–22 September 2017; pp. 217–221. [Google Scholar] [CrossRef]
- Albrektsson, T.; Tengvall, P.; Amengual-Peñafiel, L.; Coli, P.; Kotsakis, G.; Cochran, D.L. Implications of considering peri-implant bone loss a disease, a narrative review. Clin. Implant Dent. Relat. Res. 2022, 24, 532–543. [Google Scholar] [CrossRef]
- Roccuzzo, M.; De Angelis, N.; Bonino, L.; Aglietta, M. Ten-year results of a three-arm prospective cohort study on implants in periodontally compromised patients. Part 1: Implant loss and radiographic bone loss. Clin. Oral Implant. Res. 2010, 21, 490–496. [Google Scholar] [CrossRef]
- Pandey, C.; Rokaya, D.; Bhattarai, B.P. Contemporary Concepts in Osseointegration of Dental Implants: A Review. BioMed Res. Int. 2022, 2022, 6170452. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chen, C.-J.; Singh, M.; Weber, H.-P.; Gallucci, G.O. Success criteria in implant dentistry: A systematic review. J. Dent. Res. 2012, 91, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Amengual-Peñafiel, L.; Córdova, L.A.; Jara-Sepúlveda, M.C.; Brañes-Aroca, M.; Marchesani-Carrasco, F.; Cartes-Velásquez, R. Osteoimmunology drives dental implant osseointegration: A new paradigm for implant dentistry. Jpn. Dent. Sci. Rev. 2021, 57, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Wu, C.; Xiao, Y. Convergence of Osteoimmunology and Immunomodulation for the Development and Assessment of Bone Biomaterials. In The Immune Response to Implanted Materials and Devices; Corradetti, B., Ed.; Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- Negrescu, A.-M.; Cimpean, A. The State of the Art and Prospects for Osteoimmunomodulatory Biomaterials. Materials 2021, 14, 1357. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Li, Q.; Zhang, D.; Zhang, X.; Qi, X.; Wang, Q.; Chen, Y.; Liu, C.; Li, H.; Zhang, S.; et al. Mapping the immune microenvironment for mandibular alveolar bone homeostasis at single-cell resolution. Bone Res. 2021, 9, 17. [Google Scholar] [CrossRef]
- Atcha, H.; Meli, V.S.; Davis, C.T.; Brumm, K.T.; Anis, S.; Chin, J.; Jiang, K.; Pathak, M.M.; Liu, W.F. Crosstalk Between CD11b and Piezo1 Mediates Macrophage Responses to Mechanical Cues. Front. Immunol. 2021, 12, 689397. [Google Scholar] [CrossRef]
- Refai, A.K.; Cochran, D.L. Harnessing Omics Sciences and Biotechnologies in Understanding Osseointegration—Personalized Dental Implant Therapy. Int. J. Oral Maxillofac. Implant. 2020, 35, e27–e39. [Google Scholar] [CrossRef]
- Tengvall, P.; Skoglund, B.; Askendal, A.; Aspenberg, P. Surface immobilized bisphosphonate improves stainless-steel screw fixation in rats. Biomaterials 2004, 25, 2133–2138. [Google Scholar] [CrossRef]
- Abtahi, J.; Henefalk, G.; Aspenberg, P. Impact of a zoledronate coating on early post-surgical implant stability and marginal bone resorption in the maxilla—A Split-Mouth Randomized Clinical Trial. Clin. Oral Implant. Res. 2019, 30, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Abtahi, J.; Henefalk, G.; Aspenberg, P. Randomised trial of bisphosphonate-coated dental implants: Radiographic follow-up after five years of loading. Int. J. Oral Maxillofac. Surg. 2016, 45, 1564–1569. [Google Scholar] [CrossRef]
- Kim, J.-J.; Lee, J.-H.; Kim, J.C.; Lee, J.-B.; Yeo, I.-S.L. Biological Responses to the Transitional Area of Dental Implants: Material- and Structure-Dependent Responses of Peri-Implant Tissue to Abutments. Materials 2020, 13, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios-Garzón, N.; Velasco-Ortega, E.; López-López, J. Bone Loss in Implants Placed at Subcrestal and Crestal Level: A Systematic Review and Meta-Analysis. Materials 2019, 12, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piattelli, A.; Vrespa, G.; Petrone, G.; Iezzi, G.; Annibali, S.; Scarano, A. Role of the Microgap Between Implant and Abutment: A Retrospective Histologic Evaluation in Monkeys. J. Periodontol. 2003, 74, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Apse, P.; Grybauskas, S.; Puisys, A. The influence of soft tissue thickness on crestal bone changes around implants: A 1-year prospective controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2009, 24, 712–719. [Google Scholar]
- Aslroosta, H.; Akbari, S.; Naddafpour, N.; Adnaninia, S.T.; Khorsand, A.; Esfahani, N.N. Effect of microthread design on the preservation of marginal bone around immediately placed implants: A 5-years prospective cohort study. BMC Oral Health 2021, 21, 541. [Google Scholar] [CrossRef] [PubMed]
- Covani, U.; Chiappe, G.; Bosco, M.; Orlando, B.; Quaranta, A.; Barone, A. A 10-Year Evaluation of Implants Placed in Fresh Extraction Sockets: A Prospective Cohort Study. J. Periodontol. 2012, 83, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Sheikhan, E.; Kadkhodazadeh, M.; Amid, R.; Lafzi, A. Interactive Effects of Five Dental Implant Design Parameters on the Peak Strains at the Interfacial Bone: A Finite Element Study. Int. J. Oral Maxillofac. Implant. 2022, 37, 302–310. [Google Scholar] [CrossRef]
- Bryant, S.R. Oral Implant Outcomes Predicted by Age- and Site-Specific Aspects of Bone Condition. Ph.D. Thesis, University of Toronto, Toronto, ON, Canada, 2001. [Google Scholar]
- Linkevicius, T.; Puisys, A.; Vindasiute, E.; Linkeviciene, L.; Apse, P. Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis. Clin. Oral Implant. Res. 2013, 24, 1179–1184. [Google Scholar] [CrossRef]
- Carcuac, O.; Jansson, L. Peri-implantitis in a specialist clinic of periodontology. Clinical features and risk indicators. Swed. Dent. J. 2010, 34, 53–61. [Google Scholar]
- Roos-Jansåker, A.-M. Long time follow up of implant therapy and treatment of peri-implantitis. Swed. Dent. J. Suppl. 2007, 188, 7–66. [Google Scholar]
- Fransson, C.; Lekholm, U.; Jemt, T.; Berglundh, T. Prevalence of subjects with progressive bone loss at implants. Clin. Oral Implant. Res. 2005, 16, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Gesing, A. The thyroid gland and the process of aging. Thyroid Res. 2015, 8, A8. [Google Scholar] [CrossRef] [Green Version]
- Biondi, B.; Cooper, D.S. The Clinical Significance of Subclinical Thyroid Dysfunction. Endocr. Rev. 2008, 29, 76–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borowska, M.; Bębas, E.; Szarmach, J.; Oczeretko, E. Multifractal characterization of healing process after bone loss. Biomed. Signal Process. Control 2019, 52, 179–186. [Google Scholar] [CrossRef]
- Borowska, M.; Szarmach, J.; Oczeretko, E. Fractal texture analysis of the healing process after bone loss. Comput. Med. Imaging Graph. 2015, 46, 191–196. [Google Scholar] [CrossRef]
- Pociask, E.; Nurzynska, K.; Obuchowicz, R.; Bałon, P.; Uryga, D.; Strzelecki, M.; Izworski, A.; Piórkowski, A. Differential Diagnosis of Cysts and Granulomas Supported by Texture Analysis of Intraoral Radiographs. Sensors 2021, 21, 7481. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
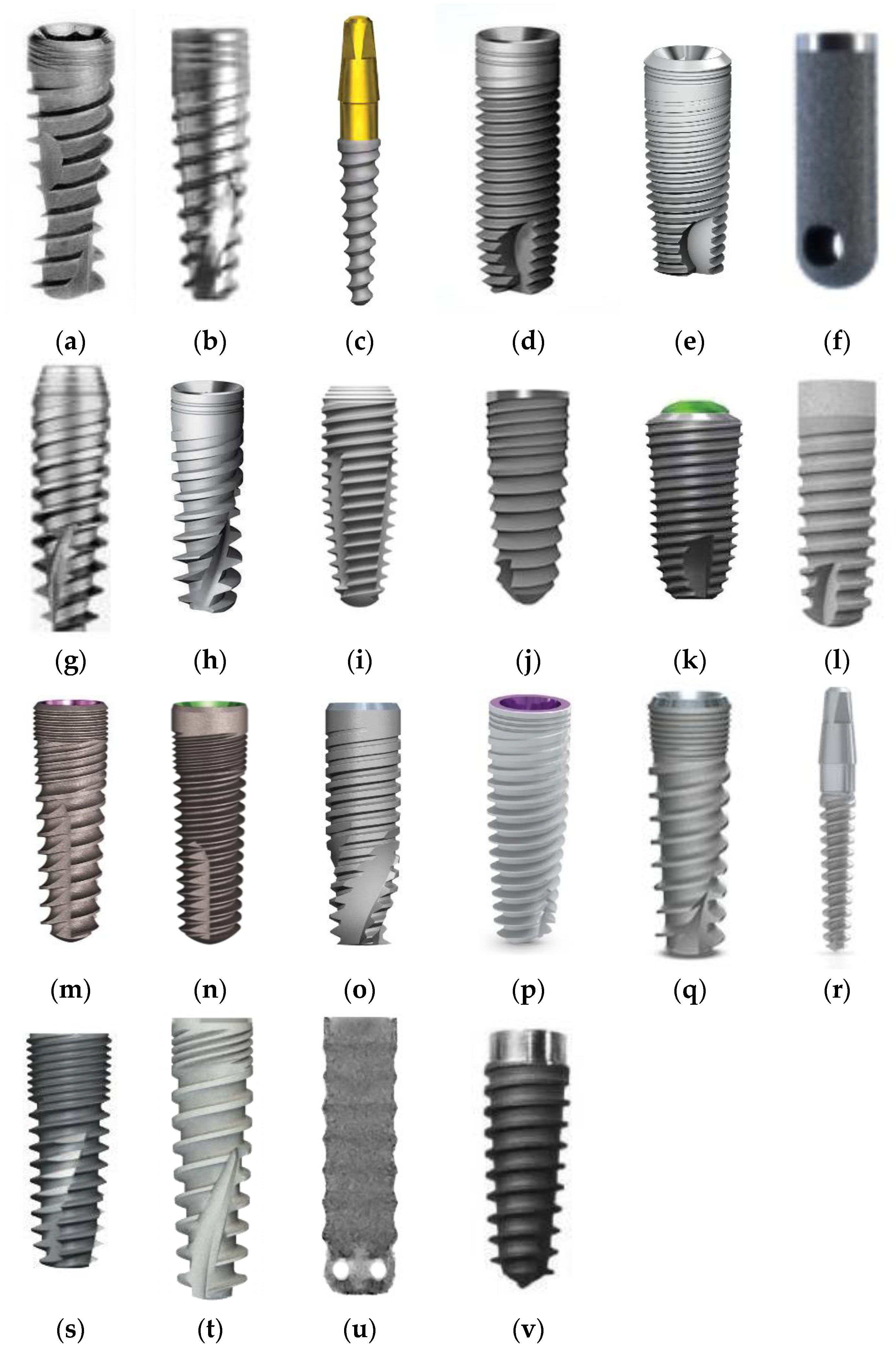
| Manufacturer Implant Type | Titanium Alloy | Level | Connection Type | Connection Shape | Neck Shape | Neck Microthreads | Body Shape | Body Threads | Apex Shape | Apex Hole | Apex Groove |
|---|---|---|---|---|---|---|---|---|---|---|---|
| AB Dental Devices I5 | Grade 5 | Bone Level | Internal | Hexagon | Straight | No | Tapered | Square | Flat | No Hole | Yes |
| ADIN Dental Implants Touareg | Grade 5 | Bone Level | Internal | Hexagon | Straight | Yes | Tapered | Square | Flat | No Hole | Yes |
| Alpha Bio ARRP | Grade 5 | Tissue Level | Custom | One Piece Abutment | Straight | No | Tapered | Reverse Buttress | Cone | No Hole | No |
| Alpha Bio ATI | Grade 5 | Bone Level | Internal | Hexagon | Straight | Yes | Straight | Square | Flat | No Hole | Yes |
| Alpha Bio DFI | Grade 5 | Bone Level | Internal | Hexagon | Straight | Yes | Tapered | Square | Flat | No Hole | Yes |
| Alpha Bio OCI | Grade 5 | Bone Level | Internal | Hexagon | Straight | No | Straight | No Threads | Dome | Round | No |
| Alpha Bio SFB | Grade 5 | Bone Level | Internal | Hexagon | Straight | No | Tapered | V Shaped | Flat | No Hole | Yes |
| Alpha Bio SPI | Grade 5 | Bone Level | Internal | Hexagon | Straight | Yes | Tapered | Square | Flat | No Hole | Yes |
| Argon Medical Prod. K3pro Rapid | Grade 4 | Subcrestal | Internal | Conical | Straight | Yes | Tapered | V Shaped | Dome | No Hole | Yes |
| Bego Semados RI | Grade 4 | Bone Level | Internal | Hexagon | Straight | Yes | Tapered | Reverse Buttress | Cone | No Hole | Yes |
| Dentium Super Line | Grade 5 | Bone Level | Internal | Conical | Straight | No | Tapered | Buttress | Dome | No Hole | Yes |
| Friadent Ankylos C/X | Grade 4 | Subcrestal | Internal | Conical | Straight | No | Tapered | V Shaped | Dome | No Hole | Yes |
| Implant Direct InterActive | Grade 5 | Bone Level | Internal | Conical | Straight | Yes | Tapered | Reverse Buttress | Dome | No Hole | Yes |
| Implant Direct Legacy 3 | Grade 5 | Bone Level | Internal | Hexagon | Straight | Yes | Tapered | Reverse Buttress | Dome | No Hole | Yes |
| MIS BioCom M4 | Grade 5 | Bone Level | Internal | Hexagon | Straight | No | Straight | V Shaped | Flat | No Hole | Yes |
| MIS C1 | Grade 5 | Bone Level | Internal | Conical | Straight | Yes | Tapered | Reverse Buttress | Dome | No Hole | Yes |
| MIS Seven | Grade 5 | Bone Level | Internal | Hexagon | Straight | Yes | Tapered | Reverse Buttress | Dome | No Hole | Yes |
| MIS UNO One Piece | Grade 5 | Tissue Level | Custom | One Piece Abutment | Straight | No | Tapered | Square | Dome | No Hole | Yes |
| Osstem Implant Company GS III | Grade 5 | Bone Level | Internal | Conical | Straight | Yes | Tapered | V Shaped | Dome | No Hole | Yes |
| SGS Dental P7N | Grade 5 | Bone Level | Internal | Hexagon | Straight | Yes | Tapered | V Shaped | Flat | No Hole | Yes |
| TBR Implanté | Grade 5 | Bone Level | Internal | Octagon | Straight | No | Straight | No Threads | Flat | Round | Yes |
| Wolf Dental Conical Screw-Type | Grade 4 | Bone Level | Internal | Hexagon | Straight | No | Tapered | V Shaped | Cone | No Hole | Yes |
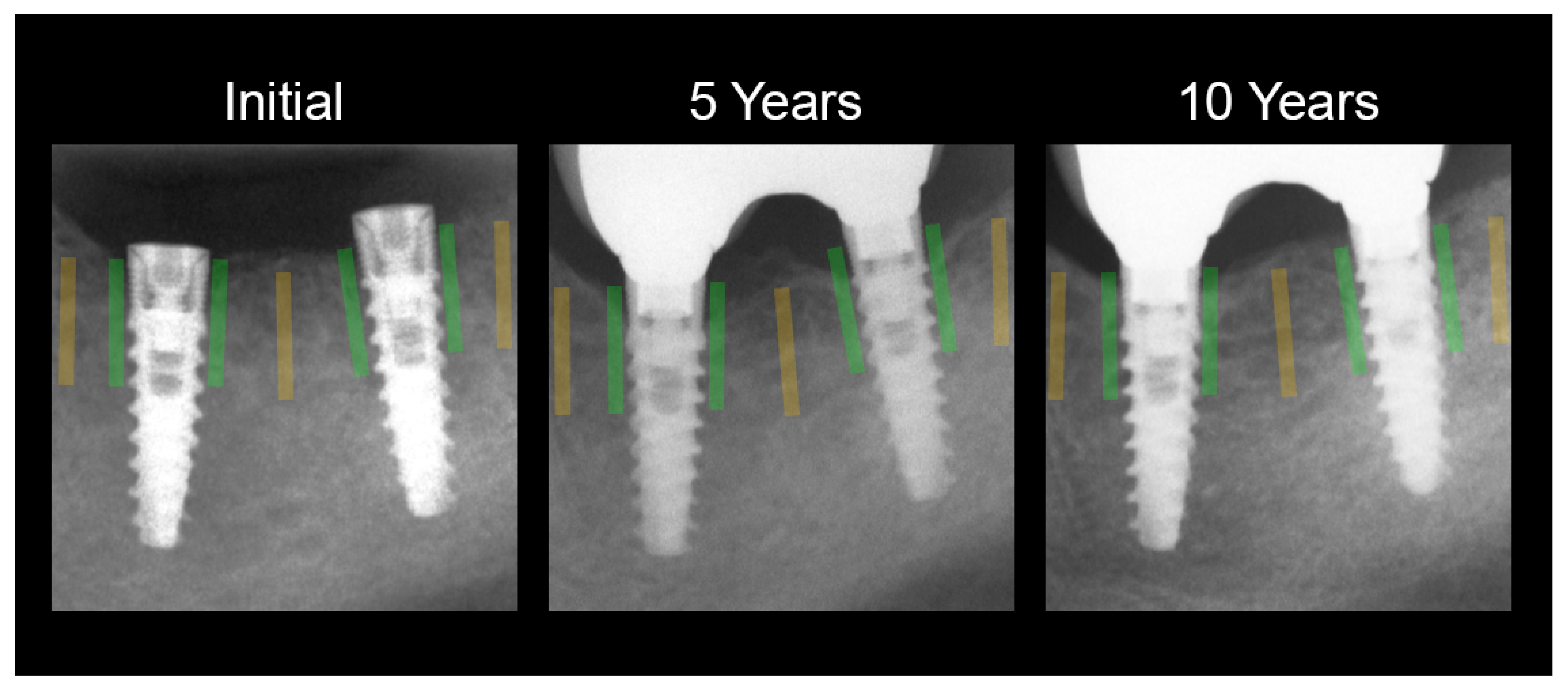
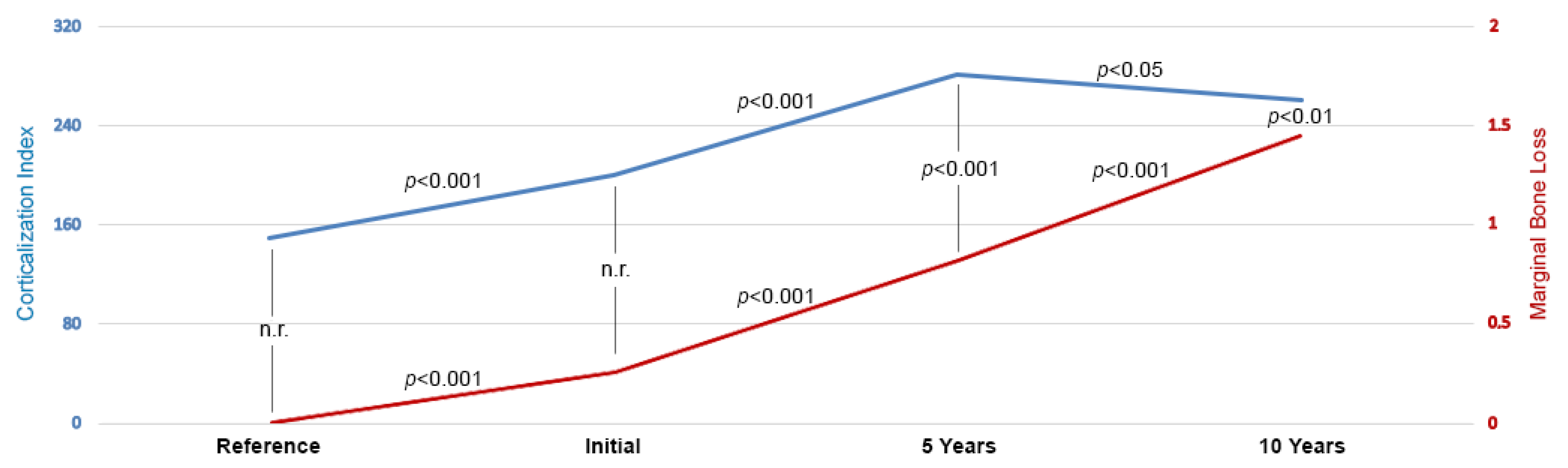
| Region of Interest/Period | Corticalization Index | Marginal Bone Loss [mm] | Simple Regression |
|---|---|---|---|
| Reference Cancellous Bone | 149 ± 178 | 0.00 ± 0.00 | n.a. |
| Initial Peri-Implant Observation | 200 ± 146 | 0.25 ± 0.94 | n.s. |
| 5 Years Peri-Implant Observation | 282 ± 182 | 0.83 ± 1.26 | CC = 0.11; R2 = 1.2%; p < 0.001 |
| 10 Years Peri-Implant Observation | 261 ± 168 | 1.48 ± 2.01 | CC = 0.12; R2 = 1,4%; p < 0.01 |
| Clinical Feature | Option/Value of the Feature | Corticalization Index | ||
|---|---|---|---|---|
| Initial | 5 Years | 10 Years | ||
| Sex | Female | 205 ± 169 | 279 ± 176 | 263 ± 151 |
| Male | 194 ± 114 | 285 ± 190 | 260 ± 190 | |
| Tobacco Smoking | Non-Smoker | 200 ± 152 L | 283 ± 185 | 257 ± 166 L |
| Smoker | 203 ± 91 H | 272 ±155 | 301 ± 184 H | |
| Jaw | Maxilla | 175 ± 108 L | 239 ± 151 L | 223 ± 148 L |
| Mandible | 190 ± 179 H | 336 ± 203 H | 302 ± 179 H | |
| Localization in Dental Arch | Anterior | 166 ± 92 L | 247 ± 163 L | 226 ± 162 L |
| Posterior | 212 ± 174 H | 295 ± 188 H | 273 ± 169 H | |
| Jawbone Status | Augmented | 220 ± 210 | 267 ± 164 | 263 ± 142 |
| Intact | 193 ± 116 | 286 ± 188 | 261 ± 176 | |
| Augmentation Technique | Implant Neck Bone Chips | 236 ± 269 | 292 ± 187 | 271 ± 133 |
| Implant Neck Bone Substitute | 183 ± 107 | 210 ± 138 | 280 ± 211 | |
| Bone Substitute Sinus Lift | 210 ± 143 | 248 ± 138 | 252 ± 135 | |
| Age | 47 ± 13 years | Direct Relation * | Direct Relation * | No Relation |
| Patient Height | 1.70 ± 0.09 m | No Relation | No Relation | Inverse Relation * |
| Patient Weight | 75 ± 19 Kg | No Relation | Inverse Relation * | Inverse Relation * |
| Body Mass Index | 26 ± 4 | No Relation | Inverse Relation * | Inverse Relation * |
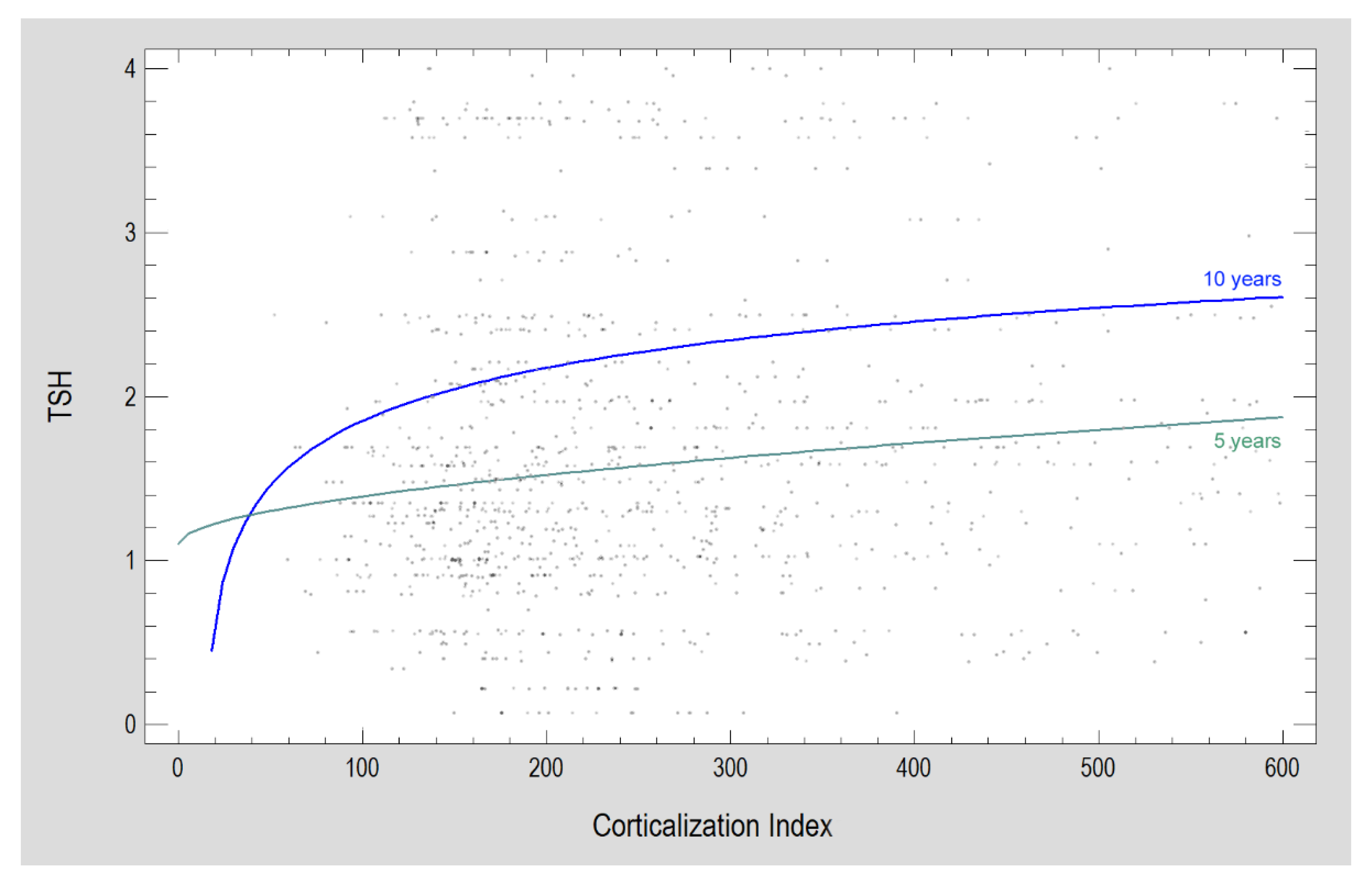
| Serum Thyrotropin | 1.73 ± 1.07 mU/L | Direct Relation * | Direct Relation * | Direct Relation * |
| Total Serum Calcium | 2.39 ± 0.61 mmol/dL | Inverse Relation * | Inverse Relation * | Inverse Relation * |
| Serum Triglycerides | 1.24 ± 0.57 mmol/L | Direct Relation * | No Relation | No Relation |
| Design Parameter | Option | Feature | Initial | 5 Years | 10 Years |
|---|---|---|---|---|---|
| Titanium Alloy n = 2196 | Grade 4 | MBL | 0.00 L | 0.00 L | 0.00 |
| CI | 184 H | 179 L | 189 | ||
| Grade 5 | MBL | 0.00 H | 0.00 H | 0.91 | |
| CI | 163 L | 225 H | 209 | ||
| Immersion Level n = 2196 | Subcrestal | MBL | 0.00 L | 0.00 L | 0.00 L |
| CI | 198 H | 181 | 201 L | ||
| Bone Level | MBL | 0.00 | 0.00 | 0.97 H | |
| CI | 163 L | 224 | 205 L | ||
| Tissue Level | MBL | 0.00 H | 1.24 H | 0.00 | |
| CI | 154 | 222 | 439 H | ||
| Connection Type n = 2196 | Internal | MBL | 0.00 L | 0.00 L | 0.91 |
| CI | 167 | 221 | 205 L | ||
| Custom | MBL | 0.00 H | 1.24 H | 0.00 | |
| CI | 154 | 222 | 439 H | ||
| Connection Shape n = 2196 | Conical | MBL | 0.00 | 0.00 | 0.00 |
| CI | 202 H | 225 | 200 L | ||
| Internal Hexagon | MBL | 0.00 | 0.00 | 0.97 | |
| CI | 151 L | 220 | 205 L | ||
| Internal Octagon | MBL | 0.00 | 0.67 | 2.91 | |
| CI | 205 | 168 | 268 | ||
| One Piece Abutm | MBL | 0.00 | 1.24 | 0.00 | |
| CI | 154 | 222 | 439 H | ||
| Head Microthreads n = 2196 | Yes | MBL | 0.00 | 0.00 L | 0.73 L |
| CI | 170 H | 221 | 201 | ||
| No | MBL | 0.00 | 0.61 H | 1.15 H | |
| CI | 158 L | 222 | 227 | ||
| Body Shape n = 2196 | Tapered | MBL | 0.00 | 0.00 L | 0.85 |
| CI | 167 | 226 H | 206 | ||
| Straight | MBL | 0.00 | 1.33 H | 1.15 | |
| CI | 172 | 147 L | 206 | ||
| Body Threads n = 1760 | Butteress | MBL | 0.00 | 2.15 H | n.a. |
| CI | 190 | 383 H | n.a | ||
| Reverse Butteress | MBL | 0.00 L | 0.00 L | 0.79 L | |
| CI | 171 H | 239 H | 213 | ||
| V Shape | MBL | 0.00 L | 0.00 L | 0.00 L | |
| CI | 174 H | 197 L | 184 | ||
| Square | MBL | 0.00 L | 0.00 L | 0.91 L | |
| CI | 150 L | 201 L | 211 | ||
| No Threads | MBL | 0.30 H | 1.54 H | 2.57 H | |
| CI | 190 | 164 L | 232 | ||
| Apex Shape n = 2196 | Cone | MBL | 0.00 | 0.00 | 0.00 |
| CI | 122 L | 199 | 193 | ||
| Dome | MBL | 0.00 | 0.00 | 0.79 | |
| CI | 174 H | 230 H | 213 | ||
| Flat | MBL | 0.00 | 0.45 H | 1.21 | |
| CI | 148 | 103 L | 201 | ||
| Apex Hole n = 1447 | Round | MBL | 0.00 L | 1.54 H | 2.57 H |
| CI | 190 | 164 L | 232 | ||
| No or other | MBL | 0.30 H | 0.00 L | 0.79 L | |
| CI | 167 | 221 H | 206 | ||
| Apex Groove n = 2196 | Yes | MBL | 0.00 L | 0.00 L | 0.79 L |
| CI | 167 | 220 | 105 | ||
| No | MBL | 0.00 H | 1.66 H | 2.00 H | |
| CI | 154 | 297 | 258 |
| Prosthetic | n | Feature | Initial | 5 Years | 10 Years |
|---|---|---|---|---|---|
| Single Crown | 734 | MBL | 0.00 H | 0.00 | 0.91 |
| CI | 153 L | 196 L | 186 L | ||
| Splinted Crowns | 794 | MBL | 0.00 | 0.00 | 1.20 H |
| CI | 198 | 224 | 227 H | ||
| Bridge | 576 | MBL | 0.00 L | 0.00 L | 0.00 L |
| CI | 172 H | 251 H | 215 | ||
| Overdenture | 160 | MBL | 0.00 | 0.49 H | 0.00 L |
| CI | 185 H | 392 H | 239 H | ||
| Platform Switching | 509 | MBL | 0.00 | 0.00 | 1.06 |
| CI | 155 L | 197 L | 200 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozakiewicz, M.; Wach, T. Exploring the Importance of Corticalization Occurring in Alveolar Bone Surrounding a Dental Implant. J. Clin. Med. 2022, 11, 7189. https://doi.org/10.3390/jcm11237189
Kozakiewicz M, Wach T. Exploring the Importance of Corticalization Occurring in Alveolar Bone Surrounding a Dental Implant. Journal of Clinical Medicine. 2022; 11(23):7189. https://doi.org/10.3390/jcm11237189
Chicago/Turabian StyleKozakiewicz, Marcin, and Tomasz Wach. 2022. "Exploring the Importance of Corticalization Occurring in Alveolar Bone Surrounding a Dental Implant" Journal of Clinical Medicine 11, no. 23: 7189. https://doi.org/10.3390/jcm11237189