
Learning Curves in Pediatric Robot-Assisted Pyeloplasty: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
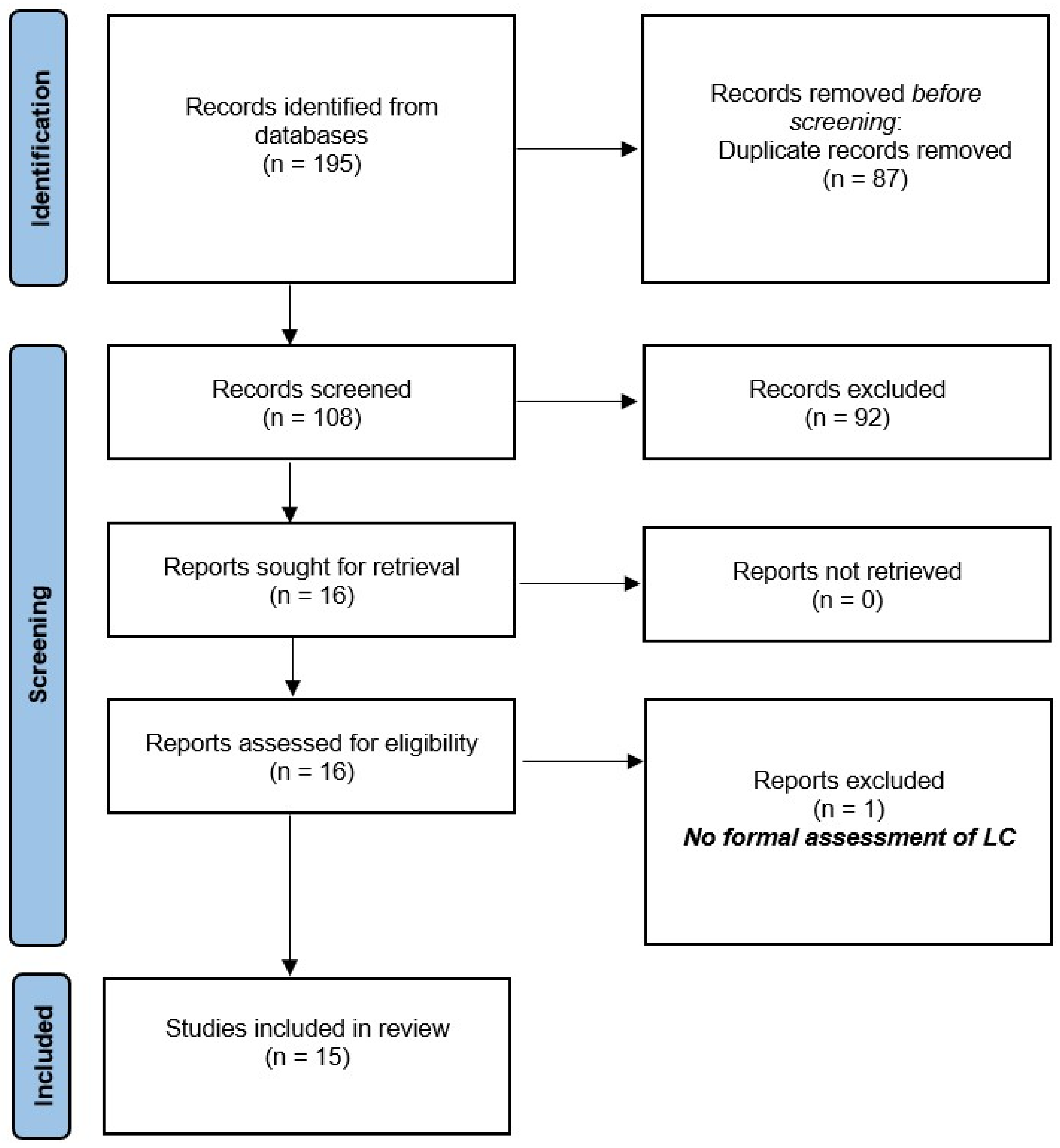
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Summary of Included Studies
3.2. Outcomes
3.2.1. Primary Outcomes
3.2.2. Secondary Outcomes
3.3. Methodological Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Database | Studies |
| PubMed | 54 |
| Embase | 6 |
| Scopus | 68 |
| Web of Science | 67 |
| Total | 195 |
| Duplications | 87 |
| After duplications removal | 108 |
References
- Varda, B.K.; Wang, Y.; Chung, B.I.; Lee, R.S.; Kurtz, M.P.; Nelson, C.P.; Chang, S.L. Has the robot caught up? National trends in utilization, perioperative outcomes, and cost for open, laparoscopic, and robotic pediatric pyeloplasty in the United States from 2003 to 2015. J. Pediatr. Urol. 2018, 14, 336.e1–336.e8. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, M.E.; DaJusta, D.G. Robotics in Pediatric Urology. Int. Braz J. Urol. 2020, 46, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Pakkasjärvi, N.; Taskinen, S. Introduction of Pediatric Robot-Assisted Pyeloplasty in A Low-Volume Center. Clin. Pract. 2021, 11, 143–150. [Google Scholar] [CrossRef]
- Salö, M.; Sjöberg Altemani, S.; Anderberg, M. Pyeloplasty in children: Perioperative results and long-term outcomes of robotic-assisted laparoscopic surgery compared to open surgery. Pediatr. Surg. Int. 2016, 32, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Kassite, I.; Braik, K.; Villemagne, T.; Lardy, H.; Binet, A. The learning curve of robot-assisted laparoscopic pyeloplasty in children: A multi-outcome approach. J. Pediatr. Urol. 2018, 14, 570.e1–570.e10. [Google Scholar] [CrossRef]
- Wong, Y.S.; Pang, K.K.Y.; Tam, Y.H. Comparing Robot-Assisted Laparoscopic Pyeloplasty vs. Laparoscopic Pyeloplasty in Infants Aged 12 Months or Less. Front. Pediatr. 2021, 9, 647139. [Google Scholar] [CrossRef]
- Maizlin, I.I.; Shroyer, M.C.; Yu, D.C.; Martin, C.A.; Chen, M.K.; Russell, R.T. Survey on Robot-Assisted Surgical Techniques Utilization in US Pediatric Surgery Fellowships. J. Laparoendosc. Adv. Surg. Tech. A 2017, 27, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Aldousari, S.A.; Buabbas, A.J.; Yaiesh, S.M.; Alyousef, R.J.; Alenezi, A.N. Multiple perceptions of robotic-assisted surgery among surgeons and patients: A cross-sectional study. J. Robot. Surg. 2021, 15, 529–538. [Google Scholar] [CrossRef]
- Andolfi, C.; Kumar, R.; Boysen, W.R.; Gundeti, M.S. Current Status of Robotic Surgery in Pediatric Urology. J. Laparoendosc. Adv. Surg. Tech. A 2019, 29, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, K.; Kojima, Y.; Nishio, H.; Hoshi, S.; Sato, Y.; Hayashi, Y. Robotic surgery in pediatric urology: Current status. Asian J. Endosc. Surg. 2018, 11, 308–317. [Google Scholar] [CrossRef]
- Esposito, C.; Autorino, G.; Castagnetti, M.; Cerulo, M.; Coppola, V.; Cardone, R.; Esposito, G.; Borgogni, R.; Escolino, M. Robotics and future technical developments in pediatric urology. Semin. Pediatr. Surg. 2021, 30, 151082. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Abboudi, H.; Khan, M.S.; Dasgupta, P.; Ahmed, K. Measuring the surgical ‘learning curve’: Methods, variables and competency. BJU Int. 2014, 113, 504–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality If Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 12 September 2022).
- Kang, S.K.; Jang, W.S.; Kim, S.H.; Kim, S.W.; Han, S.W.; Lee, Y.S. Comparison of intraoperative and short-term postoperative outcomes between robot-assisted laparoscopic multi-port pyeloplasty using the da Vinci Si system and single-port pyeloplasty using the da Vinci SP system in children. Investig. Clin. Urol. 2021, 62, 592–599. [Google Scholar] [CrossRef]
- Sorensen, M.D.; Delostrinos, C.; Johnson, M.H.; Grady, R.W.; Lendvay, T.S. Comparison of the learning curve and outcomes of robotic assisted pediatric pyeloplasty. J. Urol. 2011, 185, 2517–2522. [Google Scholar] [CrossRef]
- Stern, N.; Li, Y.; Wang, P.Z.; Dave, S. A cumulative sum (CUSUM) analysis studying operative times and complications for a surgeon transitioning from laparoscopic to robot-assisted pediatric pyeloplasty: Defining proficiency and competency. J. Pediatr. Urol. 2022. [Google Scholar] [CrossRef]
- Reinhardt, S.; Ifaoui, I.B.; Thorup, J. Robotic surgery start-up with a fellow as the console surgeon. Scand. J. Urol. 2017, 51, 335–338. [Google Scholar] [CrossRef]
- Cundy, T.P.; Gattas, N.E.; White, A.D.; Najmaldin, A.S. Learning curve evaluation using cumulative summation analysis—A clinical example of pediatric robot-assisted laparoscopic pyeloplasty. J. Pediatr. Surg. 2015, 50, 1368–1373. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.T.; Shukla, A.R. Transition from open to robotic-assisted pediatric pyeloplasty: A feasibility and outcome study. J. Pediatr. Urol. 2012, 8, 276–281. [Google Scholar] [CrossRef]
- Espositio, C.; Masieri, L.; Castagnetti, M.; Sforza, S.; Farina, A.; Cerulo, M.; Cini, C.; Del Conte, F.; Escolinio, M. Robot-assisted vs laparoscopic pyeloplasty in children with uretero-pelvic junction obstruction (UPJO): Technical considerations and results. J. Pediatr. Urol. 2019, 15, 667.e1–667.e8. [Google Scholar] [CrossRef]
- Radford, A.; Turner, A.; Ashraf, J.; Subramaniam, R. Robotic Pyeloplasty in Children: A “Barbed” Shortcut. J. Laparoendosc. Adv. Surg. Tech. A 2018, 28, 486–489. [Google Scholar] [CrossRef] [PubMed]
- Tasian, G.E.; Wiebe, D.J.; Casale, P. Learning curve of robotic assisted pyeloplasty for pediatric urology fellows. J. Urol. 2013, 190, 1622–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, M.D.; Herndon, C.D.A.; Herbst, K.W.; Poston, T.L.; Brandt, E.J.; Peters, C.A.; Corbett, S.T. Proctor environment facilitates faculty training in pediatric robotic-assisted laparoscopic pyeloplasty. J. Robot. Surg. 2014, 8, 365–369. [Google Scholar] [CrossRef]
- Murthy, P.; Cohn, J.A.; Gundeti, M.S. Evaluation of robotic-assisted laparoscopic and open pyeloplasty in children: Single-surgeon experience. Ann. R. Coll. Surg. Engl. 2015, 97, 109–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andolfi, C.; Lombardo, A.M.; Aizen, J.; Recabal, X.; Walker, J.P.; Barashi, N.S.; Reed, F.; Lopez, P.J.; Wilcox, D.T.; Gundeti, M.S. Laparoscopic and robotic pyeloplasty as minimally invasive alternatives to the open approach for the treatment of uretero-pelvic junction obstruction in infants: A multi-institutional comparison of outcomes and learning curves. World J. Urol. 2022, 40, 1049–1056. [Google Scholar] [CrossRef]
- Bowen, D.K.; Lindgren, B.W.; Cheng, E.Y.; Gong, E.M. Can proctoring affect the learning curve of robotic-assisted laparoscopic pyeloplasty? Experience at a high-volume pediatric robotic surgery center. J. Robot. Surg. 2017, 11, 63–67. [Google Scholar] [CrossRef]
- Dothan, D.; Raisin, G.; Jaber, J.; Kocherov, S.; Chertin, B. Learning curve of robotic-assisted laparoscopic pyeloplasty (RALP) in children: How to reach a level of excellence? J. Robot. Surg. 2021, 15, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Junejo, N.N.; Alotaibi, A.; Alshahrani, S.M.; Alshammari, A.; Peters, C.A.; Alhazmi, H.; Vallasciani, S.A. The learning curve for robotic-assisted pyeloplasty in children: Our initial experience from a single center. Urol. Ann. 2020, 12, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Baartman, L.K.; Bastiaens, T.J.; Kirschner, P.A.; Van der Vleuten, C.P. Evaluating assessment quality in competence-based education: A qualitative comparison of two frameworks. Educ. Res. Rev. 2007, 2, 114–129. [Google Scholar] [CrossRef]
- Pusic, M.V.; Kessler, D.; Szyld, D.; Kalet, A.; Pecaric, M.; Boutis, K. Experience curves as an organizing framework for deliberate practice in emergency medical learning. Acad. Emerg. Med. 2012, 19, 1476–1480. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, C.R.; Grant, A.M.; Wallace, S.A.; Garthwaite, P.H.; Monk, A.F.; Russell, I.T. Assessment of the learning curve in health technologies. A systematic review. Int. J. Technol. Assess. Health Care 2000, 16, 1095–1108. [Google Scholar] [CrossRef] [PubMed]
- Darzi, A.; Smith, S.; Taffinder, N. Assessing operative skill. BMJ 1999, 318, 887–888. [Google Scholar] [CrossRef] [PubMed]
- Valsamis, E.M.; Chouari, T.; O’Dowd-Booth, C.; Rogers, B.; Ricketts, D. Learning curves in surgery: Variables, analysis, and applications. Postgrad. Med. J. 2018, 94, 525–530. [Google Scholar] [CrossRef]
- Kassite, I.; Bejan-Angoulvant, T.; Lardy, H.; Binet, A. A systematic review of the learning curve in robotic surgery: Range and heterogeneity. Surg. Endosc. 2019, 33, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Hopper, A.N.; Jamison, M.H.; Lewis, W.G. Learning curves in surgical practice. Postgrad. Med. J. 2007, 83, 777–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, J.A.; Ramsay, C.R.; Fayers, P. Statistical evaluation of learning curve effects in surgical trials. Clin. Trials 2004, 1, 421–427. [Google Scholar] [CrossRef]
- Cook, J.A.; Ramsay, C.R.; Fayers, P. Using the literature to quantify the learning curve: A case study. Int. J. Technol. Assess. Health Care 2007, 23, 255–260. [Google Scholar] [CrossRef] [Green Version]
- Sudan, R.; Bennett, K.M.; Jacobs, D.O.; Sudan, D.L. Multifactorial analysis of the learning curve for robot-assisted laparoscopic biliopancreatic diversion with duodenal switch. Ann. Surg. 2012, 255, 940–955. [Google Scholar] [CrossRef]
- Spampinato, G.; Binet, A.; Fourcade, L.; Sagaon Mendoza, M.; Villemagne, T.; Braik, K.; Grosos, C.; Lardy, H.; Ballouhey, Q. Comparison of the Learning Curve for Robot-Assisted Laparoscopic Pyeloplasty Between Senior and Junior Surgeons. J. Laparoendosc. Adv. Surg. Tech. A 2021, 31, 478–483. [Google Scholar] [CrossRef]


{kind=link}
| Year of Publication | Author | Journal | Country | Sample Size | No. of Surgeons | Study Design |
|---|---|---|---|---|---|---|
| 2011 | Sorensen et al. [16] | J Urol | USA | 33 | 2 | Retro |
| 2012 | O’Brien et al. [20] | J Pediatr Urol | USA | 20 | 1 | Retro |
| 2013 | Tasian at al. [23] | J Urol | USA | 100 | 5 | Pro |
| 2014 | Mason et al. [24] | J Robotic Surg | USA | 134 | 3 | Retro |
| 2015 | Cundy et al. [19] | J Pediatr Surg | UK | 90 | 1 | Pro |
| 2015 | Murthy et al. [25] | Ann R Coll Surg Engl | USA | 52 | 1 | Retro |
| 2016 | Bowen et al. [27] | J Robot Surg | USA | 28 | 3 | Retro |
| 2017 | Reinhardt et al. [18] | Scandinavian J Urol | Denmark | 25 | 1 | Pro |
| 2017 | Radford et al. [22] | J Laparoendosc Adv Surg Tech A | UK | 25 | NA | Retro |
| 2018 | Kassite et al. [5] | J Pediatr Urol | France | 42 | 2 | Pro |
| 2019 | Esposito et al. [21] | J Pediatr Urol | Italy | 37 | 3 | Retro |
| 2019 | Junejo et al. [29] | Urol Ann | Saudi Arabia | 15 | NA | Retro |
| 2020 | Dothan et al. [28] | J Robot Surg | Israel | 33 | 1 | Retro |
| 2022 | Stern et al. [17] | J Pediatr Urol | Canada | 50 | 1 | Pro |
| 2022 | Andolfi et al. [26] | World J Urol | USA | 39 | 1 | Retro |
| Year of Publication | Author | LC Presentation | LC Outcomes | LC Comparison with Open/Laparoscopy | LC Case Number |
|---|---|---|---|---|---|
| 2011 | Sorensen et al. [16] | Narrative, line graph | Total operative time; postoperative complications | Open | 15 to 20 |
| 2012 | O’Brien et al. [20] | Narrative, line graph | Total operative time | Laparoscopy, Open | NA |
| 2013 | Tasian at al. [23] | Narrative, plot graph | Console time, intraoperative complications, resolution | No | 37 |
| 2014 | Mason et al. [24] | Narrative, line graph | Total operative time, intraoperative complications, postoperative complications, length of hospital stay | No | 3 |
| 2015 | Cundy et al. [19] | CUSUM chart, narrative, line graph, plot graph | Set up time, docking time, console time, operating time, total operating room time, postoperative complications | No | LC transitioned beyond the learning phase at cases 10, 15, 42, 57, and 58 for set-up time, docking time, console time, operating time, and total operating room time, respectively |
| 2015 | Murthy et al. [25] | Narrative, plot graph | Total operative time, intraoperative complications | Open | 42 |
| 2017 | Bowen et al. [27] | Narrative, line graph | Total operative time, intraoperative complications, postoperative complications, length of hospital stay, resolution | No | |
| 2017 | Reinhardt et al. [18] | Narrative, line graph | Total operative time, length of hospital stay, complications | Laparoscopy, Open | NA |
| 2017 | Radford et al. [22] | Narrative, plot graph | Operative time | No | NA |
| 2018 | Kassite et al. [5] | CUSUM chart | Operative time, adjusted operative time, composite parameter (operative time adjusted for patient complexity factors, complications factor and success factor) | No | 41 |
| 2019 | Esposito et al. [21] | Narrative, line graph | Time for docking and anastomosis duration | Laparoscopy | 23 |
| 2019 | Junejo et al. [29] | Narrative, line graph, table | Total operation duration, length of stay, complications, resolution | No | 15 |
| 2021 | Dothan et al. [28] | Narrative | Total operation duration, length of stay, complications, resolution | Laparoscopy, Open | NA |
| 2022 | Stern et al. [17] | Narrative, CUSUM chart | Total operative time, step-specific operative times for port placement, dissection, and hitch stitch placement, pelvis dismemberment, and spatulation, suturing and port removal | No | Learning—initial 13 cases, proficiency—middle 16 cases, competency—last 21 cases |
| 2022 | Andolfi et al. [26] | r-to-z transformation, CUSUM | Total operation duration, complications, resolution | Laparoscopy, Open | LC showed plateau in OT after 13 cases and a second phase of further improvements after 37 cases |
| Author, Year | Selection | Comparability | Outcome | Total Score | Quality | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | |||
| Sorensen et al., 2011 [16] | * | * | * | * | * | * | * | * | 8 | Good |
| O’Brien et al., 2012 [20] | * | * | * | * | - | * | * | * | 7 | Poor |
| Tasian at al., 2013 [23] | * | - | * | * | - | * | * | * | 6 | Poor |
| Mason et al., 2014 [24] | * | - | * | * | - | * | - | * | 5 | Poor |
| Cundy et al., 2015 [19] | * | - | * | * | - | * | * | * | 6 | Poor |
| Murthy et al., 2015 [25] | * | * | * | * | - | * | * | * | 7 | Poor |
| Bowen et al., 2017 [27] | * | - | * | * | - | * | * | * | 6 | Poor |
| Reinhardt et al., 2017 [18] | * | * | * | * | * | * | * | * | 8 | Good |
| Radford et al., 2017 [22] | * | - | * | * | - | * | * | * | 6 | Poor |
| Kassite et al., 2018 [5] | * | - | * | * | - | * | * | * | 6 | Poor |
| Esposito et al., 2019 [21] | * | * | * | * | - | * | * | * | 7 | Poor |
| Junejo et al., 2019 [29] | * | - | * | * | - | * | * | * | 6 | Poor |
| Dothan et al., 2021 [28] | * | * | * | * | - | * | - | * | 6 | Poor |
| Stern et al., 2022 [17] | * | - | * | * | - | * | * | * | 6 | Poor |
| Andolfi et al., 2022 [26] | * | * | * | * | - | * | * | * | 7 | Poor |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pakkasjärvi, N.; Krishnan, N.; Ripatti, L.; Anand, S. Learning Curves in Pediatric Robot-Assisted Pyeloplasty: A Systematic Review. J. Clin. Med. 2022, 11, 6935. https://doi.org/10.3390/jcm11236935
Pakkasjärvi N, Krishnan N, Ripatti L, Anand S. Learning Curves in Pediatric Robot-Assisted Pyeloplasty: A Systematic Review. Journal of Clinical Medicine. 2022; 11(23):6935. https://doi.org/10.3390/jcm11236935
Chicago/Turabian StylePakkasjärvi, Niklas, Nellai Krishnan, Liisi Ripatti, and Sachit Anand. 2022. "Learning Curves in Pediatric Robot-Assisted Pyeloplasty: A Systematic Review" Journal of Clinical Medicine 11, no. 23: 6935. https://doi.org/10.3390/jcm11236935