

Bladder Management Strategies for Urological Complications in Patients with Chronic Spinal Cord Injury
 , ,
, ,  , , , and
on behalf of the Taiwan Continence Society Spinal Cord Injury Study Group
, , , and
on behalf of the Taiwan Continence Society Spinal Cord Injury Study Group
Abstract
:1. Introduction
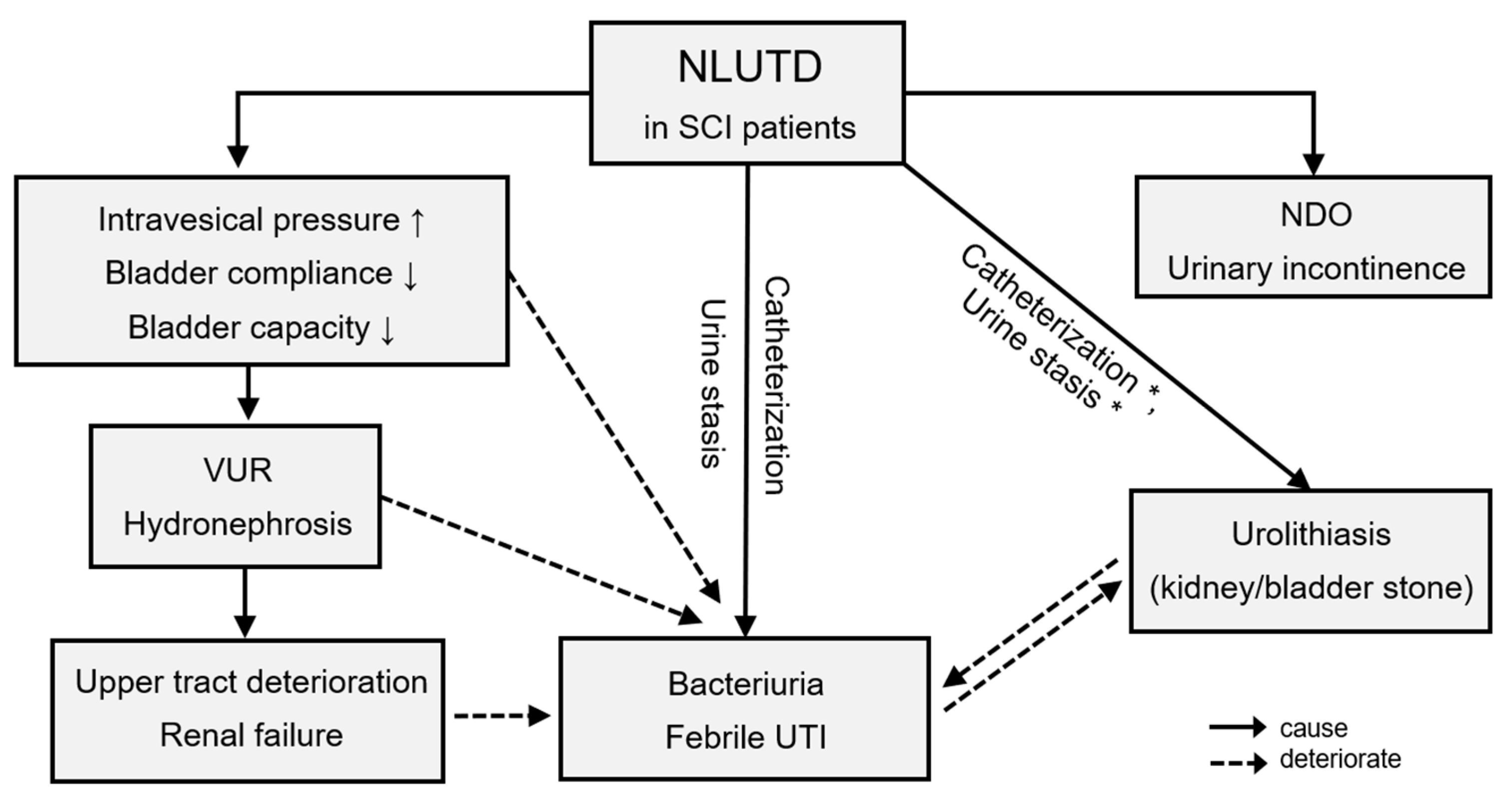
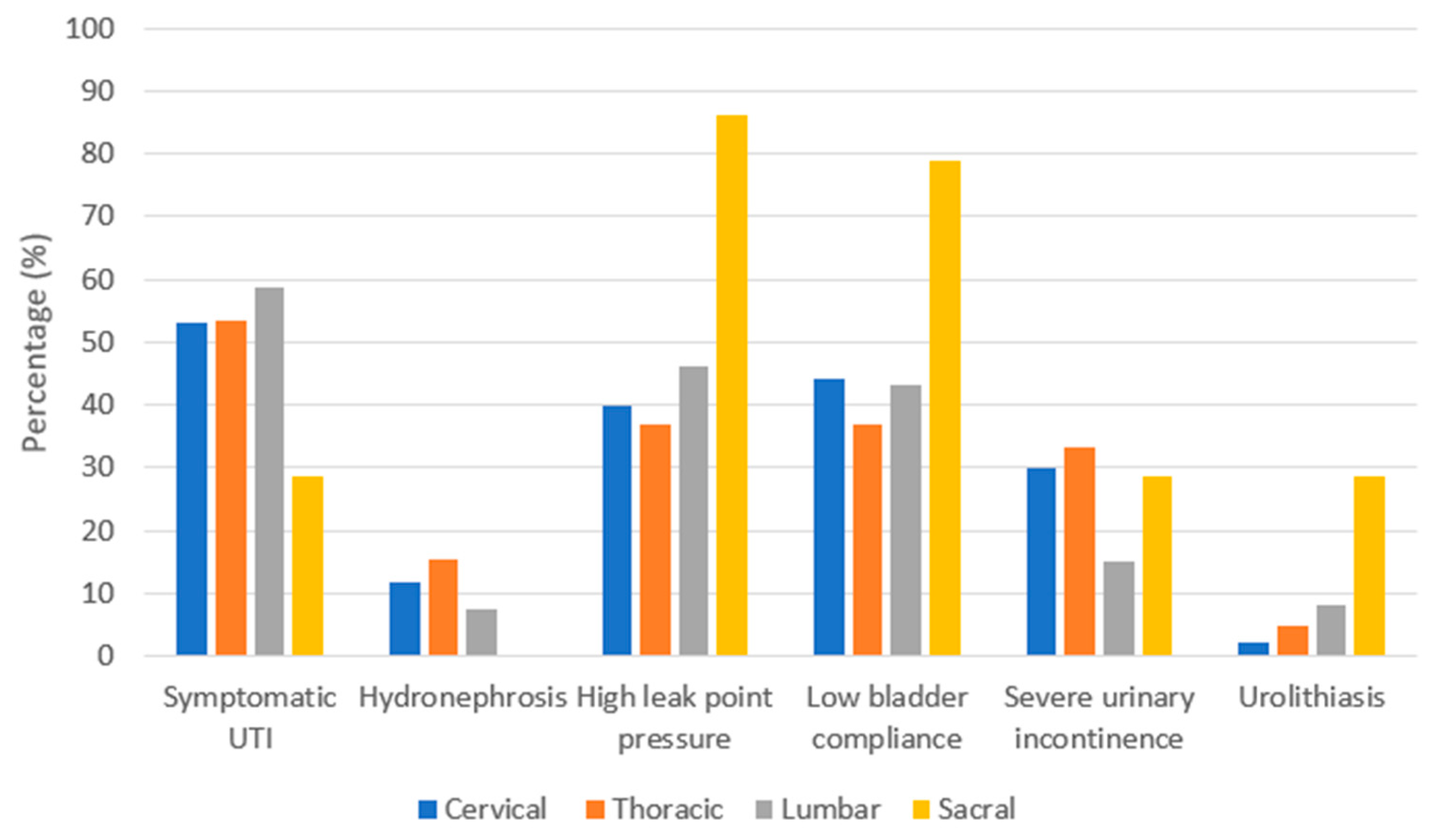
2. Urological Complications in Chronic SCI Patients
3. The Effects of Different Types of Bladder Management on UTI Post-SCI
4. Bladder Management of Urge Urinary Incontinence (UUI) in Chronic SCI Patients
5. Different Types of Bladder Management of Poor Bladder Compliance
6. Renal Function Preservation in Chronic SCI Patients
7. The Risk of Urolithiasis in the Different Types of Bladder Management
8. Long-Term Complications and Satisfaction of Augmentation Enterocystoplasty (AE) in Chronic SCI Patients
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Spinal Cord Injury Statistical Center. Spinal Cord Injury (SCI) Facts and Figures at a Glance. 2016 Data Sheet. Available online: www.nscisc.uab.edu/Public/Facts%202016.pdf (accessed on 1 July 2022).
- Ku, J.H. The management of neurogenic bladder and quality of life in spinal cord injury. BJU Int. 2006, 98, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Wada, N.; Karnup, S.; Kadekawa, K.; Shimizu, N.; Kwon, J.; Shimizu, T.; Gotoh, D.; Kakizaki, H.; de Groat, W.C.; Yoshimura, N. Current Knowledge and Novel Frontiers in Lower Urinary Tract Dysfunction after Spinal Cord Injury: Basic Research Perspectives. Urol. Sci. 2022, 33, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Linsenmeyer, T.A.; Bodner, D.R.; Creasey, G.H.; Green, B.G.; Groah, S.L.; Joseph, A. Bladder management for adults with spinal cord injury: A clinical practice guideline for health-care providers. J. Spinal Cord Med. 2006, 29, 527–573. [Google Scholar]
- Esclarin De Ruz, A.; Garcia Leoni, E.; Herruzo Cabrera, R. Epidemiology and risk factors for urinary tract infection in patients with spinal cord injury. J. Urol. 2000, 164, 1285–1289. [Google Scholar] [CrossRef]
- Adriaansen, J.J.; van Asbeck, F.W.; Tepper, M.; Faber, W.X.; Visser-Meily, J.M.; de Kort, L.M.; Post, M.W. Bladder-emptying methods, neurogenic lower urinary tract dysfunction and impact on quality of life in people with long-term spinal cord injury. J. Spinal Cord Med. 2017, 40, 43–53. [Google Scholar] [CrossRef]
- Apostolidis, A.; Drake, M.J.; Emmanuel, A.; Gajewski, J.; Hamid, R.; Heesakkers, J.; Kessler, T.; Madersbacher, H.; Mangera, A.; Panicker, J.; et al. Neurologic Urinary and Faecal Incontinence. In Incontinence, 6th ed.; Abrams, P., Cardozo, L., Khoury, S., Wein, A., Eds.; Wiley Online Library: Hoboken, NJ, USA, 2017. [Google Scholar]
- Bloemen-Vrencken, J.H.; Post, M.W.; Hendriks, J.M.; De Reus, E.C.; De Witte, L.P. Health problems of persons with spinal cord injury living in the Netherlands. Disabil. Rehabil. 2005, 27, 1381–1389. [Google Scholar] [CrossRef]
- Frankel, H.L.; Coll, J.R.; Charlifue, S.W.; Whiteneck, G.G.; Gardner, B.P.; A Jamous, M.; Krishnan, K.R.; Nuseibeh, I.; Savic, G.; Sett, P. Long-term survival in spinal cord injury: A fifty year investigation. Spinal Cord 1998, 36, 266–274. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.; Rohilla, R.K.; Sangwan, K.; Siwach, R.; Magu, N.K.; Sangwan, S.S. Bladder management methods and urological complications in spinal cord injury patients. Indian J. Orthop. 2011, 45, 141–147. [Google Scholar] [CrossRef]
- Soden, R.; Walsh, J.; Middleton, J.; Craven, M.; Rutkowski, S.; Yeo, J. Causes of death after spinal cord injury. Spinal Cord 2000, 38, 604–610. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Jiang, Y.; Jhang, J.; Lee, C.; Kuo, H. Bladder management and urological complications in patients with chronic spinal cord injuries in Taiwan. Tzu Chi Med. J. 2014, 26, 25–28. [Google Scholar] [CrossRef] [Green Version]
- Kinnear, N.; Barnett, D.; O’Callaghan, M.; Horsell, K.; Gani, J.; Hennessey, D. The impact of catheter-based bladder drainage method on urinary tract infection risk in spinal cord injury and neurogenic bladder: A systematic review. Neurourol. Urodyn. 2020, 39, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Weld, K.J.; Dmochowski, R.R. Effect of bladder management on urological complications in spinal cord injured patients. J. Urol. 2000, 163, 768–772. [Google Scholar] [CrossRef]
- Weld, K.J.; Graney, M.J.; Dmochowski, R.R. Differences in bladder compliance with time and associations of bladder management with compliance in spinal cord injured patients. J. Urol. 2000, 163, 1228–1233. [Google Scholar] [CrossRef]
- Lai, E.C.; Kao Yang, Y.H.; Kuo, H.C. Complication rate of neurogenic lower urinary tract dysfunction after spinal cord injury in Taiwan. Int. Urol. Nephrol. 2014, 46, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.B.; A Cripps, R.; Fitzharris, M.; Wing, P.C. The global map for traumatic spinal cord injury epidemiology: Update 2011, global incidence rate. Spinal Cord 2014, 52, 110–116. [Google Scholar] [CrossRef] [Green Version]
- Simpson, L.A.; Eng, J.J.; Hsieh, J.T.; Dalton, L. The health and life priorities of individuals with spinal cord injury: A systematic review. J. Neurotrauma 2012, 29, 1548–1555. [Google Scholar] [CrossRef] [Green Version]
- Stillman, M.D.; Barber, J.; Burns, S.; Williams, S.; Hoffman, J.M. Complications of Spinal Cord Injury Over the First Year After Discharge From Inpatient Rehabilitation. Arch. Phys. Med. Rehabil. 2017, 98, 1800–1805. [Google Scholar] [CrossRef]
- Jeong, S.J.; Cho, S.Y.; Oh, S.J. Spinal cord/brain injury and the neurogenic bladder. Urol. Clin. N. Am. 2010, 37, 537–546. [Google Scholar] [CrossRef]
- Weld, K.J.; Graney, M.J.; Dmochowski, R.R. Clinical significance of detrusor sphincter dyssynergia type in patients with post-traumatic spinal cord injury. Urology 2000, 56, 565–568. [Google Scholar] [CrossRef]
- Weld, K.J.; Dmochowski, R.R. Association of level of injury and bladder behavior in patients with post-traumatic spinal cord injury. Urology 2000, 55, 490–494. [Google Scholar] [CrossRef]
- McGuire, E.J.; Cespedes, R.D.; O’Connell, H.E. Leak-point pressures. Urol. Clin. N. Am. 1996, 23, 253–262. [Google Scholar] [CrossRef]
- Stöhrer, M.; Goepel, M.; Kondo, A.; Kramer, G.; Madersbacher, H.; Millard, R.; Rossier, R.; Wyndaele, J.-J. The standardization of terminology in neurogenic lower urinary tract dysfunction with suggestions for diagnostic procedures. Neurourol. Urodyn. 1999, 18, 139–158. [Google Scholar] [CrossRef]
- Cardenas, D.D.; Hoffman, J.M.; Kirshblum, S.; McKinley, W. Etiology and incidence of rehospitalization after traumatic spinal cord injury: A multicenter analysis. Arch. Phys. Med. Rehabil. 2004, 85, 1757–1763. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Danforth, T.; Ginsberg, D.A. Urologic Management and Complications in Spinal Cord Injury Patients: A 40- to 50-year Follow-up Study. Urology 2017, 104, 52–58. [Google Scholar] [CrossRef]
- Pickelsimer, E.; Shiroma, E.J.; Wilson, D.A. Statewide investigation of medically attended adverse health conditions of persons with spinal cord injury. J. Spinal Cord Med. 2010, 33, 221–231. [Google Scholar] [CrossRef]
- Morton, S.C.; Shekelle, P.G.; Adams, J.L.; Bennett, C.; Dobkin, B.H.; Montgomerie, J.; Vickrey, B.G. Antimicrobial prophylaxis for urinary tract infection in persons with spinal cord dysfunction. Arch. Phys. Med. Rehabil. 2002, 83, 129–138. [Google Scholar] [CrossRef]
- Kriz, J.; Sediva, K.; Maly, M. Causes of death after spinal cord injury in the Czech Republic. Spinal Cord 2021, 59, 814–820. [Google Scholar] [CrossRef]
- Hooton, T.M.; Bradley, S.F.; Cardenas, D.D.; Colgan, R.; Geerlings, S.E.; Rice, J.C.; Saint, S.; Schaeffer, A.J.; Tambayh, P.A.; Tenke, P.; et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 625–663. [Google Scholar] [CrossRef] [Green Version]
- Cameron, A.P.; Wallner, L.P.; Tate, D.G.; Sarma, A.V.; Rodriguez, G.M.; Clemens, J.Q. Bladder management after spinal cord injury in the United States 1972 to 2005. J. Urol. 2010, 184, 213–217. [Google Scholar] [CrossRef]
- Blok, B.F.; Castro-Diaz, D.; Del Popolo, G.; Groen, J.; Hamid, R.; Karsenty, G.; Kessler, T.M.; Pannek, J. EAU Guidelines on Neuro-Urology; European Association of Urology: Arnhem, The Netherlands, 2022. [Google Scholar]
- Averch, T.D.; Stoffel, J.; Goldman, H.B. Cather-Associated Urinary Tract Infections: Definitions and Significance in the Urologic Patient; American Urological Association: Arnhem, The Netherlands, 2014. [Google Scholar]
- Penders, J.; Huylenbroeck, A.A.; Everaert, K.; Van Laere, M.; Verschraegen, G.L. Urinary infections in patients with spinal cord injury. Spinal Cord 2003, 41, 549–552. [Google Scholar] [CrossRef]
- Jia, C.; Liao, L.M.; Chen, G.; Sui, Y. Detrusor botulinum toxin A injection significantly decreased urinary tract infection in patients with traumatic spinal cord injury. Spinal Cord 2013, 51, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Biering-Sørensen, F.; Bagi, P.; Høiby, N. Urinary tract infections in patients with spinal cord lesions: Treatment and prevention. Drugs 2001, 61, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Garibaldi, R.A.; Burke, J.P.; Dickman, M.L.; Smith, C.B. Factors predisposing to bacteriuria during indwelling urethral catheterization. N. Engl. J. Med. 1974, 291, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Dinh, A.; Hallouin-Bernard, M.-C.; Davido, B.; Lemaignen, A.; Bouchand, F.; Duran, C.; Even, A.; Denys, P.; Perrouin-Verbe, B.; Sotto, A.; et al. Weekly Sequential Antibioprophylaxis for Recurrent Urinary Tract Infections Among Patients with Neurogenic Bladder: A Randomized Controlled Trial. Clin. Infect. Dis. 2020, 71, 3128–3135. [Google Scholar] [CrossRef]
- Salomon, J.; Denys, P.; Merle, C.; Chartier-Kastler, E.; Perronne, C.; Gaillard, J.-L.; Bernard, L. Prevention of urinary tract infection in spinal cord-injured patients: Safety and efficacy of a weekly oral cyclic antibiotic (WOCA) programme with a 2 year follow-up—An observational prospective study. J. Antimicrob. Chemother. 2006, 57, 784–788. [Google Scholar] [CrossRef] [Green Version]
- New, F.J.; Theivendrampillai, S.; Juliebø-Jones, P.; Somani, B. Role of Probiotics for Recurrent UTIs in the Twenty-First Century: A Systematic Review of Literature. Curr. Urol. Rep. 2022, 23, 19–28. [Google Scholar] [CrossRef]
- Cox, L.; He, C.; Bevins, J.; Clemens, J.Q.; Stoffel, J.T.; Cameron, A.P. Gentamicin bladder instillations decrease symptomatic urinary tract infections in neurogenic bladder patients on intermittent catheterization. Can. Urol. Assoc. J. 2017, 11, E350–E354. [Google Scholar] [CrossRef]
- Huen, K.H.; Nik-Ahd, F.; Chen, L.; Lerman, S.; Singer, J. Neomycin-polymyxin or gentamicin bladder instillations decrease symptomatic urinary tract infections in neurogenic bladder patients on clean intermittent catheterization. J. Pediatr. Urol. 2019, 15, e1–e178. [Google Scholar] [CrossRef]
- Ziadeh, T.; Chebel, R.; Labaki, C.; Saliba, G.; Helou, E.E. Bladder instillation for urinary tract infection prevention in neurogenic bladder patients practicing clean intermittent catheterization: A systematic review. Urologia 2022, 89, 261–267. [Google Scholar] [CrossRef]
- King, G.K.; Goodes, L.M.; Hartshorn, C.; Thavaseelan, J.; Jonescu, S.; Watts, A.; Rawlins, M.; Woodland, P.; Synnott, E.L.; Barrett, T.; et al. Intravesical hyaluronic acid with chondroitin sulphate to prevent urinary tract infection after spinal cord injury. J. Spinal Cord Med. 2022, 6, 1–7. [Google Scholar] [CrossRef]
- Gallien, P.; Amarenco, G.; Benoit, N.; Bonniaud, V.; Donzé, C.; Kerdraon, J.; de Seze, M.; Denys, P.; Renault, A.; Naudet, F.; et al. Cranberry versus placebo in the prevention of urinary infections in multiple sclerosis: A multicenter, randomized, placebo-controlled, double-blind trial. Mult. Scler. J. 2014, 20, 1252–1259. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.S.; Bhuta, T.; Simpson, J.M.; Craig, J.C. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst. Rev. 2012, 10, CD003265. [Google Scholar] [CrossRef] [PubMed]
- Günther, M.; Noll, F.; Nutzel, R.; Glaser, E.; Kramer, G.; Stohrer, M. Harnwegsinfektprophylaxe. Urinansäuerung mittels L-Methionin bei neurogener Blasenfunktionsstörung. Urol. B 2002, 42, 218. [Google Scholar] [CrossRef]
- Hansen, R.B.; Biering-Sørensen, F.; Kristensen, J.K. Urinary incontinence in spinal cord injured individuals 10–45 years after injury. Spinal Cord 2010, 48, 27–33. [Google Scholar] [CrossRef]
- Blanes, L.; Lourenco, L.; Carmagnani, M.I.; Ferreira, L.M. Clinical and socio-demographic characteristics of persons with traumatic paraplegia living in Sao Paulo, Brazil. Arq. Neuropsiquiatr. 2009, 67, 388–390. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.T.; Chiang, B.J.; Liao, C.H. Perspectives of medical treatment for overactive bladder. Urol. Sci. 2020, 31, 91–98. [Google Scholar]
- El Helou, E.; Labaki, C.; Chebel, R.; El Helou, J.; Abi Tayeh, G.; Jalkh, G.; Nemr, E. The use of mirabegron in neurogenic bladder: A systematic review. World J. Urol. 2020, 38, 2435–2442. [Google Scholar] [CrossRef]
- Park, J.S.; Lee, Y.S.; Lee, C.N.; Kim, S.H.; Kim, S.W.; Han, S.W. Efficacy and safety of mirabegron, a β3-adrenoceptor agonist, for treating neurogenic bladder in pediatric patients with spina bifida: A retrospective pilot study. World J. Urol. 2019, 37, 1665–1670. [Google Scholar] [CrossRef]
- Krhut, J.; Borovička, V.; Bílková, K.; Sýkora, R.; Míka, D.; Mokriš, J.; Zachoval, R. Efficacy and safety of mirabegron for the treatment of neurogenic detrusor overactivity-Prospective, randomized, double-blind, placebo-controlled study. Neurourol. Urodyn. 2018, 37, 2226–2233. [Google Scholar] [CrossRef]
- Welk, B.; Hickling, D.; McKibbon, M.; Radomski, S.; Ethans, K. A pilot randomized-controlled trial of the urodynamic efficacy of mirabegron for patients with neurogenic lower urinary tract dysfunction. Neurourol. Urodyn. 2018, 37, 2810–2817. [Google Scholar] [CrossRef]
- Wöllner, J.; Pannek, J. Initial experience with the treatment of neurogenic detrusor overactivity with a new β-3 agonist (mirabegron) in patients with spinal cord injury. Spinal Cord 2016, 54, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.; Momose, H.; Gotoh, D.; Morizawa, Y.; Hori, S.; Nakai, Y.; Miyake, M.; Anai, S.; Torimoto, K.; Tanaka, N.; et al. Video-urodynamic effects of vibegron, a new selective β3-adrenoceptor agonist, on antimuscarinic-resistant neurogenic bladder dysfunction in patients with spina bifida. Int. J. Urol. 2022, 29, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, K.; Teruya, K.; Uemura, O. Urodynamic effect of vibegron on neurogenic lower urinary tract dysfunction in individuals with spinal cord injury: A retrospective study. Spinal Cord 2022, 60, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Schurch, B.; Stöhrer, M.; Kramer, G.; Schmid, D.M.; Gaul, G.; Hauriet, D. Botulinum-A toxin for treating detrusor hyperreflexia in spinal cord injured patients: A new alternative to anticholinergic drugs? Preliminary results. J. Urol. 2000, 164, 692–697. [Google Scholar] [CrossRef]
- Reitz, A.; Stöhrer, M.; Kramer, G.; Del Popolo, G.; Chartier-Kastler, E.; Pannek, J.; Burgdörfer, H.; Göcking, K.; Madersbacher, H.; Schumacher, S.; et al. European experience of 200 cases treated with botulinum-A toxin injections into the detrusor muscle for urinary incontinence due to neurogenic detrusor overactivity. Eur Urol. 2004, 45, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Schurch, B.; Hauri, D.; Rodic, B.; Curt, A.; Meyer, M.; Rossier, A.B. Botulinum-A toxin as a treatment of detrusor-sphincter dyssynergia: A prospective study in 24 spinal cord injury patients. J. Urol. 1996, 155, 1023–1029. [Google Scholar] [CrossRef]
- Kuo, H.C. Botulinum A toxin urethral injection for the treatment of lower urinary tract dysfunction. J. Urol. 2003, 170, 1908–1912. [Google Scholar] [CrossRef]
- Schulte-Baukloh, H.; Weiss, C.; Stolze, T.; Herholz, J.; Sturzebecher, B.; Miller, K.; Knispel, H.H. Botulinum-A toxin detrusor and sphincter injection in treatment of overactive bladder syndrome: Objective outcome and patient satisfaction. Eur. Urol. 2005, 48, 984–990. [Google Scholar] [CrossRef]
- Dykstra, D.D.; Sidi, A.A. Treatment of detrusor-sphincter dyssynergia with botulinum A toxin: A doubleblind study. Arch. Phys. Med. Rehabil. 1990, 71, 24. [Google Scholar]
- Huang, M.; Chen, H.; Jiang, C.; Xie, K.; Tang, P.; Ou, R.; Zeng, J.; Liu, Q.; Li, Q.; Huang, J.; et al. Effects of botulinum toxin A injections in spinal cord injury patients with detrusor overactivity and detrusor sphincter dyssynergia. J. Rehabil. Med. 2016, 48, 683. [Google Scholar] [CrossRef] [Green Version]
- Utomo, E.; Groen, J.; Blok, B.F. Surgical management of functional bladder outlet obstruction in adults with neurogenic bladder dysfunction. Cochrane Database Syst. Rev. 2014, 24, CD004927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayo, M.E.; Ansell, J.S. The effect of bladder function on the dynamics of the ureterovesical junction. J. Urol. 1980, 123, 229–231. [Google Scholar] [CrossRef]
- Hackler, R.H.; Hall, M.K.; Zampieri, T.A. Bladder hypocompliance in the spinal cord injury population. J. Urol. 1989, 141, 1390–1393. [Google Scholar] [CrossRef]
- Park, W.H.; Kim, H.G.; Heo, Y.C.; So, J.G.; Lim, Y.S.; Shim, H.B. Urodynamic study in spinal cord injured patients: Classification and analysis of high risk parameters for upper tract deterioration. Korean J. Urol. 2000, 41, 92–98. [Google Scholar]
- Ahn, J.H.; Suh, J.K.; Lee, T. The role of bladder compliance observed by the videourodynamic study in spinal cord injured patients. Korean J. Urol. 2003, 44, 979–985. [Google Scholar]
- Klaphajone, J.; Kitisomprayoonkul, W.; Sriplakit, S. Botulinum toxin type A injections for treating neurogenic detrusor overactivity combined with low-compliance bladder in patients with spinal cord lesions. Arch. Phys. Med. Rehabil. 2000, 86, 2114–2118. [Google Scholar] [CrossRef]
- Goldwasser, B.; Webster, G.D. Augmentation and substitution enterocystoplasty. J. Urol. 1986, 135, 215–224. [Google Scholar] [CrossRef]
- Stöhrer, M.; Kramer, A.; Goepel, M.; Löchner-Ernst, D.; Kruse, D.; Rübben, H. Bladder autoaugmentation: An alternative for enterocystoplasty. Preliminary results. Neurourol. Urodyn. 1995, 14, 11–23. [Google Scholar] [CrossRef]
- Weinberg, A.C.; Boyd, S.D.; Lieskovsky, G.; Ahlering, T.A.; Skinner, D.G. The hemi-Kock ileocystoplasty: A low pressure anti-refluxing system. J. Urol. 1988, 140, 1380–1384. [Google Scholar] [CrossRef]
- Linker, D.G.; Tanagho, E.A. Complete sphincteric sphincterotomy: Correlation between endoscopin observation and the anatomic sphincter. J. Urol. 1975, l13, 348–352. [Google Scholar] [CrossRef]
- Farrugia, M.K.; Malone, P.S. Educational article: The Mitrofanoff procedure. J. Pediatr. Urol. 2010, 6, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Bailly, G.G.; Herschorn, S. Urinary diversion. In Textbook of the Neurogenic Bladder, 3rd ed.; Corcos, J., Ginsberg, D., Karsenty, G., Eds.; CRC Press: New York, NY, USA, 2016; pp. 531–543. [Google Scholar]
- Razdan, S.; Leboeuf, L.; Meinbach, D.S.; Weinstein, D.; Gousse, A.E. Current practice patterns in the urologic surveillance and management of patients with spinal cord injury. Urology 2003, 61, 893–896. [Google Scholar] [CrossRef]
- Stover, S.L.; Fine, P.R. The epidemiology and economics of spinal cord injury. Paraplegia 1987, 25, 225–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenwell, M.W.; Mangold, T.M.; Tolley, E.A.; Wall, B.M. Kidney disease as a predictor of mortality in chronic spinal cord injury. Am. J. Kidney Dis. 2007, 49, 383–393. [Google Scholar] [CrossRef]
- Consortium for Spinal Cord Medicine. Early acute management in adults with spinal cord injury: A clinical practice guideline for health-care professionals. J. Spinal Cord Med. 2008, 31, 403–479. [Google Scholar] [CrossRef]
- Wing, P.C. Early acute management in adults with spinal cord injury: A clinical practice guideline for health-care providers. Who should read it? J. Spinal Cord Med. 2008, 31, 360. [Google Scholar] [CrossRef] [Green Version]
- Samson, G.; Cardenas, D.D. Neurogenic bladder in spinal cord injury. Phys. Med. Rehabil. Clin. N. Am. 2007, 18, 255–274. [Google Scholar] [CrossRef]
- Chancellor, M.B.; Anderson, R.U.; Boone, T.B. Pharmacotherapy for neurogenic detrusor overactivity. Am. J. Phys. Med. Rehabil. 2006, 85, 536–545. [Google Scholar] [CrossRef]
- Lawrenson, R.; Wyndaele, J.J.; Vlachonikolis, I.; Farmer, C.; Glickman, S. Renal failure in patients with neurogenic lower urinary tract dysfunction. Neuroepidemiology 2001, 20, 138–143. [Google Scholar] [CrossRef]
- Kuo, H.C. Videourodynamic precision diagnosis and treatment of lower urinary tract symptoms in women. Urol. Sci. 2021, 32, 94–101. [Google Scholar] [CrossRef]
- Post, M.; Noreau, L. Quality of life after spinal cord injury. J. Neurol. Phys. Ther. 2005, 29, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Lane, G.I.; Roberts, W.W.; Mann, R.; O’Dell, D.; Stoffel, J.T.; Clemens, J.Q.; Cameron, A.P. Outcomes of renal calculi in patients with spinal cord injury. Neurourol. Urodyn. 2019, 38, 1901–1906. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; DeVivo, M.J.; Roseman, J.M. Current trend and risk factors for kidney stones in persons with spinal cord injury: A longitudinal study. Spinal Cord 2000, 38, 346–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartel, P.; Krebs, J.; Wöllner, J.; Göcking, K.; Pannek, J. Bladder stones in patients with spinal cord injury: A long-term study. Spinal Cord 2014, 52, 295–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; DeVivo, M.J.; Lloyd, L.K. Bladder stone incidence in persons with spinal cord injury: Determinants and trends, 1973–1996. Urology 2001, 58, 665–670. [Google Scholar] [CrossRef]
- Ord, J.; Lunn, D.; Reynard, J. Bladder management and risk of bladder stone formation in spinal cord injured patients. J. Urol. 2003, 170, 1734–1737. [Google Scholar] [CrossRef]
- DeVivo, M.J.; Fine, P.R.; Cutter, G.R.; Maetz, H.M. The risk of bladder calculi in patients with spinal cord injuries. Arch. Intern. Med. 1985, 145, 428–430. [Google Scholar] [CrossRef]
- Linsenmeyer, M.A.; Linsenmeyer, T.A. Accuracy of predicting bladder stones based on catheter encrustation in individuals with spinal cord injury. J. Spinal Cord Med. 2006, 29, 402–405. [Google Scholar] [CrossRef] [Green Version]
- Ost, M.C.; Lee, B.R. Review urolithiasis in patients with spinal cord injuries: Risk factors, management, and outcomes. Curr. Opin. Urol. 2006, 16, 93–99. [Google Scholar] [CrossRef]
- Grima, F.; Chartier-Kastler, E.; Ruffion, A. Surgical management of bladder stones in neurogenic bladder. Prog. Urol. 2007, 17, 465–469. [Google Scholar] [CrossRef]
- Kuo, H.C. Urodynamic evidence of effectiveness of botulinum A toxin injection in treatment of detrusor overactivity refractory to anticholinergic agents. Urology 2004, 63, 868–872. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.L.; Kuo, H.C. Long-term outcomes of augmentation enterocystoplasty with an ileal segment in patients with spinal cord injury. J. Formos. Med. Assoc. 2009, 108, 475–480. [Google Scholar] [CrossRef] [Green Version]
- Krebs, J.; Bartel, P.; Pannek, J. Functional outcome of supratrigonal cystectomy and augmentation ileocystoplasty in adult patients with refractory neurogenic lower urinary tract dysfunction. Neurourol. Urodyn. 2016, 35, 260–266. [Google Scholar] [CrossRef]
- Lendvay, T.S.; Cowan, C.A.; Mitchell, M.M.; Joyner, B.D.; Grady, R.W. Augmentation cystoplasty rates at children’s hospitals in the United States: A Pediatric Health Information System database study. J. Urol. 2006, 176, 1716–1720. [Google Scholar] [CrossRef]
- Reyblat, P.; Ginsberg, D.A. Augmentation cystoplasty: What are the indications? Curr. Urol. Rep. 2008, 9, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.Y.; Kuo, H.C. A real-world experience with augmentation enterocystoplasty-High patient satisfaction with high complication rates. Neurourol. Urodyn. 2018, 37, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Ali-El-Dein, B.; El-Tabey, N.; Abdel-Latif, M.; Abdel-Rahim, M.; El-Bahnasawy, M.S. Late uro-ileal cancer after incorporation of ileum into the urinary tract. J. Urol. 2002, 167, 84–87. [Google Scholar] [CrossRef]
- Husmann, D.A.; Rathbun, S.R. Long-term follow up of enteric bladder augmentations: The risk for malignancy. J. Pediatr. Urol. 2008, 4, 381–385. [Google Scholar] [CrossRef]
- Higuchi, T.; Granberg, C.; Fox, J.; Husmann, D. Augmentation cystoplasty and risk of neoplasia: Fact, fiction and controversy. J. Urol. 2010, 184, 2492–2496. [Google Scholar] [CrossRef]
- Kälble, T.; Hofmann, I.; Riedmiller, H.; Vergho, D. Tumor growth in urinary diversion: A multicenter analysis. Eur. Urol. 2011, 60, 1081–1086. [Google Scholar] [CrossRef]
- Castellan, M.; Gosalbez, R.; Perez-Brayfield, M.; Healey, P.; McDonald, R.; Labbie, A.; Lendvay, T. Tumor in bladder reservoir after gastrocystoplasty. J. Urol. 2007, 178, 1771–1774. [Google Scholar] [CrossRef] [PubMed]
- Vemulakonda, V.M.; Lendvay, T.S.; Shnorhavorian, M.; Joyner, B.D.; Kaplan, H.; Mitchell, M.E.; Grady, R.W. Metastatic adenocarcinoma after augmentation gastrocystoplasty. J. Urol. 2008, 179, 1094–1097. [Google Scholar] [CrossRef] [PubMed]
- Soergel, T.M.; Cain, M.P.; Misseri, R.; Gardner, T.A.; Koch, M.O.; Rink, R.C. Transitional cell carcinoma of the bladder following augmentation cystoplasty for the neuropathic bladder. J. Urol. 2004, 172, 1649–1652. [Google Scholar] [CrossRef]
- Kispal, Z.; Balogh, D.; Erdei, O.; Kehl, D.; Juhász, Z.; Vastyan, A.M.; Farkas, A.; Pinter, A.B.; Vajda, P. Complications after bladder augmentation or substitution in children: A prospective study of 86 patients. BJU Int. 2011, 108, 282. [Google Scholar] [CrossRef] [PubMed]
- Biardeau, X.; Chartier-Kastler, E.; Rouprêt, M.; Phé, V. Risk of malignancy after augmentation cystoplasty: A systematic review. Neurourol. Urodyn. 2016, 35, 675–682. [Google Scholar] [CrossRef]
- Higgy, N.A.; Verma, A.K.; Ertürk, E.; Oberley, T.D.; El-Aaser, A.A.; El-Merzabani, M.M.; Bryan, G.T. Escherichia coli infection of the urinary bladder: Induction of tumours in rats receiving nitrosamine precursors and augmentation of bladder carcinogenesis by N-nitrosobutyl (4-hydroxybutyl) amine. IARC Sci. Publ. 1987, 84, 380–383. [Google Scholar]
- Nurse, D.E.; Mundy, A.R. Cystoplasty infection and cancer. Neurourol. Urodyn. 1989, 8, 343–344. [Google Scholar]
- Vajda, P.; Kaiser, L.; Magyarlaki, T.; Farkas, A.; Vastyan, A.M.; Pinter, A.B. Histological findings after colocystoplasty and gastrocystoplasty. J. Urol. 2002, 168, 698–701. [Google Scholar] [CrossRef]
- Austen, M.; Kalble, T. Secondary malignancies in different forms of urinary diversion using isolated gut. J. Urol. 2004, 172, 831–838. [Google Scholar] [CrossRef]
- Malone, M.J.; Izes, J.K.; Hurley, L.J. Carcinogenesis: The fate of intestinal segments used in urinary reconstruction. Urol. Clin. N. Am. 1997, 24, 723–728. [Google Scholar] [CrossRef]
- Dixon, B.P.; Chu, A.; Henry, J.; Kim, R.; Bissler, J.J. Increased cancer risk of augmentation cystoplasty: Possible role for hyperosmolal microenvironment on DNA damage recognition. Mutat. Res. 2009, 670, 88–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamid, R.; Greenwell, T.; Nethercliffe, J.M.; Freeman, A.; Venn, S.N.; Woodhouse, C.R.J. Routine surveillance cystoscopy for patients with augmentation and substitution cystoplasty for benign urological conditions: Is it necessary? BJU Int. 2009, 104, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.; Lewis, M.A. Bladder augmentation surgery—What about the malignant risk? Eur. J. Pediatr. Surg. 1999, 9, 39–40. [Google Scholar] [CrossRef]
- Anquetil, C.; Abdelhamid, S.; Gelis, A.; Fattal, C. Botulinum toxin therapy for neurogenic detrusor hyperactivity versus augmentation enterocystoplasty: Impact on the quality of life of patients with SCI. Spinal Cord 2016, 54, 1031–1035. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.C.; Chen, S.L.; Chou, C.L.; Chuang, Y.C.; Huang, Y.H.; Juan, Y.S.; Lee, W.C.; Liao, C.H.; Tsai, Y.C.; Tsai, Y.A.; et al. Taiwanese Continence Society clinical guidelines for diagnosis and management of neurogenic lower urinary tract dysfunction. Urol. Sci. 2014, 25, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Schurch, B. Neurogenic voiding disorders. Current status of diagnosis and therapy. Schweiz. Med. Wochenschr. 2000, 130, 1618–1626. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Ou, Y.-C.; Hu, J.-C.; Yang, M.-H.; Lin, W.-Y.; Huang, S.-W.; Lin, W.-Y.; Lin, C.-C.; Lin, V.C.; Chuang, Y.-C.; et al. Bladder Management Strategies for Urological Complications in Patients with Chronic Spinal Cord Injury. J. Clin. Med. 2022, 11, 6850. https://doi.org/10.3390/jcm11226850
Chen Y-C, Ou Y-C, Hu J-C, Yang M-H, Lin W-Y, Huang S-W, Lin W-Y, Lin C-C, Lin VC, Chuang Y-C, et al. Bladder Management Strategies for Urological Complications in Patients with Chronic Spinal Cord Injury. Journal of Clinical Medicine. 2022; 11(22):6850. https://doi.org/10.3390/jcm11226850
Chicago/Turabian StyleChen, Yu-Chen, Yin-Chien Ou, Ju-Chuan Hu, Min-Hsin Yang, Wei-Yu Lin, Shi-Wei Huang, Wei-Yu Lin, Chih-Chieh Lin, Victor C. Lin, Yao-Chi Chuang, and et al. 2022. "Bladder Management Strategies for Urological Complications in Patients with Chronic Spinal Cord Injury" Journal of Clinical Medicine 11, no. 22: 6850. https://doi.org/10.3390/jcm11226850