

Prevalence of Venous Thromboembolism in Intensive Care Units: A Meta-Analysis
 ,
,
Abstract
:1. Introduction
2. Methods
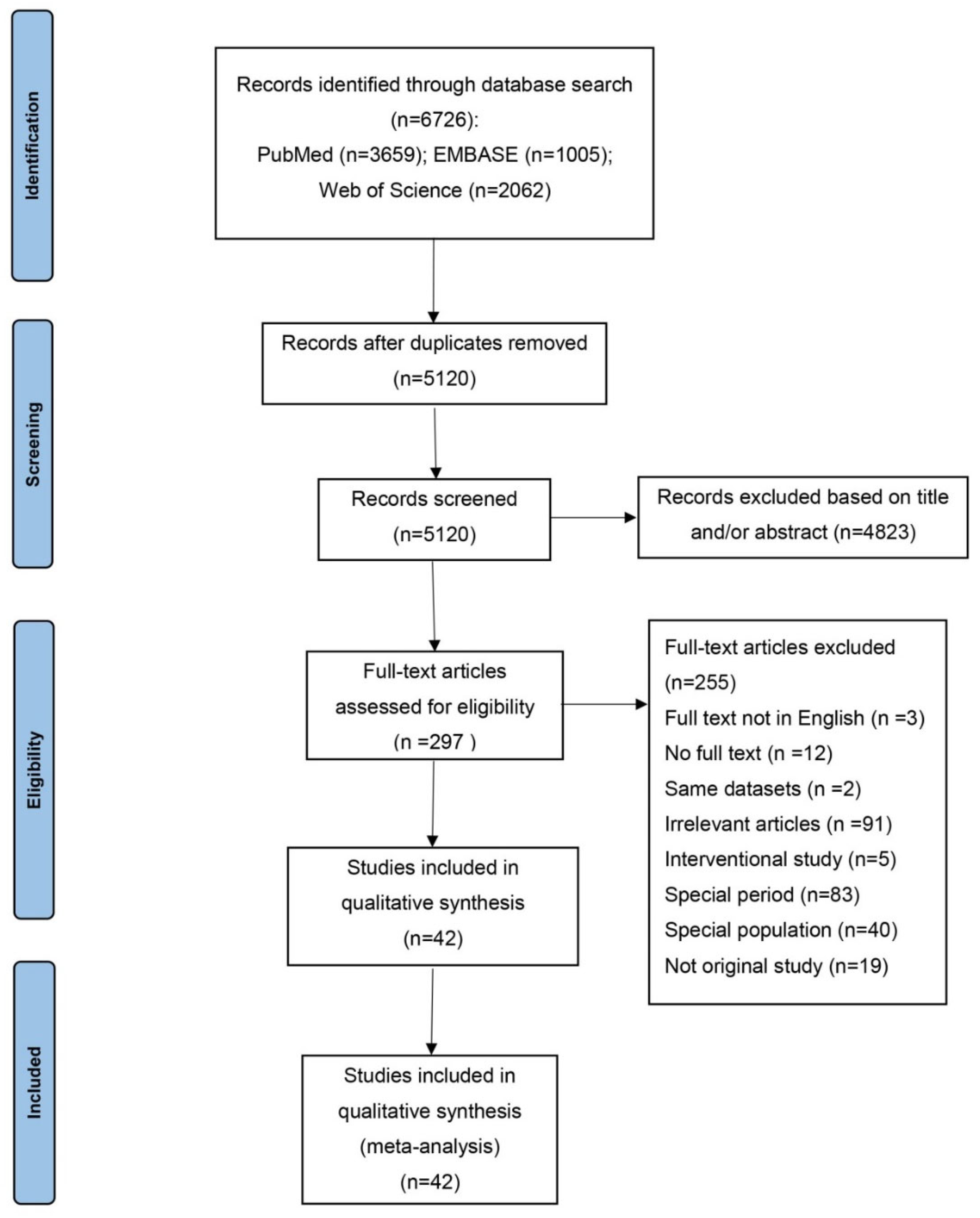
2.1. Literature Search
2.2. Study Selection and Data Extraction
2.3. Quality Evaluation
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Included Studies and Quality Assessment
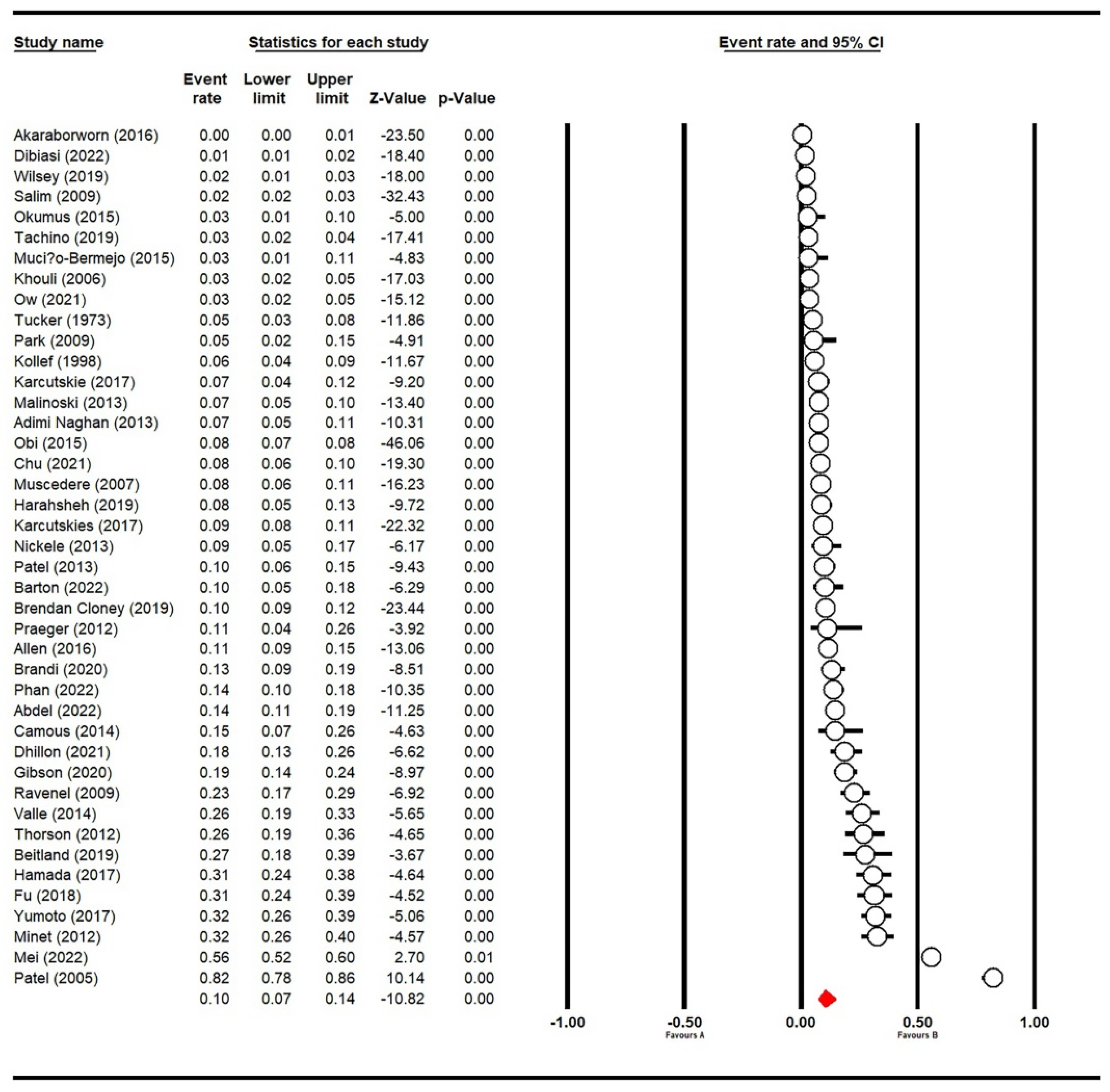
3.2. Prevalence of VTE in ICU Patients
3.3. Subgroup Analyses and Meta-Regression
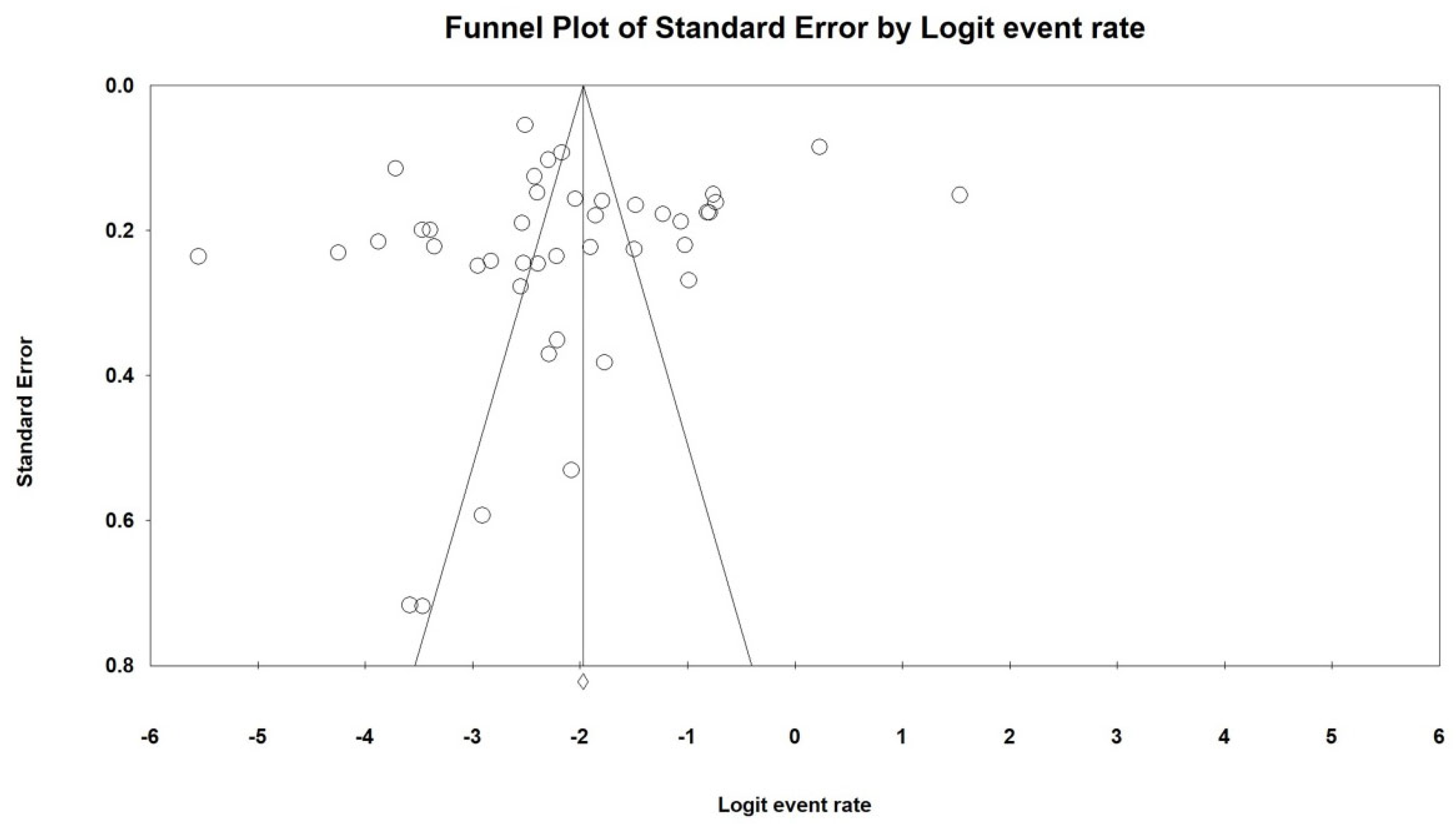
3.4. Publication Bias and Sensitivity Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tritschler, T.; Salvatore, S.P.; Kahn, S.R.; Garcia, D.; Delluc, A.; Kraaijpoel, N.; Langlois, N.; Girard, P.; Le Gal, G. ISTH definition of pulmonary embolism-related death and classification of the cause of death in venous thromboembolism studies: Validation in an autopsy cohort. J. Thromb. Haemost. JTH 2021, 19, 2514–2521. [Google Scholar] [CrossRef]
- Wichmann, D.; Sperhake, J.P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients with COVID-19: A Prospective Cohort Study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Wickham, N.; Gallus, A.S.; Walters, B.N.; Wilson, A.; NHMRC VTE Prevention Guideline Adaptation Committee. Prevention of venous thromboembolism in patients admitted to Australian hospitals: Summary of national health and medical research council clinical practice guideline. Intern. Med. J. 2012, 42, 698–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheres, L.J.J.; Lijfering, W.M.; Cannegieter, S.C. Current and future burden of venous thrombosis: Not simply predictable. Res. Pract. Thromb. Haemost. 2018, 2, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Cook, D.J.; Meade, M.O.; Griffith, L.E.; Mehta, G.; Rocker, G.M.; Marshall, J.C.; Hodder, R.; Martin, C.M.; Heyland, D.K.; et al. Burden of illness in venous thromboembolism in critical care: A multicenter observational study. J. Crit. Care 2005, 20, 341–347. [Google Scholar] [CrossRef]
- Akaraborworn, O.; Chittawatanarat, K.; Chatmongkolchart, S.; Kitsiripant, C. Modalities in venous thromboembolism prophylaxis and symptomatic venous thromboembolism occurrence in critically ill surgical patients (THAI-SICU Study). J. Med. Assoc. Thail. 2016, 99 (Suppl. S6), S112–S117. [Google Scholar]
- Baylis, R.A.; Smith, N.L.; Klarin, D.; Fukaya, E. Epidemiology and Genetics of Venous Thromboembolism and Chronic Venous Disease. Circ. Res. 2021, 128, 1988–2002. [Google Scholar] [CrossRef]
- Nobre, C.; Thomas, B. Analysis of National Trends in Admissions for Pulmonary Embolism. Chest 2016, 150, 250. [Google Scholar] [CrossRef] [Green Version]
- Gregson, J.; Kaptoge, S.; Bolton, T.; Pennells, L.; Willeit, P.; Burgess, S.; Bell, S.; Sweeting, M.; Rimm, E.B.; Kabrhel, C.; et al. Cardiovascular Risk Factors Associated With Venous Thromboembolism. JAMA Cardiol. 2019, 4, 163–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krenitsky, N.; Friedman, A.M.; Yu, K.; Gyamfi-Bannerman, C.; Williams-Kane, J.; O’Shaugnessy, F.; Huang, Y.; Wright, J.D.; D’Alton, M.E.; Wen, T. Trends in Venous Thromboembolism and Associated Risk Factors During Delivery Hospitalizations from 2000 to 2018. Obstet. Gynecol. 2022, 139, 223–234. [Google Scholar] [CrossRef]
- Nemeth, B.; Lijfering, W.M.; Nelissen, R.; Schipper, I.B.; Rosendaal, F.R.; le Cessie, S.; Cannegieter, S.C. Risk and Risk Factors Associated With Recurrent Venous Thromboembolism Following Surgery in Patients with History of Venous Thromboembolism. JAMA Netw. Open 2019, 2, e193690. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Bang, S.M.; Kim, S.; Lee, H.J.; Shin, D.Y.; Koh, Y.; Lee, Y.G.; Cha, Y.; Kim, Y.J.; Kim, J.H.; et al. The incidence, risk factors and prognostic implications of venous thromboembolism in patients with gastric cancer. J. Thromb. Haemost. JTH 2010, 8, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Tøndel, B.G.; Morelli, V.M.; Hansen, J.B.; Braekkan, S.K. Risk factors and predictors for venous thromboembolism in people with ischemic stroke: A systematic review. J. Thromb. Haemost. JTH 2022, 20, 2173–2186. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.T.; Jitaroon, K.; Song, S.; Roozdar, P.; Wangworat, Y.; Ibrahim, N.; Ma, Y.; Rao, V.K.; Chang, S.D.; Fernandez-Miranda, J.C.; et al. Venous thromboembolism rates and risk factors following endoscopic skull base surgery. Int. Forum Allergy Rhinol. 2022, 12, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Spencer, F.A.; White, R.H. The epidemiology of venous thromboembolism. J. Thromb. Thrombolysis 2016, 41, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Flinterman, L.E.; van Hylckama Vlieg, A.; Cannegieter, S.C.; Rosendaal, F.R. Long-term survival in a large cohort of patients with venous thrombosis: Incidence and predictors. PLoS Med. 2012, 9, e1001155. [Google Scholar] [CrossRef] [Green Version]
- Morange, P.E.; Suchon, P. Genetics of venous thrombosis: Update in 2015. Thromb. Haemost. 2015, 114, 910–919. [Google Scholar]
- Lutsey, P.L.; Evensen, L.H.; Thenappan, T.; Prins, K.W.; Walker, R.F.; Farley, J.F.; MacLehose, R.F.; Alonso, A.; Zakai, N.A. Incidence and Risk Factors of Pulmonary Hypertension After Venous Thromboembolism: An Analysis of a Large Health Care Database. J. Am. Heart Assoc. 2022, 11, e024358. [Google Scholar] [CrossRef]
- Makedonov, I.; Kahn, S.R.; Abdulrehman, J.; Schulman, S.; Delluc, A.; Gross, P.; Galanaud, J.P. Prevention of the Postthrombotic Syndrome with Anticoagulation: A Narrative Review. Thromb. Haemost. 2022, 122, 1255–1264. [Google Scholar] [CrossRef]
- Vrabel, M. Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Oncol. Nurs. Forum 2015, 42, 552–554. [Google Scholar] [CrossRef]
- Parker, G.; Beresford, B.; Clarke, S.; Gridley, K.; Pitman, R.; Spiers, G.; Light, K. Technical Report for SCIE Research Review on the Prevalence and Incidence of Parental Mental Health Problems and the Detection, Screening and Reporting of Parental Mental Health Problems; University of York: Heslington, UK, 2008. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, H.H.; Carson, P.H.; Bass, N.M.; Sharratt, G.P.; Stock, J.P. Results of early mobilization and discharge after myocardial infarction. Br. Med. J. 1973, 1, 10–13. [Google Scholar] [CrossRef] [Green Version]
- Kollef, M.H.; Eisenberg, P.R.; Shannon, W. A rapid assay for the detection of circulating D-dimer is associated with clinical outcomes among critically ill patients. Crit. Care Med. 1998, 26, 1054–1060. [Google Scholar] [CrossRef]
- Khouli, H.; Shapiro, J.; Pham, V.P.; Arfaei, A.; Esan, O.; Jean, R.; Homel, P. Efficacy of deep venous thrombosis prophylaxis in the medical intensive care unit. J. Intensive Care Med. 2006, 21, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Muscedere, J.G.; Heyland, D.K.; Cook, D. Venous thromboembolism in critical illness in a community intensive care unit. J. Crit. Care 2007, 22, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Salim, A.; Hadjizacharia, P.; Dubose, J.; Kobayashi, L.; Inaba, K.; Chan, L.S.; Margulies, D.R. What is the significance of thrombocytosis in patients with trauma? J. Trauma-Inj. Infect. Crit. Care 2009, 66, 1349–1354. [Google Scholar] [CrossRef]
- Ravenel, J.G.; Northam, M.C.; Nguyen, S.A. Negative predictive value of computed tomography pulmonary angiography with indirect computed tomography venography in intensive care unit patients. J. Comput. Assist. Tomogr. 2009, 33, 739–742. [Google Scholar] [CrossRef]
- Park, M.S.; Martini, W.Z.; Dubick, M.A.; Salinas, J.; Butenas, S.; Kheirabadi, B.S.; Pusateri, A.E.; Vos, J.A.; Guymon, C.H.; Wolf, S.E.; et al. Thromboelastography as a better indicator of hypercoagulable state after injury than prothrombin time or activated partial thromboplastin time. J. Trauma 2009, 67, 266–275; discussion 275–276. [Google Scholar] [CrossRef] [Green Version]
- Thorson, C.M.; Ryan, M.L.; Van Haren, R.M.; Curia, E.; Barrera, J.M.; Guarch, G.A.; Busko, A.M.; Namias, N.; Livingstone, A.S.; Proctor, K.G. Venous thromboembolism after trauma: A never event?*. Crit. Care Med. 2012, 40, 2967–2973. [Google Scholar] [CrossRef] [PubMed]
- Praeger, A.J.; Westbrook, A.J.; Nichol, A.D.; Wijemunige, R.; Davies, A.R.; Lyon, S.M.; Wills, J.L.; Bailey, M.; Rosenfeld, J.V.; Cooper, D.J. Deep vein thrombosis and pulmonary embolus in patients with traumatic brain injury: A prospective observational study. Crit. Care Resusc. J. Australas. Acad. Crit. Care Med. 2012, 14, 10–13. [Google Scholar]
- Minet, C.; Lugosi, M.; Savoye, P.Y.; Menez, C.; Ruckly, S.; Bonadona, A.; Schwebel, C.; Hamidfar-Roy, R.; Dumanoir, P.; Ara-Somohano, C.; et al. Pulmonary embolism in mechanically ventilated patients requiring computed tomography: Prevalence, risk factors, and outcome. Crit. Care Med. 2012, 40, 3202–3208. [Google Scholar] [CrossRef] [PubMed]
- Adimi Naghan, P.; Malekmohammad, M.; Jamaati, H.; Sharifkashani, B.; Najafi, A.; Hashemian, S.M. Venous thromboembolism in medical critically ill patients: Prevalence and incidence. Acta Med. Iran. 2013, 51, 168–171. [Google Scholar] [PubMed]
- Malinoski, D.; Ewing, T.; Patel, M.S.; Jafari, F.; Sloane, B.; Nguyen, B.; Barrios, C.; Kong, A.; Cinat, M.; Dolich, M.; et al. Risk factors for venous thromboembolism in critically ill trauma patients who cannot receive chemical prophylaxis. Inj. Int. J. Care Inj. 2013, 44, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Nickele, C.M.; Kamps, T.K.; Medow, J.E. Safety of a DVT chemoprophylaxis protocol following traumatic brain injury: A single center quality improvement initiative. Neurocritical Care 2013, 18, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.S.; Ewing, T.; Kong, A.; Nguyen, D.; Lau, C.; Barrios, C.; Cinat, M.; Dolich, M.; Lekawa, M.; Malinoski, D. Risk factors for venous thromboembolism in critically ill nontrauma surgical patients who cannot receive chemical prophylaxis. Am. J. Surg. 2013, 206, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Camous, L.; Veyradier, A.; Darmon, M.; Galicier, L.; Mariotte, E.; Canet, E.; Parquet, N.; Azoulay, É. Macrovascular thrombosis in critically ill patients with thrombotic micro-angiopathies. Intern. Emerg. Med. 2014, 9, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Valle, E.J.; Van Haren, R.M.; Allen, C.J.; Jouria, J.M.; Bullock, M.R.; Schulman, C.I.; Namias, N.; Livingstone, A.S.; Proctor, K.G. Does traumatic brain injury increase the risk for venous thromboembolism in polytrauma patients? J. Trauma Acute Care Surg. 2014, 77, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Okumus, G.; Ozcelik, B.; Sasani, H.; Ozcan, P.E.; Kiyan, E.; Salmaslioglu, A.; Senturk, E.; Issever, H.; Arseven, O. Do appropriate thromboprophylaxis and routine physiotherapy prevent venous thromboembolism in intensive care unit? Turk. Gogus Kalp Damar Cerrahisi Derg. -Turk. J. Thorac. Cardiovasc. Surg. 2015, 23, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Obi, A.T.; Pannucci, C.J.; Nackashi, A.; Abdullah, N.; Alvarez, R.; Bahl, V.; Wakefield, T.W.; Henke, P.K. Validation of the Caprini venous thromboembolism risk assessment model in citically ill surgical patients. JAMA Surg. 2015, 150, 941–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muciño-Bermejo, J.; Carrillo-Esper, R.; Méndez-Sánchez, N.; Uribe, M. Thrombosis and hemorrhage in the critically ill cirrhotic patients: Five years retrospective prevalence study. Ann. Hepatol. 2015, 14, 93–98. [Google Scholar] [CrossRef]
- Allen, C.J.; Murray, C.R.; Meizoso, J.P.; Ginzburg, E.; Schulman, C.I.; Lineen, E.B.; Namias, N.; Proctor, K.G. Surveillance and early management of deep vein thrombosis decreases rate of pulmonary embolism in high-risk trauma patients. J. Am. Coll. Surg. 2016, 222, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Hamada, S.R.; Espina, C.; Guedj, T.; Buaron, R.; Harrois, A.; Figueiredo, S.; Duranteau, J. High level of venous thromboembolism in critically ill trauma patients despite early and well-driven thromboprophylaxis protocol. Ann. Intensive Care 2017, 7, 97. [Google Scholar] [CrossRef] [PubMed]
- Karcutskie, C.A.; Dharmaraja, A.; Patel, J.; Eidelson, S.A.; Martin, A.G.; Lineen, E.B.; Namias, N.; Schulman, C.I.; Proctor, K.G. Relation of antifactor-Xa peak levels and venous thromboembolism after trauma. J. Trauma Acute Care Surg. 2017, 83, 1102–1107. [Google Scholar] [CrossRef] [PubMed]
- Karcutskie, C.A.; Meizoso, J.P.; Ray, J.J.; Horkan, D.; Ruiz, X.D.; Schulman, C.I.; Namias, N.; Proctor, K.G. Association of mechanism of Injury with risk for venous thromboembolism after trauma. JAMA Surg. 2017, 152, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Yumoto, T.; Naito, H.; Yamakawa, Y.; Iida, A.; Tsukahara, K.; Nakao, A. Venous thromboembolism in major trauma patients: A single-center retrospective cohort study of the epidemiology and utility of D-dimer for screening. Acute Med. Surg. 2017, 4, 394–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Y.; Liu, Y.; Chen, S.; Jin, Y.; Jiang, H. The combination of Caprini risk assessment scale and thrombotic biomarkers to evaluate the risk of venous thromboembolism in critically ill patients. Medicine 2018, 97, e13232. [Google Scholar] [CrossRef] [PubMed]
- Wilsey, H.A.; Pandya, K.; Beavers, C.; Li, X.S.; Ather, A. Comparison of venous thromboembolism prophylactic measures post coronary artery bypass graft surgery. Am. J. Cardiovasc. Drugs 2019, 19, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Brendan Cloney, M.; Goergen, J.; Hopkins, B.S.; Dhillon, E.S.; Dahdaleh, N.S. Factors associated with venous thromboembolic events following ICU admission in patients undergoing spinal surgery: An analysis of 1269 consecutive patients. J. Neurosurg. Spine 2019, 30, 99–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beitland, S.; Wimmer, H.; Lorentsen, T.; Jacobsen, D.; Draegni, T.; Brunborg, C.; Klow, N.E.; Sandset, P.M.; Sunde, K. Venous thromboembolism in the critically ill: A prospective observational study of occurrence, risk factors and outcome. Acta Anaesthesiol. Scand. 2019, 63, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Harahsheh, Y.; Duff, O.C.; Ho, K.M. Thromboelastography predicts thromboembolism in critically ill coagulopathic patients*. Crit. Care Med. 2019, 47, 826–832. [Google Scholar] [CrossRef]
- Tachino, J.; Yamamoto, K.; Shimizu, K.; Shintani, A.; Kimura, A.; Ogura, H.; Shimazu, T. Quick risk assessment profile (qRAP) is a prediction model for post-traumatic venous thromboembolism. Injury 2019, 50, 1540–1544. [Google Scholar] [CrossRef] [PubMed]
- Brandi, G.; Schmidlin, A.; Klinzing, S.; Schüpbach, R.; Unseld, S.; Pagnamenta, A. Delayed prophylaxis with unfractionated heparin increases the risk of venous thromboembolic events in patients with moderate to severe traumatic brain injury: A retrospective analysis. Anaesthesiol. Intensive Ther. 2020, 52, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.D.; Colvin, M.O.; Park, M.J.; Lai, Q.; Lin, J.; Negassa, A.; Shah, C.D.; Langston, M.D. Prevalence and predictors of deep vein thrombosis in critically ill medical patients who underwent diagnostic duplex ultrasonography. J. Intensive Care Med. 2020, 35, 1062–1066. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, N.K.; Hashim, Y.M.; Conde, G.; Phillips, G.; Fierro, N.M.; Yong, F.; Berezin, N.; Ley, E.J. Early propranolol is associated with lower risk of venous thromboembolism after traumatic brain injury. Am. Surg. 2021, 87, 1556–1560. [Google Scholar] [CrossRef] [PubMed]
- Chu, Q.; Liao, L.; Wei, W.; Ye, Z.; Zeng, L.; Qin, C.; Tang, Y. Venous thromboembolism in ICU patients with intracerebral hemorrhage: Risk factors and the prognosis after anticoagulation therapy. Int. J. Gen. Med. 2021, 14, 5397–5404. [Google Scholar] [CrossRef] [PubMed]
- Ow, T.W.; Fatourou, E.; Rabinowich, L.; van den Boom, B.P.; Nair, S.; Patel, V.C.; Hogan, B.; McPhail, M.; Roberts, L.N.; Bernal, W. Prevalence of bleeding and thrombosis in critically ill patients with chronic liver disease. Thromb. Haemost. 2021, 122, 1006–1016. [Google Scholar] [CrossRef]
- Phan, B.; Fagaragan, L.; Alaraj, A.; Kim, K.S. Multidisciplinary bundle approach in venous thromboembolism prophylaxis in patients with non-traumatic subarachnoid hemorrhage. Clin. Appl. Thromb. Hemost. 2022, 28, 10760296221074682. [Google Scholar] [CrossRef] [PubMed]
- Mei, R.; Wang, G.; Chen, R.; Wang, H. The ICU-venous thromboembolism score and tumor grade can predict inhospital venous thromboembolism occurrence in critical patients with tumors. World J. Surg. Oncol. 2022, 20, 245. [Google Scholar] [CrossRef] [PubMed]
- Dibiasi, C.; Gratz, J.; Wiegele, M.; Schaden, E. Anti-factor Xa activity is not associated with venous thromboembolism in critically ill patients receiving enoxaparin for thromboprophylaxis: A retrospective observational study. Front. Med. 2022, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Barton, C.; Shapiro, D. Safety of prophylactic anticoagulation during bedside procedures: A prospective multicenter observational study. World J. Surg. 2022, 46, 2625–2631. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aziz, H.; Alikhan, R.; Arabi, Y.M. The association of timing of pharmacological prophylaxis and venous thromboembolism in patients with moderate-to-severe traumatic brain injury: A retrospective cohort study. Ann. Thorac. Med. 2022, 17, 102–109. [Google Scholar]
- Ajmal, F.; Haroon, M.; Kaleem, U.; Gul, A.; Khan, J. Comparison of chemical and mechanical prophylaxis of venous thromboembolism in non-surgical mechanically ventilated patients. Cureus 2021, 13, e19548. [Google Scholar] [CrossRef] [PubMed]
- Abizanda, R.; Marse, P.; Abadal, J.M. Simplified acute physiology score. Crit. Care Med. 1985, 13, 517. [Google Scholar] [CrossRef]
- Horinuki, F.; Noguchi-Watanabe, M.; Takai, Y.; Yamahana, R.; Ohno, N.; Okada, S.; Mori, S.I.; Yamamoto-Mitani, N. The experience of persons with hematological malignancy when communicating with health care professionals. Qual. Health Res. 2018, 28, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Buja, A.; Damiani, G.; Gini, R.; Visca, M.; Federico, B.; Donato, D.; Francesconi, P.; Marini, A.; Donatini, A.; Brugaletta, S.; et al. Systematic age-related differences in chronic disease management in a population-based cohort study: A new paradigm of primary care is required. PLoS ONE 2014, 9, e91340. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, I.; Thukral, N.; Hasija, Y. Genetics of human age related disorders. Adv. Gerontol. 2015, 28, 228–247. [Google Scholar]
- Outlaw, D.; Dai, C.; Al-Obaidi, M.; Harmon, C.; Giri, S.; Bhatia, S.; Williams, G.R. The association of polypharmacy with functional status impairments, frailty, and health-related quali ty of life in older adults with gastrointestinal malignancy—Results from the Cancer and Aging Resi lience Evaluation (CARE) registry. J. Geriatr. Oncol 2022, 38, 118. [Google Scholar]
- Roldn, V.; Marn, F.; Garca, A.; Tello-Montoliu, A.; Lip, G.Y. Is an advanced age an additive risk factor to the prothrombotic or hypercoagulable state in atrial fi brillation? Int. J. Cardiol. 2006, 110, 265–266. [Google Scholar] [CrossRef] [PubMed]
- Merli, G.J.; Crabbe, S.; Paluzzi, R.G.; Fritz, D. Etiology, incidence, and prevention of deep vein thrombosis in acute spinal cord injury. Arch. Phys. Med. Rehabil. 1993, 74, 1199–1205. [Google Scholar] [PubMed]
- Putz, C.; Schuld, C.; Gantz, S.; Grieser, T.; Akbar, M.; Moradi, B.; Wiedenhöfer, B.; Fürstenberg, C.H.; Gerner, H.J.; Rupp, R. The effect of polytrauma as a possible confounder in the outcome of monotraumatic vs polytraumatic pa raplegic patients: A clinical cohort study. Spinal Cord 2011, 49, 721–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, M.; Ortego, A. Calculated Decisions: Injury Severity Score (ISS). Pediatr. Emerg. Med. Pract. 2019, 16, Cd1-2. [Google Scholar] [PubMed]
- Helms, J.; Middeldorp, S.; Spyropoulos, A.C. Thromboprophylaxis in critical care. Intensive Care Med. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Khatri, A.; Davies, A.H.; Shalhoub, J. Mechanical prophylaxis for venous thromboembolism prevention in obese individuals. Phlebology 2021, 36, 768–770. [Google Scholar] [CrossRef] [PubMed]
- Afshari, A.; Fenger-Eriksen, C.; Monreal, M.; Verhamme, P. European guidelines on perioperative venous thromboembolism prophylaxis: Mechanical prophylaxis. Eur. J. Anaesth. 2018, 35, 112–115. [Google Scholar] [CrossRef]
- Hong, Y.; Zhang, Y.; Xiang, Y.; Ye, Z.; Lu, X. Incidence of venous thromboembolism and hemorrhage in Chinese patients after pulmonary lobectomy: Mechanical prophylaxis or mechanical prophylaxis combined with pharmacological prophylaxis: A randomized controlled trial. Ann. Transl. Med. 2021, 9, 1478. [Google Scholar] [CrossRef]
- Kakkos, S.; Kirkilesis, G.; Caprini, J.A.; Geroulakos, G.; Nicolaides, A.; Stansby, G.; Reddy, D.J. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism. Cochrane Database Syst. Rev. 2022, 1, Cd005258. [Google Scholar] [CrossRef]
- Long, J.; Huang, G.; Liang, W.; Liang, B.; Chen, Q.; Xie, J.; Jiang, J.; Su, L. The prevalence of schizophrenia in mainland China: Evidence from epidemiological surveys. Acta Psychiatr. Scand. 2014, 130, 244–256. [Google Scholar] [CrossRef]
- Winsper, C.; Ganapathy, R.; Marwaha, S.; Large, M.; Birchwood, M.; Singh, S.P. A systematic review and meta-regression analysis of aggression during the first episode of psychosis. Acta Psychiatr. Scand. 2013, 128, 413–421. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. | First Author (Year) | Reference | Country | Year of Study Conducted | Sampling Method | Department | Sample Size | Male | Mean Age | BMI | Thromboprophylaxis Strategy | SAPS II Score | Malignancy | Spinal Cord Injury | ISS | Quality Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Tucker (1973) | (Tucker et al., 1973) [25] | Britain | 1970–1971 | NR | CICU | 342 | 342 | 56.5 | NR | Pharmacological prophylaxis | NR | NR | NR | NR | 3 |
| 2 | Kollef (1998) | (Kollef et al., 1998) [26] | USA | 1995 | NR | MICU | 323 | 164 | 57.5 | NR | NR | NR | NR | NR | NR | 4 |
| 3 | Patel (2005) | (Patel et al., 2005) [5] | Canada | 2000 | consecutive | ICU | 299 | 159 | 63.1 | NR | Both * | NR | NR | NR | NR | 5 |
| 4 | Khouli (2006) | (Khouli et al., 2006) [27] | USA | 1999–2001 | consecutive | MICU | 801 | NR | NR | NR | NR | NR | NR | NR | NR | 3 |
| 5 | Muscedere (2007) | (Muscedere et al., 2007) [28] | Canada | 2001–2002 | consecutive | ICU | 600 | 362 | 59.5 | NR | Both * | NR | NR | NR | NR | 6 |
| 6 | Salim (2009) | (Salim et al., 2009) [29] | USA | 1998–2005 | NR | SICU | 3286 | 2609 | 36.7 | 26.9 | NR | NR | NR | NR | 19.3 | 2 |
| 7 | Ravenel (2009) | (Ravenel et al., 2009) [30] | USA | 2004–2006 | consecutive | ICU | 181 | 107 | 54.3 | NR | Pharmacological prophylaxis | NR | NR | NR | NR | 6 |
| 8 | Park (2009) | (Park et al., 2009) [31] | USA | 2004–2005 | NR | ICU | 58 | 44 | 48.6 | NR | Both * | NR | NR | NR | 20.2 | 4 |
| 9 | Thorson (2012) | (Thorson et al., 2012) [32] | USA | 2009–2012 | NR | TICU | 106 | 78 | 47.0 | NR | Both * | NR | 2 | 5 | 30.0 | 3 |
| 10 | Praeger (2012) | (Praeger et al., 2012) [33] | Australia | 2008 | NR | ICU | 36 | 28 | 40.3 | NR | Both * | NR | NR | NR | NR | 5 |
| 11 | Minet (2012) | (Minet et al., 2012) [34] | France | 2009–2011 | consecutive | ICU | 176 | 109 | NR | NR | Pharmacological prophylaxis | NR | 16 | NR | NR | 6 |
| 12 | Adimi Naghan (2013) | (Adimi Naghan et al., 2013) [35] | Iran | 2006–2008 | consecutive | MICU | 243 | 141 | NR | NR | Pharmacological prophylaxis | NR | NR | NR | NR | 5 |
| 13 | Malinoski (2013) | (Malinoski et al., 2013) [36] | USA | 2008–2009 | NR | SICU | 411 | 296 | 48.0 | 28.1 | Both * | NR | 13 | 18 | 22.0 | 3 |
| 14 | Nickele (2013) | (Nickele et al., 2013) [37] | USA | 2009 | consecutive | NICU | 87 | 64 | 54.1 | NR | Both * | NR | NR | NR | NR | 4 |
| 15 | Patel (2013) | (Patel et al., 2013) [38] | USA | 2008–2009 | NR | SICU | 204 | 116 | 59.0 | 27.0 | Both * | NR | 54 | NR | NR | 3 |
| 16 | Camous (2014) | (Camous et al., 2014) [39] | France | 2003–2009 | consecutive | MICU | 55 | 14 | NR | NR | NR | NR | NR | NR | NR | 4 |
| 17 | Valle (2014) | (Valle et al., 2014) [40] | USA | 2011–2013 | NR | ICU | 148 | 115 | 47.0 | NR | Both * | NR | 3 | 8 | 27.0 | 4 |
| 18 | Okumus (2015) | (Okumus et al., 2015) [41] | Turkey | 2009–2010 | consecutive | ICU | 74 | 40 | 55.8 | NR | Both * | NR | 19 | NR | NR | 4 |
| 19 | Obi (2015) | (Obi et al., 2015) [42] | USA | 2007–2012 | consecutive | SICU | 4844 | NR | NR | NR | Pharmacological prophylaxis | NR | 1947 | 0 | NR | 5 |
| 20 | Mucino-Bermejo (2015) | (Muciño-Bermejo et al., 2015) [43] | Mexico | 2007–2012 | NR | ICU | 66 | 33 | 61.1 | NR | NR | NR | 5 | NR | NR | 3 |
| 21 | Allen (2016) | (Allen et al., 2016) [44] | USA | 2011–2014 | NR | TICU | 402 | 300 | 47.0 | NR | Both * | NR | 12 | 14 | 28.0 | 3 |
| 22 | Akaraborworn (2016) | (Akaraborworn et al., 2016) [6] | Thailand | 2011–2013 | NR | SICU | 4652 | 2728 | NR | NR | Both * | NR | NR | NR | NR | 4 |
| 23 | Hamada (2017) | (Hamada et al., 2017) [45] | France | 2015–2016 | consecutive | SICU | 153 | 110 | 44.6 | 26.1 | Both * | 34.9 | 6 | 22 | 23.7 | 4 |
| 24 | Karcutskies (2017) | (Karcutskies et al., 2017) [46] | USA | 2011–2015 | NR | ICU | 1137 | NR | 43.6 | NR | Both * | NR | 17 | 28 | 20.9 | 5 |
| 25 | Karcutskie (2017) | (Karcutskie et al., 2017) [47] | USA | 2015–2017 | NR | ICU | 194 | 156 | 38.7 | NR | Pharmacological prophylaxis | NR | 11 | 23 | 23.0 | 5 |
| 26 | Yumoto (2017) | (Yumoto et al., 2017) [48] | Japan | 2013–2016 | consecutive | EICU | 204 | 144 | NR | NR | Pharmacological prophylaxis | NR | NR | 12 | NR | 4 |
| 27 | Fu (2018) | (Fu et al., 2018) [49] | China | 2016–2017 | NR | ICU | 151 | 100 | NR | NR | NR | NR | 20 | NR | NR | 5 |
| 28 | Wilsey (2019) | (Wilsey et al., 2019) [50] | USA | 2013–2017 | NR | CICU | 1085 | NR | NR | NR | Pharmacological prophylaxis | NR | NR | NR | NR | 4 |
| 29 | Brendan Cloney (2019) | (Brendan Cloney et al., 2019) [51] | USA | 2009–2015 | consecutive | ICU | 1269 | 645 | 58.9 | NR | Both * | NR | NR | NR | NR | 4 |
| 30 | Beitland (2019) | (Beitland et al., 2019) [52] | Norway | 2012–2016 | consecutive | ICU | 70 | 55 | 62.0 | NR | Both * | 40.4 | 11 | NR | NR | 5 |
| 31 | Harahsheh (2019) | (Harahsheh et al., 2019) [53] | Australia | 2015–2017 | NR | ICU | 215 | 131 | NR | NR | Both * | NR | NR | NR | NR | 4 |
| 32 | Tachino (2019) | (Tachino et al., 2019) [54] | Japan | 2013–2016 | consecutive | ICU | 859 | 547 | 58.0 | NR | Both * | NR | 42 | 106 | NR | 6 |
| 33 | Brandi (2020) | (Brandi et al., 2020) [55] | Switzerland | 2012–2015 | consecutive | SICU | 177 | 130 | 50.1 | NR | physical prophylaxis | 46.0 | NR | NR | 23.5 | 4 |
| 34 | Gibson (2020) | (Gibson et al., 2020) [56] | USA | 2014–2015 | consecutive | MICU | 243 | 140 | 64.3 | 29.8 | Both * | NR | 37 | NR | NR | 3 |
| 35 | Dhillon (2021) | (Dhillon et al., 2021) [57] | USA | 2013–2015 | NR | ICU | 131 | 92 | 55.6 | NR | Pharmacological prophylaxis | NR | NR | NR | 30.6 | 5 |
| 36 | Chu (2021) | (Chu et al., 2021) [58] | USA | 2001–2012 | NR | ICU | 848 | 474 | NR | NR | NR | NR | 123 | NR | NR | 5 |
| 37 | Ow (2021) | (Ow et al., 2021) [59] | Britain | 2009–2016 | consecutive | LICU | 623 | 383 | NR | NR | Pharmacological prophylaxis | NR | 77 | NR | NR | 4 |
| 38 | Phan (2022) | (Phan et al., 2022) [60] | USA | 2014–2018 | NR | NICU | 266 | 106 | 57.0 | 30.0 | NR | NR | NR | NR | NR | 4 |
| 39 | Mei (2022) | (Mei et al., 2022) [61] | China | 2011–2022 | NR | ICU | 560 | 365 | NR | 23.9 | Both * | NR | NR | NR | NR | 4 |
| 40 | Dibiasi (2022) | (Dibiasi et al., 2022) [62] | Austria | 2015–2018 | NR | ICU | 1352 | 838 | NR | NR | NR | NR | NR | NR | NR | 4 |
| 41 | Barton (2022) | (Barton et al., 2022) [63] | USA | 2017–2019 | NR | ICU | 91 | 55 | NR | NR | Pharmacological prophylaxis | NR | NR | NR | NR | 5 |
| 42 | Abdel (2022) | (Abdel et al., 2022) [64] | Saudi Arabia | 2016–2019 | NR | ICU | 322 | 306 | 31.3 | 23.9 | Pharmacological prophylaxis | NR | NR | NR | 28.9 | 5 |
| Subgroups | Categories (No. of Studies) | Prevalence (%) | 95% CI (%) | Sample Size | Events | I2 (%) | p Value within Subgroup | Q (p Value across Subgroups) |
|---|---|---|---|---|---|---|---|---|
| Year of survey | 1971–2013 (22) | 9.1 | 5.3–15.2 | 17,394 | 1122 | 98.34 | <0.001 | 0.472 (0.492) |
| 2014–2022 (20) | 11.6 | 7.2–18.4 | 9950 | 1096 | 98.25 | <0.001 | ||
| Country | Asia region (8) | 9.5 | 2.8–27.7 | 7065 | 534 | 99.14 | 0.001 | 1.958 (0.58) |
| European (7) | 14.4 | 6.9–27.6 | 1596 | 192 | 95.95 | <0.001 | ||
| North America (24) | 10.3 | 7.0–15.0 | 17,080 | 1451 | 95.95 | <0.001 | ||
| Oceania (3) | 5.0 | 1.2–18.2 | 1603 | 41 | 97.83 | <0.001 | ||
| Obesity (%) | >26.8 (4) | 17.8 | 8.3–34.0 | 5341 | 475 | 97.40 | 0.001 | 1.41 (0.24) |
| ≤26.8 (5) | 9.7 | 4.8–18.6 | 2745 | 237 | 96.24 | <0.001 | ||
| Abnormal coagulation (%) | >39.18 (4) | 16.5 | 9.4–27.3 | 1793 | 216 | 94.15 | <0.001 | 1.00 (0.32) |
| ≤39.18 (4) | 9.2 | 3.1–24.0 | 2077 | 166 | 97.65 | <0.001 | ||
| Lower extremity fracture (%) | >23.04 (4) | 22.4 | 13.7–34.4 | 809 | 159 | 91.05 | <0.001 | 4.02 (0.05) |
| ≤23.04 (5) | 9.0 | 4.0–18.9 | 2805 | 239 | 97.09 | <0.001 | ||
| Pelvic fracture (%) | >20.10 (4) | 16.0 | 8.8–27.3 | 850 | 126 | 91.38 | <0.001 | 0.28 (0.60) |
| ≤20.10 (5) | 12.2 | 5.2–26.0 | 2764 | 272 | 97.82 | <0.001 | ||
| Operations (%) | >28.74 (4) | 23.9 | 15.5–34.9 | 646 | 148 | 86.89 | <0.001 | 1.66 (0.20) |
| ≤28.74 (4) | 14.2 | 6.9–27.1 | 580 | 112 | 90.19 | <0.001 | ||
| CVC (%) | >54.29 (4) | 19.7 | 11.0–32.8 | 458 | 114 | 85.31 | <0.001 | 0.23 (0.63) |
| ≤54.29 (5) | 16.3 | 9.3–27.1 | 5665 | 502 | 95.96 | <0.001 | ||
| ICU LOS | <8 (4) | 7.6 | 5.7–10.1 | 6502 | 514 | 79.68 | <0.001 | 0.06 (0.81) |
| ≥8 (5) | 6.9 | 3.1–14.6 | 4486 | 185 | 96.18 | <0.001 | ||
| Thromboprophylaxis strategy | Both * (20) | 13.4 | 7.6–22.7 | 12,583 | 1311 | 98.8 | <0.001 | 32.21 (<0.001) |
| Pharmacological prophylaxis (12) | 9.3 | 6.0–14.1 | 3401 | 267 | 91.34 | <0.001 | ||
| Mechanical prophylaxis (1) | 31.9 | 25.8–38.6 | 204 | 65 | 0.00 | <0.001 | ||
| SAPS | >40.4 (1) | 13.0 | 8.8–18.8 | 177 | 23 | 0.00 | <0.001 | 15.01 (<0.001) |
| ≤40.4 (2) | 29.6 | 24.0–36.0 | 223 | 66 | 0.00 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, X.; Zeng, L.; Wang, H.; Zeng, S.; Tian, J.; Chen, L.; Peng, T. Prevalence of Venous Thromboembolism in Intensive Care Units: A Meta-Analysis. J. Clin. Med. 2022, 11, 6691. https://doi.org/10.3390/jcm11226691
Gao X, Zeng L, Wang H, Zeng S, Tian J, Chen L, Peng T. Prevalence of Venous Thromboembolism in Intensive Care Units: A Meta-Analysis. Journal of Clinical Medicine. 2022; 11(22):6691. https://doi.org/10.3390/jcm11226691
Chicago/Turabian StyleGao, Xiaoyu, Liangnan Zeng, Haorun Wang, Shan Zeng, Junjie Tian, Ligang Chen, and Tangming Peng. 2022. "Prevalence of Venous Thromboembolism in Intensive Care Units: A Meta-Analysis" Journal of Clinical Medicine 11, no. 22: 6691. https://doi.org/10.3390/jcm11226691