
Bacterial Aspiration Pneumonia in Generalized Convulsive Status Epilepticus: Incidence, Associated Factors and Outcome

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Definitions
2.4.1. Aspiration Syndrome
2.4.2. Bacterial Aspiration Pneumonia, Pneumonitis, and Ventilator-Associated Pneumonia
- Bacterial aspiration pneumonia in the case of microbiological confirmation, with the isolation in the endotracheal aspirate of at least 105 colony-forming units per mL.
- Pneumonitis, when endotracheal aspirate culture was sterile.
2.4.3. Measurements of Serum Levels of C-Reactive Protein (CRP), Procalcitonin (PCT), and Albumin during First 24 h after Admission
2.5. Outcomes
2.6. Statistical Analysis
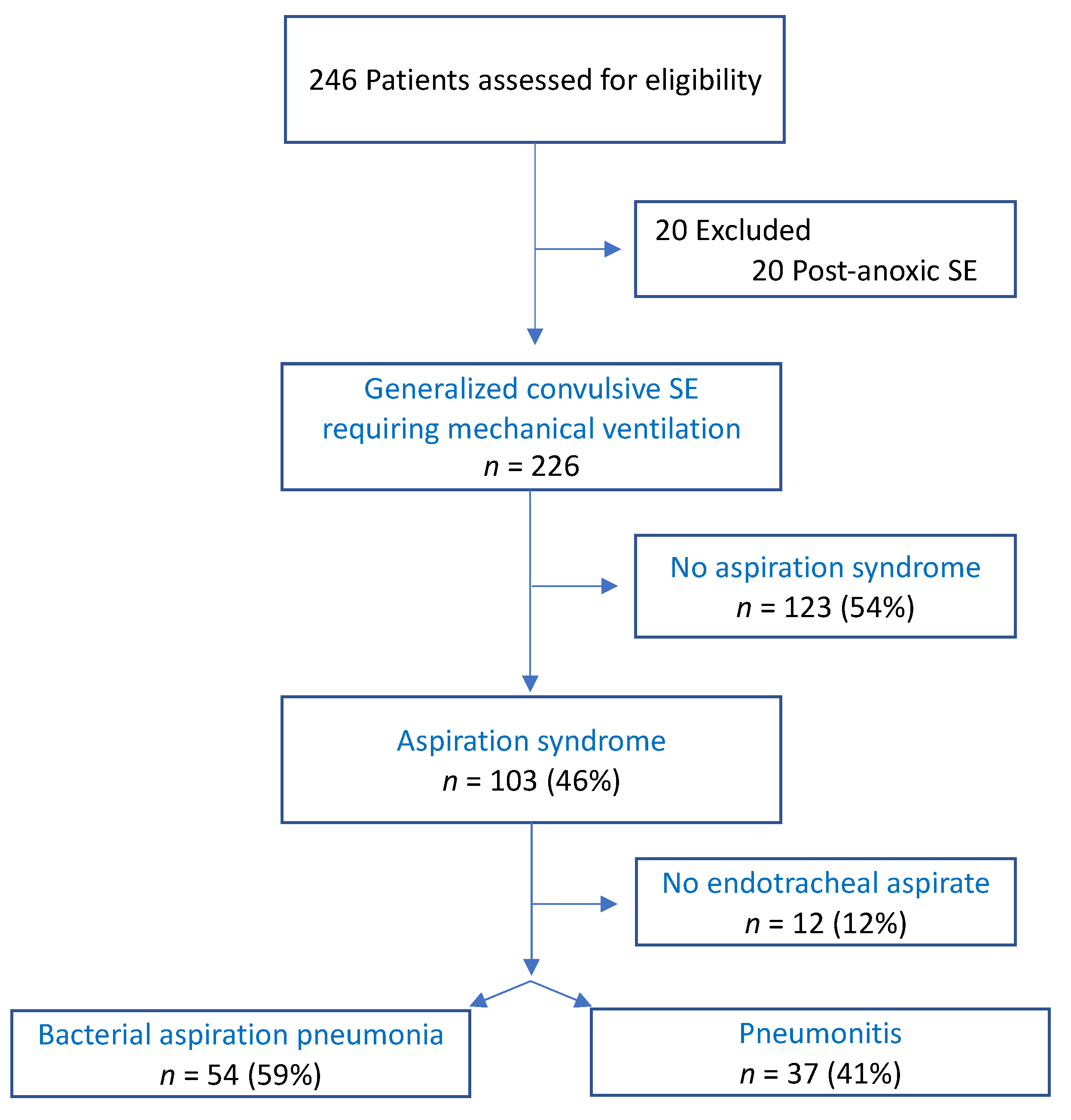
3. Results
3.1. Patient Characteristics
3.2. Comparison of Patients with and without Aspiration Syndrome
3.3. Comparison of Patients with BAP Versus Pneumonitis
3.4. Etiology of Bacterial Aspiration Pneumonia
3.5. Antibiotic Therapy
3.6. Outcomes of BAP Versus Pneumonitis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Betjemann, J.P.; Lowenstein, D.H. Status Epilepticus in Adults. Lancet Neurol. 2015, 14, 615–624. [Google Scholar] [CrossRef]
- Trinka, E.; Cock, H. A Definition and Classification of Status Epilepticus—Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia 2015, 56, 1515–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, J.; Elm, J. Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus. N. Engl. J. Med. 2019, 381, 2103–2113. [Google Scholar] [CrossRef] [PubMed]
- Sutter, R.; Dittrich, T. Acute Systemic Complications of Convulsive Status Epilepticus-A Systematic Review. Crit. Care Med. 2018, 46, 138–145. [Google Scholar] [CrossRef]
- Semmlack, S.; Tschudin-Sutter, S. Independent Impact of Infections on the Course and Outcome of Status Epilepticus: A 10-Year Cohort Study. J. Neurol. 2016, 263, 1303–1313. [Google Scholar] [CrossRef]
- DiBardino, D.M.; Wunderink, R.G. Aspiration Pneumonia: A Review of Modern Trends. J. Crit. Care 2015, 30, 40–48. [Google Scholar] [CrossRef]
- Lascarrou, J.B.; Lissonde, F. Antibiotic Therapy in Comatose Mechanically Ventilated Patients Following Aspiration: Differentiating Pneumonia from Pneumonitis. Crit. Care Med. 2017, 45, 1268–1275. [Google Scholar] [CrossRef]
- Ruijter, B.J.; Keijzer, H.M. Treating Rhythmic and Periodic EEG Patterns in Comatose Survivors of Cardiac Arrest. N. Engl. J. Med. 2022, 386, 724–734. [Google Scholar] [CrossRef]
- Le Gall, J.-R.; Lemeshow, S. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957. [Google Scholar] [CrossRef]
- Rossetti, A.O.; Lowenstein, D.H. Management of Refractory Status Epilepticus in Adults: Still More Questions than Answers. Lancet Neurol. 2011, 10, 922–930. [Google Scholar] [CrossRef]
- Mezouar, N.; Demeret, S. Psychogenic Non-Epileptic Seizure-Status in Patients Admitted to the Intensive Care Unit. Eur. J. Neurol. 2021, 28, 2775–2779. [Google Scholar] [CrossRef] [PubMed]
- Van Swieten, J.C.; Koudstaal, P.J. Interobserver Agreement for the Assessment of Handicap in Stroke Patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019.
- Neill, S.; Dean, N. Aspiration Pneumonia and Pneumonitis: A Spectrum of Infectious/Noninfectious Diseases Affecting the Lung. Curr. Opin. Infect. Dis. 2019, 32, 152–157. [Google Scholar] [CrossRef]
- Legriel, S.; Grigoresco, B. Diagnostic Accuracy of Procalcitonin for Early Aspiration Pneumonia in Critically Ill Patients with Coma: A Prospective Study. Neurocrit. Care 2019, 30, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Herzig, S.J.; Howell, M.D. Acid-Suppressive Medication Use and the Risk for Hospital-Acquired Pneumonia. JAMA 2009, 301, 2120–2128. [Google Scholar] [CrossRef] [Green Version]
- Becker, K.L.; Snider, R. Procalcitonin in Sepsis and Systemic Inflammation: A Harmful Biomarker and a Therapeutic Target. Br. J. Pharmacol. 2010, 159, 253–264. [Google Scholar] [CrossRef] [PubMed]
- De Kruif, M.D.; Limper, M. Additional Value of Procalcitonin for Diagnosis of Infection in Patients with Fever at the Emergency Department. Crit. Care Med. 2010, 38, 457–463. [Google Scholar] [CrossRef]
- El-Solh, A.A.; Vora, H. Diagnostic Use of Serum Procalcitonin Levels in Pulmonary Aspiration Syndromes. Crit. Care Med. 2011, 39, 1251–1256. [Google Scholar] [CrossRef]
- Sutter, R.; Valença, M. Procalcitonin and Mortality in Status Epilepticus: An Observational Cohort Study. Crit. Care 2015, 19, 361. [Google Scholar] [CrossRef] [Green Version]
- Sutter, R.; Grize, L. Acute-Phase Proteins and Mortality in Status Epilepticus: A 5-Year Observational Cohort Study. Crit. Care Med. 2013, 41, 1526–1533. [Google Scholar] [CrossRef]
- Engel, H.; ben Hamouda, N. Serum Procalcitonin as a Marker of Post-Cardiac Arrest Syndrome and Long-Term Neurological Recovery, but Not of Early-Onset Infections, in Comatose Post-Anoxic Patients Treated with Therapeutic Hypothermia. Resuscitation 2013, 84, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Deng, W.-J.; Shen, R.-L. Relationship between Procalcitonin Serum Levels and Functional Outcome in Stroke Patients. Cell Mol. Neurobiol. 2015, 35, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Bretonnière, C.; Leone, M. Strategies to Reduce Curative Antibiotic Therapy in Intensive Care Units (Adult and Paediatric). Intensive Care Med. 2015, 41, 1181–1196. [Google Scholar] [CrossRef] [PubMed]
- Clavel, M.; Barraud, O. Molecular Quantification of Bacteria from Respiratory Samples in Patients with Suspected Ventilator-Associated Pneumonia. Clin. Microbiol. Infect. 2016, 22, 812.e1–812.e7. [Google Scholar] [CrossRef] [Green Version]
- Tortuyaux, R.; Voisin, B. Could Polymerase Chain Reaction-Based Methods Differentiate Pneumonitis from Bacterial Aspiration Pneumonia? Crit. Care Med. 2018, 46, e96–e97. [Google Scholar] [CrossRef]
- Dragan, V.; Wei, Y. Prophylactic Antimicrobial Therapy for Acute Aspiration Pneumonitis. Clin. Infect. Dis. 2018, 67, 513–518. [Google Scholar] [CrossRef]
- Sutter, R.; Rüegg, S. Seizures as Adverse Events of Antibiotic Drugs: A Systematic Review. Neurology 2015, 85, 1332–1341. [Google Scholar] [CrossRef]
- Lauterbach, E.; Voss, F. Bacteriology of Aspiration Pneumonia in Patients with Acute Coma. Intern. Emerg. Med. 2014, 9, 879–885. [Google Scholar] [CrossRef]
- Rebuck, J.A.; Rasmussen, J.R. Clinical Aspiration-Related Practice Patterns in the Intensive Care Unit: A Physician Survey. Crit. Care Med. 2001, 29, 2239–2244. [Google Scholar] [CrossRef]
- Torres, A.; Niederman, M.S. International ERS/ESICM/ESCMID/ALAT Guidelines for the Management of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia. Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef] [Green Version]
- Premachandra, A.; Mazeraud, A. Is Amoxicillin/Clavulanic Acid the Best Option to Treat Early-Onset Ventilator-Acquired Pneumonia in Brain-Injured Patients. J. Glob Antimicrob. Resist. 2021, 27, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Mandell, L.A.; Niederman, M.S. Aspiration Pneumonia. N. Engl. J. Med. 2019, 380, 651–663. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Overall Cohort (n = 226) | Aspiration Syndrome (n = 103) | No Aspiration Syndrome (n = 123) | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Age (years), median (IQR) | 55 (43–68) | 56 (43–68) | 55 (39–67) | 0.395 |
| Male sex, n (%) | 146 (65) | 66 (64) | 80 (65) | 0.880 |
| mRS score 0–1, n (%) | 132 (58) | 53 (51) | 79 (64) | 0.052 |
| SAPS II (without age), median (IQR) | 46 (36–54) | 50 (34–58) | 45 (37–50) | 0.113 |
| Medical history, n (%) | ||||
| History of epilepsy | 109 (48) | 50 (49) | 59 (48) | 0.931 |
| Previous status epilepticus | 40 (18) | 14 (14) | 26 (21) | 0.139 |
| Alcohol | 83 (37) | 43 (42) | 40 (33) | 0.152 |
| Status epilepticus characteristics, n (%) | ||||
| Continuous seizure | 72 (32) | 32 (31) | 40 (33) | 0.815 |
| Refractory status epilepticus | 55 (24) | 22 (21) | 33 (27) | 0.340 |
| Intubation before ICU admission | 128 (57) | 56 (54) | 72 (59) | 0.529 |
| Intubation for respiration failure | 130 (58) | 57 (55) | 73 (59) | 0.544 |
| Clinical characteristics at admission | ||||
| Core temperature (°C), median (IQR) | 36.9 (36.2–37.4) | 36.9 (36.2–37.4) | 36.8 (36.3–37.4) | 0.897 |
| Heart rate (bpm), median (IQR) | 97 (80–119) | 102 (85–125) | 95 (78–112) | 0.011 |
| Persistent seizures, n (%) | 43 (19) | 29 (28) | 14 (11) | 0.001 |
| History of macroaspiration, n (%) | 23 (10) | 12 (12) | 11 (9) | 0.503 |
| Biological characteristics at admission, median (IQR) | ||||
| Leukocyte count (109/L) | 11.62 (8.88–15.63) | 12.12 (9.55–15.67) | 11.10 (8.47–15.20) | 0.538 |
| Serum CRP level (mg/L) | 10 (0–27) | 15 (4–36) | 6 (0–18) | 0.002 |
| Serum PCT level (ng/mL) | 0.15 (0.00–0.54) | 0.18 (0.00–0.91) | 0.10 (0.00–0.30) | 0.134 |
| Serum albumin level (g/L) | 36 (32–40) | 35 (31–38) | 36 (32–40) | 0.030 |
| PaO2/FiO2 (mmHg) | 286 (200–390) | 265 (179–335) | 313 (223–410) | <0.001 |
| Arterial lactate level (mmol/L) | 2.1 (1.2–4.0) | 2.0 (1.1–3.6) | 2.2 (1.3–4.2) | 0.569 |
| Etiologic categories, n (%) | ||||
| Acute symptomatic | 71 (31) | 33 (32) | 38 (31) | 0.853 |
| Remote symptomatic | 104 (46) | 46 (45) | 58 (47) | 0.708 |
| Progressive symptomatic | 31 (14) | 13 (13) | 18 (15) | 0.661 |
| Unknown | 14 (6) | 10 (10) | 4 (3) | 0.045 |
| PNES | 6 (3) | 1 (1) | 5 (4) | 0.224 * |
| Main etiologies, n (%) | ||||
| Vascular | 26 (11) | 10 (10) | 16 (13) | 0.439 |
| Toxic | 34 (15) | 20 (19) | 14 (11) | 0.092 |
| Brain tumor | 25 (11) | 14 (14) | 11 (9) | 0.267 |
| Outcomes | ||||
| Ventilator-associated pneumonia, n (%) | 35 (15) | 15 (15) | 20 (16) | 0.725 |
| Mechanical ventilation duration (days), median (IQR) | 1.90 (0.88–4.87) | 2.71 (1.50–7.10) | 1.50 (0.60–3.65) | 0.002 |
| ICU stay length (days), median (IQR) | 4.94 (2.71–9.69) | 6.04 (4.23–12.93) | 3.90 (2.11–6.92) | 0.011 |
| ICU mortality, n (%) | 11 (5) | 7 (7) | 4 (3) | 0.217 |
| Three-month poor functional outcome, n (%) | 78 (35) | 38 (38) | 40 (33) | 0.363 |
| Three-month mortality, n (%) | 25 (11) | 13 (13) | 12 (10) | 0.429 |
| Characteristics | BAP (n = 54) | Pneumonitis (n = 37) | p-Value |
|---|---|---|---|
| Demographics | |||
| Age (years), median (IQR) | 55 (42–67) | 65 (48–71) | 0.126 |
| Male sex, n (%) | 37 (69) | 25 (68) | 0.924 |
| mRS score 0–1, n (%) | 26 (48) | 21 (57) | 0.420 |
| SAPS II (without age), median (IQR) | 51 (38–58) | 44 (28–58) | 0.035 |
| Medical history, n (%) | |||
| History of epilepsy | 25 (46) | 18 (49) | 0.825 |
| Previous status epilepticus | 4 (7) | 9 (24) | 0.023 |
| Alcohol | 17 (31) | 21 (57) | 0.016 |
| Use of proton pump inhibitor | 19 (35) | 13 (35) | 0.996 |
| Status epilepticus characteristics, n (%) | |||
| Continuous seizure | 17 (31) | 11 (30) | 0.859 |
| Refractory status epilepticus | 11 (20) | 9 (24) | 0.655 |
| Intubation before ICU admission | 29 (54) | 21 (57) | 0.774 |
| Intubation for respiration failure | 34 (63) | 17 (46) | 0.108 |
| Clinical characteristics at admission | |||
| Core temperature (°C), median (IQR) | 36.8 (36.1–37.1) | 37.0 (36.3–37.8) | 0.095 |
| Heart rate (bpm), median (IQR) | 96 (81–120) | 111 (90–124) | 0.191 |
| Persistent seizures, n (%) | 15 (28) | 10 (27) | 0.937 |
| History of macroaspiration, n (%) | 4 (7) | 6 (16) | 0.306 * |
| Biological characteristics at admission, median (IQR) | |||
| Leukocyte count (109/L) | 12.28 (9.58–15.31) | 11.88 (9.53–15.68) | 0.792 |
| Serum CRP level (mg/L) | 12 (2–36) | 13 (0–31) | 0.777 |
| Serum PCT level (ng/mL) | 0.17 (0.00–0.63) | 0.14 (0.00–0.53) | 0.869 |
| Serum albumin level (g/L) | 35 (32–39) | 35 (31–37) | 0.411 |
| PaO2/FiO2 (mmHg) | 281 (185–391) | 263 (192–314) | 0.344 |
| Arterial lactate level (mmol/L) | 1.85 (1.00–3.17) | 2.40 (1.42–4.92) | 0.306 |
| Etiologic categories, n (%) | |||
| Acute symptomatic | 15 (28) | 13 (35) | 0.455 |
| Remote symptomatic | 24 (44) | 16 (43) | 0.910 |
| Progressive symptomatic | 8 (15) | 4 (11) | 0.755 * |
| Unknown | 6 (11) | 4 (11) | 0.964 * |
| Main etiologies, n (%) | |||
| Vascular | 5 (9) | 2 (5) | 0.696 * |
| Toxic | 9 (17) | 9 (24) | 0.368 |
| Brain tumor | 8 (15) | 5 (14) | 0.862 |
| Type of Bacteria | Bacteria | Number of Isolates, n (%) | Resistance |
|---|---|---|---|
| Gram + (30 bacteria isolated from 29 patients, 54 %) | |||
| Staphylococcus spp. | Staphylococcus aureus | 18 (33) | Methicillin-sensitive: 16 (penicillin-resistant: 8, tested in 10 isolates) Methicillin-resistant: 2 * |
| Streptococcus spp. | Streptococcus pneumoniae | 10 (19) | Wild-type: 6 Decreased susceptibility to penicillin: 4 |
| Streptococcus agalactiae | 2 (4) | Wild-type: 2 | |
| Gram − (41 bacteria isolated from 36 patients, 67 %) | |||
| Group 1, 2, and 5 enterobacterales | Klebsiella pneumoniae | 9 (17) | Wild-type: 6 β-Lactamase: 1 * ESBL: 2 * |
| Escherichia coli | 7 (13) | Wild-type: 3 Low-production of β-lactamase: 1 Hyperproduction of β-lactamase: 3 * | |
| Klebsiella oxytoca | 1 (2) | Wild-type: 1 | |
| Proteus vulgaris | 1 (2) | Wild-type: 1 | |
| Group 3 enterobacterales | Enterobacter cloacae | 2 (4) | Wild-type: 1 * ESBL: 1 * |
| Hafnia alvei | 1 (2) | Wild-type: 1 * | |
| Non-fermenting bacilli | Pseudomonas aeruginosa | 2 (4) | Wild-type: 2 * |
| Acinetobacter baumannii | 1 (2) | Wild-type: 1 * | |
| Other bacteria | Haemophilus influenzae | 13 (24) | Wild-type: 12 β-Lactamase: 1 |
| Moraxella catarrhalis | 2 (4) | β-Lactamase: 1 Wild-type: 1 | |
| Lelliottia amnigena | 1 (2) | ACA-resistant: 1 * | |
| Pasteurella multocida | 1 (2) | Wild-type: 1 | |
| Characteristics | BAP (n = 54) | Pneumonitis (n = 37) | p-Value |
|---|---|---|---|
| Ventilator-associated pneumonia, n (%) | 10 (19) | 4 (11) | 0.317 |
| Mechanical ventilation duration (days), median (IQR) | 3.39 (1.71–8.35) | 2.37 (0.83–6.88) | 0.179 |
| ICU stay length (days), median (IQR) | 6.83 (4.38–13.25) | 6.46 (3.58–12.50) | 0.180 |
| ICU mortality, n (%) | 6 (11) | 1 (3) | 0.234 * |
| Three-month poor functional outcome, n (%) | 24 (44) | 10 (27) | 0.057 |
| Three-month mortality, n (%) | 9 (17) | 3 (8) | 0.198 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tortuyaux, R.; Wallet, F.; Derambure, P.; Nseir, S. Bacterial Aspiration Pneumonia in Generalized Convulsive Status Epilepticus: Incidence, Associated Factors and Outcome. J. Clin. Med. 2022, 11, 6673. https://doi.org/10.3390/jcm11226673
Tortuyaux R, Wallet F, Derambure P, Nseir S. Bacterial Aspiration Pneumonia in Generalized Convulsive Status Epilepticus: Incidence, Associated Factors and Outcome. Journal of Clinical Medicine. 2022; 11(22):6673. https://doi.org/10.3390/jcm11226673
Chicago/Turabian StyleTortuyaux, Romain, Frédéric Wallet, Philippe Derambure, and Saad Nseir. 2022. "Bacterial Aspiration Pneumonia in Generalized Convulsive Status Epilepticus: Incidence, Associated Factors and Outcome" Journal of Clinical Medicine 11, no. 22: 6673. https://doi.org/10.3390/jcm11226673