


Significance of Temporal Muscle Thickness in Chronic Subdural Hematoma
 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
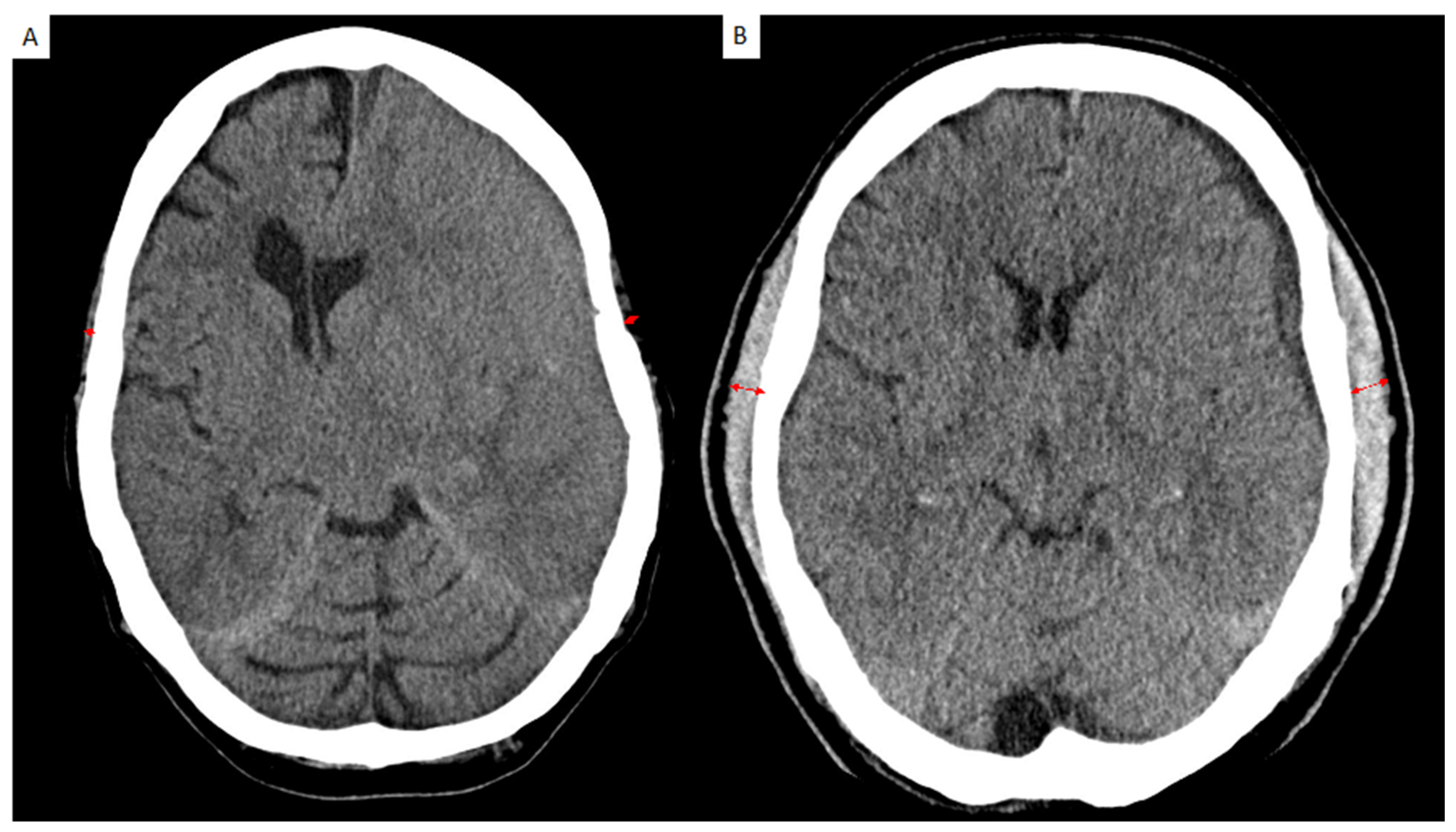
2.2. Image Analysis
2.3. Surgical Treatment
2.4. Study Design
2.5. Statistics
3. Results
3.1. Participant Characteristics
3.2. Characteristics and Admission Status in CSDH According to Temporal Muscle Thickness
3.3. Preexisting Conditions and Temporal Muscle Thickness in Patients with CSDH
3.4. Symptoms at Admission and Temporal Muscle Thickness in Patients with CSDH
3.5. Association of Radiological Parameters and TMT in Patients with CSDH
3.6. Postoperative Seizures and Temporal Muscle Thickness in Patients with CSDH
3.7. Clinical Outcome and Temporal Muscle Thickness in Patients with CSDH
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bounajem, M.T.; Campbell, R.A.; Denorme, F.; Grandhi, R. Paradigms in chronic subdural hematoma pathophysiology: Current treatments and new directions. J. Trauma Acute Care Surg. 2021, 91, e134–e141. [Google Scholar] [CrossRef] [PubMed]
- Feghali, J.; Yang, W.; Huang, J. Updates in Chronic Subdural Hematoma: Epidemiology, Etiology, Pathogenesis, Treatment, and Outcome. World Neurosurg. 2020, 141, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Won, S.Y.; Dubinski, D.; Eibach, M.; Gessler, F.; Herrmann, E.; Keil, F.; Seifert, V.; Konczalla, J.; Behmanesh, B. External validation and modification of the Oslo grading system for prediction of postoperative recurrence of chronic subdural hematoma. Neurosurg. Rev. 2021, 44, 961–970. [Google Scholar] [CrossRef]
- Strasser, E.M.; Draskovits, T.; Praschak, M.; Quittan, M.; Graf, A. Association between ultrasound measurements of muscle thickness, pennation angle, echogenicity and skeletal muscle strength in the elderly. Age 2013, 35, 2377–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef] [PubMed]
- Furtner, J.; Genbrugge, E.; Gorlia, T.; Bendszus, M.; Nowosielski, M.; Golfinopoulos, V.; Weller, M.; Van Den Bent, M.J.; Wick, W.; Preusser, M. Temporal muscle thickness is an independent prognostic marker in patients with progressive glioblastoma: Translational imaging analysis of the EORTC 26101 trial. Neuro-Oncol. 2019, 21, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Furtner, J.; Weller, M.; Weber, M.; Gorlia, T.; Nabors, B.; Reardon, D.A.; Tonn, J.C.; Stupp, R.; Preusser, M. Temporal Muscle Thickness as a Prognostic Marker in Patients with Newly Diagnosed Glioblastoma: Translational Imaging Analysis of the CENTRIC EORTC 26071-22072 and CORE Trials. Clin. Cancer Res. 2022, 28, 129–136. [Google Scholar] [CrossRef]
- Yan, O.Y.; Teng, H.B.; Fu, S.N.; Chen, Y.Z.; Liu, F. Temporal Muscle Thickness is an Independent Prognostic Biomarker in Patients with Glioma: Analysis of 261 Cases. Cancer Manag. Res. 2021, 13, 6621. [Google Scholar] [CrossRef]
- Dodds, R.; Sayer, A.A. Sarcopenia and frailty: New challenges for clinical practice. Clin. Med. 2016, 16, 455. [Google Scholar] [CrossRef]
- Hernández-Durán, S.; Behme, D.; Rohde, V.; von der Brelie, C. A matter of frailty: The modified Subdural Hematoma in the Elderly (mSHE) score. Neurosurg. Rev. 2022, 45, 701. [Google Scholar] [CrossRef] [PubMed]
- Furtner, J.; Berghoff, A.S.; Schöpf, V.; Reumann, R.; Pascher, B.; Woitek, R.; Asenbaum, U.; Pelster, S.; Leitner, J.; Widhalm, G.; et al. Temporal muscle thickness is an independent prognostic marker in melanoma patients with newly diagnosed brain metastases. J. Neurooncol. 2018, 140, 173–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanabe, C.; Reed, M.J.; Pham, T.N.; Penn, K.; Bentov, I.; Kaplan, S.J. Association of Brain Atrophy and Masseter Sarcopenia With 1-Year Mortality in Older Trauma Patients. JAMA Surg. 2019, 154, 716. [Google Scholar] [CrossRef] [PubMed]
- Scerrati, A.; Pangallo, G.; Dughiero, M.; Mongardi, L.; Ricciardi, L.; Lofrese, G.; Dones, F.; Cavallo, M.A.; De Bonis, P. Influence of nutritional status on the clinical outcome of patients with chronic subdural hematoma: A prospective multicenter clinical study. Nutr. Neurosci. 2022, 25, 1756–1763. [Google Scholar] [CrossRef]
- Katsuki, M.; Suzuki, Y.; Kunitoki, K.; Sato, Y.; Sasaki, K.; Mashiyama, S.; Matsuoka, R.; Allen, E.; Saimaru, H.; Sugawara, R.; et al. Temporal Muscle as an Indicator of Sarcopenia is Independently Associated with Hunt and Kosnik Grade on Admission and the Modified Rankin Scale Score at 6 Months of Patients with Subarachnoid Hemorrhage Treated by Endovascular Coiling. World Neurosurg. 2020, 137, e526–e534. [Google Scholar] [CrossRef]
- Katsuki, M.; Kakizawa, Y.; Nishikawa, A.; Yamamoto, Y.; Uchiyama, T.; Agata, M.; Wada, N.; Kawamura, S.; Koh, A. Temporal Muscle and Stroke—A Narrative Review on Current Meaning and Clinical Applications of Temporal Muscle Thickness, Area, and Volume. Nutrients 2022, 14, 687. [Google Scholar] [CrossRef]
- Katsuki, M.; Kakizawa, Y.; Nishikawa, A.; Yamamoto, Y.; Uchiyama, T. Temporal muscle thickness and area are an independent prognostic factors in patients aged 75 or younger with aneurysmal subarachnoid hemorrhage treated by clipping. Surg. Neurol. Int. 2021, 12, 151. [Google Scholar] [CrossRef]
- Edlmann, E.; Giorgi-Coll, S.; Whitfield, P.C.; Carpenter, K.L.H.; Hutchinson, P.J. Pathophysiology of chronic subdural haematoma: Inflammation, angiogenesis and implications for pharmacotherapy. J. Neuroinflammation 2017, 14, 108. [Google Scholar] [CrossRef] [Green Version]
- Dalle, S.; Rossmeislova, L.; Koppo, K. The Role of Inflammation in Age-Related Sarcopenia. Front. Physiol. 2017, 8, 1045. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.; Park, M.; Moon, W.J.; Han, S.H.; Moon, Y. Sarcopenia in patients with dementia: Correlation of temporalis muscle thickness with appendicular muscle mass. Neurol. Sci. 2022, 43, 3089–3095. [Google Scholar] [CrossRef]
- Khandelwal, N.; Kross, E.K.; Engelberg, R.A.; Coe, N.B.; Long, A.C.; Curtis, J.R. Estimating the effect of palliative care interventions and advance care planning on ICU utilization: A systematic review. Crit. Care Med. 2015, 43, 1102–1111. [Google Scholar] [CrossRef] [PubMed]
- Katsuki, M.; Narita, N.; Sasaki, K.; Sato, Y.; Suzuki, Y.; Mashiyama, S.; Tominaga, T. Standard values for temporal muscle thickness in the Japanese population who undergo brain check-up by magnetic resonance imaging. Surg. Neurol. Int. 2021, 12, 67. [Google Scholar] [CrossRef] [PubMed]
- Kanat, A.; Kayaci, S.; Yazar, U.; Kazdal, H.; Terzi, Y. Chronic subdural hematoma in adults: Why does it occur more often in males than females? Influence of patient’s sexual gender on occurrence. J. Neurosurg. Sci. 2010, 54, 99–103. [Google Scholar]
- Dubinski, D.; Won, S.Y.; Behmanesh, B.; Brawanski, N.; Geisen, C.; Seifert, V.; Senft, C.; Konczalla, J. The clinical relevance of ABO blood type in 100 patients with acute subdural hematoma. PLoS ONE 2018, 13, e0204331. [Google Scholar] [CrossRef] [PubMed]
- Dubinski, D.; Won, S.Y.; Konczalla, J.; Mersmann, J.; Geisen, C.; Herrmann, E.; Seifert, V.; Senft, C. The Role of ABO Blood Group in Cerebral Vasospasm, Associated Intracranial Hemorrhage, and Delayed Cerebral Ischemia in 470 Patients with Subarachnoid Hemorrhage. World Neurosurg. 2017, 97, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Dubinski, D.; Won, S.Y.; Behmanesh, B.; Kashefiolasl, S.; Geisen, C.; Seifert, V.; Senft, C.; Konczalla, J. Influence of ABO blood type on the outcome after non-aneurysmal subarachnoid hemorrhage. Acta Neurochir. 2018, 160, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Nozoe, M.; Kubo, H.; Kanai, M.; Yamamoto, M.; Okakita, M.; Suzuki, H.; Shimada, S.; Mase, K. Reliability and validity of measuring temporal muscle thickness as the evaluation of sarcopenia risk and the relationship with functional outcome in older patients with acute stroke. Clin. Neurol. Neurosurg. 2021, 201, 106444. [Google Scholar] [CrossRef]
- Lee, B.; Bae, Y.J.; Jeong, W.J.; Kim, H.; Choi, B.S.; Kim, J.H. Temporalis muscle thickness as an indicator of sarcopenia predicts progression-free survival in head and neck squamous cell carcinoma. Sci. Rep. 2021, 11, 19717. [Google Scholar] [CrossRef]


{kind=link}
| Patient Characteristics | (n = 171) |
|---|---|
| Sex | |
| male, n (%) | 115 (67) |
| Age, median (IQR) | 74.5 (63–82) |
| GCS at admission, median (IQR) | 15 (14–15) |
| Anticoagulation, n (%) | 96 (56) |
| Preexisting conditions | |
| Hypertension, n (%) | 122 (71) |
| Atrial fibrillation, n (%) | 39 (23) |
| Diabetes mellitus, n (%) | 47 (27) |
| Coronary heart disease, n (%) | 77 (45) |
| Dementia, n (%) | 21 (12) |
| Symptoms at admission | |
| Headache, n (%) | 59 (35) |
| Confusion, n (%) | 35 (20) |
| Impaired consciousness, n (%) | 40 (23) |
| Nausea, n (%) | 16 (9) |
| Hemiparesis, n (%) | 119 (70) |
| Seizure, n (%) | 9 (5) |
| Radiological parameters | |
| Hematoma median, mm (IQR) | 18.4 (12–25) |
| Midline-shift, median, mm (IQR) | 6 (2–9) |
| Postoperative seizures | |
| Early seizure (<7 d), n (%) | 6 (4) |
| Late seizure (>7 d), n (%) | 4 (3) |
| Status epilepticus, n (%) | 1 (1) |
| Status at discharge | |
| GCS at discharge, median (IQR) | 15 (15–15) |
| mRS at discharge, median (IQR) | 2 (1–3) |
| Recurrence, n (%) | 56 (33) |
| Outcome | |
| mRS3 months, median (IQR) | 1.5 (0.5–3) |
| Patient Characteristics (n = 171) | Mean TMT | Univariate | |||
|---|---|---|---|---|---|
| Low Volume n = 91 | High Volume n = 80 | OR | 95% CI | p-Value | |
| Sex | |||||
| male, n (%) | 54 (59.3) | 61 (76.3) | 0.5 | 0.23–0.88 | 0.022 |
| Age, median (IQR) | 79 (71–84) | 70 (56–79) | - | 4.58–13.42 | 0.000 |
| GCS at admission, median (IQR) | 15 (14–15) | 15 (14–15) | - | −0.44–0.44 | 1 |
| Anticoagulation, n (%) | 57 (62.6) | 39 (48.8) | 1.8 | 0.96–3.25 | 0.089 |
| Preexisting conditions | |||||
| Hypertension, n (%) | 71 (78) | 51 (63.8) | 2 | 1.03–4.00 | 0.043 |
| Atrial fibrillation, n (%) | 21 (23.1) | 18 (22.5) | 1 | 0.51–2.12 | 1 |
| Diabetes mellitus, n (%) | 27 (29.7) | 20 (25.0) | 1.3 | 0.64–2.50 | 0.606 |
| Coronary heart disease, n (%) | 42 (46.2) | 35 (43.8) | 1.1 | 0.60–2.02 | 0.760 |
| Dementia, n (%) | 18 (19.8) | 3 (3.8) | 6.3 | 1.79–22.39 | 0.001 |
| Symptoms at admission | |||||
| Headache, n (%) | 24 (26.4) | 35 (43.8) | 0.5 | 0.24–0.88 | 0.023 |
| Confusion, n (%) | 33 (36.3) | 12 (15.0) | 3.2 | 1.53–6.81 | 0.001 |
| Impaired consciousness, n (%) | 20 (22.0) | 20 (25.0) | 0.9 | 0.42–1.72 | 0.718 |
| Nausea, n (%) | 3 (3.3) | 13 (16.3) | 0.2 | 0.10–0.64 | 0.004 |
| Hemiparesis, n (%) | 39 (42.9) | 40 (50.0) | 0.8 | 0.41–1.37 | 0.361 |
| Seizure, n (%) | 5 (5.5) | 4 (5.0) | 1.1 | 0.29–4.26 | 1 |
| Radiological parameters | |||||
| Hematoma median, mm (IQR) | 20 (13–25) | 17 (11–25) | 1.5 | 0.49–5.1 | 0.019 |
| Midline-shift, median, mm (IQR) | 6 (2–8) | 6 (2–11) | - | −1.44–1.44 | 1 |
| Postoperative seizures | |||||
| Early seizure (<7 d), n (%) | 2 (2.2) | 4 (5.0) | 0.4 | 0.08–40 | 0.420 |
| Late seizure (>7 d), n (%) | 3 (3.3) | 1 (1.3) | 2.7 | 0.27–26.43 | 0.623 |
| Status epilepticus, n (%) | 1 (1.1) | 0 (0) | - | - | 1 |
| Status at discharge | |||||
| GCS at discharge, median (IQR) | 15 (15–15) | 15 (15–15) | - | −0.13–0.13 | 1 |
| mRS at discharge, median (IQR) | 2 (1–3) | 1 (0.75–2) | - | 0.58–1.42 | 0.001 |
| Recurrence, n (%) | 27 (29.7) | 29 (36.3) | 0.7 | 0.39–1.41 | 0.415 |
| Outcome | |||||
| mRS3 months, median (IQR) | 2 (1–4) | 1 (0–2) | - | 0.36–1.63 | 0.002 |
| Patient Characteristics (n = 171) | Mean TMT | Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|---|---|
| 1–5 mm N = 91 | 6–9 mm N = 80 | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Sex | ||||||||
| Male, n (%) | 54 (59.3) | 61 (76.3) | 0.5 | 0.23–0.88 | 0.022 | 2.8 | 1.31–6.05 | 0.008 |
| Age, median (IQR) | 79 (71–84) | 70 (56–79) | - | 4.58–13.42 | 0.001 | |||
| Preexisting conditions | ||||||||
| Hypertension, n (%) | 71 (78.0) | 51 (63.8) | 2 | 1.03–4.00 | 0.043 | 0.5 | 0.25–1.14 | 0.102 |
| Dementia, n (%) | 18 (19.8) | 3 (3.8) | 6.3 | 1.79–22.39 | 0.001 | 0.3 | 0.07–1.0 | 0.050 |
| Symptoms at admission | ||||||||
| Headache, n (%) | 24 (26.4) | 35 (43.8) | 0.5 | 0.24–0.88 | 0.023 | 1.7 | 0.78–3.58 | 0.183 |
| Confusion, n (%) | 33 (36.3) | 12 (15.0) | 3.2 | 1.53–6.81 | 0.001 | 0.5 | 0.21–1.21 | 0.124 |
| Nausea, n (%) | 3 (3.3) | 13 (16.3) | 0.2 | 0.10–0.64 | 0.004 | 4.1 | 1.0–17.43 | 0.054 |
| Radiological parameters | ||||||||
| Hematoma median, mm (IQR) | 20 (13–25) | 17 (11–25) | 1.5 | 0.49–5.1 | 0.019 | 8.1 | 0.26–0.61 | 0.012 |
| Outcome | ||||||||
| mRS3 months, median (IQR) | 2 (1–4) | 1 (0–2) | - | 0.36–1.63 | 0.002 | 0.2 | 0.58–1.36 | 0.613 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dubinski, D.; Won, S.-Y.; Behmanesh, B.; Cantré, D.; Mattes, I.; Trnovec, S.; Baumgarten, P.; Schuss, P.; Freiman, T.M.; Gessler, F. Significance of Temporal Muscle Thickness in Chronic Subdural Hematoma. J. Clin. Med. 2022, 11, 6456. https://doi.org/10.3390/jcm11216456
Dubinski D, Won S-Y, Behmanesh B, Cantré D, Mattes I, Trnovec S, Baumgarten P, Schuss P, Freiman TM, Gessler F. Significance of Temporal Muscle Thickness in Chronic Subdural Hematoma. Journal of Clinical Medicine. 2022; 11(21):6456. https://doi.org/10.3390/jcm11216456
Chicago/Turabian StyleDubinski, Daniel, Sae-Yeon Won, Bedjan Behmanesh, Daniel Cantré, Isabell Mattes, Svorad Trnovec, Peter Baumgarten, Patrick Schuss, Thomas M. Freiman, and Florian Gessler. 2022. "Significance of Temporal Muscle Thickness in Chronic Subdural Hematoma" Journal of Clinical Medicine 11, no. 21: 6456. https://doi.org/10.3390/jcm11216456