1. Introduction
The incidence of bone/spinal metastasis has increased because of improvements in cancer therapy [
1,
2,
3,
4]. Bone/spinal metastasis is a debilitating complication that causes intractable pain and/or neurological deficits [
5]. In particular, a symptomatic spinal metastasis (SSM) markedly decreases the performance status (PS) and activities of daily living (ADL) [
6], rendering it difficult to maintain and improve the quality of life (QOL). Furthermore, because SSM decreases the PS and ADL, primary cancer treatments such as chemotherapy and radiotherapy must often be cancelled due to the patients’ poor general condition. Therefore, patient survival is shortened. Bone/spinal metastasis is thus a growing global health problem that requires appropriate management.
In the management of SSM, Patchell et al. reported that direct decompressive surgery followed by radiotherapy is superior to radiotherapy alone in improving patients’ ambulatory status and survival rate [
7]. However, in contrast to these findings, a matched pair analysis did not prove the superiority of spine surgery over radiotherapy [
8]. Other studies revealed that spine surgery improves physical activity, pain, and neurological function [
9,
10]. Prospective cohort studies have also investigated the effect of spine surgery on the PS, ADL, neurological status and QOL of patients with SSM [
6,
11,
12]; however, these studies included patients who underwent postoperative chemotherapy, which affects survival. Overall, the impact of spine surgery for SMM remains unclear and requires investigation in a prospective study of patients who do not undergo postoperative chemotherapy.
At present, the management of SSM is ultimately palliative and aims to achieve a favorable QOL. In addition, it is important for patients with SSM to stay at home as long as possible until they reach the terminal phase. The prediction of the chronological clinical course of patients with SSM is essential for the planning of a multidisciplinary treatment or terminal care.
Studies have reported patient survival rate after surgery for SSM and retrospectively identified independent prognostic factors. The ambulatory status is strongly associated with prolonged survival [
13,
14,
15]. In addition, the body mass index is an independent predictor of survival, as a favorable nutritional status is associated with improved survival [
16]. Thus, surgery is expected to indirectly improve survival. However, Jansson and Bauer [
10] concluded that surgery for SSM is purely palliative, does not affect survival and must be weighed against other treatment options. The impact of spine surgery on the survival and outcome of patients with SSM remains controversial. We hypothesized that spine surgery improves the general condition, ambulatory status, ADL and QOL of patients with SSM, and that these effects improve survival. Hence, this prospective cohort study aimed to determine the effect of surgery on the survival rate and outcomes of patients with SSM.
2. Patients and Methods
2.1. Ethics Statement
This prospective cohort study was conducted at our hospital. The study protocol was approved by the ethics committee and institutional review board of our hospital. Written informed consent was obtained from each patient. The study was conducted in concordance with the principles of the Declaration of Helsinki and with the laws and regulations of our country.
2.2. Patients and Procedures
This prospective cohort study was performed in a single institution. A consecutive cohort of 122 patients with SSM was prospectively studied from 2013 to 2017. The diagnosis of spinal metastasis was based on magnetic resonance imaging and computed tomography of the whole spine. In some cases, the final diagnosis was established using positron emission tomography–computed tomography and needle biopsy.
SSM was defined as spinal metastases associated with progressive neurological deficits, spinal instability or intractable pain resistant to conservative care. Consequently, all patients with SSM were surgical candidates. The exclusion criteria were (1) impaired consciousness due to cerebral metastasis, (2) terminal phase with an expected survival of maximum 2 weeks, (3) complete paraplegia for more than 72 h, (4) previous spine surgery, (5) a single spinal metastasis lesion (such patients received curative treatment via total spondylectomy).
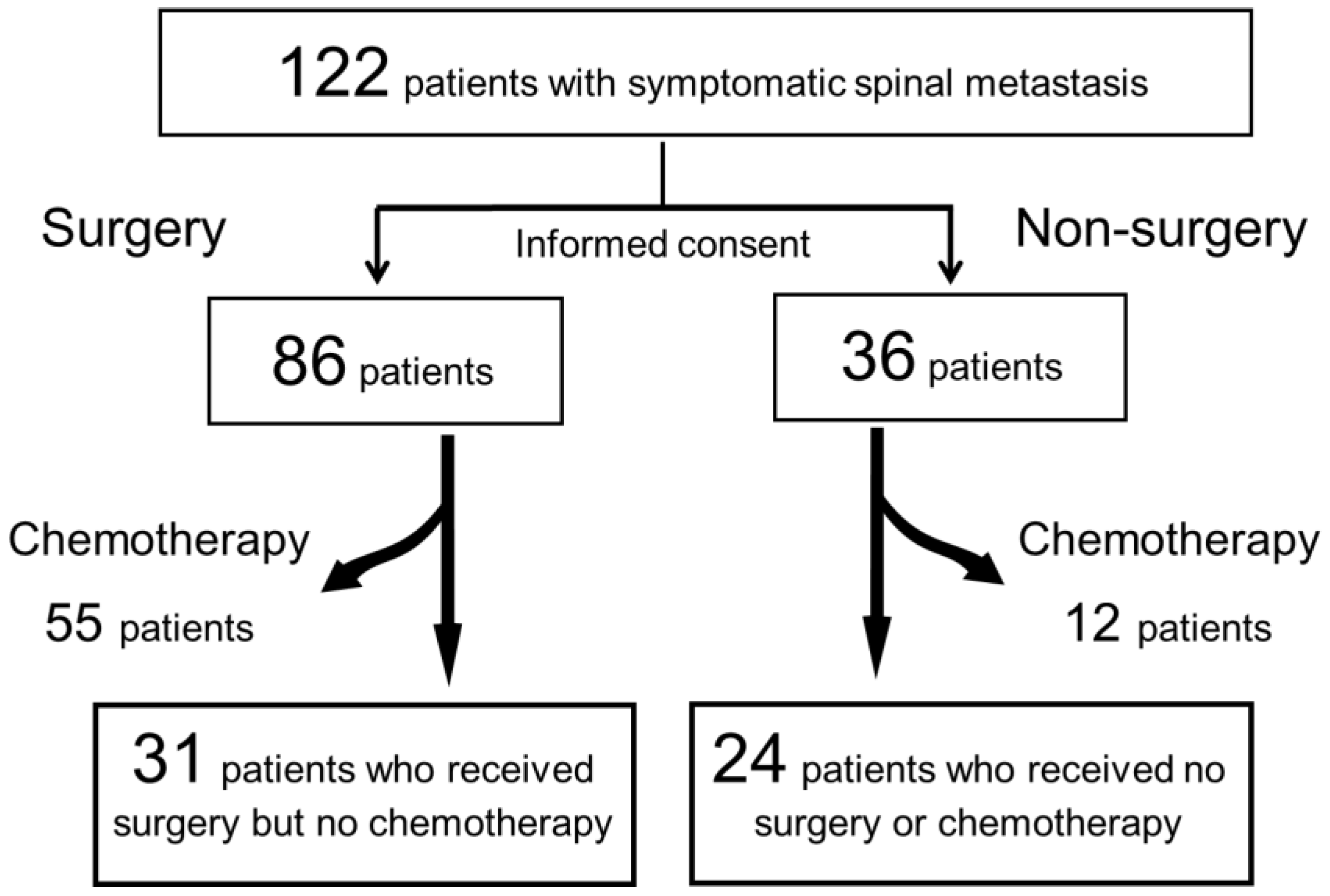
After the diagnosis of SSM, a recommendation of spine surgery and a comprehensive explanation of the risks and benefits of surgery and other adjuvant therapies were given to all patients and their families using written documentation. Patients chose to undergo surgery by their own volition. Both patients who underwent surgery (surgery group) and those who did not (non-surgery group) were administered radiotherapy, physical therapy and palliative care services. Chemotherapy, including molecular targeted drugs and hormone therapy, was administered if indicated. However, as chemotherapy is a strong positive prognostic factor, patients who underwent chemotherapy were excluded from the present study in order to maintain the homogeneity of the cohort and enable the evaluation of the effect of spine surgery alone on the outcome (
Figure 1). The patients underwent clinical evaluations before treatment.
All surgeries involved single-stage posterior decompression and stabilization with fixation using lateral mass screws for the cervical spine and pedicle screws for the thoracic and lumbar spine. Neither corpectomy nor an anterior approach was performed. All patients then underwent the removal of their immobilization devices. The patients were mobilized immediately after surgery and underwent radiotherapy and chemotherapy 2 weeks postoperatively.
2.3. Clinical Assessment
The clinical evaluations included the Tokuhashi score [
17], the new Katagiri score [
18,
19], a nomogram [
20], the Eastern Cooperative Oncology Group PS [
21], the Barthel Index (BI) [
22], the ambulatory status based on the Frankel classification [
23] and the EuroQol Five Dimension questionnaire score (EQ-5D) [
24]. A BI of less than 40 points indicates the need for another person’s help for every daily activity. The primary endpoint was the PS, BI, QOL and ambulatory status at 1 month after the diagnosis of SSM. Follow-up was routinely performed once a month from the study commencement until patient’s death. The survival time after study commencement was recorded as the final endpoint. Patients who were alive but could not visit our department were contacted by telephone to obtain the final follow-up information [
25].
2.4. Statistical Analysis
All values are expressed as mean ± standard deviation. Demographic data were compared using the t-test, Mann–Whitney U test, chi-square test, and Fisher exact test. The survival rates of the surgery and non-surgery groups were compared by the Kaplan–Meier method and log-rank test.
The potential prognostic factors investigated at study commencement in both groups were: sex, age, Tokuhashi score, new Katagiri score, nomogram, location, primary cancer growth rate, visceral or cerebral metastasis, use of a bone-modifying agent (BMA), PS, ambulatory status, BI and EQ-5D. The location was categorized based on the spinal instability neoplastic score as junctional spine (occiput–C2, C7–T2, T11–L1, L5–S1), mobile spine (C3–6, L2–4), or rigid spine (T3–10) [
26]. The primary cancer was categorized using the new Katagiri score as a slowly growing tumor (hormone-dependent breast and prostate cancer, thyroid cancer, multiple myeloma, malignant lymphoma), a moderately growing tumor (lung cancer treated with molecular targeted drugs, hormone-independent breast and prostate cancer, renal cell carcinoma, endometrial and ovarian cancer, sarcoma, others) or a rapidly growing tumor (lung cancer not treated with molecular targeted drugs, colorectal cancer, esophageal cancer, other urological cancers, hepatocellular carcinoma, gall bladder cancer, cervical cancer, cancer of unknown origin) [
18]. Categorical variables with more than two modalities were recorded using dummy variables.
For the chronological evaluation of the endpoints, the Kruskal–Wallis test and Scheffe post hoc test were used to assess the significance of differences between the surgery and the non-surgery groups. An intention-to-treat population was used throughout. Statistical significance was set at p < 0.05. The analyses were performed using PASW Statistics 18 (SPSS, Chicago, IL, USA).
4. Discussion
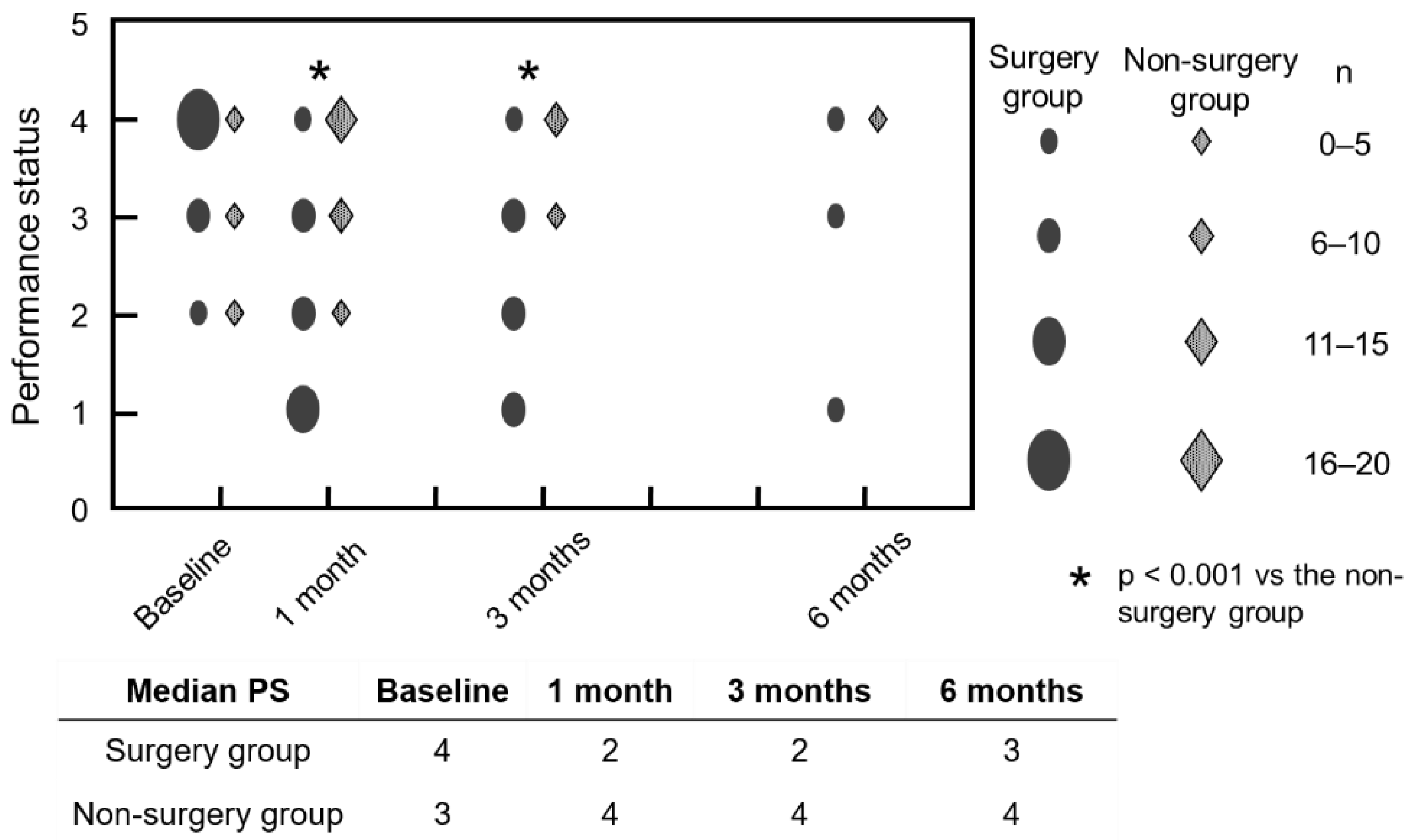
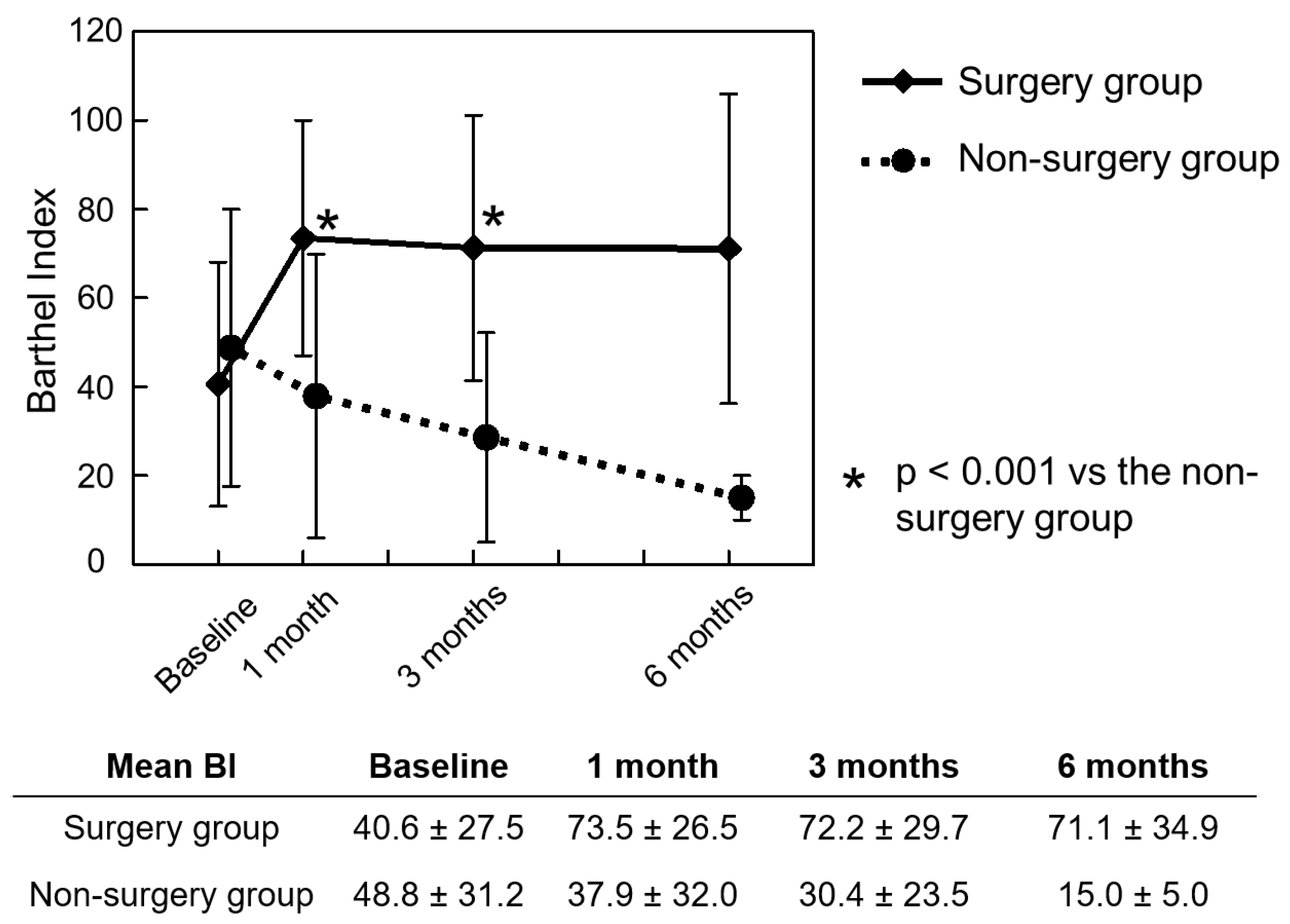
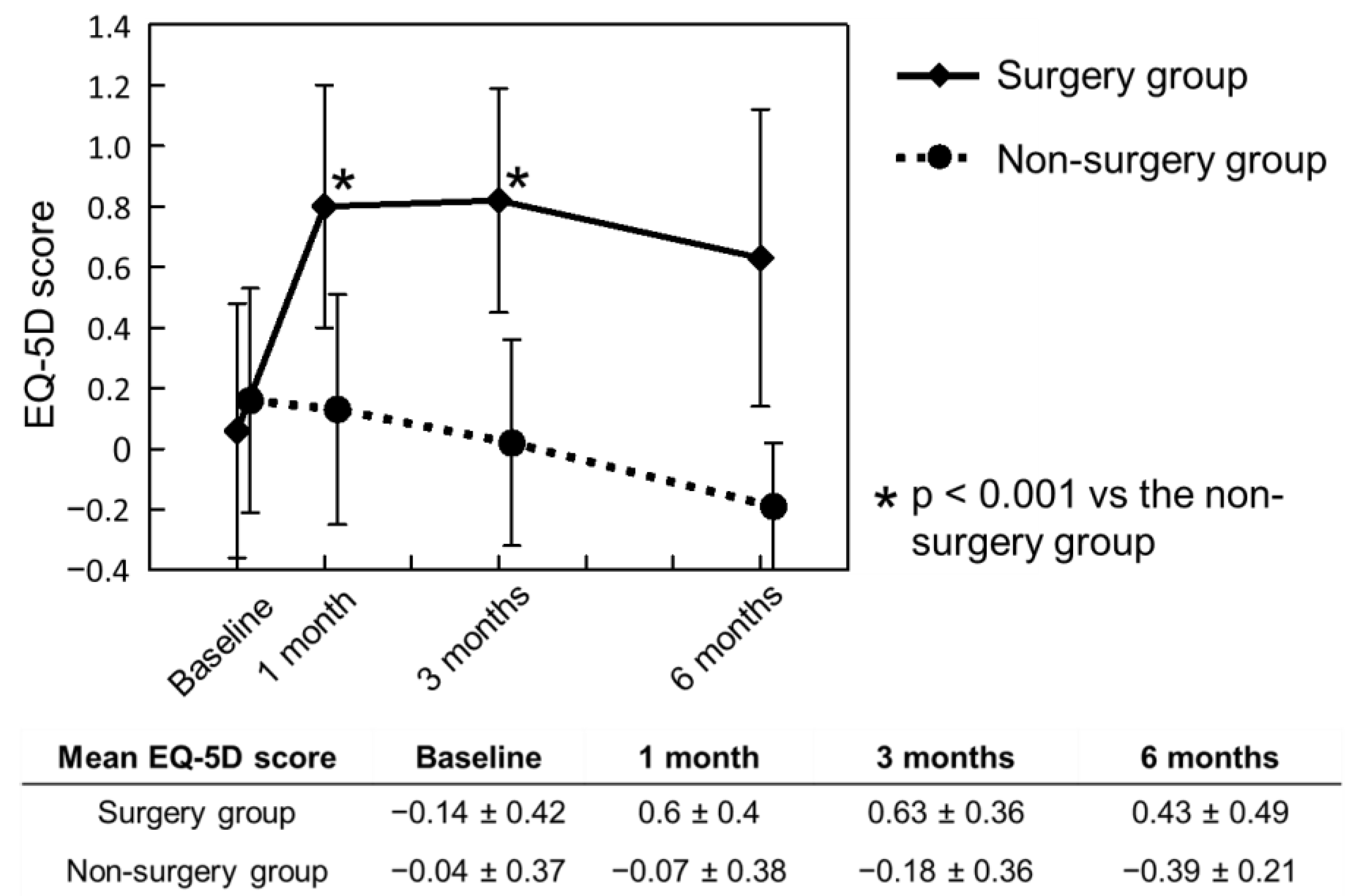
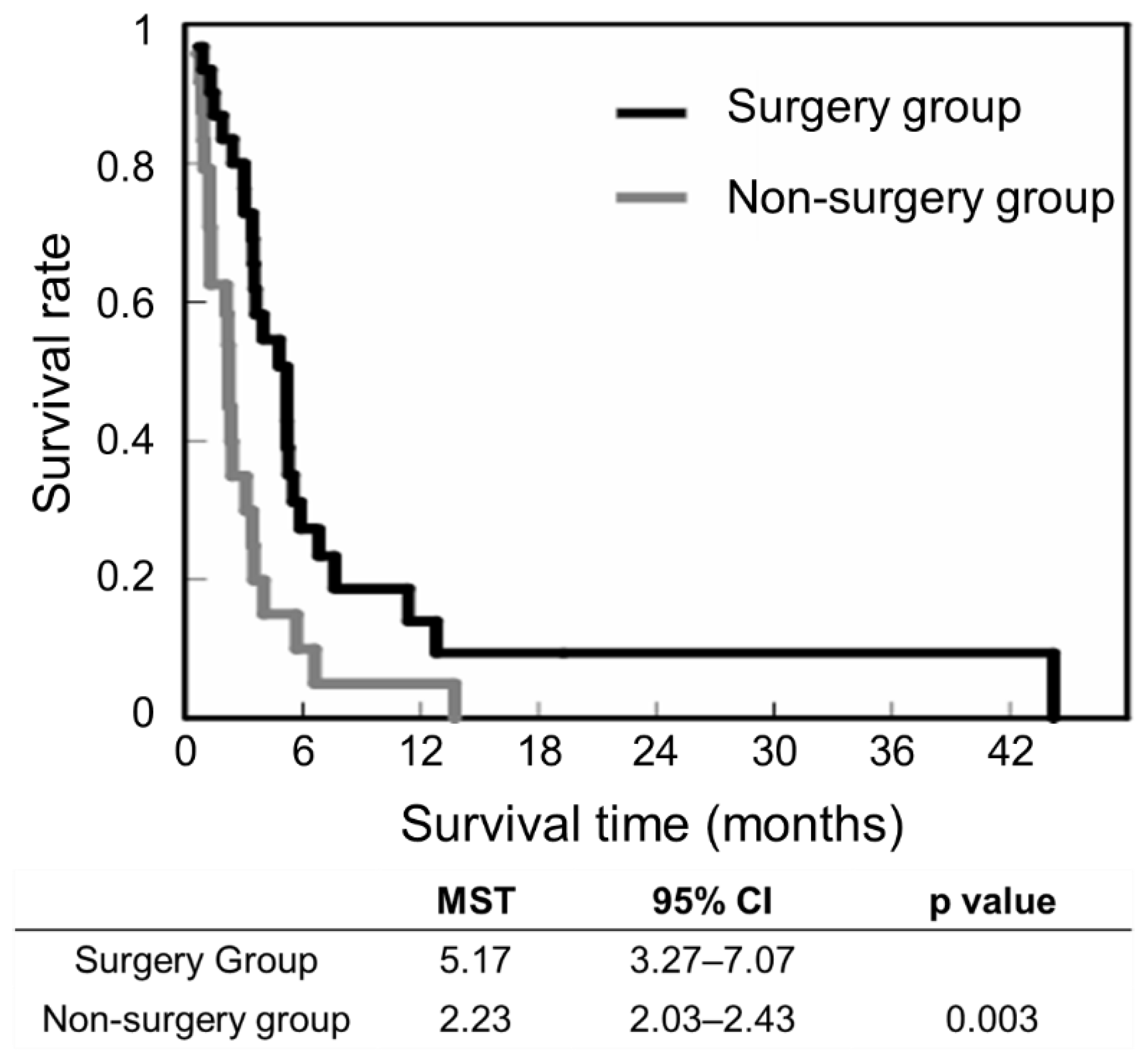
This prospective study was performed to elucidate the effect of spine surgery after the development of SSM. The results revealed that spine surgery for SSM significantly improved the PS, ADL, ambulatory status and QOL. In addition, patients who underwent spine surgery had a significantly longer survival than those who did not undergo surgery.
The natural history of patients with spinal cord compression due to spinal metastasis remains unclear [
27]. In the current study, 24 patients did not undergo either surgery or chemotherapy; in this group, the MST was 2.23 months, and the PS, BI, EQ-5D and ambulatory status decreased during 6 months of follow-up. These results suggest that the natural history of SSM is severe deterioration. In contrast, spine surgery instantly improved the PS, BI, EQ-5D and ambulatory status, and these improvements were maintained for 3 months. However, the PS and EQ-5D regressed at 6 months. As the improvements in the BI, ambulatory status and neurological status were maintained for 6 months, the main reason for the re-exacerbation of the PS and EQ-5D might be the progression of the primary cancer rather than the exacerbation of spinal cord compression.
It remains unclear whether the current management options improve the condition of patients with SSM. Studies on spinal metastasis have reported that radiotherapy improves pain [
28,
29], and BMA therapy prevents skeletal-related events [
30]. However, there is no evidence that radiation and BMA therapy improve intractable pain and deteriorated neurological status due to SSM. Furthermore, the previous studies that reported that spine surgery improves spinal instability and neurological status were retrospective, and the results included the effect of chemotherapy. Thus, the current study was performed to evaluate the effect of spine surgery without chemotherapy on the PS, ADL, walking ability and QOL of patients with SSM.
Regarding the effect of spine surgery for SSM on survival, several studies report that spine surgery provides the opportunity for patients to receive adjuvant therapy and thus may lead to improved survival [
9,
13,
31]. However, these studies were also retrospective and included patients who received chemotherapy. Therefore, there is a need for a prospective study to investigate the effect of spine surgery alone (i.e., excluding patients who receive chemotherapy) on the survival of patients with SSM. In the current study, the survival time was relatively short in the non-surgery group but was significantly extended in the surgery group. As there were no significant differences between the two groups in baseline clinical characteristics and adjuvant therapy, this result suggests that spine surgery improves the survival of patients with SSM.
To determine the relationship between survival and general condition, we assessed the PS, ambulatory status and BI using the log-rank test. The factors associated with a significantly longer survival were a PS of 0–2, an ambulatory neurological status and a BI ≥ 60. As the spine is not a vital organ, spine surgery does not directly improve the survival. Therefore, the longer survival after spine surgery might be due to improvements in patients’ general condition. Furthermore, many enrolled patients who underwent surgery were subsequently excluded because they received chemotherapy. These patients were able to undergo chemotherapy because spine surgery improved their PS and ADL. As chemotherapy is a strong prognostic factor, the survival of patients who received both spine surgery and chemotherapy is expected to be much longer than that of patients who received spine surgery alone. There is a need for a future study evaluating multidisciplinary treatments for SSM.
The major limitations of the current study are the small sample size and the lack of randomization regarding the treatment. As patients decided to undergo surgery by their own volition, the results may have been affected by their positive feelings associated with the completion of treatment (i.e., patients may have chosen surgery to receive chemotherapy). This might have affected the improvements in the PS, ADL and ambulation, leading to the administration of chemotherapy. The exclusion of patients who received chemotherapy means that the study cohort comprised patients with sarcoma or hepatocellular carcinoma and those with contraindications for chemotherapy. Thus, the results might be limited to patients with specific types of cancer that rarely cause bone metastasis.
In summary, this prospective cohort study revealed that spine surgery alone improves the general condition and survival rate of patients with SSM.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}