
High Temporal Resolution Dual-Source Photon-Counting CT for Coronary Artery Disease: Initial Multicenter Clinical Experience
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. CT Imaging
2.3. Image Evaluation
2.4. Definition of Evaluated Parameters
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Patient Outcome
3.3. Radiation Dose
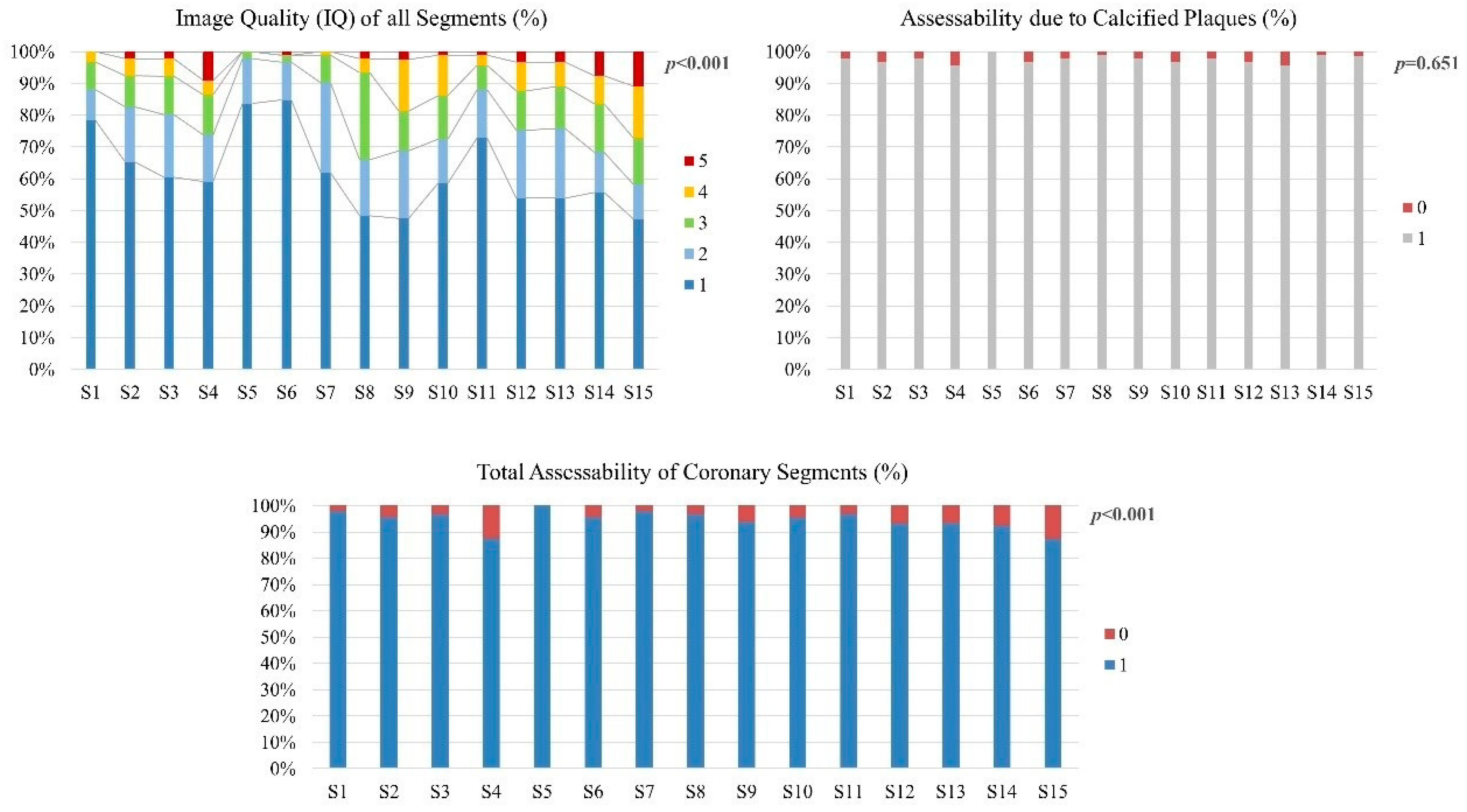
3.4. Image Quality and Assessability of Coronary Segments
3.5. Image Quality, Assessability and CNR of the Three Main Vessels
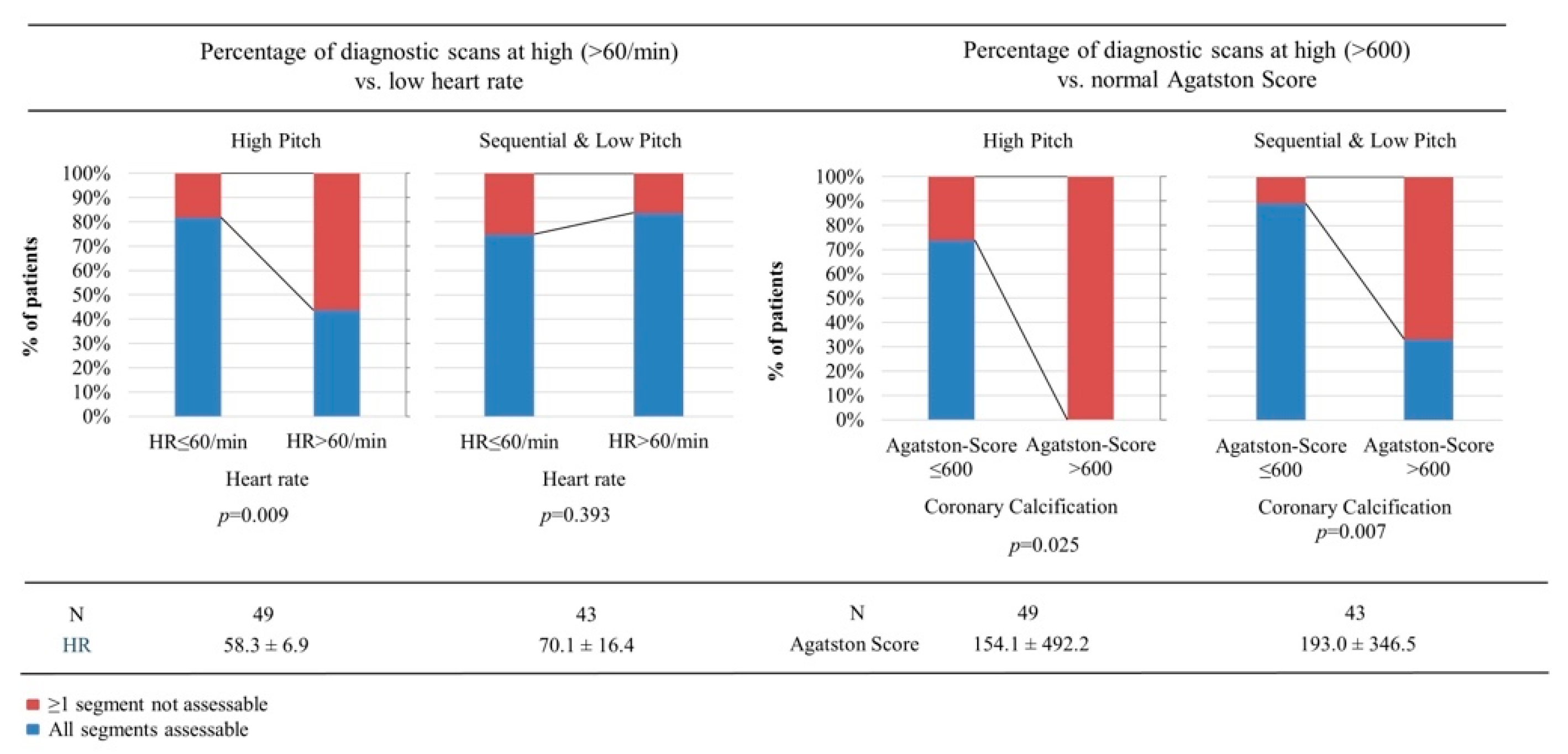
3.6. Assessability of Whole Spectral PCD-CCTA Scans
3.7. Diagnostic Performance in the Subgroup with ICA as Reference Standard
4. Discussion
4.1. Diagnostic Performance in Clinical Practice
4.2. Radiation Dose
4.3. Diagnostic Performance with ICA as Reference Standard
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Gulati, M.; Levy, P.D.; Mukherjee, D.; Amsterdam, E.; Bhatt, D.L.; Birtcher, K.K.; Blankstein, R.; Boyd, J.; Bullock-Palmer, R.P.; Conejo, T.; et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 144, e368–e454. [Google Scholar] [CrossRef] [PubMed]
- Dey, D.; Lee, C.J.; Ohba, M.; Gutstein, A.; Slomka, P.J.; Cheng, V.; Suzuki, Y.; Suzuki, S.; Wolak, A.; Le Meunier, L.; et al. Image quality and artifacts in coronary CT angiography with dual-source CT: Initial clinical experience. J. Cardiovasc. Comput. Tomogr. 2008, 2, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Hecht, H.S.; Bhatti, T. How much calcium is too much calcium for coronary computerized tomographic angiography? J. Cardiovasc. Comput. Tomogr. 2008, 2, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Si-Mohamed, S.A.; Boccalini, S.; Lacombe, H.; Diaw, A.; Varasteh, M.; Rodesch, P.-A.; Dessouky, R.; Villien, M.; Tatard-Leitman, V.; Bochaton, T.; et al. Coronary CT Angiography with Photon-counting CT: First-In-Human Results. Radiology 2022, 303, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef] [PubMed]
- Allmendinger, T.; Nowak, T.; Flohr, T.; Klotz, E.; Hagenauer, J.; Alkadhi, H.; Schmidt, B. Photon-Counting Detector CT-Based Vascular Calcium Removal Algorithm: Assessment Using a Cardiac Motion Phantom. Investig. Radiol. 2022, 57, 399–405. [Google Scholar] [CrossRef]
- van der Werf, N.R.; Greuter, M.J.W.; Booij, R.; van der Lugt, A.; Budde, R.P.J.; van Straten, M. Coronary calcium scores on dual-source photon-counting computed tomography: An adapted Agatston methodology aimed at radiation dose reduction. Eur. Radiol. 2022, 32, 5201–5209. [Google Scholar] [CrossRef] [PubMed]
- Sandfort, V.; Persson, M.; Pourmorteza, A.; Noël, P.B.; Fleischmann, D.; Willemink, M.J. Spectral photon-counting CT in cardiovascular imaging. J. Cardiovasc. Comput. Tomogr. 2021, 15, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, K.; Petersilka, M.; Henning, A.; Shanblatt, E.R.; Schmidt, B.; Flohr, T.G.; Ferrero, A.; Baffour, F.; Diehn, F.E.; Yu, L.; et al. First Clinical Photon-counting Detector CT System: Technical Evaluation. Radiology 2022, 303, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Abbara, S.; Blanke, P.; Maroules, C.D.; Cheezum, M.; Choi, A.D.; Han, B.K.; Marwan, M.; Naoum, C.; Norgaard, B.L.; Rubinshtein, R.; et al. SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J. Cardiovasc. Comput. Tomogr. 2016, 10, 435–449. [Google Scholar] [CrossRef]
- Ochs, M.M.; aus dem Siepen, F.; Fritz, T.; Andre, F.; Gitsioudis, G.; Korosoglou, G.; Seitz, S.; Bogomazov, Y.; Schlett, C.L.; Sokiranski, R.; et al. Limits of the possible: Diagnostic image quality in coronary angiography with third-generation dual-source CT. Clin. Res. Cardiol. 2017, 106, 485–492. [Google Scholar] [CrossRef]
- Leschka, S.; Wildermuth, S.; Boehm, T.; Desbiolles, L.; Husmann, L.; Plass, A.; Koepfli, P.; Schepis, T.; Marincek, B.; Kaufmann, P.A.; et al. Noninvasive Coronary Angiography with 64-Section CT: Effect of Average Heart Rate and Heart Rate Variability on Image Quality. Radiology 2006, 241, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Stocker, T.J.; Deseive, S.; Leipsic, J.; Hadamitzky, M.; Chen, M.Y.; Rubinshtein, R.; Heckner, M.; Bax, J.J.; Fang, X.-M.; Grove, E.L.; et al. Reduction in radiation exposure in cardiovascular computed tomography imaging: Results from the PROspective multicenter registry on radiaTion dose Estimates of cardiac CT angIOgraphy iN daily practice in 2017 (PROTECTION VI). Eur. Heart J. 2018, 39, 3715–3723. [Google Scholar] [CrossRef]
- Bild, D.E. Multi-Ethnic Study of Atherosclerosis: Objectives and Design. Am. J. Epidemiol. 2002, 156, 871–881. [Google Scholar] [CrossRef] [PubMed]
- Gassenmaier, S.; Tsiflikas, I.; Greulich, S.; Kuebler, J.; Hagen, F.; Nikolaou, K.; Niess, A.M.; Burgstahler, C.; Krumm, P. Prevalence of pathological FFRCT values without coronary artery stenosis in an asymptomatic marathon runner cohort. Eur. Radiol. 2021, 31, 8975–8982. [Google Scholar] [CrossRef]
- Li, P.; Xu, L.; Yang, L.; Wang, R.; Hsieh, J.; Sun, Z.; Fan, Z.; Leipsic, J.A. Blooming Artifact Reduction in Coronary Artery Calcification by A New De-blooming Algorithm: Initial Study. Sci. Rep. 2018, 8, 6945. [Google Scholar] [CrossRef] [PubMed]
- Renker, M.; Nance, J.W.; Schoepf, U.J.; O’Brien, T.X.; Zwerner, P.L.; Meyer, M.; Kerl, J.M.; Bauer, R.W.; Fink, C.; Vogl, T.J.; et al. Evaluation of Heavily Calcified Vessels with Coronary CT Angiography: Comparison of Iterative and Filtered Back Projection Image Reconstruction. Radiology 2011, 260, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, U.; Moselewski, F.; Cury, R.C.; Ferencik, M.; Jang, I.; Diaz, L.J.; Abbara, S.; Brady, T.J.; Achenbach, S. Predictive Value of 16-Slice Multidetector Spiral Computed Tomography to Detect Significant Obstructive Coronary Artery Disease in Patients at High Risk for Coronary Artery Disease: Patient- Versus Segment-Based Analysis. Circulation 2004, 110, 2638–2643. [Google Scholar] [CrossRef]
- Leber, A.W.; Knez, A.; von Ziegler, F.; Becker, A.; Nikolaou, K.; Paul, S.; Wintersperger, B.; Reiser, M.; Becker, C.R.; Steinbeck, G.; et al. Quantification of Obstructive and Nonobstructive Coronary Lesions by 64-Slice Computed Tomography. J. Am. Coll. Cardiol. 2005, 46, 147–154. [Google Scholar] [CrossRef]
- Ahn, S.J.; Kang, D.K.; Sun, J.S.; Yoon, M.-H. Accuracy and Predictive Value of Coronary Computed Tomography Angiography for the Detection of Obstructive Coronary Heart Disease in Patients With an Agatston Calcium Score Above 400. J. Comput. Assist. Tomogr. 2013, 37, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Ochs, M.M.; Andre, F.; Korosoglou, G.; Fritz, T.; Seitz, S.; Bogomazov, Y.; Schlett, C.L.; Sokiranski, R.; Sommer, A.; Gückel, F.; et al. Strengths and limitations of coronary angiography with turbo high-pitch third-generation dual-source CT. Clin. Radiol. 2017, 72, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.J.H.; Eisenberg, E.; Friedman, J.; Cheng, V.; Hayes, S.; Tamarappoo, B.; Thomson, L.; Berman, D.S. Impact of heart rate on coronary computed tomographic angiography interpretability with a third-generation dual-source scanner. Int. J. Cardiol. 2019, 295, 42–47. [Google Scholar] [CrossRef]
- Krumm, P. Editorial Comment: Radiologists Should Implement Dose Reduction Strategies for Coronary CTA Given the Preserved High Image Quality. Am. J. Roentgenol. 2021, 217, 1352. [Google Scholar] [CrossRef]
- Stocker, T.J.; Nühlen, N.; Schmermund, A.; Leipsic, J.; Grove, E.L.; Deseive, S.; Bax, J.J.; Maurovich-Horvat, P.; Otton, J.; Hadamitzky, M.; et al. Impact of Dose Reduction Strategies on Image Quality of Coronary CTA in Real-World Clinical Practice: A Subanalysis of PROTECTION VI Registry Data. Am. J. Roentgenol. 2021, 217, 1344–1352. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Z.; Kong, L.; Song, L.; Merges, R.D.; Chen, J.; Jin, Z. Dual-source CT coronary angiography in patients with atrial fibrillation: Comparison with single-source CT. Eur. J. Radiol. 2008, 68, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Rist, C.; Johnson, T.R.; Müller-Starck, J.; Arnoldi, E.; Saam, T.; Becker, A.; Leber, A.W.; Wintersperger, B.J.; Becker, C.R.; Reiser, M.F.; et al. Noninvasive Coronary Angiography Using Dual-Source Computed Tomography in Patients With Atrial Fibrillation. Investig. Radiol. 2009, 44, 159–167. [Google Scholar] [CrossRef]
- Budoff, M.J.; Dowe, D.; Jollis, J.G.; Gitter, M.; Sutherland, J.; Halamert, E.; Scherer, M.; Bellinger, R.; Martin, A.; Benton, R.; et al. Diagnostic Performance of 64-Multidetector Row Coronary Computed Tomographic Angiography for Evaluation of Coronary Artery Stenosis in Individuals Without Known Coronary Artery Disease. J. Am. Coll. Cardiol. 2008, 52, 1724–1732. [Google Scholar] [CrossRef]
- Meijboom, W.B.; Meijs, M.F.L.; Schuijf, J.D.; Cramer, M.J.; Mollet, N.R.; van Mieghem, C.A.G.; Nieman, K.; van Werkhoven, J.M.; Pundziute, G.; Weustink, A.C.; et al. Diagnostic Accuracy of 64-Slice Computed Tomography Coronary Angiography. J. Am. Coll. Cardiol. 2008, 52, 2135–2144. [Google Scholar] [CrossRef]
- Min, J.K.; Shaw, L.J.; Devereux, R.B.; Okin, P.M.; Weinsaft, J.W.; Russo, D.J.; Lippolis, N.J.; Berman, D.S.; Callister, T.Q. Prognostic Value of Multidetector Coronary Computed Tomographic Angiography for Prediction of All-Cause Mortality. J. Am. Coll. Cardiol. 2007, 50, 1161–1170. [Google Scholar] [CrossRef]
- Stein, P.D.; Beemath, A.; Kayali, F.; Skaf, E.; Sanchez, J.; Olson, R.E. Multidetector Computed Tomography for the Diagnosis of Coronary Artery Disease: A Systematic Review. Am. J. Med. 2006, 119, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Scheffel, H.; Alkadhi, H.; Plass, A.; Vachenauer, R.; Desbiolles, L.; Gaemperli, O.; Schepis, T.; Frauenfelder, T.; Schertler, T.; Husmann, L.; et al. Accuracy of dual-source CT coronary angiography: First experience in a high pre-test probability population without heart rate control. Eur. Radiol. 2006, 16, 2739–2747. [Google Scholar] [CrossRef] [PubMed]
- Catalán, P.; Leta, R.; Hidalgo, A.; Montiel, J.; Alomar, X.; Viladés, D.; Barros, A.; Pujadas, S.; Carreras, F.; Padró, J.M.; et al. Ruling Out Coronary Artery Disease with Noninvasive Coronary Multidetector CT Angiography before Noncoronary Cardiovascular Surgery. Radiology 2011, 258, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Levin, D.C.; Halpern, E.J.; Fischman, D.; Savage, M.; Walinsky, P. Accuracy of MDCT in Assessing the Degree of Stenosis Caused by Calcified Coronary Artery Plaques. Am. J. Roentgenol. 2008, 191, 1676–1683. [Google Scholar] [CrossRef] [PubMed]
- Mergen, V.; Sartoretti, T.; Baer-Beck, M.; Schmidt, B.; Petersilka, M.; Wildberger, J.E.; Euler, A.; Eberhard, M.; Alkadhi, H. Ultra-High-Resolution Coronary CT Angiography With Photon-Counting Detector CT: Feasibility and Image Characterization. Investig. Radiol. 2022. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SD or N (%) | |
|---|---|
| Age (years) | 58.4 ± 13.7 |
| Male gender | 60 (65%) |
| History of CAD | 8 (8.9%) |
| History of stenting | 4 (4.3%) |
| History of coronary artery bypass graft (CABG) | 0 |
| History of myocardial infarction (MI) | 0 |
| Hyperlipidemia | 38% |
| Hypertension | 59% |
| Smoking | 17% |
| Diabetes mellitus | 14% |
| BMI (kg/m²) | 26.9 ± 5.9 |
| Agatston score | 172.3 ± 428.5 |
| kV average (kV) | 120 ± 0 |
| Effective mAs (mAs) | 52.5 ± 29.6 |
| CTDI.vol (mGy) | 16.4 ± 25.3 |
| Dose length product (mGy.cm) | 234.1 ± 347.6 |
| Effective dose (mSv) | 3.51 ± 5.21 |
| Contrast volume (mL) | 70.9 ± 8.3 |
| Contrast flow (mL/s) | 5.3 ± 0.5 |
| Received beta-blockers | 72 (78%) |
| Average heart rate (bpm) | 63.8 ± 13.6 |
| Minimum heart rate (bpm) | 62.8 ± 29.3 |
| Maximum heart rate (bpm) | 68.1 ± 19.3 |
| HR variability | 0.095 ± 0.285 |
| Right coronary artery dominance | 61 (66%) |
| Co-dominance of coronary arteries | 18 (20%) |
| Left coronary artery dominance | 13 (14%) |
| Coronary Artery | Segments | Assessability (%) | Image Quality (Mean ± SD) | Image Quality (Median, (IQR)) |
|---|---|---|---|---|
| Overall | all | 95 | 1.70 ± 0.76 | 1 (IQR 1–2) |
| RCA | 1 | 98 | 1.37 | 1 |
| 2 | 96 | 1.62 | 1 | |
| 3 | 97 | 1.69 | 1 | |
| 4 | 88 | 1.90 | 1 | |
| LAD | 5 | 100 | 1.18 | 1 |
| 6 | 96 | 1.21 | 1 | |
| 7 | 98 | 1.49 | 1 | |
| 8 | 97 | 1.95 | 2 | |
| 9 | 94 | 2.05 | 2 | |
| 10 | 95 | 1.84 | 1 | |
| LCX | 11 | 97 | 1.45 | 1 |
| 12 | 93 | 1.87 | 1 | |
| 13 | 93 | 1.85 | 1 | |
| 14 | 92 | 2.00 | 1 | |
| 15 | 87 | 2.33 | 2 | |
| p-value | <0.001 | <0.001 | <0.001 |
| Coronary Artery | IQ (Median, IQR) | CNR (Mean ± SD) | Agatston-Score (Mean ± SD) | Diagnostic (%) | Diagnostic CAC (%) | Diagnostic Mov. (%) |
|---|---|---|---|---|---|---|
| LAD | 1 (1–2) | 20.65 ± 10.01 | 79.84 ± 210.34 | 87 | 92 | 95 |
| LCX | 1 (1–3) | 19.86 ± 10.09 | 24.37 ± 86.50 | 87 | 95 | 90 |
| RCA | 1 (1–2) | 20.44 ± 11.35 | 59.43 ± 169.73 | 86 | 93 | 90 |
| p-value | 0.007 | 0.041 | 0.001 | 0.951 | 0.549 | 0.431 |
| Assessability at High-Pitch | Assessability Sequential and Low-Pitch | |||||
|---|---|---|---|---|---|---|
| All Segments Assessable (n = 34; 69%) | ≥1 Segment Not Assessable (n = 15; 31%) | p-Value | All Segments Assessable (n = 35; 81%) | ≥1 Segment Not Assessable (n = 8; 19%) | p-Value | |
| BMI [kg/m2] (mean ± SD | 25.3 ± 2.4 | 26.7 ± 8.2 | 0.402 | 26.2 ± 5.7 | 33.6 ± 7.4 | 0.013 |
| HR [bpm] (mean ± SD | 57.2 ± 6.8 | 60.9 ± 6.6 | 0.044 | 70.8 ± 15.9 | 66.8 ± 19.5 | 0.267 |
| HV (mean ± SD) | 0.035 ± 0.052 | 0.059 ± 0.116 | 0.164 | 0.118 ± 0.401 | 0.314 ± 0.393 | 0.110 |
| Agatston Score (mean ± SD) | 48.2 ± 107.7 | 392.9 ± 845.7 | 0.011 | 125.9 ± 265.7 | 486.6 ± 506.4 | 0.043 |
| Age (mean ± SD) | 56.1 ± 14.2 | 56.7 ± 15.4 | 0.446 | 60.9 ± 12.5 | 60.0 ± 14.1 | 0.430 |
| Male Gender (%) | 68% | 76% | 0.474 | 50% | 57% | 0.507 |
| Per Segment | For Coronary Stenosis > 50% |
| Total Number (n) | 126 |
| Significant Stenosis (≥50%) | 13 |
| No Significant Stenosis | 113 |
| Segments with Stents | 3 (all evaluable) |
| True Negative | 108 |
| True Positive | 12 |
| False Negative | 1 |
| False Positive | 5 |
| Sensitivity | 92% |
| Specificity | 96% |
| PPV | 71% |
| NPV | 99% |
| Accuracy | 95% |
| per patient | For coronary stenosis >50% |
| Total Number (n) | 9 |
| Significant Stenosis (≥50%) | 3 |
| No Significant Stenosis | 6 |
| Patients with Stents | 1 (evaluable) |
| True Negative | 4 |
| True Positive | 3 |
| False Negative | 0 |
| False Positive | 2 |
| Sensitivity | 100% |
| Specificity | 67% |
| PPV | 60% |
| NPV | 100% |
| Accuracy | 78% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soschynski, M.; Hagen, F.; Baumann, S.; Hagar, M.T.; Weiss, J.; Krauss, T.; Schlett, C.L.; von zur Mühlen, C.; Bamberg, F.; Nikolaou, K.; et al. High Temporal Resolution Dual-Source Photon-Counting CT for Coronary Artery Disease: Initial Multicenter Clinical Experience. J. Clin. Med. 2022, 11, 6003. https://doi.org/10.3390/jcm11206003
Soschynski M, Hagen F, Baumann S, Hagar MT, Weiss J, Krauss T, Schlett CL, von zur Mühlen C, Bamberg F, Nikolaou K, et al. High Temporal Resolution Dual-Source Photon-Counting CT for Coronary Artery Disease: Initial Multicenter Clinical Experience. Journal of Clinical Medicine. 2022; 11(20):6003. https://doi.org/10.3390/jcm11206003
Chicago/Turabian StyleSoschynski, Martin, Florian Hagen, Stefan Baumann, Muhammad Taha Hagar, Jakob Weiss, Tobias Krauss, Christopher L. Schlett, Constantin von zur Mühlen, Fabian Bamberg, Konstantin Nikolaou, and et al. 2022. "High Temporal Resolution Dual-Source Photon-Counting CT for Coronary Artery Disease: Initial Multicenter Clinical Experience" Journal of Clinical Medicine 11, no. 20: 6003. https://doi.org/10.3390/jcm11206003