
Evidence-Based Mechanical Ventilatory Strategies in ARDS

 ,
,
Abstract
:1. Introduction
2. Lung Protective Ventilation
3. Optimal PEEP
4. Driving Pressure
5. Recruitment Maneuvers
6. Prone Ventilation
7. Neuromuscular Blockade
8. Conservative Lung Strategy
9. Other Strategies
9.1. High Frequency Oscillatory Ventilation
9.2. Non-Invasive Ventilation
9.3. Airway Pressure Release Ventilation
9.4. Venovenous Extracorporeal Membranous Oxygenation (ECMO)
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ashbaugh, D.G.; Bigelow, D.B.; Petty, T.L.; Levine, B.E. Acute respiratory distress in adults. Lancet 1967, 2, 319–323. [Google Scholar] [CrossRef]
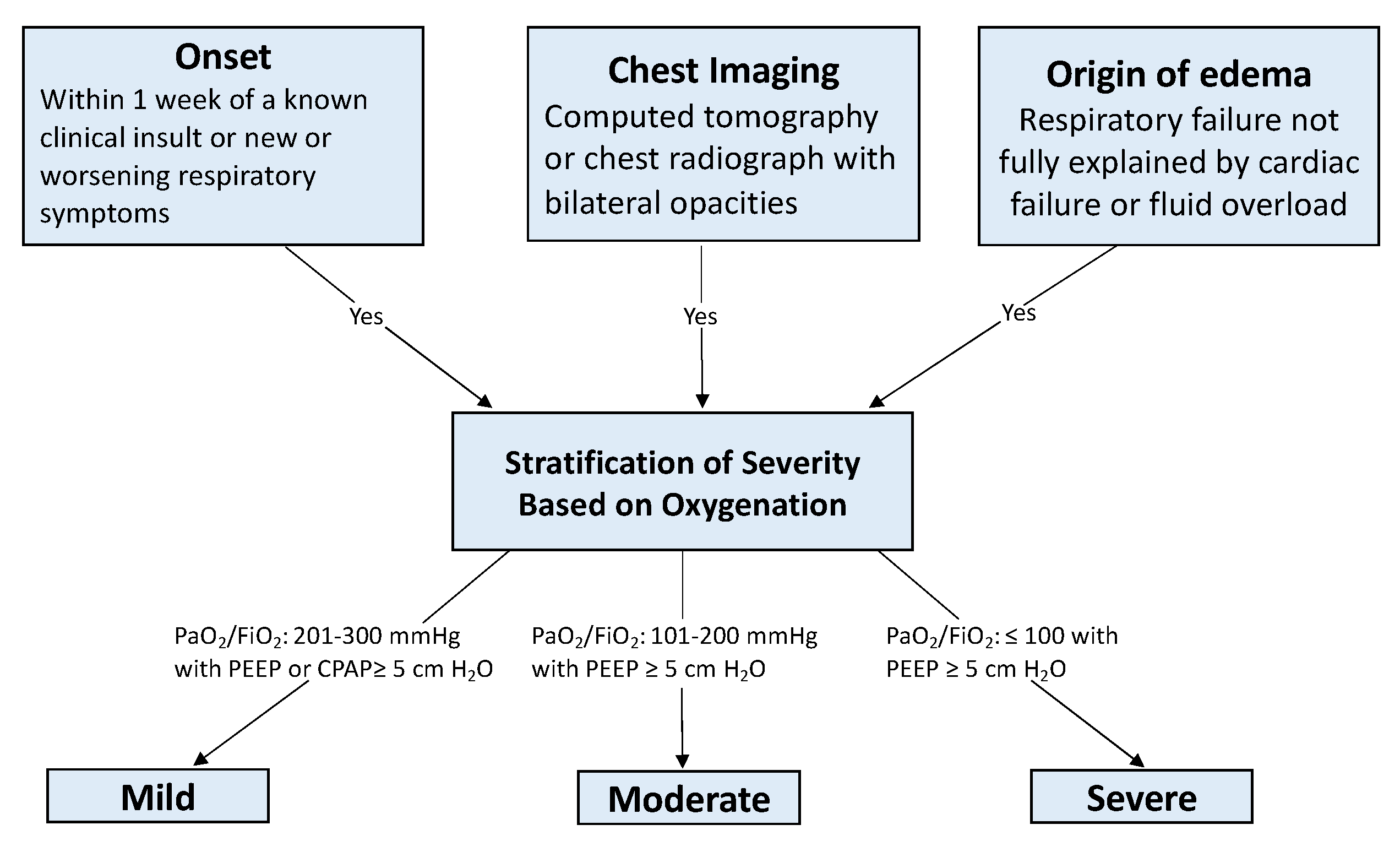
- The ARDS Definition Task Force. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Rubenfeld, G.D.; Caldwell, E.; Peabody, E.; Weaver, J.; Martin, D.P.; Neff, M.; Stern, E.J.; Hudson, L.D. Incidence and outcomes of acute lung injury. N. Engl. J. Med. 2005, 353, 1685–1693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.; Rubenfeld, G.D. Fifty Years of Research in ARDS. The Epidemiology of Acute Respiratory Distress Syndrome. A 50th Birthday Review. Am. J. Respir. Crit. Care Med. 2017, 195, 860–870. [Google Scholar] [CrossRef] [PubMed]
- Fan, E.; Del Sorbo, L.; Goligher, E.C.; Hodgson, C.L.; Munshi, L.; Walkey, A.J.; Adhikari, N.K.J.; Amato, M.B.P.; Branson, R.; Brower, R.G.; et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1253–1263. [Google Scholar] [CrossRef]
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar] [CrossRef]
- Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A.; Wiedemann, H.P.; Arroliga, A.C.; Fisher, C.J., Jr.; Komara, J.J. Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef] [Green Version]
- Brower, R.G.; Lanken, P.N.; MacIntyre, N.; Matthay, M.A.; Morris, A.; Ancukiewicz, M.; Schoenfeld, D.; Thompson, B.T. Higher versus Lower Positive End-Expiratory Pressures in Patients with the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2004, 351, 327–336. [Google Scholar] [CrossRef] [Green Version]
- Williams, E.C.; Motta-Ribeiro, G.C.; Vidal Melo, M.F. Driving Pressure and Transpulmonary Pressure: How Do We Guide Safe Mechanical Ventilation? Anesthesiology 2019, 131, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical Ventilation to Minimize Progression of Lung Injury in Acute Respiratory Failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Caironi, P.; Cressoni, M.; Chiumello, D.; Ranieri, M.; Quintel, M.; Russo, S.G.; Cornejo, R.; Bugedo, G.; Carlesso, E.; Russo, R.; et al. Lung opening and closing during ventilation of acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2010, 181, 578–586. [Google Scholar] [CrossRef]
- Mercat, A.; Richard, J.-C.M.; Vielle, B.; Jaber, S.; Osman, D.; Diehl, J.-L.; Lefrant, J.-Y.; Prat, G.; Richecoeur, J.; Nieszkowska, A.; et al. Positive End-Expiratory Pressure Setting in Adults With Acute Lung Injury and Acute Respiratory Distress Syndrome: A Randomized Controlled Trial. JAMA 2008, 299, 646–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meade, M.O.; Cook, D.J.; Guyatt, G.H.; Slutsky, A.S.; Arabi, Y.M.; Cooper, D.J.; Davies, A.R.; Hand, L.E.; Zhou, Q.; Thabane, L.; et al. Ventilation Strategy Using Low Tidal Volumes, Recruitment Maneuvers, and High Positive End-Expiratory Pressure for Acute Lung Injury and Acute Respiratory Distress Syndrome: A Randomized Controlled Trial. JAMA 2008, 299, 637–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, L.; Xie, J.; Huang, Y.; Pan, C.; Yang, Y.; Qiu, H.; Liu, L. Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation response to PEEP: A systematic review and meta-analysis. BMC Anesthesiol. 2018, 18, 172. [Google Scholar] [CrossRef]
- Talmor, D.; Sarge, T.; Malhotra, A.; O’Donnell, C.R.; Ritz, R.; Lisbon, A.; Novack, V.; Loring, S.H. Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury. N. Engl. J. Med. 2008, 359, 2095–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beitler, J.R.; Sarge, T.; Banner-Goodspeed, V.M.; Gong, M.N.; Cook, D.; Novack, V.; Loring, S.H.; Talmor, D. Effect of Titrating Positive End-Expiratory Pressure (PEEP) With an Esophageal Pressure-Guided Strategy vs an Empirical High PEEP-Fio2 Strategy on Death and Days Free From Mechanical Ventilation Among Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2019, 321, 846–857. [Google Scholar] [CrossRef] [Green Version]
- Sarge, T.; Baedorf-Kassis, E.; Banner-Goodspeed, V.; Novack, V.; Loring, S.H.; Gong, M.N.; Cook, D.; Talmor, D.; Beitler, J.R. Effect of Esophageal Pressure-guided Positive End-Expiratory Pressure on Survival from Acute Respiratory Distress Syndrome: A Risk-based and Mechanistic Reanalysis of the EPVent-2 Trial. Am. J. Respir. Crit. Care Med. 2021, 204, 1153–1163. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, H.; Yamada, Y.; Fan, E. The future of driving pressure: A primary goal for mechanical ventilation? J. Intensive Care 2018, 6, 64. [Google Scholar] [CrossRef]
- Amato, M.B.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Borges, J.B.; Hedenstierna, G.; Larsson, A.; Suarez-Sipmann, F. Altering the mechanical scenario to decrease the driving pressure. Crit. Care 2015, 19, 342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grieco, D.L.; Chen, L.; Dres, M.; Brochard, L. Should we use driving pressure to set tidal volume? Curr. Opin. Crit. Care 2017, 23, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Costa, E.L.V.; Slutsky, A.S.; Brochard, L.J.; Brower, R.; Serpa-Neto, A.; Cavalcanti, A.B.; Mercat, A.; Meade, M.; Morais, C.C.A.; Goligher, E.; et al. Ventilatory Variables and Mechanical Power in Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2021, 204, 303–311. [Google Scholar] [CrossRef]
- Tonetti, T.; Vasques, F.; Rapetti, F.; Maiolo, G.; Collino, F.; Romitti, F.; Camporota, L.; Cressoni, M.; Cadringher, P.; Quintel, M.; et al. Driving pressure and mechanical power: New targets for VILI prevention. Ann. Transl. Med. 2017, 5, 286. [Google Scholar] [CrossRef] [Green Version]
- Rothen, H.U.; Neumann, P.; Berglund, J.E.; Valtysson, J.; Magnusson, A.; Hedenstierna, G. Dynamics of re-expansion of atelectasis during general anaesthesia. Br. J. Anaesth. 1999, 82, 551–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelosi, P.; Gama de Abreu, M.; Rocco, P.R. New and conventional strategies for lung recruitment in acute respiratory distress syndrome. Crit. Care 2010, 14, 210. [Google Scholar] [CrossRef] [Green Version]
- Güldner, A.; Kiss, T.; Serpa Neto, A.; Hemmes, S.N.; Canet, J.; Spieth, P.M.; Rocco, P.R.; Schultz, M.J.; Pelosi, P.; Gama de Abreu, M. Intraoperative protective mechanical ventilation for prevention of postoperative pulmonary complications: A comprehensive review of the role of tidal volume, positive end-expiratory pressure, and lung recruitment maneuvers. Anesthesiology 2015, 123, 692–713. [Google Scholar] [CrossRef]
- Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial Investigators. Effect of Lung Recruitment and Titrated Positive End-Expiratory Pressure (PEEP) vs Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2017, 318, 1335–1345. [Google Scholar] [CrossRef]
- Hodgson, C.L.; Cooper, D.J.; Arabi, Y.; King, V.; Bersten, A.; Bihari, S.; Brickell, K.; Davies, A.; Fahey, C.; Fraser, J.; et al. Maximal Recruitment Open Lung Ventilation in Acute Respiratory Distress Syndrome (PHARLAP). A Phase II, Multicenter Randomized Controlled Clinical Trial. Am. J. Respir. Crit. Care Med. 2019, 200, 1363–1372. [Google Scholar] [CrossRef]
- Chen, L.; Del Sorbo, L.; Grieco, D.L.; Junhasavasdikul, D.; Rittayamai, N.; Soliman, I.; Sklar, M.C.; Rauseo, M.; Ferguson, N.D.; Fan, E.; et al. Potential for Lung Recruitment Estimated by the Recruitment-to-Inflation Ratio in Acute Respiratory Distress Syndrome. A Clinical Trial. Am. J. Respir. Crit. Care Med. 2020, 201, 178–187. [Google Scholar] [CrossRef]
- Abroug, F.; Ouanes-Besbes, L.; Elatrous, S.; Brochard, L. The effect of prone positioning in acute respiratory distress syndrome or acute lung injury: A meta-analysis. Areas of uncertainty and recommendations for research. Intensive Care Med. 2008, 34, 1002–1011. [Google Scholar] [CrossRef]
- Sud, S.; Friedrich, J.O.; Taccone, P.; Polli, F.; Adhikari, N.K.; Latini, R.; Pesenti, A.; Guérin, C.; Mancebo, J.; Curley, M.A.; et al. Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: Systematic review and meta-analysis. Intensive Care Med. 2010, 36, 585–599. [Google Scholar] [CrossRef]
- Menk, M.; Estenssoro, E.; Sahetya, S.K.; Neto, A.S.; Sinha, P.; Slutsky, A.S.; Summers, C.; Yoshida, T.; Bein, T.; Ferguson, N.D. Current and evolving standards of care for patients with ARDS. Intensive Care Med 2020, 46, 2157–2167. [Google Scholar] [CrossRef]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Sud, S.; Friedrich, J.O.; Adhikari, N.K.J.; Taccone, P.; Mancebo, J.; Polli, F.; Latini, R.; Pesenti, A.; Curley, M.A.Q.; Fernandez, R.; et al. Effect of prone positioning during mechanical ventilation on mortality among patients with acute respiratory distress syndrome: A systematic review and meta-analysis. Can. Med. Assoc. J. 2014, 186, E381–E390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laffey, J.G.; Bellani, G.; Pham, T.; Fan, E.; Madotto, F.; Bajwa, E.K.; Brochard, L.; Clarkson, K.; Esteban, A.; Gattinoni, L.; et al. Potentially modifiable factors contributing to outcome from acute respiratory distress syndrome: The LUNG SAFE study. Intensive Care Med. 2016, 42, 1865–1876. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Forel, J.M.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.M.; Perez, D.; Seghboyan, J.M.; et al. Neuromuscular blockers in early acute respiratory distress syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [Green Version]
- Ho, A.T.N.; Patolia, S.; Guervilly, C. Neuromuscular blockade in acute respiratory distress syndrome: A systematic review and meta-analysis of randomized controlled trials. J. Intensive Care 2020, 8, 12. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Belley-Cote, E.; Møller, M.H.; Angus, D.C.; Papazian, L.; Arabi, Y.M.; Citerio, G.; Connolly, B.; Denehy, L.; Fox-Robichaud, A.; et al. Neuromuscular blockade in patients with ARDS: A rapid practice guideline. Intensive Care Med. 2020, 46, 1977–1986. [Google Scholar] [CrossRef]
- Keddissi, J.I.; Youness, H.A.; Jones, K.R.; Kinasewitz, G.T. Fluid management in Acute Respiratory Distress Syndrome: A narrative review. Can. J. Respir. Ther. 2019, 55, 1–8. [Google Scholar] [CrossRef]
- Wiedemann, H.P.; Wheeler, A.P.; Bernard, G.R.; Thompson, B.T.; Hayden, D.; deBoisblanc, B.; Connors, A.F., Jr.; Hite, R.D.; Harabin, A.L. Comparison of two fluid-management strategies in acute lung injury. N. Engl. J. Med. 2006, 354, 2564–2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphrey, H.; Hall, J.; Sznajder, I.; Silverstein, M.; Wood, L. Improved survival in ARDS patients associated with a reduction in pulmonary capillary wedge pressure. Chest 1990, 97, 1176–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyers, M.; Rodrigues, N.; Ari, A. High-frequency oscillatory ventilation: A narrative review. Can. J. Respir. Ther. CJRT Rev. Can. De La Ther. Respir. RCTR 2019, 55, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Derdak, S.; Mehta, S.; Stewart, T.E.; Smith, T.; Rogers, M.; Buchman, T.G.; Carlin, B.; Lowson, S.; Granton, J. High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults: A randomized, controlled trial. Am. J. Respir. Crit. Care Med. 2002, 166, 801–808. [Google Scholar] [CrossRef]
- Putensen, C.; Mutz, N.J.; Putensen-Himmer, G.; Zinserling, J. Spontaneous breathing during ventilatory support improves ventilation-perfusion distributions in patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1999, 159, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Liu, Y.; Li, N.; You, D.; Zhao, Y. The safety and efficacy of airway pressure release ventilation in acute respiratory distress syndrome patients: A PRISMA-compliant systematic review and meta-analysis. Medicine 2020, 99, e18586. [Google Scholar] [CrossRef]
- Gu, X.L.; Wu, G.N.; Yao, Y.W.; Shi, D.H.; Song, Y. Is high-frequency oscillatory ventilation more effective and safer than conventional protective ventilation in adult acute respiratory distress syndrome patients? A meta-analysis of randomized controlled trials. Crit. Care 2014, 18, R111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabrini, L.; Landoni, G.; Oriani, A.; Plumari, V.P.; Nobile, L.; Greco, M.; Pasin, L.; Beretta, L.; Zangrillo, A. Noninvasive ventilation and survival in acute care settings: A comprehensive systematic review and metaanalysis of randomized controlled trials. Crit. Care Med. 2015, 43, 880–888. [Google Scholar] [CrossRef]
- Tucci, M.R.; Costa, E.L.; Nakamura, M.A.; Morais, C.C. Noninvasive ventilation for acute respiratory distress syndrome: The importance of ventilator settings. J. Thorac. Dis. 2016, 8, E982–E986. [Google Scholar] [CrossRef] [Green Version]
- Schnell, D.; Timsit, J.F.; Darmon, M.; Vesin, A.; Goldgran-Toledano, D.; Dumenil, A.S.; Garrouste-Orgeas, M.; Adrie, C.; Bouadma, L.; Planquette, B.; et al. Noninvasive mechanical ventilation in acute respiratory failure: Trends in use and outcomes. Intensive Care Med. 2014, 40, 582–591. [Google Scholar] [CrossRef]
- Meeder, A.M.; Tjan, D.H.; van Zanten, A.R. Noninvasive and invasive positive pressure ventilation for acute respiratory failure in critically ill patients: A comparative cohort study. J. Thorac. Dis. 2016, 8, 813–825. [Google Scholar] [CrossRef] [Green Version]
- Patel, B.K.; Wolfe, K.S.; Pohlman, A.S.; Hall, J.B.; Kress, J.P. Effect of Noninvasive Ventilation Delivered by Helmet vs Face Mask on the Rate of Endotracheal Intubation in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2016, 315, 2435–2441. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.S.; Garpestad, E. The Bumpy Road for Noninvasive Ventilation in Acute Respiratory Distress Syndrome. Coming to an End? Am. J. Respir. Crit. Care Med. 2017, 195, 9–10. [Google Scholar] [CrossRef]
- Bellani, G.; Laffey, J.G.; Pham, T.; Madotto, F.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Bumbasirevic, V.; Piquilloud, L.; et al. Noninvasive Ventilation of Patients with Acute Respiratory Distress Syndrome. Insights from the LUNG SAFE Study. Am. J. Respir. Crit. Care Med. 2017, 195, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Frat, J.P.; Thille, A.W.; Mercat, A.; Girault, C.; Ragot, S.; Perbet, S.; Prat, G.; Boulain, T.; Morawiec, E.; Cottereau, A.; et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N. Engl. J. Med. 2015, 372, 2185–2196. [Google Scholar] [CrossRef] [Green Version]
- Grieco, D.L.; Menga, L.S.; Cesarano, M.; Rosà, T.; Spadaro, S.; Bitondo, M.M.; Montomoli, J.; Falò, G.; Tonetti, T.; Cutuli, S.L.; et al. Effect of Helmet Noninvasive Ventilation vs High-Flow Nasal Oxygen on Days Free of Respiratory Support in Patients With COVID-19 and Moderate to Severe Hypoxemic Respiratory Failure: The HENIVOT Randomized Clinical Trial. JAMA 2021, 325, 1731–1743. [Google Scholar] [CrossRef]
- Mireles-Cabodevila, E.; Dugar, S.; Chatburn, R.L. APRV for ARDS: The complexities of a mode and how it affects even the best trials. J. Thorac. Dis. 2018, 10, S1058–S1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Jin, X.; Lv, Y.; Wang, P.; Yang, Y.; Liang, G.; Wang, B.; Kang, Y. Early application of airway pressure release ventilation may reduce the duration of mechanical ventilation in acute respiratory distress syndrome. Intensive Care Med. 2017, 43, 1648–1659. [Google Scholar] [CrossRef] [PubMed]
- Seal, K.; Featherstone, R. Airway Pressure Release Ventilation for Acute Respiratory Distress Syndrome: Clinical Effectiveness and Guidelines [Internet]; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2018.
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef]
- Munshi, L.; Walkey, A.; Goligher, E.; Pham, T.; Uleryk, E.M.; Fan, E. Venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: A systematic review and meta-analysis. Lancet Respir. Med. 2019, 7, 163–172. [Google Scholar] [CrossRef]
- ELSO Guidelines for Cardiopulmonary Extracorporeal Life Support; Extracorporeal Life Support Organization: Ann Arbor, MI, USA, 2017.
- Wilcox, M.E.; Jaramillo-Rocha, V.; Hodgson, C.; Taglione, M.S.; Ferguson, N.D.; Fan, E. Long-Term Quality of Life After Extracorporeal Membrane Oxygenation in ARDS Survivors: Systematic Review and Meta-Analysis. J. Intensive Care Med. 2020, 35, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Scaravilli, V.; Tubiolo, D.; Russo, R.; Crimella, F.; Bichi, F.; Morlacchi, L.C.; Scotti, E.; Patrini, L.; Gattinoni, L.; et al. Quality of Life and Lung Function in Survivors of Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. Anesthesiology 2019, 130, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.J.D.; McAuley, D.F.; Perkins, G.D.; Barrett, N.; Blackwood, B.; Boyle, A.; Chee, N.; Connolly, B.; Dark, P.; Finney, S.; et al. Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respir. Res. 2019, 6, e000420. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Society | Recommendation | Strength of Recommendation | Evidence |
|---|---|---|---|
| ATS/ESICM/SCCM | Mechanical ventilation with low tidal volumes and inspiratory pressures | Strong | Moderate |
| Daily prone positioning >12 h | Strong | Moderate-high | |
| Avoid HFOV in patients with moderate or severe ARDS | Strong | Moderate-high | |
| Mechanical ventilation with higher levels of PEEP for moderate or severe ARDS | Conditional | Moderate | |
| Recruitment maneuvers should be used | Conditional | Low-moderate | |
| Additional research needed to recommend use of ECMO in patients with ARDS | Not applicable | Not applicable | |
| FICM/ICS | Mechanical ventilation with low tidal volumes (<6 mL/kg ideal body weight) and plateau pressure (<30 cm H2O) | Strong | Moderate |
| Daily prone positioning ≥12 h in patients with moderate/severe ARDS | Strong | Moderate | |
| Avoid HFOV | Strong | Moderate | |
| Conservative fluid management | Weakly in favor | Low | |
| Mechanical ventilation with higher levels of PEEP in patients with moderate/severe ARDS | Weakly in favor | Low | |
| Neuromuscular blocking agents in patients with moderate/severe ARDS | Weakly in favor | Moderate | |
| Use of ECMO in patients with severe ARDS | Weakly in favor | Very low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liaqat, A.; Mason, M.; Foster, B.J.; Kulkarni, S.; Barlas, A.; Farooq, A.M.; Patak, P.; Liaqat, H.; Basso, R.G.; Zaman, M.S.; et al. Evidence-Based Mechanical Ventilatory Strategies in ARDS. J. Clin. Med. 2022, 11, 319. https://doi.org/10.3390/jcm11020319
Liaqat A, Mason M, Foster BJ, Kulkarni S, Barlas A, Farooq AM, Patak P, Liaqat H, Basso RG, Zaman MS, et al. Evidence-Based Mechanical Ventilatory Strategies in ARDS. Journal of Clinical Medicine. 2022; 11(2):319. https://doi.org/10.3390/jcm11020319
Chicago/Turabian StyleLiaqat, Adnan, Matthew Mason, Brian J. Foster, Sagar Kulkarni, Aisha Barlas, Awais M. Farooq, Pooja Patak, Hamza Liaqat, Rafaela G. Basso, Mohammed S. Zaman, and et al. 2022. "Evidence-Based Mechanical Ventilatory Strategies in ARDS" Journal of Clinical Medicine 11, no. 2: 319. https://doi.org/10.3390/jcm11020319