
Comparison between Ecological Momentary Assessment and Questionnaire for Assessing the Frequency of Waking-Time Non-Functional Oral Behaviours
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
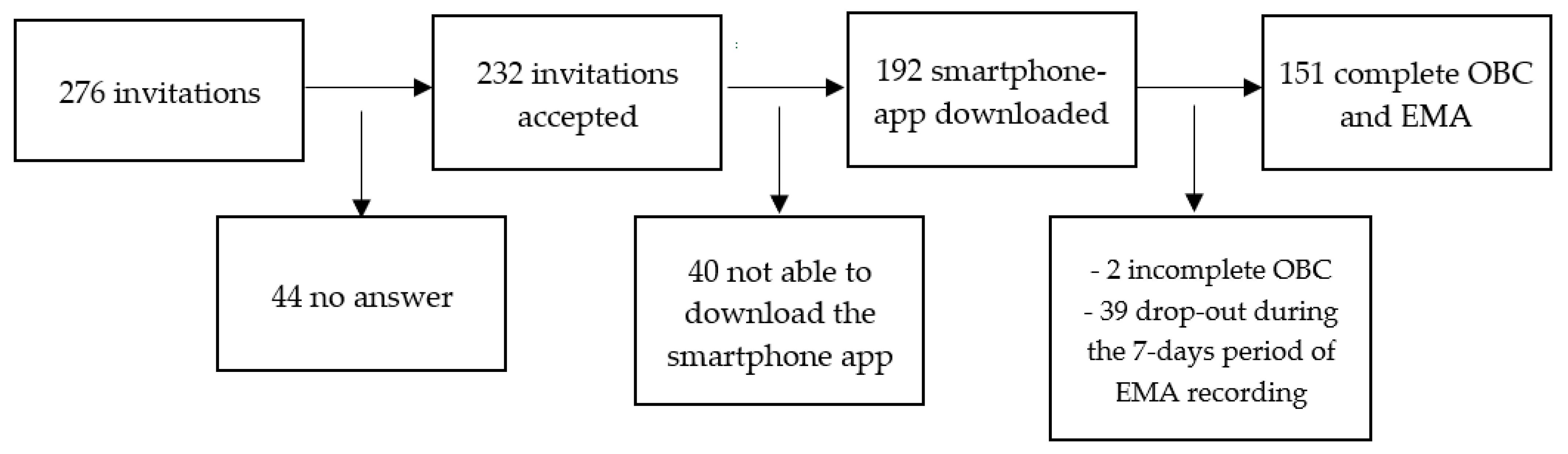
2.1. Participants’ Recruitment
2.2. Assessment of Waking-State Oral Behaviours
2.2.1. Questionnaire
- -
- Q3: Grind teeth together during waking hours.
- -
- Q4: Clench teeth together during waking hours.
- -
- Q5: Press, touch, or hold teeth together other than while eating (that is, contact between upper and lower teeth).
- -
- Q6: Hold, tighten, or tense muscles without clenching or bringing teeth together.
2.2.2. Ecological Momentary Assessment (EMA)
2.2.3. Satisfaction with the Tool
2.2.4. Statistical Analysis
3. Results
3.1. Sample
3.2. Assessment of Waking-State Oral Behaviours
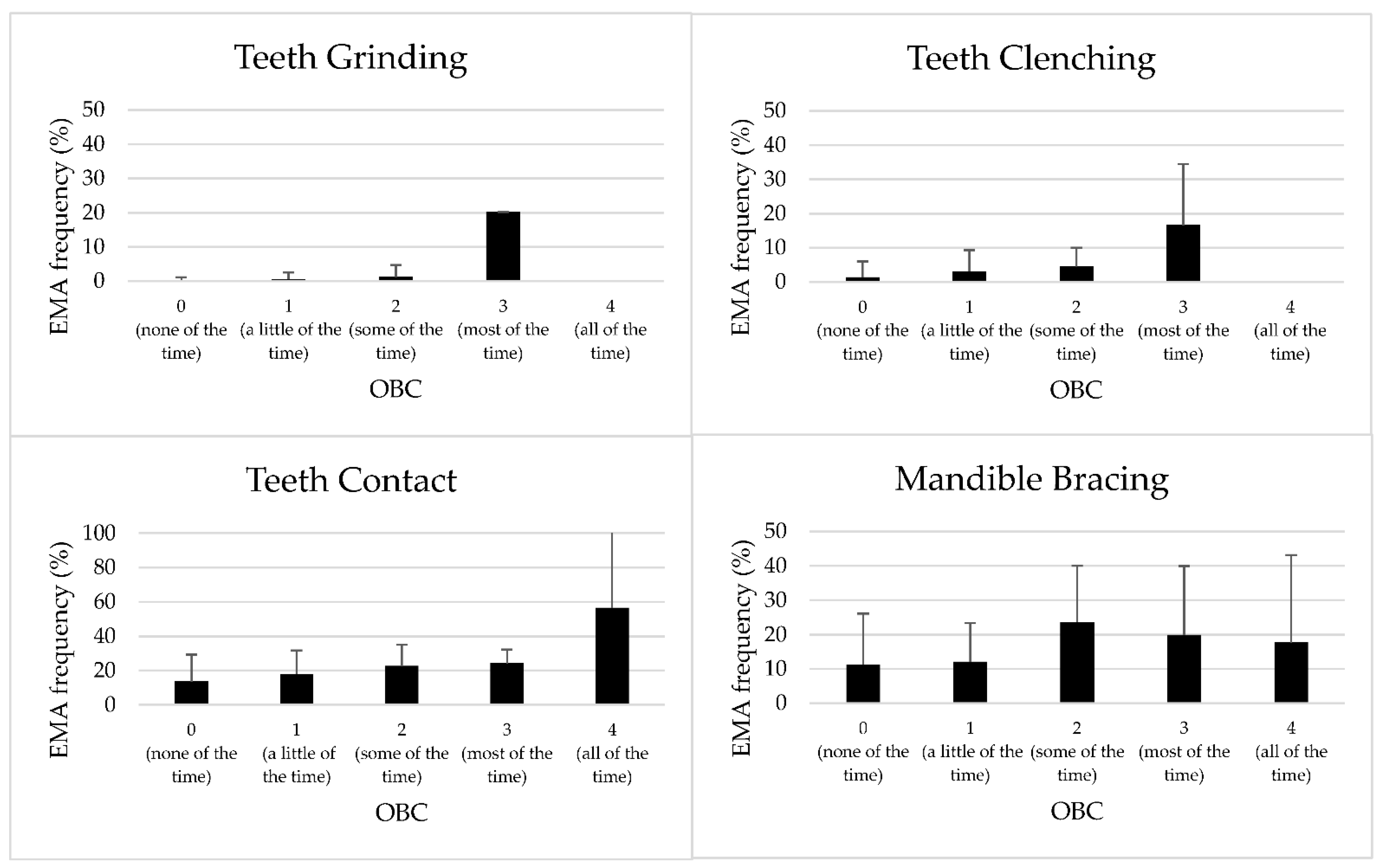
3.3. Relationship between OBC and EMA Responses
3.4. Satisfaction with the Tool
4. Discussion
5. Conclusions
- In the current sample of adults recruited from the general population, the use of a standardised questionnaire (i.e., Oral Behaviour Checklist) correctly measured the frequency of non-functional oral behaviours during waking hours as compared with a real-time assessment through a smartphone-based application for ecological momentary assessment over a 7-day period.
- Due to the limited interference with the daily activities, Oral Behaviour Checklist can be suggested for screening purpose during initial consultations.
- Given the increased awareness of awake bruxism activities observed in the general population following the use of the smartphone-based app, studies are needed to test the role of this tool in behavioural therapy for patients with potential clinical consequences.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ohrbach, R.; Markiewicz, M.R.; McCall, W.D.J. Waking-State Oral Parafunctional Behaviors: Specificity and Validity as Assessed by Electromyography. Eur. J. Oral Sci. 2008, 116, 438–444. [Google Scholar] [CrossRef]
- Donnarumma, V.; Cioffi, I.; Michelotti, A.; Cimino, R.; Vollaro, S.; Amato, M. Analysis of the Reliability of the Italian Version of the Oral Behaviours Checklist and the Relationship between Oral Behaviours and Trait Anxiety in Healthy Individuals. J. Oral Rehabil. 2018, 45, 317–322. [Google Scholar] [CrossRef]
- Donnarumma, V.; Ohrbach, R.; Simeon, V.; Lobbezoo, F.; Piscicelli, N.; Michelotti, A. Association between Waking-State Oral Behaviours, according to the Oral Behaviors Checklist, and TMD Subgroups. J. Oral Rehabil. 2021, 48, 996–1003. [Google Scholar] [CrossRef]
- Ohrbach, R.; Bair, E.; Fillingim, R.B.; Gonzalez, Y.; Gordon, S.M.; Lim, P.-F.; Ribeiro-Dasilva, M.; Diatchenko, L.; Dubner, R.; Greenspan, J.D.; et al. Clinical Orofacial Characteristics Associated with Risk of First-Onset TMD: The OPPERA Prospective Cohort Study. J. Pain 2013, 14, T33–T50. [Google Scholar] [CrossRef] [Green Version]
- Slade, G.D.; Ohrbach, R.; Greenspan, J.D.; Fillingim, R.B.; Bair, E.; Sanders, A.E.; Dubner, R.; Diatchenko, L.; Meloto, C.B.; Smith, S.; et al. Painful Temporomandibular Disorder: Decade of Discovery from OPPERA Studies. J. Dent. Res. 2016, 95, 1084–1092. [Google Scholar] [CrossRef] [Green Version]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International Consensus on the Assessment of Bruxism: Report of a Work in Progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef]
- Amato, M.; Zingone, F.; Caggiano, M.; Iovino, P.; Bucci, C.; Ciacci, C. Tooth Wear Is Frequent in Adult Patients with Celiac Disease. Nutrients 2017, 9, 1321. [Google Scholar] [CrossRef] [Green Version]
- Bucci, R.; Koutris, M.; Lobbezoo, F.; Michelotti, A. Occlusal Sensitivity in Individuals with Different Frequencies of Oral Parafunction. J. Prosthet. Dent. 2019, 122, 119–122. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network * and Orofacial Pain Special Interest Group †. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Perrotta, S.; Bucci, R.; Simeon, V.; Martina, S.; Michelotti, A.; Valletta, R. Prevalence of Malocclusion, Oral Parafunctions and Temporomandibular Disorder-Pain in Italian Schoolchildren: An Epidemiological Study. J. Oral Rehabil. 2019, 46, 611–616. [Google Scholar] [CrossRef]
- Paduano, S.; Bucci, R.; Rongo, R.; Silva, R.; Michelotti, A. Prevalence of Temporomandibular Disorders and Oral Parafunctions in Adolescents from Public Schools in Southern Italy. Cranio 2018, 38, 370–375. [Google Scholar] [CrossRef]
- Raphael, K.G.; Sirois, D.A.; Janal, M.N.; Wigren, P.E.; Dubrovsky, B.; Nemelivsky, L.V.; Klausner, J.J.; Krieger, A.C.; Lavigne, G.J. Sleep Bruxism and Myofascial Temporomandibular Disorders: A Laboratory-Based Polysomnographic Investigation. J. Am. Dent. Assoc. 2012, 143, 1223–1231. [Google Scholar] [CrossRef]
- Markiewicz, M.R.; Ohrbach, R.; McCall, W.D., Jr. Oral Behaviors Checklist: Reliability of Performance in Targeted Waking-State Behaviors. J. Orofac. Pain 2006, 20, 306–316. [Google Scholar]
- Shiffman, S.; Stone, A.A. Introduction to the Special Section: Ecological Momentary Assessment in Health Psychology. Health Psychol. 1998, 17, 3–5. [Google Scholar] [CrossRef]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological Momentary Assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Moskowitz, D.S.; Young, S.N. Ecological Momentary Assessment: What It Is and Why It Is a Method of the Future in Clinical Psychopharmacology. J. Psychiatry Neurosci. 2006, 31, 13–20. [Google Scholar]
- Runyan, J.D.; Steinke, E.G. Virtues, Ecological Momentary Assessment/Intervention and Smartphone Technology. Front. Psychol. 2015, 6, 481. [Google Scholar] [CrossRef] [Green Version]
- Guidance. Ecological Momentary Assessment Using an Ecological Momentary Assessment to Evaluate Your Digital Health Product. Available online: https://www.gov.uk/guidance/ecological-momentary-assessment (accessed on 26 September 2022).
- Manfredini, D.; Bracci, A.; Djukic, G. BruxApp: The Ecological Momentary Assessment of Awake Bruxism. Minerva Stomatol. 2016, 65, 252–255. [Google Scholar]
- Kaplan, S.E.F.; Ohrbach, R. Self-Report of Waking-State Oral Parafunctional Behaviors in the Natural Environment. J. Oral Facial Pain Headache 2016, 30, 107–119. [Google Scholar] [CrossRef]
- Ramanan, D.; Palla, S.; Bennani, H.; Polonowita, A.; Farella, M. Oral Behaviours and Wake-Time Masseter Activity in Patients with Masticatory Muscle Pain. J. Oral Rehabil. 2021, 48, 979–988. [Google Scholar] [CrossRef]
- Martina, S.; Amato, A.; Faccioni, P.; Iandolo, A.; Amato, M.; Rongo, R. The Perception of COVID-19 among Italian Dental Patients: An Orthodontic Point of View. Prog. Orthod. 2021, 22, 11. [Google Scholar] [CrossRef]
- Colonna, A.; Guarda-Nardini, L.; Ferrari, M.; Manfredini, D. COVID-19 Pandemic and the Psyche, Bruxism, Temporomandibular Disorders Triangle. Cranio 2021, 15, 1–6. [Google Scholar] [CrossRef]
- Bracci, A.; Djukic, G.; Favero, L.; Salmaso, L.; Guarda-Nardini, L.; Manfredini, D. Frequency of Awake Bruxism Behaviours in the Natural Environment. A 7-Day, Multiple-Point Observation of Real-Time Report in Healthy Young Adults. J. Oral Rehabil. 2018, 45, 423–429. [Google Scholar] [CrossRef]
- Emodi-Perlman, A.; Manfredini, D.; Shalev, T.; Yevdayev, I.; Frideman-Rubin, P.; Bracci, A.; Arnias-Winocur, O.; Eli, I. Awake Bruxism-Single-Point Self-Report versus Ecological Momentary Assessment. J. Clin. Med. 2021, 10, 1699. [Google Scholar] [CrossRef]
- Zani, A.; Lobbezoo, F.; Bracci, A.; Ahlberg, J.; Manfredini, D. Ecological Momentary Assessment and Intervention Principles for the Study of Awake Bruxism Behaviors, Part 1: General Principles and Preliminary Data on Healthy Young Italian Adults. Front. Neurol. 2019, 10, 169. [Google Scholar] [CrossRef] [Green Version]
- Colonna, A.; Lombardo, L.; Siciliani, G.; Bracci, A.; Guarda-Nardini, L.; Djukic, G.; Manfredini, D. Smartphone-Based Application for EMA Assessment of Awake Bruxism: Compliance Evaluation in a Sample of Healthy Young Adults. Clin. Oral Investig. 2020, 24, 1395–1400. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 0 (None of the Time) N (%) | 1 (Little of the Time) N (%) | 2 (Some of the Time) N (%) | 3 (Most of the Time) N (%) | 4 (All of the Time) N (%) | |
|---|---|---|---|---|---|
| Q3 | 106 (70.2%) | 28 (18.5%) | 16 (10.6%) | 1 (0.7%) | 0 (0) |
| Q4 | 44 (29.1%) | 65 (43.0%) | 34 (22.5%) | 8 (5.3%) | 0 (0) |
| Q5 | 38 (25.1%) | 67 (44.3%) | 35 (23.1%) | 9 (5.9%) | 2 (1.3%) |
| Q6 | 71 (47.0%) | 41 (27%) | 27 (17.8%) | 10 (6.6%) | 2 (1.3%) |
| Days | Frequency % |
|---|---|
| 7 | 17.8% |
| 8 | 31.7% |
| 9 | 15.2% |
| 10 | 12.5% |
| 11 | 6.6% |
| 12 | 7.2% |
| 13 | 4.6% |
| 15 | 0.6% |
| 16 | 1.3% |
| 19 | 0.6% |
| 20 | 0.6% |
| 21 | 0.6% |
| 22 | 0.6% |
| Mean (%) | SD | |
|---|---|---|
| Relaxed | 62.5% | 26 |
| Teeth Clenching | 3.6% | 7.3 |
| Teeth Contact | 18.8% | 15.2 |
| Teeth Grinding | 0.5% | 2.2 |
| Mandible Bracing | 14.3% | 15.3 |
| EMA Recording Day | Relaxed | Mandible Bracing | Teeth Contact | Grinding | Clenching | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | C.I. | Mean | C.I. | Mean | C.I. | Mean | C.I. | Mean | C.I. | |
| 1 | 61.36% | 59.14–63.58 | 14.59% | 13.03–16.14 | 20.57% | 18.78–22.36 | 2.88% | 1.89–3.86 | 0.58% | 0.26–0.91 |
| 2 | 60.67% | 58.45–62.89 | 14.74% | 13.18–16.29 | 19.46% | 17.67–21.24 | 4.7% | 3.72–5.69 | 0.36% | 0.04–0.69 |
| 3 | 61.93% | 59.72–64.15 | 14.62% | 13.07–16.17 | 18.86% | 17.07–20.65 | 3.83% | 2.84–4.81 | 0.63% | 0.3–0.95 |
| 4 | 63.96% | 61.74–66.17 | 13.9% | 12.34–15.45 | 18.64% | 16.85–20.42 | 3.12% | 2.13–4.10 | 0.48% | 0.15–0.81 |
| 5 | 63.1% | 60.88–65.32 | 13.36% | 11.81–14.91 | 18.63% | 16.85–20.42 | 4.24% | 3.25–5.22 | 0.64% | 0.31–0.97 |
| 6 | 63.69% | 61.47–65.9 | 14.99% | 13.44–16.54 | 17.09% | 15.31–18.88 | 3.79% | 2.8–4.77 | 0.42% | 0.97–0.75 |
| 7 | 63.98% | 61.76–66.2 | 13.65% | 12.1–15.2 | 18.7% | 16.91–20.48 | 2.98% | 1.99–3.96 | 0.67% | 0.34–0.99 |
| df | Chi2 | p-Value | ||
|---|---|---|---|---|
| Teeth Griding | Day | 6 | 214.80 | <0.001 |
| Q3 | 3 | 176.33 | <0.001 | |
| Day × Q3 | 18 | 262.23 | <0.001 | |
| Teeth Clenching | Day | 6 | 20.56 | 0.002 |
| Q4 | 3 | 35.77 | <0.001 | |
| Day × Q4 | 18 | 26.11 | 0.097 | |
| Teeth Contact | Day | 6 | 9.12 | 0.166 |
| Q5 | 4 | 22.00 | <0.001 | |
| Day × Q5 | 24 | 22.25 | 0.564 | |
| Mandible Bracing | Day | 6 | 6.55 | 0.364 |
| Q5 | 4 | 16.25 | 0.003 | |
| Day × Q5 | 24 | 27.04 | 0.302 |
| OBC Sum Category | Mean % | SD |
|---|---|---|
| 0 | 25.24% | 25.7 |
| 1–4 | 31.03% | 22.7 |
| >4 | 53.13% | 25.1 |
| OBC | EMA | p-Value | |
|---|---|---|---|
| Time | 3.15 ± 2.2 | 3.70 ± 2.3 | 0.017 |
| Interference | 2.39 ± 1.8 | 3.37 ± 2.3 | 0.000 |
| Awareness | 4.92 ± 2.9 | 5.8 ± 2.9 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bucci, R.; Manfredini, D.; Lenci, F.; Simeon, V.; Bracci, A.; Michelotti, A. Comparison between Ecological Momentary Assessment and Questionnaire for Assessing the Frequency of Waking-Time Non-Functional Oral Behaviours. J. Clin. Med. 2022, 11, 5880. https://doi.org/10.3390/jcm11195880
Bucci R, Manfredini D, Lenci F, Simeon V, Bracci A, Michelotti A. Comparison between Ecological Momentary Assessment and Questionnaire for Assessing the Frequency of Waking-Time Non-Functional Oral Behaviours. Journal of Clinical Medicine. 2022; 11(19):5880. https://doi.org/10.3390/jcm11195880
Chicago/Turabian StyleBucci, Rosaria, Daniele Manfredini, Francesca Lenci, Vittorio Simeon, Alessandro Bracci, and Ambrosina Michelotti. 2022. "Comparison between Ecological Momentary Assessment and Questionnaire for Assessing the Frequency of Waking-Time Non-Functional Oral Behaviours" Journal of Clinical Medicine 11, no. 19: 5880. https://doi.org/10.3390/jcm11195880