
The Oscillometric Pulse Wave Analysis Is Useful in Evaluating the Arterial Stiffness of Obese Children with Relevant Cardiometabolic Risks
 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
- Obese group: patients with a BMI score ≥ 95th percentile for age and sex.
- Control group: BMI ranging from the 5th percentile to the 85th.
- Both sexes were included, and ages ranged from 6 to 18.
2.2. Exclusion Criteria
2.3. Clinical Examination, Targeted Anamnesis, Medical History
2.4. Arterial Stiffness Assessment Using the Mobil-O-Graph
2.5. Statistical Analysis
3. Results
3.1. Descriptive Analysis of the Data
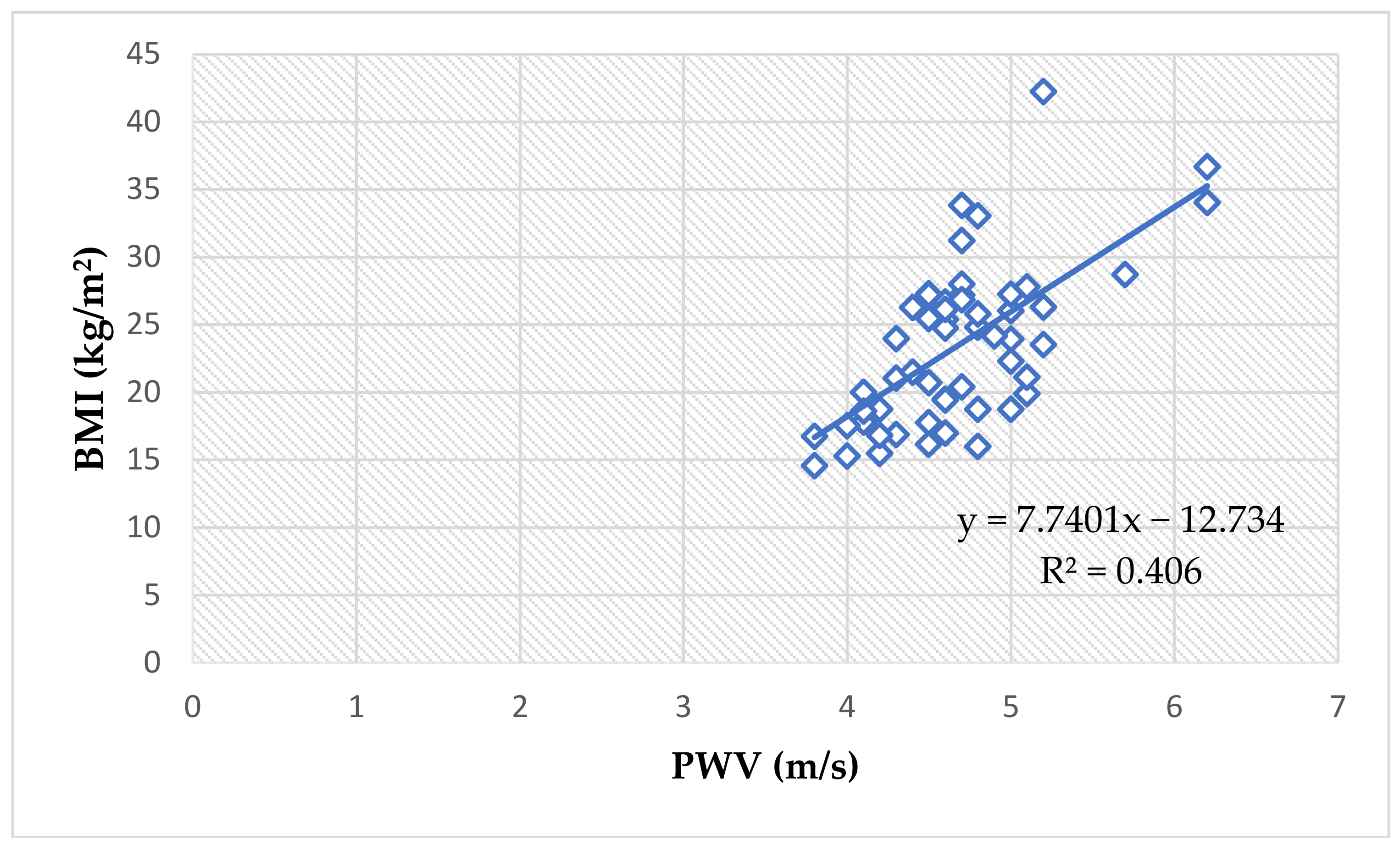
3.2. Pulse Wave Analysis with Regard to BMI
3.3. Pulse Wave Analysis with Regard to Sex
3.4. Pulse Wave Analysis with Regard to Age
3.5. Pulse Wave Analysis with Regard to Tanner Puberty Development Stages
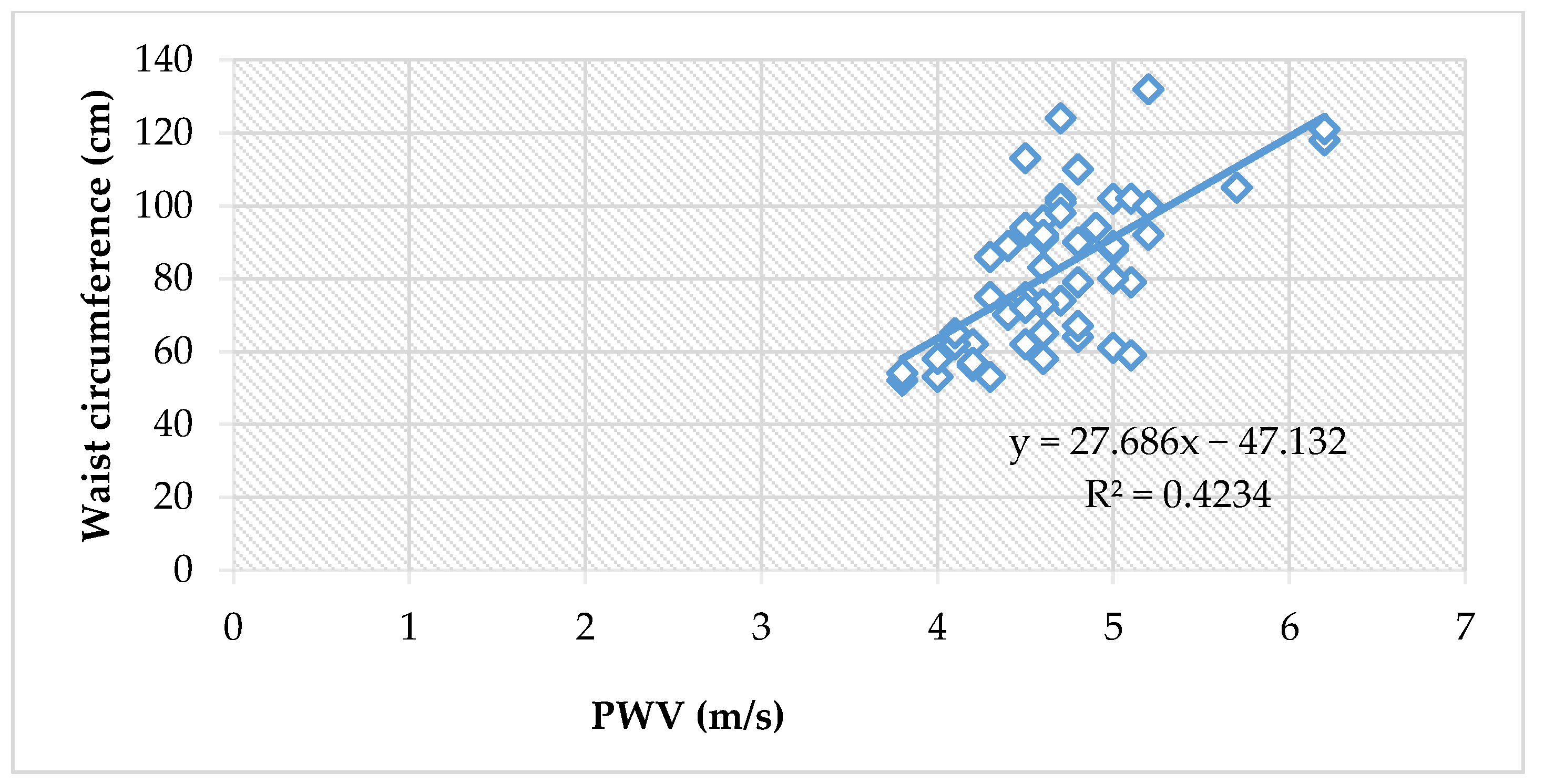
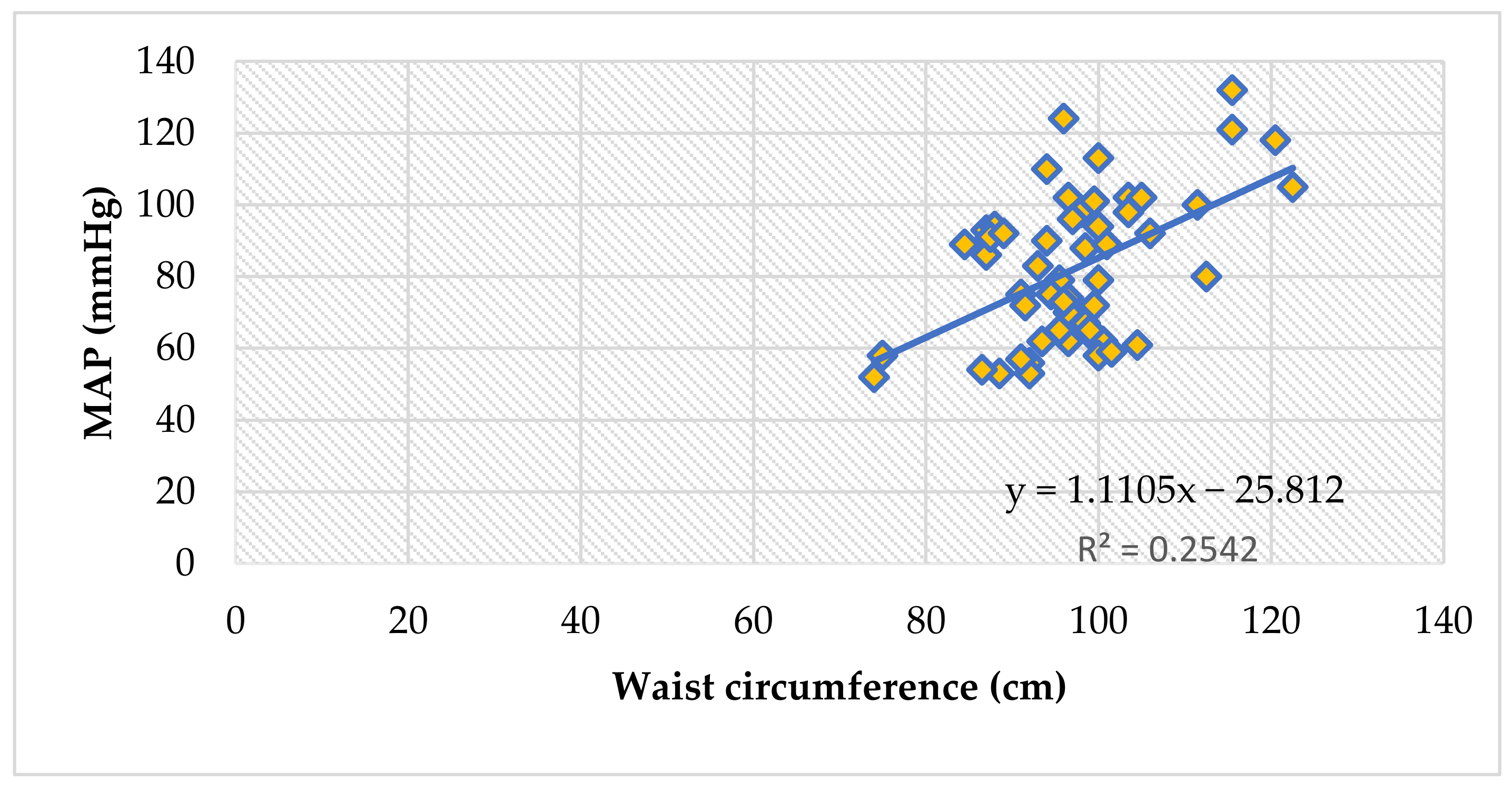
3.6. PWA and the Waist Circumference
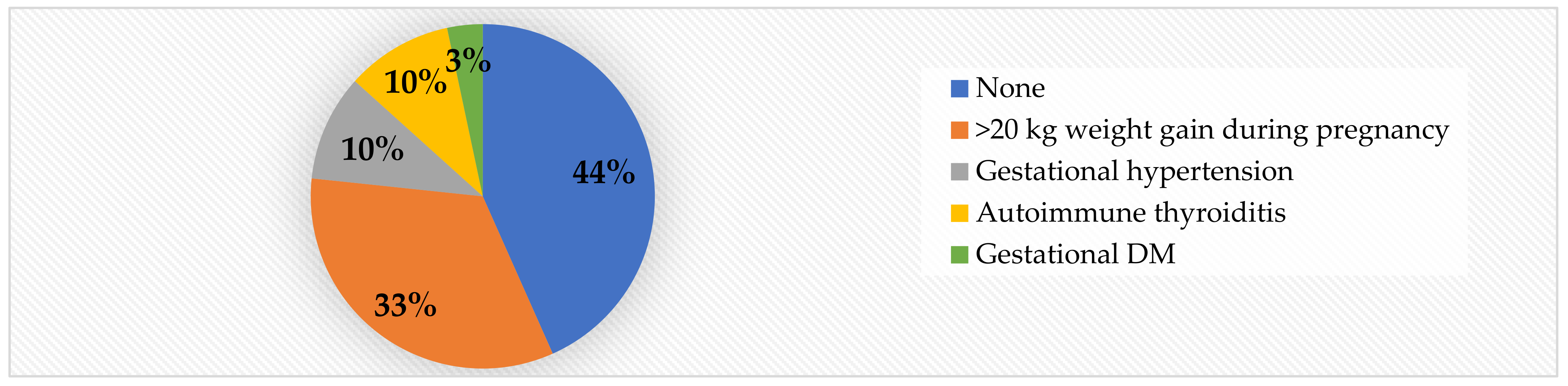
3.7. The Assessment of Risk Factors
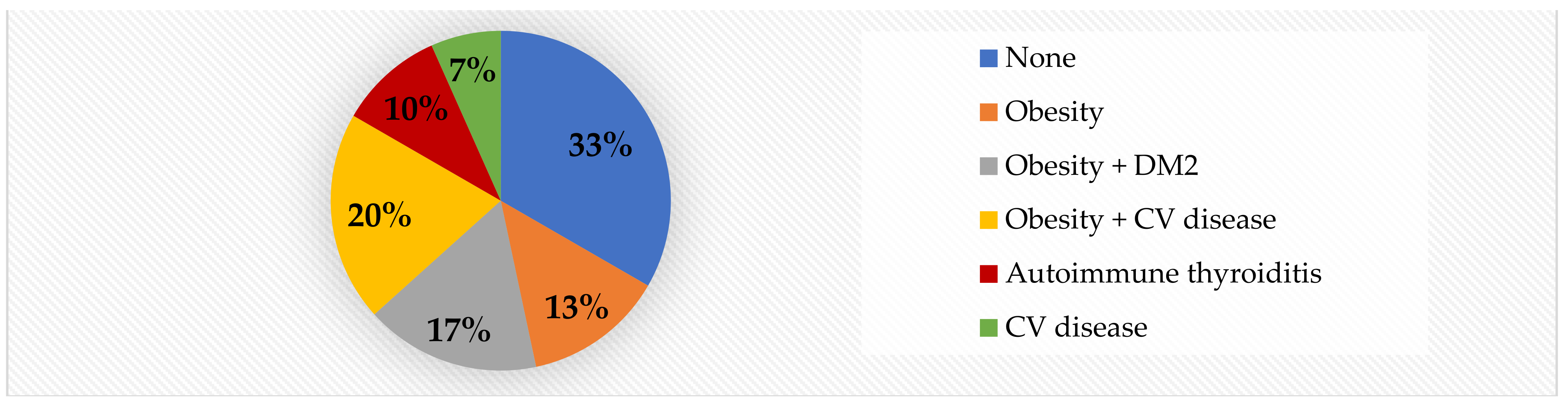
3.7.1. PWA and Risk Factors in the Obese Group
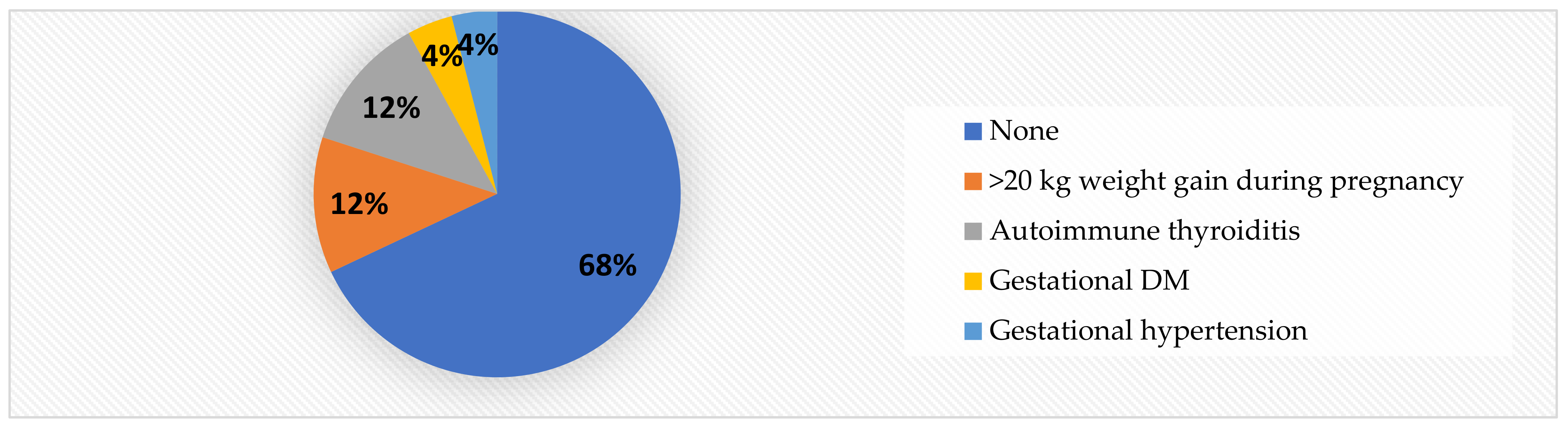
3.7.2. PWA and Risk Factors in the Normal-Weight Group
3.8. The Multilinear Regression Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Aix | augmentation index |
| AP | augmentation pressure |
| BMI | body mass index |
| BP | blood pressure |
| cDBP | central diastolic blood pressure |
| CI | confidence interval |
| CIMT | carotid intima-media thickness |
| cPP | central pulse pressure |
| cSBP | central systolic blood pressure |
| DBP | diastolic blood pressure |
| DM | diabetes mellitus |
| HR | heart rate |
| MAP | mean arterial pressure |
| N-weight | normal weight |
| PWV | pulse wave velocity |
| PP | pulse pressure |
| SBP | systolic blood pressure |
References
- World Health Organization. Fact Sheet. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 12 June 2022).
- Browne, N.T.; Snethen, J.A.; Greenberg, C.S.; Frenn, M.; Kilanowski, J.F.; Gance-Cleveland, B.; Burke, P.; Lewandowski, L. When Pandemics Collide: The Impact of COVID-19 on Childhood Obesity. J. Pediatr. Nurs. 2021, 56, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Stavridou, A.; Kapsali, E.; Panagouli, E.; Thirios, A.; Polychronis, K.; Bacopoulou, F.; Psaltopoulou, T.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Obesity in Children and Adolescents during COVID-19 Pandemic. Children 2021, 8, 135. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef]
- Csige, I.; Ujvárosy, D.; Szabó, Z.; Lőrincz, I.; Paragh, G.; Harangi, M.; Somodi, S. The Impact of Obesity on the Cardiovascular System. J. Diabetes Res. 2018, 2018, 3407306. [Google Scholar] [CrossRef]
- Savant, J.D.; Furth, S.L.; Meyers, K.E.C. Arterial stiffness in children: Pediatric measurement and considerations. Pulse 2015, 2, 69–80. [Google Scholar] [CrossRef]
- Ben-Shlomo, Y.; Spears, M.; Boustred, C.; May, M.; Anderson, S.G.; Benjamin, E.J.; Boutouyrie, P.; Cameron, J.; Chen, C.H.; Cruickshank, J.K. Aortic pulse wave velocity improves cardiovascular event prediction: An individual participant meta-analysis of prospective observational data from 17,635 subjects. J. Am. Coll. Cardiol. 2014, 63, 636–646. [Google Scholar] [CrossRef]
- Townsend, R.R.; Black, H.R.; Chirinos, J.A.; Feig, P.U.; Ferdinand, K.C.; Germain, M.; Rosendorff, C.; Steigerwalt, S.P.; Stepanek, J.A. Clinical use of pulse wave analysis: Proceedings from a symposium sponsored by North American Artery. J. Clin. Hypertens. 2015, 17, 503–513. [Google Scholar] [CrossRef]
- Tomiyama, H.; Yamashina, A. Ankle-Brachial Pressure Index and Pulse Wave Velocity in Cardiovascular Risk Assessment. In Encyclopedia of Cardiovascular Research and Medicine; Vasan, R.S., Sawyer, D.B., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2018; ISBN 978-0-12-805154-2. [Google Scholar]
- Antsiperov, V.E.; Mansurov, G.K.; Bugaev, A. Methods of the Pulse Wave Velocity Estimation based on Pneumatic Blood Pressure Sensor Data and Synchronous ECG Records. In Proceedings of the BIOSTEC 2020—13th International Joint Conference on Biomedical Engineering Systems and Technologies, Valetta, Malta, 24–26 February 2020. [Google Scholar] [CrossRef]
- Ding, F.H.; Fan, W.X.; Zhang, R.Y.; Zhang, Q.; Li, Y.; Wang, J.G. Validation of the noninvasive assessment of central blood pressure by the SphygmoCor and Omron devices against the invasive catheter measurement. Am. J. Hypertens. 2011, 24, 1306–1311. [Google Scholar] [CrossRef] [Green Version]
- Reusz, G.S.; Cseprekal, O.; Temmar, M.; Kis, E.; Cherif, A.B.; Thaleb, A.; Fekete, A.; Szabó, A.J.; Benetos, A.; Salvi, P. Reference values of pulse wave velocity in healthy children and teenagers. Hypertension 2010, 56, 217–224. [Google Scholar] [CrossRef]
- Ohyama, Y.; Ambale-Venkatesh, B.; Noda, C.; Chugh, A.R.; Teixido-Tura, G.; Kim, J.Y.; Donekal, S.; Yoneyama, K.; Gjesdal, O.; Redheuil, A.; et al. Association of Aortic Stiffness with Left Ventricular Remodeling and Reduced Left Ventricular Function Measured by Magnetic Resonance Imaging: The Multi-Ethnic Study of Atherosclerosis. Circ. Cardiovasc. Imaging 2016, 9, e004426. [Google Scholar] [CrossRef] [PubMed]
- Weber, T.; Wassertheurer, S.; Rammer, M.; Maurer, E.; Hametner, B.; Mayer, C.C.; Kropf, J.; Eber, B. Validation of a brachial cuff-based method for estimating central systolic blood pressure. Hypertension 2011, 58, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, M.; Kario, K. Review: Role of the augmentation index in hypertension. TACA 2008, 2, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Wilenius, M.; Tikkakoski, A.J.; Tahvanainen, A.M.; Haring, A.; Koskela, J.; Huhtala, H.; Kähönen, M.; Kööbi, T.; Mustonen, J.T.; Pörsti, I.H. Central wave reflection is associated with peripheral arterial resistance in addition to arterial stiffness in subjects without antihypertensive medication. BMC Cardiovasc. Disord. 2016, 16, 131. [Google Scholar] [CrossRef]
- Qi, Z.; Ding, S. Obesity-associated sympathetic overactivity in children and adolescents: The role of catecholamine resistance in lipid metabolism. J. Pediatr. Endocrinol. Metab. 2016, 29, 113–125. [Google Scholar] [CrossRef]
- Močnik, M.; Nikolić, S.; Varda, N.M. Arterial Compliance Measurement in Overweight and Hypertensive Children. Indian J. Pediatr. 2016, 83, 510–516. [Google Scholar] [CrossRef]
- Jakab, A.E.; Hidvégi, E.V.; Illyés, M.; Cziráki, A.; Kalmár, T.; Maróti1, Z.; Bereczki, C. Childhood Obesity: Does it Have Any Effect on Young Arteries? Front. Pediatr. 2020, 8, 389. [Google Scholar] [CrossRef]
- Coutinho, T.; Bailey, K.R.; Turner, S.T.; Kullo, I.J. Arterial stiffness is associated with increase in blood pressure over time in treated hypertensives. J. Am. Soc. Hypertens. 2014, 6, 414–421. [Google Scholar] [CrossRef]
- Urbina, E.M.; Khoury, P.R.; McCoy, C.; Daniels, S.R.; Kimball, T.R.; Dolan, L.M. Cardiac and vascular consequences of pre-hypertension in youth. J. Clin. Hypertens. 2011, 13, 332–342. [Google Scholar] [CrossRef]
- Urbina, E.M.; Kimball, T.R.; Khoury, P.R.; Daniels, S.R.; Dolan, L.M. Increased arterial stiffness is found in adolescents with obesity or obesity-related type 2 diabetes mellitus. J. Hypertens. 2010, 28, 1692–1698. [Google Scholar] [CrossRef]
- Cheung, Y.F. Arterial stiffness in the young: Assessment, determinants, and implications. Korean Circ. J. 2010, 40, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Downing, R., 2nd; Michael, T.; Place, R.; Hoffman, E.; Visich, P. The Influence of Metabolic Syndrome Risk Factors on Carotid Intima Media Thickness in Children. Glob. Pediatr. Health 2021, 8, 2333794X20987453. [Google Scholar] [CrossRef] [PubMed]
- Velea, I.P.; Albulescu, R.; Arghirescu, S.T. Obezitatea la copil. In Pediatrie-Curs Pentru Studentii Facultătii de Medicină: Obezitatea la Copil; Velea, I., Ed.; Editura Victor Babes: Timisoara, Romania, 2016; pp. 289–297. [Google Scholar]
- Mozos, I.; Maidana, J.P.; Stoian, D.; Stehlik, M. Gender Differences of Arterial Stiffness and Arterial Age in Smokers. Int. J. Environ. Res. Public Health 2017, 14, 565. [Google Scholar] [CrossRef] [PubMed]
- Mihuta, M.-S.; Paul, C.; Ciulpan, A.; Dacca, F.; Velea, I.P.; Mozos, I.; Stoian, D. Subclinical Atherosclerosis Progression in Obese Children with Relevant Cardiometabolic Risk Factors Can Be Assessed through Carotid Intima Media Thickness. Appl. Sci. 2021, 11, 10721. [Google Scholar] [CrossRef]
- Chirita-Emandi, A.; Munteanu, D.; Andreescu, N.; Tutac, P.; Paul, C.; Velea, I.P.; Pusztai, A.M.; Hlistun, V.; Boiciuc, C.; Sacara, V.; et al. No clinical utility of common polymorphisms in IGF1, IRS1, GCKR, PPARG, GCK1 and KCTD1 genes previously associated with insulin resistance in overweight children from Romania and Moldova. J. Pediatr. Endocrinol. Metab. 2019, 32, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Ek, A.; Delisle Nyström, C.; Chirita-Emandi, A.; Tur, J.A.; Nordin, K.; Bouzas, C.; Argelich, E.; Martínez, J.A.; Frost, G.; Garcia-Perez, I.; et al. A randomized controlled trial for overweight and obesity in preschoolers: The More and Less Europe study—An intervention within the STOP project. BMC Public Health 2019, 19, 945. [Google Scholar] [CrossRef]
- Weiss, W.; Gohlisch, C.; Harsch-Gladisch, C.; Tölle, M.; Zidek, W.; van der Giet, M. Oscillometric estimation of central blood pressure: Validation of the Mobil-O-Graph in comparison with the SphygmoCor device. Blood Press. Monit. 2012, 17, 128–131. [Google Scholar] [CrossRef]
- Sarafidis, P.A.; Georgianos, P.I.; Karpetas, A.; Bikos, A.; Korelidou, L.; Tersi, M.; Divanis, D.; Tzanis, G.; Mavromatidis, K.; Liakopoulos, V.; et al. Evaluation of a novel brachial cuff-based oscillometric method for estimating central systolic pressure in hemodialysis patients. Am. J. Nephrol. 2014, 40, 242–250. [Google Scholar] [CrossRef]
- Gotzmann, M.; Hogeweg, M.; Seibert, F.S.; Rohn, B.J.; Bergbauer, M.; Babel, N.; Bauer, F.; Mügge, A.; Westhoff, T.H. Accuracy of fully automated oscillometric central aortic blood pressure measurement techniques. J. Hypertens. 2020, 38, 235–242. [Google Scholar] [CrossRef]
- Araujo-Moura, K.; Souza, L.G.; Mello, G.L.; De Moraes, A.C.F. Blood pressure measurement in pediatric population: Comparison between automated oscillometric devices and mercury sphygmomanometers-a systematic review and meta-analysis. Eur. J. Pediatr. 2022, 181, 9–22. [Google Scholar] [CrossRef]
- Mynard, J.P.; Goldsmith, G.; Springall, G.; Eastaugh, L.; Lane, G.K.; Zannino, D.; Smolich, J.J.; Avolio, A.; Cheung, M.M.H. Central aortic blood pressure estimation in children and adolescents: Results of the KidCoreBP study. J. Hypertens. 2020, 38, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Kim, S.H. Blood pressure measurements and hypertension in infants, children, and adolescents: From the postmercury to mobile devices. Clin. Exp. Pediatr. 2022, 65, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, M.; Murakami, T.; Higashi, K. The accuracy of central blood pressure obtained by oscillometric noninvasive method using Mobil-O-Graph in children and adolescents. J. Hypertens. 2020, 38, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.P. Is Atherosclerosis a Pediatric Disease? In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Mikael, L.R.; Paiva, A.M.G.; Gomes, M.M.; Sousa, A.L.L.; Jardim, P.C.B.V.; Vitorino, P.V.O.; Euzébio, M.B.; Sousa, W.M.; Barroso, W.K.S. Vascular Aging and Arterial Stiffness. Arq. Bras. Cardiol. 2017, 109, 253–258. [Google Scholar] [CrossRef]
- Harbin, M.M.; Hultgren, N.E.; Kelly, A.S.; Dengel, D.R.; Evanoff, N.G.; Ryder, J.R. Measurement of central aortic blood pressure in youth: Role of obesity and sex. Am. J. Hypertens. 2018, 31, 1286–1292. [Google Scholar] [CrossRef]
- Cai, T.Y.; Qasem, A.; Ayer, J.G.; Butlin, M.; O’Meagher, S.; Melki, C.; Marks, G.B.; Avolio, A.; Celermajer, D.S.; Skilton, M.R. Central blood pressure in children and adolescents: Non-invasive development and testing of novel transfer functions. J. Hum. Hypertens. 2017, 31, 831–837. [Google Scholar] [CrossRef]
- Yano, S. Does body height affect vascular function? Hypertens. Res. 2022, 45, 369–371. [Google Scholar] [CrossRef]
- Qiu, Q.; Meng, X.; Li, Y.; Liu, X.; Teng, F.; Wang, Y.; Zang, X.; Wang, Y.; Liang, J. Evaluation of the associations of body height with blood pressure and early-stage atherosclerosis in Chinese adults. J. Clin. Hypertens. 2020, 22, 1018–1024. [Google Scholar] [CrossRef]
- Moon, J.; Hwang, I.C.; Han, S.H. Short stature is associated with higher pulse wave velocity in subjects without overt cardiovascular disease. Medicine 2020, 99, e22219. [Google Scholar] [CrossRef]
- Ahimastos, A.A.; Formosa, M.; Dart, A.M.; Kingwell, B.A. Gender differences in large artery stiffness pre- and post-puberty. J. Clin. Endocrinol. Metab. 2003, 88, 5375–5380. [Google Scholar] [CrossRef]
- Karas, R.H.; Patterson, B.L.; Mendelsohn, M.E. Human vascular smooth muscle cells contain functional estrogen receptor. Circulation 1994, 89, 1943–1950. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Hadoke, P.W.; Mair, I.; Lim, W.G.; Miller, E.; Denvir, M.A.; Smith, L.B. Modulation of neointimal lesion formation by endogenous androgens is independent of vascular androgen receptor. Cardiovasc. Res. 2014, 103, 281–290. [Google Scholar] [CrossRef] [PubMed]
- DuPont, J.J.; Kenney, R.M.; Patel, A.R.; Jaffe, I.Z. Sex differences in mechanisms of arterial stiffness. Br. J. Pharmacol. 2019, 176, 4208–4225. [Google Scholar] [CrossRef] [PubMed]
- Regnault, V.; Thomas, F.; Safar, M.E.; Osborne-Pellegrin, M.; Khalil, R.A.; Pannier, B.; Lacolley, P. Sex difference in cardiovascular risk: Role of pulse pressure amplification. J. Am. Coll. Cardiol. 2012, 59, 1771–1777. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.D.; Cullinane, E.M.; Sady, S.P.; Chenevert, C.; Saritelli, A.L.; Sady, M.A.; Herbert, P.N. Contrasting effects of testosterone and stanozolol on serum lipoprotein levels. JAMA 1989, 261, 1165–1168. [Google Scholar] [CrossRef]
- Webb, C.M.; Elkington, A.G.; Kraidly, M.M.; Keenan, N.; Pennell, D.J.; Collins, P. Effects of oral testosterone treatment on myocardial perfusion and vascular function in men with low plasma testosterone and coronary heart disease. Am. J. Cardiol. 2008, 101, 618–624. [Google Scholar] [CrossRef]
- Dockery, F.; Bulpitt, C.J.; Donaldson, M.; Fernandez, S.; Rajkumar, C. The relationship between androgens and arterial stiffness in older men. JAGS 2003, 51, 1627–1632. [Google Scholar] [CrossRef]
- Hougaku, H.; Fleg, J.L.; Najjar, S.S.; Lakatta, E.G.; Harman, S.M.; Blackman, M.R.; Metter, E.J. Relationship between androgenic hormones and arterial stiffness, based on longitudinal hormone measurements. Am. J. Physiol. Endocrinol. Metab. 2006, 290, E234–E242. [Google Scholar] [CrossRef]
- Qiu, H.; Zhu, Y.; Sun, Z.; Trzeciakowski, J.P.; Gansner, M.; Depre, C.; Vatner, S.F. Short communication: Vascular smooth muscle cell stiffness as a mechanism for increased aortic stiffness with aging. Circ. Res. 2010, 107, 615–619. [Google Scholar] [CrossRef] [Green Version]
- Díaz, A.; Galli, C.; Tringler, M.; Ramírez, A.; Fischer, E.I.C. Reference Values of Pulse Wave Velocity in Healthy People from an Urban and Rural Argentinean Population. Int. J. Hypertens. 2014, 2014, 653239. [Google Scholar] [CrossRef]
- Li, Y.; Staessen, J.; Sheng, C.S.; Huang, Q.F.; O’Rourke, M.; Wang, J.G. Age dependency of peripheral and central systolic blood pressures: Cross-sectional and longitudinal observations in a Chinese population. Hypertens. Res. 2012, 35, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Lentferink, Y.E.; Kromwijk, L.A.J.; van der Aa, M.P.; Knibbe, C.A.J.; van der Vorst, M.M.J. Increased Arterial Stiffness in Adolescents with Obesity. Glob. Pediatr. Health 2019, 25, 6. [Google Scholar] [CrossRef] [PubMed]
- Solorzano, C.M.B.; Helm, K.D.; Patrie, J.T.; Shayya, R.F.; Cook-Andersen, H.L.; Chang, R.J.; McCartney, C.R.; Marshall, J.C. Increased adrenal androgens in overweight peripubertal girls. J. Endocr. Soc. 2017, 1, 538–552. [Google Scholar] [CrossRef] [PubMed]
- Bassali, R.; Waller, J.L.; Gower, B.; Allison, J.; Davis, C.L. Utility of waist circumference percentile for risk evaluation in obese children. Int. J. Pediatric. Obes. 2010, 5, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Kahn, H.S.; Mei, Z.; Grummer-Strawn, L.M.; Dietz, W.H.; Srinivasan, S.R.; Berenson, G.S. Relation of body mass index and waist-to-height ratio to cardiovascular disease risk factors in children and adolescents: The Bogalusa Heart Study. Am. J. Clin. Nutr. 2007, 86, 33–40. [Google Scholar] [CrossRef]
- Golab, B.; Santos, S.; Voerman, E.; Lawlor, D.; Jaddoe, V.; Gaillard, R. Common pregnancy complications and risk of childhood obesity-influence of maternal obesity: An individual participant data. Lancet Child Adolesc. Health 2019, 2, 812. [Google Scholar] [CrossRef]
- Crispi, F.; Bijnens, B.; Figueras, F.; Bartrons, J.; Eixarch, E.; Le Noble, F.; Ahmed, A.; Gratacós, E. Fetal growth restriction results in remodeled and less efficient hearts in children. Circulation 2010, 121, 2427–2436. [Google Scholar] [CrossRef]
- Crispi, F.; Miranda, J.; Gratacós, E. Long-term cardiovascular consequences of fetal growth restriction: Biology, clinical implications, and opportunities for prevention of adult disease. Am. J. Obstet. Gynecol. 2018, 218, S869–S879. [Google Scholar] [CrossRef]
- Ambrose, J.A.; Barua, R.S. The pathophysiology of cigarette smoking and cardiovascular disease: An update. J. Am. Coll. Cardiol. 2004, 43, 1731–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holley, S.; Hill, C.M.; Stevenson, J. An hour less sleep is a risk factor for childhood conduct problems. Child Care Health Dev. 2011, 37, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, A.C.; Carmo, A.; Dos Santos, L.C. Associations between sleep practices and social behavior of children and adolescents: A systematic review. J. Public Health 2022, 30, 1101–1112. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute. How Much Sleep Is Enough? 2012. Available online: https://www.nhlbi.nih.gov/node/4606 (accessed on 22 June 2022).
- National Sleep Foundation. Sleep in America Poll. 2014. Available online: https://sleepfoundation.org/sites/default/files/2014-NSF-Sleep-in-America-poll-summary-of-findings---FINAL-Updated-3-26-14-.pdf (accessed on 22 June 2022).
- Garaulet, M.; Ortega, F.B.; Ruiz, J.R.; Rey-López, J.P.; Béghin, L.; Manios, Y.; Cuenca-García, M.; Plada, M.; Diethelm, K.; Kafatos, A.; et al. Short sleep duration is associated with increased obesity markers in European adolescents: Effect of physical activity and dietary habits. The HELENA study. Int. J. Obes. 2011, 35, 1308–1317. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Zheng, L.; Wang, J.; Zhang, X.; Zhang, X.; Li, J.; Sun, Y. Epidemiological evidence for the link between sleep duration and high blood pressure: A systematic review and meta-analysis. Sleep Med. 2013, 14, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Sunbul, M.; Kanar, B.G.; Durmus, E.; Kivrak, T.; Sari, I. Acute sleep deprivation is associated with increased arterial stiffness in healthy young adults. Sleep Breath. 2014, 18, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Kline, C.E.; Taylor, C.; Kriska, A.M.; Barinas-Mitchell, E. Short Sleep Duration is Associated with Greater Arterial Stiffness Independent of Sleep Quality. Circulation 2019, 139, AP277. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Mera, R.M.; Peñaherrera, E.; Costa, A.F.; Peñaherrera, R.; Castillo, P.R. On the Association Between Sleep Quality and Arterial Stiffness: A Population Study in Community-Dwelling Older Adults Living in Rural Ecuador (The Atahualpa Project). J. Clin. Sleep Med. 2019, 15, 1101–1106. [Google Scholar] [CrossRef]
- Yang, H.; Haack, M.; Gautam, S.; Meier-Ewert, H.K.; Mullington, J.M. Repetitive exposure to shortened sleep leads to blunted sleep-associated blood pressure dipping. J. Hypertens. 2017, 35, 1187–1194. [Google Scholar] [CrossRef]
- St-Onge, M.P.; Campbell, A.; Aggarwal, B.; Taylor, J.L.; Spruill, T.M.; Roy Choudhury, A. Mild sleep restriction increases 24-hour ambulatory blood pressure in premenopausal women with no indication of mediation by psychological effects. Am. Heart J. 2020, 223, 12–22. [Google Scholar] [CrossRef]
- Sparano, S.; Lauria, F.; Ahrens, W.; Fraterman, A.; Thumann, B.; Iacoviello, L.; Marild, S.; Michels, N.; Molnar, D.; Moreno, L.A.; et al. Sleep duration and blood pressure in children: Analysis of the pan-European IDEFICS cohort. J. Clin. Hypertens. 2019, 21, 572–578. [Google Scholar] [CrossRef] [Green Version]
- Epure, A.M.; Rios-Leyvraz, M.; Anker, D.; Di Bernardo, S.; Da Costa, B.R.; Chiolero, A.; Sekarski, N. Risk factors during first 1,000 days of life for carotid intima-media thickness in infants, children, and adolescents: A systematic review with meta-analyses. PLoS Med. 2020, 17, e1003414. [Google Scholar] [CrossRef]
- Skilton, M.R.; Siitonen, N.; Würtz, P.; Viikari, J.S.; Juonala, M.; Seppälä, I.; Laitinen, T.; Lehtimäki, T.; Taittonen, L.; Kähönen, M.; et al. High birth weight is associated with obesity and increased carotid wall thickness in young adults: The cardiovascular risk in young Finns study. Arter. Thromb. Vasc. Biol. 2014, 34, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Fall, C.H.D.; Barker, D.J.P.; Osmond, C.; Winter, P.D.; Clark, P.M.S.; Hales, C.N. Relation of infant feeding to adult serum cholesterol concentration and death from ischaemic heart disease. BMJ 1992, 304, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.M.; Ebrahim, S.; Griffin, M.; Davey-Smith, G.; Nicolaides, A.N.; Georgiou, N. Breastfeeding and atherosclerosis: Intima-media thickness and plaques at 65-year follow-up of the Boyd Orr cohort. Arter. Thromb. Vasc. Biol. 2005, 25, 1482–1488. [Google Scholar] [CrossRef]
- Corica, D.; Aversa, T.; Valenzise, M.; Messina, M.F.; Alibrandi, A.; De Luca, F.; Wasniewska, M. Does family history of obesity, cardiovascular, and metabolic diseases influence onset and severity of childhood obesity? Front. Endocrinol. 2018, 9, 187. [Google Scholar] [CrossRef] [PubMed]
- Batista, M.S.; Mill, J.G.; Pereira, T.S.; Fernandes, C.D.; Molina Mdel, C. Factors associated with arterial stiffness in children aged 9–10 years. Rev. Saude Publica 2015, 49, 23. [Google Scholar] [CrossRef]
- Keane, E.; Li, X.; Harrington, J.M.; Fitzgerald, A.P.; Perry, I.J.; Kearney, P.M. Physical Activity, Sedentary Behavior and the Risk of Overweight and Obesity in School-Aged Children. Pediatr. Exerc. Sci. 2017, 29, 408–418. [Google Scholar] [CrossRef]
- Fernandes, R.A.; Júnior, I.F.F.; Codogno, J.S.; Christofaro, D.G.D.; Monteiro, H.L.; Lopes, D.M.R. Resting hearth rate is associated with blood pressure in male children and adolescents. J. Pediatr. 2011, 158, 634–637. [Google Scholar] [CrossRef]
- Al-Qurashi, M.M.; El-Mouzan, M.I.; Al-Herbish, A.S.; Al-Salloum, A.A.; Al-Omar, A.A. Age related reference ranges of heart rate for Saudi children and adolescents. Saudi Med. J. 2009, 30, 926–931. [Google Scholar]
- Rabbia, F.; Silke, B.; Conterno, A.; Grosso, T.; De Vito, B.; Rabbone, I.; Chiandussi, L.; Veglio, F. Assesssment of cardiac autonomic modulation during adolescente obesity. Obes. Res. 2003, 11, 541–548. [Google Scholar] [CrossRef]
- Nagai, N.; Matsumoto, T.; Kita, H.; Toshio Moritani, T. Autonomic Nervous System Activity and the State and Development of Obesity in Japanese School Children. Obes. Res. 2012, 11, 25–32. [Google Scholar] [CrossRef]
- Harris, R.A.; Nishiyama, S.K.; Wray, D.W.; Richardson, R.S. Ultrasound assessment of flow-mediated dilation. Hypertension 2010, 55, 1075–1085. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, D.; Coll, M.; Guerrero, R.; Henao, L. Flow mediated vasodilation in overweight children. Rev. Chil. Pediatr. 2015, 86, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y. Flow-Mediated Dilatation in Obese Children. Clin. Pediatr. Endocrinol. 2003, 12, 43–48. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Shapiro–Wilks Test for Normality of Distribution | Accepted Normality p-Value | Rejected Normality p-Value | Mean | 95% CI | Median | 95% CI | SD |
|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | - | 0.0003 | - | - | 26.5 | 25.7–27.3 | 4.41 |
| Weight (kg) | - | 0.03 | - | - | 63 | 59.2–73.6 | 21.5 |
| Height (m) | 0.22 | - | 1.55 | 1.5–1.64 | - | - | 0.15 |
| Waist circumference (cm) | 0.38 | - | 97.61 | 92.42–102.51 | - | - | 13.9 |
| Weight at birth (g) | 0.11 | - | 3058 | 2818–3297 | - | - | 642.52 |
| PWA (m/s) | - | 0.0003 | - | - | 4.7 | 4.61–4.92 | 0.47 |
| AIx % | 0.65 | - | 24.82 | 20.61–28.92 | - | 11.12 | |
| SBP (mmHg) | - | 0.004 | - | - | 118 | 114.1–125 | 11.88 |
| DBP (mmHg) | 0.85 | - | 76.49 | 72.51–80.43 | - | - | 10.56 |
| MAP (mmHg) | 0.07 | - | 99.31 | 95.6–103 | - | - | 9.96 |
| cSBP (mmHg) | - | 0.006 | - | - | 113 | 107–117 | 11.36 |
| cDBP (mmHg) | 0.63 | - | 78.12 | 74.3–81.89 | - | - | 10.12 |
| cPP (mmHg) | 0.35 | - | 37.11 | 33.21–41.02 | - | - | 10.47 |
| HR (b/min) | 0.5 | - | 89.31 | 85.2–93.52 | - | - | 11.08 |
| Shapiro–Wilks Test for Normality of Distribution | Accepted Normality p-Value | Rejected Normality p-Value | Mean | 95% CI | Median | 95% CI | SD |
|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | - | <0.0001 | - | - | 18.6 | 16.82–19.52 | 4.22 |
| Weight (kg) | 0.22 | - | 41.32 | 36–46.7 | - | - | 12.71 |
| Height (m) | - | 0.02 | - | - | 1.52 | 1.41–1.52 | 0.18 |
| Waist circumference (cm) | 0.23 | - | 63.71 | 60.42–67.11 | - | - | 8.21 |
| Weight at birth (g) | 0.94 | - | 3322 | 3037.5–3606.4 | - | - | 689 |
| PWA (m/s) | 0.33 | 4.38 | 4.2–4.6 | - | - | 0.43 | |
| AIx % | 0.51 | - | 21.82 | 17.7–25.9 | - | - | 9.79 |
| SBP (mmHg) | 0.05 | - | 113.63 | 109.9–117.3 | - | - | 8.91 |
| DBP (mmHg) | - | 0.002 | - | - | 78 | 75–81 | 8.16 |
| MAP (mmHg) | - | 0.02 | - | - | 96.5 | 92.21–98.89 | 8.1 |
| cSBP (mmHg) | 0.29 | - | 100.31 | 96–104.6 | - | - | 10.42 |
| cDBP (mmHg) | 0.56 | - | 68.32 | 64.8–71.7 | - | - | 8.38 |
| cPP (mmHg) | 0.02 | - | - | 31 | 29.12–33.81 | 5.73 | |
| HR (b/min) | 0.61 | - | 83.74 | 81–86.44 | - | - | 6.51 |
| PWV m/s | Aix % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg | |
|---|---|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | 0.58 | 0.21 | 0.49 | 0.26 | 0.31 | 0.24 | 0.64 | 0.56 | 0.28 |
| p-value | <0.0001 | 0.11 | 0.0001 | 0.04 | 0.02 | 0.07 | <0.0001 | <0.0001 | 0.03 |
| Weight (kg) | 0.68 | 0.29 | 0.61 | 0.36 | 0.35 | 0.22 | 0.67 | 0.59 | 0.30 |
| p-value | <0.0001 | 0.03 | <0.0001 | 0.006 | 0.008 | 0.1 | <0.0001 | <0.0001 | 0.02 |
| Height (m) | 0.58 | 0.25 | 0.57 | 0.43 | 0.3 | 0.03 | 0.5 | 0.51 | 0.2 |
| p-value | <0.0001 | 0.06 | <0.0001 | 0.001 | 0.01 | 0.79 | 0.0001 | <0.0001 | 0.13 |
| Group | Sex | PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg |
|---|---|---|---|---|---|---|---|---|---|---|
| Obese | Boys | 4.75 | 19.31 | 120.31 | 75.93 | 98.12 | 85.06 | 113.68 | 76.68 | 41.5 |
| Girls | 4.78 | 30.3 | 117 | 75 | 97 | 95.53 | 112.84 | 79.07 | 33.93 | |
| p-value | 0.54 | 0.01 | 0.89 | 0.98 | 0.9 | 0.005 | 0.43 | 0.66 | 0.6 | |
| N-weight | Boys | 4.45 | 22.41 | 114.33 | 76.83 | 95.58 | 83.91 | 100.58 | 68 | 32 |
| Girls | 4.4 | 21.23 | 115 | 76 | 96.5 | 83.53 | 100.15 | 68.53 | 31.07 | |
| p-value | 0.6 | 0.7 | 0.7 | 0.49 | 0.74 | 0.88 | 0.27 | 0.87 | 0.33 |
| PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg | |
|---|---|---|---|---|---|---|---|---|---|
| Obese girls | 4.78 | 30.3 | 117 | 75 | 97 | 95.53 | 112.84 | 79.07 | 33.93 |
| N-weight girls | 4.4 | 21.23 | 115 | 76 | 96.5 | 83.53 | 100.15 | 68.53 | 31.07 |
| p-value | 0.016 | 0.02 | 0.09 | 0.93 | 0.39 | 0.004 | 0.006 | 0.01 | 0.39 |
| Obese boys | 4.75 | 19.31 | 120.31 | 75.93 | 98.12 | 85.06 | 113.68 | 76.68 | 41.5 |
| N-weight boys | 4.45 | 22.41 | 114.33 | 76.83 | 95.58 | 83.91 | 100.58 | 68 | 32 |
| p-value | 0.03 | 0.43 | 0.1 | 0.81 | 0.46 | 0.69 | 0.001 | 0.02 | 0.09 |
| n | PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg | |
|---|---|---|---|---|---|---|---|---|---|---|
| <12 years old | 11 | 4.5 | 25 | 118.91 | 70.91 | 94.91 | 91.81 | 111.63 | 73.09 | 38.36 |
| 12–15 years old | 13 | 4.8 | 24.53 | 119 | 78.38 | 100.11 | 89.15 | 117 | 79.53 | 36 |
| ≥16 years old | 6 | 4.9 | 25.16 | 123.5 | 82.66 | 102.25 | 85.16 | 117.5 | 84.33 | 37.16 |
| n | PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| <12 years | Obese | 11 | 4.5 | 25 | 118.91 | 70.91 | 94.91 | 91.81 | 111.63 | 73.09 | 38.36 |
| N-weight | 12 | 4.2 | 21 | 109.41 | 73.5 | 91.45 | 83.75 | 96.5 | 66.5 | 30.5 | |
| p-value | 0.03 | 0.38 | 0.06 | 0.55 | 0.41 | 0.052 | 0.005 | 0.12 | 0.02 |
| n | PWV m/s | Aix % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 12–15 years | Obese | 13 | 4.8 | 24.53 | 121.8 | 78.38 | 100.11 | 89.15 | 113.76 | 79.53 | 36 |
| N-weight | 10 | 4.5 | 20.7 | 115.8 | 77.4 | 96.6 | 82.3 | 102.8 | 67.9 | 33.6 | |
| p-value | 0.007 | 0.42 | 0.03 | 0.77 | 0.2 | 0.03 | 0.003 | 0.002 | 0.48 |
| Tanner Stage | PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg |
|---|---|---|---|---|---|---|---|---|---|
| I | 4.5 | 22.31 | 110.02 | 74.22 | 95.7 | 91.42 | 110 | 75.81 | 34.54 |
| II, III | 4.8 | 23.52 | 121.73 | 73 | 97.39 | 88.71 | 114.33 | 74.62 | 39.21 |
| IV, V | 4.85 | 28.33 | 126.19 | 82.5 | 104.3 | 88.74 | 118 | 84.32 | 36.14 |
| Tanner I Subjects | n | PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg |
|---|---|---|---|---|---|---|---|---|---|---|
| Obese | 7 | 4.5 | 22.31 | 110.02 | 74.22 | 95.7 | 91.42 | 110 | 75.81 | 34.54 |
| Normal weight | 9 | 4.1 | 17.4 | 109 | 72 | 89.2 | 83.7 | 92 | 63.3 | 29 |
| p-value | 0.01 | 0.32 | 0.18 | 0.67 | 0.25 | 0.17 | 0.006 | 0.02 | 0.13 |
| Tanner II, III Subjects | n | PWV m/s | Aix % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg |
|---|---|---|---|---|---|---|---|---|---|---|
| Obese | 13 | 4.8 | 23.52 | 121.73 | 73 | 97.39 | 88.71 | 114.33 | 76.62 | 39.21 |
| Normal weight | 10 | 4.5 | 23.9 | 116.6 | 73 | 97.3 | 82.9 | 106.2 | 72.2 | 35.3 |
| p-value | 0.95 | 0.94 | 0.08 | 0.19 | 0.97 | 0.06 | 0.02 | 0.5 | 0.27 |
| Tanner IV, V Subjects | n | PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg |
|---|---|---|---|---|---|---|---|---|---|---|
| Obese | 10 | 4.85 | 28.33 | 126.19 | 82.5 | 104.3 | 88.74 | 118 | 84.32 | 36.14 |
| Normal weight | 6 | 4.6 | 24.6 | 117 | 79 | 96.2 | 85 | 103.1 | 69.1 | 32.6 |
| p-value | 0.16 | 0.5 | 0.34 | 0.37 | 0.17 | 0.54 | 0.02 | 0.002 | 0.53 |
| PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg | |
|---|---|---|---|---|---|---|---|---|---|
| Obese | ρ = 0.5 | r = 0.24 | ρ = 0.48 | r = 0.53 | r = 0.57 | r = −0.07 | ρ = 0.51 | r = 0.49 | r = 0.11 |
| p-value | 0.004 | 0.19 | 0.007 | 0.003 | 0.001 | 0.69 | 0.004 | 0.005 | 0.54 |
| Normal weight | r = 0.61 | r = 0.26 | r = 0.62 | ρ = 0.37 | ρ = 0.49 | r = −0.21 | r = 0.48 | r = 0.32 | ρ = 0.24 |
| p-value | 0.001 | 0.19 | 0.0009 | 0.06 | 0.01 | 0.32 | 0.01 | 0.11 | 0.23 |
| Risk Factors | n | PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mother’s health during pregnancy | Risk during pregnancy | 17 | 4.8 | 29.21 | 121.12 | 78.53 | 102.29 | 90.31 | 116.04 | 79.73 | 38.33 |
| No risk | 13 | 4.6 | 19.02 | 114.07 | 73.71 | 95.33 | 88.11 | 108.02 | 76.12 | 35.52 | |
| p-value | 0.02 | 0.009 | 0.01 | 0.21 | 0.053 | 0.57 | 0.12 | 0.32 | 0.48 | ||
| Birth weight | <2500 g | 7 | 4.6 | 22.81 | 114.04 | 78.1 | 99.42 | 89.82 | 114.41 | 78.71 | 42.08 |
| >3500 g | 8 | 4.75 | 28.68 | 122.11 | 73.02 | 98.23 | 90.31 | 111.54 | 75.05 | 41.55 | |
| Normal | 15 | 4.7 | 23.63 | 118.02 | 77.65 | 99.62 | 88.55 | 113.43 | 79.54 | 40.03 | |
| <2500 g vs. N * | 0.85 | 0.88 | 0.59 | 0.94 | 0.96 | 0.82 | 0.82 | 0.85 | 0.64 | ||
| p-value: | >3500 g vs. N * | 0.79 | 0.26 | 0.56 | 0.34 | 0.94 | 0.7 | 0.77 | 0.33 | 0.2 | |
| <2500 g vs. >3500 g * | 1 | 0.37 | 0.59 | 0.39 | 0.89 | 0.92 | 0.81 | 0.5 | 0.37 | ||
| Postnatal nutrition | Formula | 14 | 4.8 | 27.11 | 121.55 | 78.52 | 100.03 | 90.22 | 112.52 | 79.84 | 36.31 |
| Breastfed | 16 | 4.7 | 22.82 | 117.04 | 74.64 | 94.73 | 88.55 | 113.02 | 76.66 | 37.72 | |
| p-value | 0.39 | 0.29 | 0.41 | 0.32 | 0.11 | 0.69 | 0.44 | 0.39 | 0.72 | ||
| Family history | Risk factors present | 20 | 4.75 | 27.04 | 118.52 | 75.64 | 99.41 | 99.14 | 114.57 | 76.86 | 39.52 |
| No risk factor | 10 | 4.65 | 20.42 | 116.05 | 78.21 | 99.11 | 88.45 | 110.55 | 80.72 | 32.21 | |
| p-value | 0.38 | 0.96 | 0.48 | 0.98 | 0.92 | 0.54 | 0.58 | 0.33 | 0.07 | ||
| Smoking | Smoking | 5 | 5 | 31.81 | 125.02 | 85.82 | 108.23 | 93.84 | 119.04 | 86.81 | 32.82 |
| Passive smoking | 10 | 4.8 | 26.07 | 118.07 | 77.66 | 99.65 | 87.22 | 115.43 | 78.22 | 40.44 | |
| No exposure to smoke | 20 | 4.3 | 22.82 | 116.04 | 73.93 | 97.05 | 88.71 | 113.06 | 75.97 | 37.34 | |
| p-value: | Smoking vs. no exposure * | 0.013 | 0.12 | 0.015 | 0.02 | 0.02 | 0.38 | 0.49 | 0.03 | 0.41 | |
| Passive smoking vs. no exposure * | 0.06 | 0.57 | 0.5 | 0.48 | 0.12 | 0.78 | 0.64 | 0.66 | 0.63 | ||
| Smoking vs. passive smoking * | 0.67 | 0.36 | 0.32 | 0.18 | 0.92 | 0.37 | 0.66 | 0.15 | 0.24 | ||
| Physical activity | Sedentary | 18 | 4.7 | 23.55 | 118.07 | 77.33 | 100.55 | 87.48 | 113 | 78.85 | 38.11 |
| Normal physical activity | 12 | 4.7 | 26.84 | 118.02 | 75.21 | 97.51 | 92.06 | 112.03 | 77 | 35.56 | |
| p-value | 0.65 | 0.43 | 0.6 | 0.6 | 0.43 | 0.28 | 0.47 | 0.65 | 0.52 | ||
| Sleep | Sleep issues | 13 | 5 | 24.8 | 124.98 | 79.61 | 103.44 | 91.13 | 107.03 | 76.33 | 39.72 |
| Normal sleep | 17 | 4.6 | 24.82 | 114.08 | 74.11 | 96.25 | 86.91 | 117 | 80.51 | 35 | |
| p-value | 0.004 | 0.99 | 0.008 | 0.16 | 0.04 | 0.3 | 0.017 | 0.26 | 0.22 | ||
| Risk Factors | n | PWV m/s | AIx % | SBP mmHg | DBP mmHg | MAP mmHg | HR b/min | cSBP mmHg | cDBP mmHg | cPP mmHg | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mother’s health during pregnancy | Present | 8 | 4.5 | 26.12 | 115.62 | 79.55 | 96.52 | 85.83 | 102.11 | 68.58 | 30 |
| Not present | 17 | 4.3 | 19.71 | 112.63 | 75.03 | 94.55 | 82.77 | 99.52 | 68.14 | 31 | |
| p-value | 0.29 | 0.94 | 0.44 | 0.11 | 0.18 | 0.26 | 0.57 | 0.89 | 0.86 | ||
| Birth weight | <2500 g * | 2 | - | - | - | - | - | - | - | - | - |
| >3500 g | 10 | 4.7 | 25.2 | 111.34 | 81.5 | 99.22 | 83.82 | 104.87 | 70.83 | 31.55 | |
| Normal | 13 | 4.2 | 19.71 | 116.77 | 78 | 93.51 | 83.74 | 98.04 | 67.11 | 34.31 | |
| p-value | 0.048 | 0.18 | 0.16 | 0.18 | 0.05 | 0.96 | 0.12 | 0.32 | 0.27 | ||
| Postnatal food | Formula | 9 | 4.5 | 24.21 | 115.35 | 78 | 96.33 | 84.71 | 103.7 | 70.21 | 34 |
| Breastfed | 16 | 4.4 | 20.44 | 112.62 | 77 | 94 | 83.17 | 98.42 | 67.14 | 31.49 | |
| p-value | 0.6 | 0.36 | 0.47 | 0.73 | 0.92 | 0.55 | 0.22 | 0.39 | 0.3 | ||
| Family history | Risk factors present | 7 | 4.5 | 25.73 | 115.56 | 81 | 96.51 | 85.82 | 102.72 | 69.35 | 30 |
| No risk factor | 18 | 4.4 | 20.21 | 112.85 | 75.5 | 95 | 82.84 | 99.41 | 67.83 | 31 | |
| p-value | 0.39 | 0.22 | 0.5 | 0.08 | 0.15 | 0.32 | 0.49 | 0.71 | 0.73 | ||
| Smoking | Smoking * | 2 | - | - | - | - | - | - | - | - | - |
| Passive smoking | 8 | 4.8 | 31 | 118.41 | 81 | 99.61 | 86.41 | 106.23 | 73.22 | 31 | |
| No exposure to smoke | 15 | 4.2 | 17 | 110.82 | 75 | 92.14 | 82.11 | 97 | 65.53 | 30.55 | |
| p-value | 0.02 | 0.009 | 0.03 | 0.01 | 0.02 | 0.12 | 0.03 | 0.02 | 0.57 | ||
| Physical activity | Sedentary | 8 | 4.9 | 28.71 | 119 | 81.55 | 100.21 | 87.63 | 106.31 | 74.84 | 36.53 |
| Normal physical activity | 17 | 4.3 | 18.5 | 114 | 75.05 | 94.55 | 81.82 | 97.5 | 65.14 | 30 | |
| p-value | 0.01 | 0.01 | 0.006 | 0.003 | 0.004 | 0.03 | 0.04 | 0.004 | 0.002 | ||
| Sleep | Sleep issues | 5 | 5 | 27.81 | 120.81 | 82.04 | 100.55 | 86.22 | 107.43 | 72.64 | 37.62 |
| Normal sleep | 20 | 4.35 | 20.33 | 111.84 | 76.12 | 95.72 | 83.13 | 98.61 | 67.25 | 31.11 | |
| p-value | 0.04 | 0.13 | 0.04 | 0.01 | 0.01 | 0.35 | 0.09 | 0.2 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihuta, M.S.; Paul, C.; Borlea, A.; Cepeha, C.M.; Velea, I.P.; Mozos, I.; Stoian, D. The Oscillometric Pulse Wave Analysis Is Useful in Evaluating the Arterial Stiffness of Obese Children with Relevant Cardiometabolic Risks. J. Clin. Med. 2022, 11, 5078. https://doi.org/10.3390/jcm11175078
Mihuta MS, Paul C, Borlea A, Cepeha CM, Velea IP, Mozos I, Stoian D. The Oscillometric Pulse Wave Analysis Is Useful in Evaluating the Arterial Stiffness of Obese Children with Relevant Cardiometabolic Risks. Journal of Clinical Medicine. 2022; 11(17):5078. https://doi.org/10.3390/jcm11175078
Chicago/Turabian StyleMihuta, Monica Simina, Corina Paul, Andreea Borlea, Cristina Mihaela Cepeha, Iulian Puiu Velea, Ioana Mozos, and Dana Stoian. 2022. "The Oscillometric Pulse Wave Analysis Is Useful in Evaluating the Arterial Stiffness of Obese Children with Relevant Cardiometabolic Risks" Journal of Clinical Medicine 11, no. 17: 5078. https://doi.org/10.3390/jcm11175078