
A Path Model for Subjective Well-Being during the Second Wave of the COVID-19 Pandemic: A Comparative Study among Polish and Ukrainian University Students





Abstract
:1. Introduction
The Purpose of the Present Study
2. Materials and Methods
2.1. Study Design and Procedure
2.2. Measures
2.2.1. Sociodemographic Survey
2.2.2. Exposure to the COVID-19 Pandemic
2.2.3. Positive Effects of the COVID-19 Pandemic
2.2.4. Religiosity
2.2.5. Physical Activity
2.2.6. Perceived Physical Health
2.2.7. Life Satisfaction
2.2.8. Perceived Stress
2.2.9. Coronavirus-Related Post-Traumatic Stress Disorder
2.2.10. Anxiety
2.2.11. Depression
2.3. Participants
2.4. Statistical Analysis
3. Results
3.1. Prevalence of Physical and Mental Health Indicators among Polish and Ukrainian University Students during the Second Wave of the COVID-19 Pandemic
3.2. Differences between Polish and Ukrainian University Students in Physical and Mental Health
3.3. Gender Differences in Physical and Mental Health
3.4. Differences in Physical and Mental Health between Physically Active and Inactive University Students
3.5. Associations between Subjective Well-Being and Physical and Mental Health
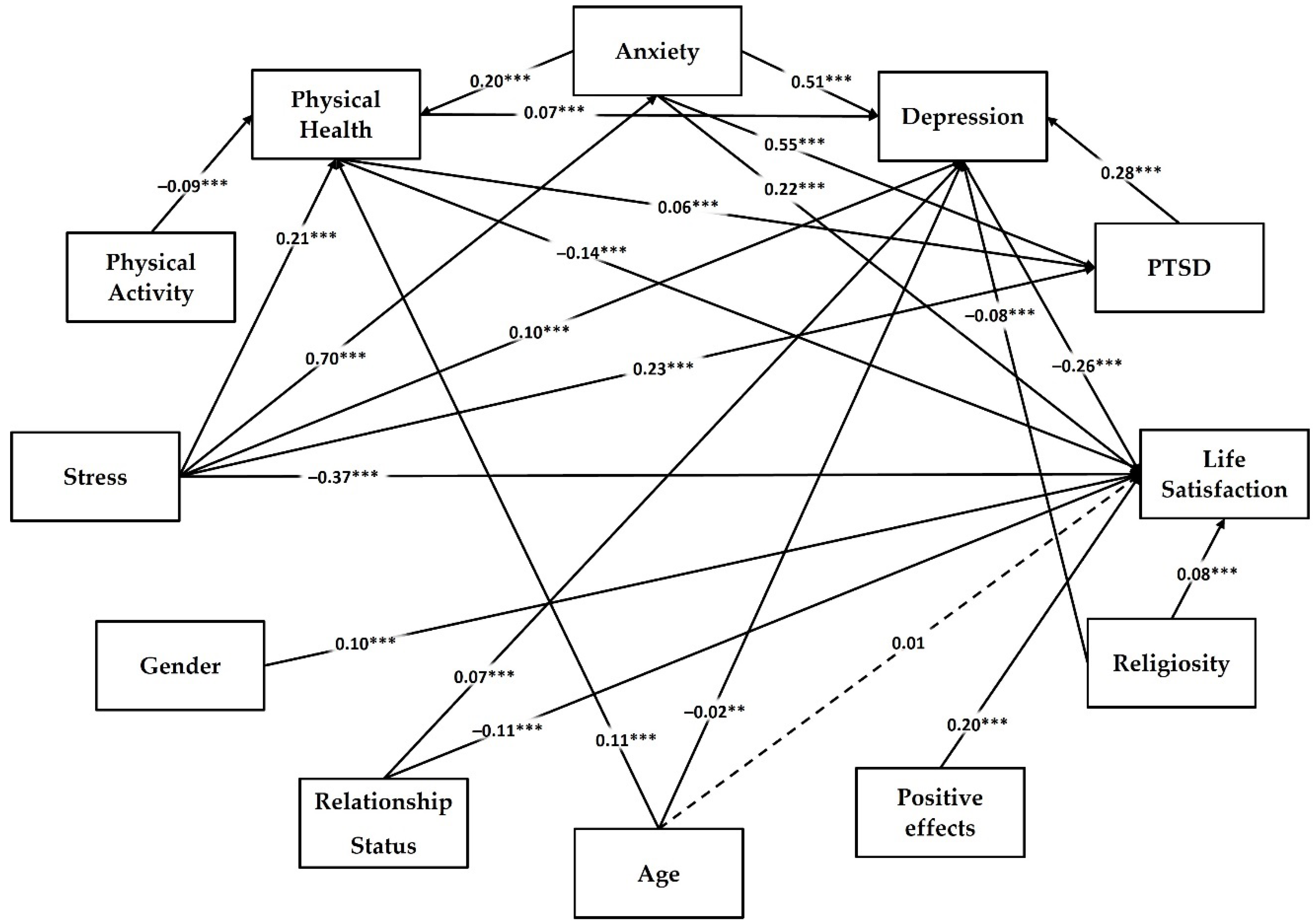
3.6. Path Model for Predictors of Life Satisfaction among University Students during the Second Wave of the COVID-19 Pandemic
3.7. Multigroup Analysis of Country Invariance for Path Model
4. Discussion
4.1. Prevalence of Physical and Mental Health Problems
4.2. Country, Gender, and Exercise Differences in Mean Levels of Mental and Physical Health and Well-Being
4.3. Associations between the Subjective Well-Being and Physical and Mental Health during the Second Wave of the COVID-19 Pandemic
4.4. Limitation of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aristovnik, A.; Keržič, D.; Ravšelj, D.; Tomaževič, N.; Umek, L. Impacts of the COVID-19 pandemic on life of higher education students: A global perspective. Sustainability 2020, 12, 8438. [Google Scholar] [CrossRef]
- Gamonal-Limcaoco, S.; Montero-Mateos, E.; Lozano-López, M.T.; Maciá-Casas, A.; Matías-Fernández, J.; Roncero, C. Perceived stress in different countries at the beginning of the coronavirus pandemic. Int. J. Psychiatry Med. 2022, 57, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Drakos, A.; Zuo, Q.K.; Huang, E. The prevalence of depressive symptoms, anxiety symptoms and sleep disturbance in higher education students during the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 301, 113863. [Google Scholar] [CrossRef] [PubMed]
- Ochnik, D.; Rogowska, A.M.; Kuśnierz, C.; Jakubiak, M.; Schütz, A.; Held, M.J.; Arzenšek, A.; Benatov, J.; Berger, R.; Korchagina, E.V.; et al. A comparison of depression and anxiety among university students in nine countries during the COVID-19 pandemic. J. Clin. Med. 2021, 10, 2882. [Google Scholar] [CrossRef]
- Ochnik, D.; Rogowska, A.M.; Kuśnierz, C.; Jakubiak, M.; Schütz, A.; Held, M.J.; Arzenšek, A.; Benatov, J.; Berger, R.; Korchagina, E.V.; et al. Mental health prevalence and predictors among university students in nine countries during the COVID-19 pandemic: A cross-national study. Sci. Rep. 2021, 11, 18644. [Google Scholar] [CrossRef]
- Rogowska, A.M.; Ochnik, D.; Kuśnierz, C.; Chilicka, K.; Jakubiak, M.; Paradowska, M.; Głazowska, L.; Bojarski, D.; Fijołek, J.; Podolak, M.; et al. Changes in mental health during three waves of the COVID-19 pandemic: A repeated cross-sectional study among Polish university students. BMC Psychiatry 2021, 21, 627. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Wilson, O.W.; Holland, K.E.; Elliott, L.D.; Duffey, M.; Bopp, M. The impact of the COVID-19 pandemic on us college students’ physical activity and mental health. J. Phys. Act. Health 2021, 18, 272–278. [Google Scholar] [CrossRef]
- Bonsaksen, T.; Leung, J.; Schoultz, M.; Thygesen, H.; Price, D.; Ruffolo, M.; Geirdal, A.Ø. Cross-national study of worrying, loneliness, and mental health during the COVID-19 pandemic: A comparison between individuals with and without infection in the family. Healthcare 2021, 9, 903. [Google Scholar] [CrossRef]
- Levkovich, I. The impact of age on negative emotional reactions, compliance with health guidelines, and knowledge about the virus during the COVID-19 epidemic: A longitudinal study from Israel. J. Prim. Care Community Health 2020, 11, 2150132720981540. [Google Scholar] [CrossRef]
- Hawley, S.R.; Thrivikraman, J.K.; Noveck, N.; Romain, T.S.; Ludy, M.J.; Barnhart, L.; Chee, W.S.S.; Cho, M.J.; Chong, M.H.Z.; Du, C.; et al. Concerns of college students during the COVID-19 pandemic: Thematic perspectives from the United States, Asia, and Europe. J. Appl. Learn. Teach. 2021, 4, 11–20. [Google Scholar] [CrossRef]
- Gupta, R.; Agrawal, R. Are the concerns destroying mental health of college students?: A qualitative analysis portraying experiences amidst COVID-19 ambiguities. Anal. Soc. Issues Public Policy 2021, 21, 621–639. [Google Scholar] [CrossRef]
- Al-Maskari, A.; Al-Riyami, T.; Kunjumuhammed, S.K. Students academic and social concerns during COVID-19 pandemic. Educ. Inf. Technol. 2021, 27, 1–21. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Kamdi, P.S.; Deogade, M.S. The hidden positive effects of COVID-19 pandemic. Int. J. Res. Pharm. Sci. 2020, 11, 276–279. [Google Scholar] [CrossRef]
- Karunathilake, K. Positive and negative impacts of COVID-19, an analysis with special reference to challenges on the supply chain in South Asian countries. J. Soc. Econ. Dev. 2021, 23, 568–581. [Google Scholar] [CrossRef]
- Walsh, A.R.; Stephenson, R. Positive and negative impacts of the COVID-19 pandemic on relationship satisfaction in male couples. Am. J. Men’s Health 2021, 15, 15579883211022180. [Google Scholar] [CrossRef]
- Sudo, N. The positive and negative effects of the COVID-19 pandemic on subjective well-being and changes in social inequality: Evidence from prefectures in Japan. SSM-Popul. Health 2022, 17, 101029. [Google Scholar] [CrossRef]
- Aknin, L.; De Neve, J.E.; Dunn, E.; Fancourt, D.; Goldberg, E.; Helliwell, J.F.; Jones, S.P.; Karam, E.; Layard, R.; Lyubomirsky, S.; et al. Mental health during the first year of the COVID-19 pandemic: A review and recommendations for moving forward. Perspect. Psychol. Sci. 2022, 14, 915–936. [Google Scholar] [CrossRef]
- Daly, M.; Sutin, A.R.; Robinson, E. Longitudinal changes in mental health and the COVID-19 pandemic: Evidence from the UK Household Longitudinal Study. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef]
- Robinson, E.; Sutin, A.R.; Daly, M.; Jones, A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J. Affect. Disord. 2021, 296, 567–576. [Google Scholar] [CrossRef]
- Fruehwirth, J.C.; Biswas, S.; Perreira, K.M. The Covid-19 pandemic and mental health of first-year college students: Examining the effect of COVID-19 stressors using longitudinal data. PLoS ONE 2021, 16, e0247999. [Google Scholar] [CrossRef]
- Nochaiwong, S.; Ruengorn, C.; Thavorn, K.; Hutton, B.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 10173. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Rogowska, A.M.; Kuśnierz, C.; Ochnik, D. Changes in stress, coping styles, and life satisfaction between the first and second waves of the COVID-19 pandemic: A longitudinal cross-lagged study in a sample of university students. J. Clin. Med. 2021, 10, 4025. [Google Scholar] [CrossRef]
- Bisht, I.P.; Bisht, R.K.; Sagar, P. Effect of gender and age in fear and stress due to COVID-19. J. Hum. Behav. Soc. Environ. 2021, 31, 70–76. [Google Scholar] [CrossRef]
- Bambra, C.; Albani, V.; Franklin, P. COVID-19 and the gender health paradox. Scand. J. Public. Health. 2021, 49, 17–26. [Google Scholar] [CrossRef]
- Rodríguez-Rey, R.; Garrido-Hernansaiz, H.; Collado, S. Psychological impact and associated factors during the initial stage of the coronavirus (COVID-19) pandemic among the general population in Spain. Front. Psychol. 2020, 11, 1540. [Google Scholar] [CrossRef]
- Niedzwiedz, C.L.; Green, M.J.; Benzeval, M.; Campbell, D.; Craig, P.; Demou, E.; Leyland, A.; Pearce, A.; Thomson, R.; Whitley, E.; et al. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: Longitudinal analyses of the UK Household Longitudinal Study. J. Epidemiol. Community Health 2020, 75, 224–231. [Google Scholar] [CrossRef]
- Benatov, J.; Ochnik, D.; Rogowska, A.M.; Arzenšek, A.; Mars Bitenc, U. Prevalence and sociodemographic predictors of mental health in a representative sample of young adults from Germany, Israel, Poland, and Slovenia: A longitudinal study during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1334. [Google Scholar] [CrossRef]
- Ochnik, D.; Rogowska, A.M.; Arzenšek, A.; Benatov, J. Can fear of COVID-19 be predicted by religiosity and trust in institutions among young adults? A prospective cross-national study. Int. J. Environ. Res. Public Health 2022, 19, 6766. [Google Scholar] [CrossRef] [PubMed]
- Rogowska, A.; Kuśnierz, C.; Bokszczanin, A. Examining anxiety, life satisfaction, general health, stress and coping styles during COVID-19 pandemic in Polish sample of university students. Psychol. Res. Behav. Manag. 2020, 13, 797–811. [Google Scholar] [CrossRef] [PubMed]
- Solomou, I.; Constantinidou, F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: Age and sex matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Di, Y.; Ye, J.; Wei, W. Study on the public psychological states and its related factors during the outbreak of coronavirus disease 2019 (COVID-19) in some regions of China. Psychol. Health Med. 2020, 26, 13–22. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Zhang, S.X.; Wang, Y.; Rauch, A.; Wei, F. Unprecedented disruption of lives and work: Health, distress and life satisfaction of working adults in China one month into the COVID-19 outbreak. Psychiatry Res. 2020, 288, 112958. [Google Scholar] [CrossRef]
- Ahmed, Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated psychological problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Lane, R.I.; Petrosky, E.; Wiley, J.F.; Christensen, A.; Njai, R.; Weaver, M.D.; Robbins, R.; Facer-Childs, E.R.; Barger, L.K.; et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic—United States, 24–30 June 2020. MMWR Morb. Mortal Wkly Rep. 2020, 69, 1049–1057. [Google Scholar] [CrossRef]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G. How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide Life Threat. Behav. 2020, 50, 1241–1249. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Mental health burden for the public affected by the COVID-19 outbreak in China: Who will be the high-risk group? Psychol. Health Med. 2021, 26, 23–34. [Google Scholar] [CrossRef]
- Liang, L.; Ren, H.; Cao, R.; Hu, Y.; Qin, Z.; Li, C.; Mei, S. The effect of COVID-19 on youth mental health. Psychiatr. Q. 2020, 91, 841–852. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Ochnik, D.; Arzenšek, A.; Rogowska, A.M.; Mars Bitenc, U.; Benatov, J. Changes in Mental Health during the COVID-19 Pandemic among Representative Sample of Young Adults from Germany, Israel, Poland, and Slovenia: A Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 5794. [Google Scholar] [CrossRef]
- Ochnik, D.; Rogowska, A.M.; Ku’snierz, C.; Jakubiak, M.; Wierzbik-Strońska, M.; Schütz, A.; Held, M.J.; Arzenšek, A.; Pavlova, I.; Korchagina, E.V.; et al. Exposure to COVID-19 during the First and the SecondWave of the Pandemic and Coronavirus-Related PTSD Risk among University Students from Six Countries—A Repeated Cross-Sectional Study. J. Clin. Med. 2021, 10, 5564. [Google Scholar] [CrossRef]
- Rogowska, A.M.; Ochnik, D.; Kuśnierz, C.; Jakubiak, M.; Schütz, A.; Held, M.J.; Arzenšek, A.; Benatov, J.; Berger, R.; Korchagina, E.V.; et al. Satisfaction with life among university students from nine countries: Cross-national study during the first wave of COVID-19 pandemic. BMC Public Health 2021, 21, 2262. [Google Scholar] [CrossRef]
- Ochnik, D.; Rogowska, A.M.; Arzenšek, A.; Benatov, J. Longitudinal Predictors of Coronavirus-Related PTSD among Young Adults from Poland, Germany, Slovenia, and Israel. Int. J. Environ. Res. Public Health 2022, 19, 7207. [Google Scholar] [CrossRef]
- Stulp, H.P.; Koelen, J.; Schep-Akkerman, A.; Glas, G.G.; Eurelings-Bontekoe, L. God representations and aspects of psychological functioning: A meta-analysis. Cogent Psychol. 2019, 6, 1647926. [Google Scholar] [CrossRef]
- Koenig, H.G. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012, 8, 278730. [Google Scholar] [CrossRef]
- Unterrainer, H.F.; Lewis, A.J.; Fink, A. Religious/spiritual well-being, personality and mental health: A review of results and conceptual issues. J. Relig. Health 2014, 53, 382–392. [Google Scholar] [CrossRef]
- Garssen, B.; Visser, A.; Pool, G. Does spirituality or religion positively affect mental health? Meta-analysis of longitudinal studies. Int. J. Psychol. Relig. 2021, 31, 4–20. [Google Scholar] [CrossRef]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef]
- Qi, M.; Li, P.; Moyle, W.; Weeks, B.; Jones, C. Physical activity, health-related quality of life, and stress among the chinese adult population during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6494. [Google Scholar] [CrossRef]
- Şimşek, E.; Koc, K.; Ozsoy, D.; Karakuş, M. Investigation the effect of performing physical activity at home on sleep quality and life satisfaction during coronavirus (COVID-19) outbreak. Int. J. Appl. Exerc. Physiol. 2020, 9, 55–62. [Google Scholar] [CrossRef]
- Sochacka, M.; Zdziarski, K. Physical activity and well-being of students of faculties medical and non-medical services during the Covid-19 pandemic. J. Educ. Health Sport 2022, 12, 63–80. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M. Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 international online survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Bertrand, L.; Shaw, K.A.; Ko, J.; Deprez, D.; Chilibeck, P.D.; Zello, G.A. The impact of the coronavirus disease 2019 (COVID-19) pandemic on university students’ dietary intake, physical activity, and sedentary behaviour. Appl. Physiol. Nutr. Metab. 2021, 46, 265–272. [Google Scholar] [CrossRef]
- Caputo, E.L.; Reichert, F.F. Studies of physical activity and COVID-19 during the pandemic: A scoping review. J. Phys. Act. Health 2020, 17, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Sabella, E.A.; Ferracuti, S.; De Giglio, O.; Caggiano, G.; Protano, C.; Valeriani, F.; Parisi, E.A.; Valerio, G.; Liguori, G.; et al. Sedentary Behaviors and Physical Activity of Italian Undergraduate Students during Lockdown at the Time of COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6171. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Ezzatvar, Y.; Casajús, J.A.; Smith, L.; Andersen, L.L.; López-Sánchez, G.F. Association between current physical activity and current perceived anxiety and mood in the initial phase of COVID-19 confinement. Front. Psychiatry 2020, 11, 729. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Suárez-Iglesias, D.; Sanchez-Lastra, M.A.; Ayán, C. Impact of COVID-19 pandemic on university students’ physical activity levels: An early systematic review. Front. Psychol. 2021, 11, 624567. [Google Scholar] [CrossRef] [PubMed]
- Rivera, P.A.; Nys, B.L.; Fiestas, F. Impact of COVID-19 induced lockdown on physical activity and sedentary behavior among university students: A systematic review. Medwave 2021, 21, e8456. [Google Scholar] [CrossRef] [PubMed]
- Rogowska, A.M.; Pavlova, I.; Kusnierz, C.; Ochnik, D.; Bodnar, I.; Petrytsa, P. Does Physical Activity Matter for the Mental Health of University Students during the COVID-19 Pandemic? J. Clin. Med. 2020, 9, 3494. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Smith, L.; Jacob, L.; Trott, M.; Yakkundi, A.; Butler, L.; Barnett, Y.; Armstrong, N.C.; McDermott, D.; Schuch, F.; Meyer, J.; et al. The association between screen time and mental health during COVID-19: A cross sectional study. Psychiatry Res. 2020, 292, 113333. [Google Scholar] [CrossRef]
- Dar, K.A.; Iqbal, N.; Mushtaq, A. Intolerance of uncertainty, depression, and anxiety: Examining the indirect and moderating effects of worry. Asian J. Psychiatr. 2017, 29, 129–133. [Google Scholar] [CrossRef]
- Yang, C.; Xia, M.; Han, M.; Liang, Y. Social support and resilience as mediators between stress and life satisfaction among people with substance use disorder in China. Front. Psychiatry 2018, 9, 436. [Google Scholar] [CrossRef]
- Lee, C.-W.; Lin, L.-C.; Hung, H.-C. Art and cultural participation and life satisfaction in adults: The role of physical health, mental health, and interpersonal relationships. Front. Public Health 2021, 8, 582342. [Google Scholar] [CrossRef]
- Böckerman, P.; Johansson, E.; Saarni, S.I. Do established health-related quality of-life measures adequately capture the impact of chronic conditions on subjective wellbeing? Health Policy 2011, 100, 91–95. [Google Scholar] [CrossRef]
- Beutel, M.E.; Glaesmer, H.; Wiltink, J.; Marian, H.; Brahler, E. Life satisfaction, anxiety, depression and resilience across the life span of men. Aging Male 2010, 13, 32–39. [Google Scholar] [CrossRef]
- Praharso, N.F.; Tear, M.J.; Cruwys, T. Stressful life transitions and wellbeing: A comparison of the stress-buffering hypothesis and the social identity model of identity change. Psychiatry Res. 2017, 247, 265–275. [Google Scholar] [CrossRef]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav. Immun. 2020, 87, 100–106. [Google Scholar] [CrossRef]
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Lehman, B.J.; David, D.M.; Gruber, J.A. Rethinking the biopsychosocial model of health: Understanding health as a dynamic system. Soc. Personal. Psychol. Compass 2017, 11, e12328. [Google Scholar] [CrossRef]
- Karunamuni, N.D.; Imayama, I.; Goonetilleke, D. Pathways to well-being: Untangling the causal relationships among biopsychosocial variables. Soc. Sci. Med. 2021, 272, 112846. [Google Scholar] [CrossRef]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; ISPOR Task Force for Translation and Cultural Adaptation. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef]
- Wild, D.; Eremenco, S.; Mear, I.; Martin, M.; Houchin, C.; Gawlicki, M.; Hareendran, A.; Wiklund, I.; Chong, L.Y.; von Maltzahn, R.; et al. Multinational trials—Recommendations on the translations required, approaches to using the same language in different countries, and the approaches to support pooling the data: The patient-reported outcomes translation and linguistic validation good research practices task force report. Value Health 2009, 12, 430–440. [Google Scholar] [CrossRef]
- Ochnik, D.; Rogowska, A.M.; Kuśnierz, C.; Jakubiak, M.; Pavlova, I.; Arzenšek, A.; Blažková, I.; Korchagina, E.; Schütz, A.; Aslan, I.; et al. Mental Health of Undergraduates during the COVID-19 Pandemic; OSF: Charlottesville, VA, USA, 2020; Available online: https://osf.io/wfsqb/ (accessed on 9 August 2022). [CrossRef]
- Tang, W.; Hu, T.; Hu, B.; Jin, C.; Wang, G.; Xie, C.; Chen, S.; Xu, J. Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese university students. J. Affect. Disord. 2020, 274, 1–7. [Google Scholar] [CrossRef]
- Alshammari, T.K.; Alkhodair, A.M.; Alhebshi, H.A.; Rogowska, A.M.; Albaker, A.B.; AL-Damri, N.T.; Bin Dayel, A.F.; Alonazi, A.S.; Alrasheed, N.M.; Alshammari, M.A. Examining Anxiety, Sleep Quality, and Physical Activity as Predictors of Depression among University Students from Saudi Arabia during the Second Wave of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 6262. [Google Scholar] [CrossRef]
- Froese, P. Baylor Religion Survey, Wave V (2017)-Instructional Dataset; Baylor Religion Survey: Waco, TX, USA, 2020. [Google Scholar]
- WHO. Coronavirus Disease (COVID-19): Staying Active; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Kuśnierz, C.; Rogowska, A.M.; Kwaśnicka, A.; Ochnik, D. The Mediating Role of Orthorexia in the Relationship between Physical Activity and Fear of COVID-19 among University Students in Poland. J. Clin. Med. 2021, 10, 5061. [Google Scholar] [CrossRef]
- DeSalvo, K.B.; Fisher, W.P.; Tran, K.; Bloser, N.; Merrill, W.; Peabody, J. Assessing measurement properties of two single-item general health measures. Qual. Life Res. 2006, 15, 191–201. [Google Scholar] [CrossRef]
- DeSalvo, K.B.; Fan, V.; McDonell, M.B.; Fihn, S.D. Predicting mortality and healthcare utilization with a single question. Health Serv. Res. 2005, 40, 1234–1246. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Weathers, F.W.; Ruscio, A.M.; Keane, T.M. Psychometric properties of nine scoring rules for the Clinician-Administered Posttraumatic Stress Disorder Scale. Psychol. Assess. 1999, 11, 124–133. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. The PTSD Checklist for DSM-5 (PCL-5). In Scale Available from the National Center for PTSD; National Center for PTSD: Hartford, VT, USA, 2013. [Google Scholar]
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD checklist (PCL). Behav. Res. Ther. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural Equation Modelling: Guidelines for Determining Model Fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- The Jamovi Project. 2021 Jamovi, Version 2.2; Windows; Available online: https://www.jamovi.org (accessed on 6 June 2022).
- R Core Team. 2021 R: A Language and Environment for Statistical Computing, Version 4.0; Windows; Available online: https://cran.r-project.org (accessed on 6 June 2022).
- Gallucci, M. PATHj: Jamovi Path Analysis. 2021. Available online: https://pathj.github.io/ (accessed on 6 June 2022).
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2019, 48, 1–36. [Google Scholar] [CrossRef]
- Helliwell, J.F.; Huang, H.; Wang, S.; Norton, M. World happiness, trust and deaths under COVID-19. In World Happiness Report 2021; Sustainable Development Solutions Network: New York, NY, USA, 2021; pp. 13–57. Available online: https://worldhappiness.report/ed/2021/happiness-trust-and-deaths-under-covid-19/ (accessed on 6 June 2021).
- Eek, F.; Larsson, C.; Wisen, A.; Ekvall, H.E. Self-perceived changes in physical activity and the relation to life satisfaction and rated physical capacity in Swedish adults during the COVID-19 pandemic—A cross sectional study. Int. J. Environ. Res. Public Health 2021, 18, 671. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, H.; Ma, X.; Di, Q. Mental health problems during the COVID-19 pandemics and the mitigation effects of exercise: A longitudinal study of college students in China. Int. J. Environ. Res. Public Health 2020, 17, 3722. [Google Scholar] [CrossRef]
- Heijnen, S.; Hommel, B.; Kibele, A.; Colzato, L.S. Neuromodulation of Aerobic Exercise—A Review. Front. Psychol. 2016, 6, 1890. [Google Scholar] [CrossRef]
- Mohamed, A.; Alawna, M. Role of increasing the aerobic capacity on improving the function of immune and respiratory systems in patients with coronavirus (COVID-19): A review. Diabetes Metab. Syndr. 2020, 14, 489–496. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Luan, X.; Tian, X.; Zhang, H.; Huang, R.; Li, N.; Chen, P.; Wang, R. Exercise as a prescription for patients with various diseases. J. Sport Health Sci. 2019, 8, 422–441. [Google Scholar] [CrossRef]
- Zhang, S.X.; Sun, S.; Afshar Jahanshahi, A.; Wang, Y.; Nazarian Madavani, A.; Li, J.; Mokhtari Dinani, M. Beyond predicting the number of infections: Predicting who is likely to be COVID negative or positive. Risk Manag. Healthc. Policy 2020, 13, 2811–2818. [Google Scholar] [CrossRef]
- Wang, X.; Lei, S.M.; Le, S.; Yang, Y.; Zhang, B.; Yao, W.; Gao, Z.; Cheng, S. Bidirectional influence of the COVID-19 pandemic lockdowns on health behaviors and quality of life among Chinese adults. Int. J. Environ. Res. Public Health 2020, 17, 5575. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sample | Total Sample | χ2 | df | p | φ | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Polish | Ukrainian | |||||||||
| Variable | n | % | n | % | n | % | ||||
| Gender | 78.98 | 2 | <0.001 | 0.156 V | ||||||
| Men | 748 | 23.16 | 528 | 16.35 | 1276 | 39.51 | ||||
| Women | 815 | 25.23 | 1097 | 33.96 | 1912 | 59.20 | ||||
| Nonbinary | 18 | 0.56 | 24 | 0.74 | 42 | 1.30 | ||||
| Relationship status | 49.74 | 1 | <0.001 | 0.124 | ||||||
| In a couple | 899 | 27.833 | 733 | 22.69 | 1632 | 50.53 | ||||
| Single | 682 | 21.12 | 916 | 28.36 | 1598 | 49.47 | ||||
| Physical activity | 4.82 | 1 | 0.028 | −0.039 | ||||||
| Insufficient | 1015 | 31.42 | 1119 | 34.64 | 2134 | 66.07 | ||||
| Sufficient | 566 | 17.52 | 530 | 16.41 | 1096 | 33.93 | ||||
| Exposure 1 | 81.48 | 1 | <0.001 | 0.159 | ||||||
| No | 1211 | 37.49 | 1021 | 31.61 | 2232 | 69.10 | ||||
| Yes | 370 | 11.46 | 628 | 19.44 | 998 | 30.90 | ||||
| Exposure 2 | 15.06 | 1 | <0.001 | 0.068 | ||||||
| No | 1388 | 42.97 | 1368 | 42.35 | 2756 | 85.33 | ||||
| Yes | 193 | 5.98 | 281 | 8.70 | 474 | 14.68 | ||||
| Exposure 3 | 2.52 | 1 | 0.112 | −0.028 | ||||||
| No | 1545 | 47.83 | 1624 | 50.28 | 3169 | 98.11 | ||||
| Yes | 36 | 1.12 | 25 | 0.77 | 61 | 1.89 | ||||
| Exposure 4 | 18.62 | 1 | <0.001 | 0.076 | ||||||
| No | 1418 | 43.90 | 1395 | 43.19 | 2813 | 87.09 | ||||
| Yes | 163 | 5.05 | 254 | 7.86 | 417 | 12.91 | ||||
| Exposure 5 | 13.06 | 1 | <0.001 | −0.064 | ||||||
| No | 724 | 22.42 | 860 | 26.63 | 1584 | 49.04 | ||||
| Yes | 857 | 26.53 | 789 | 24.43 | 1646 | 50.96 | ||||
| Exposure 6 | 0.17 | 1 | 0.679 | −0.007 | ||||||
| No | 1454 | 45.02 | 1523 | 47.15 | 2977 | 92.17 | ||||
| Yes | 127 | 3.93 | 126 | 3.90 | 253 | 7.83 | ||||
| Exposure 7 | 4.65 | 1 | 0.031 | −0.038 | ||||||
| No | 1170 | 36.22 | 1274 | 39.44 | 2444 | 75.67 | ||||
| Yes | 411 | 12.72 | 375 | 11.61 | 786 | 24.33 | ||||
| Exposure 8 | 2.09 | 1 | 0.148 | 0.025 | ||||||
| No | 549 | 17.00 | 533 | 16.50 | 1082 | 33.50 | ||||
| Yes | 1032 | 32.00 | 1116 | 34.55 | 2148 | 66.50 | ||||
| Variable | Sample | Total Sample (n = 3230) | χ2 | df | p | φ | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Polish (n = 1581) | Ukrainian (n = 1649) | |||||||||
| n | % | n | % | n | % | |||||
| Life satisfaction | 110.55 | 6 | <0.001 | 0.19 | ||||||
| Extremely dissatisfied | 54 | 1.67 | 26 | 0.81 | 80 | 2.48 | ||||
| Dissatisfied | 230 | 7.12 | 120 | 3.72 | 350 | 10.84 | ||||
| Slightly dissatisfied | 384 | 11.89 | 321 | 9.94 | 705 | 21.83 | ||||
| Neutral | 77 | 2.38 | 78 | 2.42 | 155 | 4.80 | ||||
| Slightly satisfied | 485 | 15.02 | 515 | 15.94 | 1000 | 30.96 | ||||
| Satisfied | 280 | 8.67 | 455 | 14.09 | 735 | 22.76 | ||||
| Extremely satisfied | 71 | 2.20 | 134 | 4.15 | 205 | 6.35 | ||||
| Physical health | 217.91 | 4 | <0.001 | 0.26 | ||||||
| Excellent | 144 | 4.46 | 454 | 14.06 | 598 | 18.51 | ||||
| Very good | 641 | 19.85 | 431 | 13.34 | 1072 | 33.19 | ||||
| Good | 652 | 20.19 | 681 | 21.08 | 1333 | 41.27 | ||||
| Fair | 130 | 4.03 | 77 | 2.38 | 207 | 6.41 | ||||
| Poor | 14 | 0.43 | 6 | 0.19 | 20 | 0.62 | ||||
| Perceived stress | 71.61 | 4 | <0.001 | 0.15 | ||||||
| Extremely low | 158 | 4.89 | 232 | 7.18 | 390 | 12.07 | ||||
| Low | 300 | 9.29 | 403 | 12.48 | 703 | 21.77 | ||||
| Average | 467 | 14.46 | 534 | 16.53 | 1001 | 30.99 | ||||
| High | 351 | 10.87 | 307 | 9.51 | 658 | 20.37 | ||||
| Extremely high | 305 | 9.44 | 173 | 5.36 | 478 | 14.80 | ||||
| Coronavirus-related PTSD | 49.80 | 1 | <0.001 | −0.12 | ||||||
| No | 1134 | 35.11 | 1355 | 41.95 | 2489 | 77.06 | ||||
| Yes | 447 | 13.84 | 294 | 9.10 | 741 | 22.94 | ||||
| General anxiety disorder | 36.52 | 3 | <0.001 | 0.11 | ||||||
| No anxiety | 595 | 18.42 | 711 | 22.01 | 1306 | 40.43 | ||||
| Mild anxiety | 498 | 15.42 | 545 | 16.87 | 1043 | 32.29 | ||||
| Moderate anxiety | 280 | 8.67 | 276 | 8.55 | 556 | 17.21 | ||||
| Severe anxiety | 208 | 6.44 | 117 | 3.62 | 325 | 10.06 | ||||
| Major depression | 36.85 | 4 | <0.001 | 0.11 | ||||||
| No depression | 440 | 13.62 | 569 | 17.62 | 1009 | 31.24 | ||||
| Mild depression | 456 | 14.12 | 525 | 16.25 | 981 | 30.37 | ||||
| Moderate depression | 351 | 10.87 | 309 | 9.57 | 660 | 20.43 | ||||
| Moderately severe | 214 | 6.63 | 167 | 5.17 | 381 | 11.80 | ||||
| Severe depression | 120 | 3.72 | 79 | 2.45 | 199 | 6.16 | ||||
| Variable | Polish (n = 1581) | Ukrainian (n = 1649) | t | df | p | ΔM | d | ||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||||
| Life satisfaction | 20.55 | 6.08 | 22.86 | 5.82 | −11.01 a | 3205 | <0.001 | −2.31 | −0.39 |
| Poor physical health | 2.51 | 0.81 | 2.24 | 0.92 | 8.88 a | 3201 | <0.001 | 0.27 | 0.31 |
| Stress | 21.56 | 7.53 | 19.46 | 7.16 | 8.10 a | 3201 | <0.001 | 2.10 | 0.29 |
| Coronavirus-related PTSD | 36.90 | 13.37 | 32.91 | 11.48 | 9.08 a | 3112 | <0.001 | 3.99 | 0.32 |
| Anxiety | 7.29 | 5.58 | 6.27 | 4.97 | 5.47 a | 3151 | <0.001 | 1.02 | 0.19 |
| Depression | 9.19 | 6.43 | 7.89 | 5.97 | 5.97 a | 3185 | <0.001 | 1.30 | 0.21 |
| Positive lockdown effects | 14.02 | 5.82 | 17.16 | 5.91 | −15.20 b | 3228 | 0.001 | −3.14 | −0.54 |
| Religiosity | 1.58 | 0.98 | 1.47 | 0.85 | 3.28 a | 3123 | 0.001 | 0.11 | 0.12 |
| Men (n = 1318) | Women (n = 1912) | t | df | p | ΔM | d | |||
|---|---|---|---|---|---|---|---|---|---|
| Variable | M | SD | M | SD | |||||
| Life satisfaction | 21.18 | 6.09 | 22.11 | 6.01 | −4.30 b | 3228 | <0.001 | −0.93 | −0.15 |
| Poor physical health | 2.30 | 0.88 | 2.43 | 0.87 | −4.23 b | 3228 | <0.001 | −0.13 | −0.15 |
| Stress | 19.03 | 7.43 | 21.49 | 7.24 | −9.38 b | 3228 | <0.001 | −2.46 | −0.34 |
| Coronavirus-related PTSD | 32.86 | 12.01 | 36.24 | 12.82 | −7.64 a | 2945 | <0.001 | −3.37 | −0.27 |
| Anxiety | 5.83 | 5.20 | 7.43 | 5.27 | −8.52 b | 3228 | <0.001 | −1.60 | −0.31 |
| Depression | 7.76 | 6.04 | 9.05 | 6.30 | −5.80 b | 3228 | <0.001 | −1.29 | −0.21 |
| Positive lockdown effects | 15.21 | 6.06 | 15.90 | 6.06 | −3.18 b | 3228 | 0.002 | −0.69 | −0.11 |
| Religiosity | 1.36 | 0.99 | 1.64 | 0.85 | −8.37 a | 2556 | <0.001 | −0.28 | −0.30 |
| Insufficient PA (n = 2134) | Sufficient PA (n = 1096) | t | df | p | ΔM | d | |||
|---|---|---|---|---|---|---|---|---|---|
| Variable | M | SD | M | SD | |||||
| Life satisfaction | 21.26 | 6.16 | 22.63 | 5.75 | −6.25 a | 2350 | <0.001 | −1.37 | −0.23 |
| Poor physical health | 2.47 | 0.87 | 2.19 | 0.86 | 8.71 b | 3228 | <0.001 | 0.28 | 0.32 |
| Stress | 21.28 | 7.39 | 18.95 | 7.24 | 8.53 b | 3228 | <0.001 | 2.33 | 0.32 |
| Coronavirus-related PTSD | 35.80 | 12.67 | 33.04 | 12.27 | 5.91 b | 3228 | <0.001 | 2.75 | 0.22 |
| Anxiety | 7.26 | 5.35 | 5.82 | 5.07 | 7.73 a | 2293 | <0.001 | 1.75 | 0.29 |
| Depression | 9.12 | 6.26 | 7.37 | 6.00 | 7.63 b | 3228 | <0.001 | 1.75 | 0.28 |
| Positive COVID-19 effects | 15.37 | 5.99 | 16.11 | 6.19 | −3.27 b | 3228 | 0.001 | −0.74 | −0.12 |
| Religiosity | 1.52 | 0.92 | 1.54 | 0.93 | −0.61 b | 3228 | 0.541 | −0.02 | −0.02 |
| Predictor | β | B | SE | 95% CI | t | p | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Age | 0.05 | 0.08 | 0.03 | 0.03 | 0.14 | 2.88 | 0.004 |
| Gender | 0.20 | 1.20 | 0.19 | 0.83 | 1.57 | 6.34 | <0.001 |
| Relationship status | −0.22 | −1.35 | 0.18 | −1.70 | −1.00 | −7.59 | <0.001 |
| Country | 0.19 | 1.14 | 0.20 | 0.75 | 1.53 | 5.72 | <0.001 |
| PA | 0.10 | 0.58 | 0.19 | 0.21 | 0.94 | 3.09 | 0.002 |
| Physical health | −0.13 | −0.92 | 0.11 | −1.13 | −0.71 | 8.46 | <0.001 |
| Stress | −0.35 | −0.29 | 0.02 | −0.32 | −0.25 | −16.73 | <0.001 |
| PTSD | 0.02 | 0.01 | 0.01 | −0.01 | 0.03 | 0.69 | 0.489 |
| Anxiety | 0.21 | 0.23 | 0.03 | 0.17 | 0.29 | 7.60 | <0.001 |
| Depression | −0.26 | −0.25 | 0.03 | −0.30 | −0.20 | −9.61 | <0.001 |
| Positive effects | 0.18 | 0.18 | 0.02 | 0.15 | 0.21 | 12.07 | <0.001 |
| Religiosity | 0.08 | 0.55 | 0.10 | 0.36 | 0.73 | 5.70 | <0.001 |
| Variables | Total Sample β | Polish Sample β | Ukrainian Sample β | |
|---|---|---|---|---|
| Dependent | Predictor | |||
| Life satisfaction | Physical health | −0.14 *** | −0.13 *** | −0.15 *** |
| Life satisfaction | Anxiety | 0.22 *** | 0.22 *** | 0.21 *** |
| Life satisfaction | Depression | −0.26*** | −0.26 *** | −0.25 *** |
| Life satisfaction | Relationships | −0.11 *** | −0.11 *** | −0.11 *** |
| Life satisfaction | Religiosity | 0.08 *** | 0.09 *** | 0.08 *** |
| Life satisfaction | Positive effects | 0.20 *** | 0.18 *** | 0.19 *** |
| Life satisfaction | Gender | 0.10 *** | 0.09 *** | 0.09 *** |
| Life satisfaction | Stress | −0.37 *** | −0.36 *** | −0.35 *** |
| Life satisfaction | Age | 0.01 | 0.05 ** | 0.03 ** |
| Physical health | PA | −0.09 *** | −0.11 *** | −0.09 *** |
| Physical health | Stress | 0.21 *** | 0.22 *** | 0.19 *** |
| Physical health | Age | 0.11 *** | 0.09 *** | 0.05 *** |
| Physical health | Anxiety | 0.20 *** | 0.22 *** | 0.18 *** |
| PTSD | Physical health | 0.06 *** | 0.05 *** | 0.06 *** |
| PTSD | Stress | 0.23 *** | 0.23 *** | 0.22 *** |
| PTSD | Anxiety | 0.55 *** | 0.58 *** | 0.55 *** |
| Anxiety | Stress | 0.70 *** | 0.69 *** | 0.71 *** |
| Depression | Anxiety | 0.51 *** | 0.51 *** | 0.50 *** |
| Depression | Religiosity | −0.08 *** | −0.09 *** | −0.08 *** |
| Depression | Stress | 0.10 *** | 0.10 *** | 0.10 *** |
| Depression | Age | −0.02 ** | −0.03 ** | −0.02 ** |
| Depression | Physical health | 0.07 *** | 0.07 *** | 0.08 *** |
| Depression | Relationships | 0.07 *** | 0.07 *** | 0.07 *** |
| Depression | PTSD | 0.28 *** | 0.27 *** | 0.28 *** |
| Path Parameter | B | SE | 95% CI | β | z | p | |
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| PH ⇒ PTSD ⇒ Depression ⇒ LS | −0.03 | 0.01 | −0.05 | −0.02 | 0.00 | −3.97 | <0.001 |
| PH ⇒ Depression ⇒ LS | −0.13 | 0.02 | −0.18 | −0.09 | −0.02 | −5.53 | <0.001 |
| GAD ⇒ PH ⇒ LS | −0.03 | 0.01 | −0.04 | −0.02 | −0.03 | −6.23 | <0.001 |
| GAD ⇒ PH ⇒ PTSD ⇒ Depression ⇒ LS | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | −3.68 | <0.001 |
| GAD ⇒ PH ⇒ Depression ⇒ LS | 0.00 | 0.00 | −0.01 | 0.00 | 0.00 | −4.62 | <0.001 |
| GAD ⇒ PTSD ⇒ Depression ⇒ LS | −0.05 | 0.01 | −0.06 | −0.04 | −0.04 | −7.69 | <0.001 |
| GAD ⇒ Depression ⇒ LS | −0.15 | 0.02 | −0.18 | −0.11 | −0.13 | −8.55 | <0.001 |
| Relationships ⇒ Depression ⇒ LS | −0.22 | 0.04 | −0.30 | −0.15 | −0.02 | −5.68 | <0.001 |
| Religiosity ⇒ Depression ⇒ LS | 0.14 | 0.02 | 0.10 | 0.19 | 0.02 | 6.41 | <0.001 |
| Stress ⇒ PH ⇒ LS | −0.03 | 0.00 | −0.03 | −0.02 | −0.03 | −6.41 | <0.001 |
| Stress ⇒ PH ⇒ PTSD ⇒ Depression ⇒ LS | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | −3.61 | <0.001 |
| Stress ⇒ PH ⇒ Depression ⇒ LS | 0.00 | 0.00 | −0.01 | 0.00 | 0.00 | −4.76 | <0.001 |
| Stress ⇒ PTSD ⇒ Depression ⇒ LS | −0.01 | 0.00 | −0.02 | −0.01 | −0.02 | −7.39 | <0.001 |
| Stress ⇒ GAD ⇒ LS | 0.13 | 0.02 | 0.10 | 0.16 | 0.16 | 7.82 | <0.001 |
| Stress ⇒ GAD ⇒ PH ⇒ LS | −0.02 | 0.00 | −0.02 | −0.01 | −0.02 | −6.22 | <0.001 |
| Stress ⇒ GAD ⇒ PH ⇒ PTSD ⇒ Depression ⇒ LS | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | −3.67 | <0.001 |
| Stress ⇒ GAD ⇒ PH ⇒ Depression ⇒ LS | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | −4.61 | <0.001 |
| Stress ⇒ GAD ⇒ PTSD ⇒ Depression ⇒ LS | −0.02 | 0.00 | −0.03 | −0.02 | −0.03 | −7.62 | <0.001 |
| Stress ⇒ GAD ⇒ Depression ⇒ LS | −0.08 | 0.01 | −0.09 | −0.06 | −0.09 | −8.42 | <0.001 |
| Stress ⇒ Depression ⇒ LS | −0.02 | 0.00 | −0.03 | −0.01 | −0.03 | −5.17 | <0.001 |
| Age ⇒ PH ⇒ LS | −0.03 | 0.01 | −0.04 | −0.02 | −0.02 | −5.51 | <0.001 |
| Age ⇒ PH ⇒ PTSD ⇒ Depression ⇒ LS | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | −3.33 | <0.001 |
| Age ⇒ PH ⇒ Depression ⇒ LS | 0.00 | 0.00 | −0.01 | 0.00 | 0.00 | −4.35 | <0.001 |
| Age ⇒ Depression ⇒ LS | 0.01 | 0.00 | 0.00 | 0.02 | 0.01 | 2.66 | 0.008 |
| PA ⇒ PH ⇒ LS | 0.17 | 0.04 | 0.10 | 0.24 | 0.01 | 4.72 | <0.001 |
| PA ⇒ PH ⇒ PTSD ⇒ Depression ⇒ LS | 0.01 | 0.00 | 0.00 | 0.01 | 0.00 | 3.25 | 0.001 |
| PA ⇒ PH ⇒ Depression ⇒ LS | 0.02 | 0.01 | 0.01 | 0.04 | 0.00 | 3.91 | <0.001 |
| PTSD ⇒ Depression ⇒ LS | −0.04 | 0.00 | −0.04 | −0.03 | −0.07 | −8.29 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogowska, A.M.; Kuśnierz, C.; Pavlova, I.; Chilicka, K. A Path Model for Subjective Well-Being during the Second Wave of the COVID-19 Pandemic: A Comparative Study among Polish and Ukrainian University Students. J. Clin. Med. 2022, 11, 4726. https://doi.org/10.3390/jcm11164726
Rogowska AM, Kuśnierz C, Pavlova I, Chilicka K. A Path Model for Subjective Well-Being during the Second Wave of the COVID-19 Pandemic: A Comparative Study among Polish and Ukrainian University Students. Journal of Clinical Medicine. 2022; 11(16):4726. https://doi.org/10.3390/jcm11164726
Chicago/Turabian StyleRogowska, Aleksandra M., Cezary Kuśnierz, Iuliia Pavlova, and Karolina Chilicka. 2022. "A Path Model for Subjective Well-Being during the Second Wave of the COVID-19 Pandemic: A Comparative Study among Polish and Ukrainian University Students" Journal of Clinical Medicine 11, no. 16: 4726. https://doi.org/10.3390/jcm11164726