
Polymorphisms of the 11q23.3 Locus Affect the Risk and Mortality of Coronary Artery Disease

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Controls
2.2. Serum Lipid Measurement
2.3. Genetic Analysis
2.4. Follow-Up and Events
2.5. Statistical Analysis
- -
- For the multiplicative synergy index (SIM):
- -
- For Rothman’s additive synergy index (SI):
- -
- For the relative excess risk due to interaction (RERI):
- -
- For the proportion attributable to interaction (AP):
3. Results
3.1. Study Group Characteristics
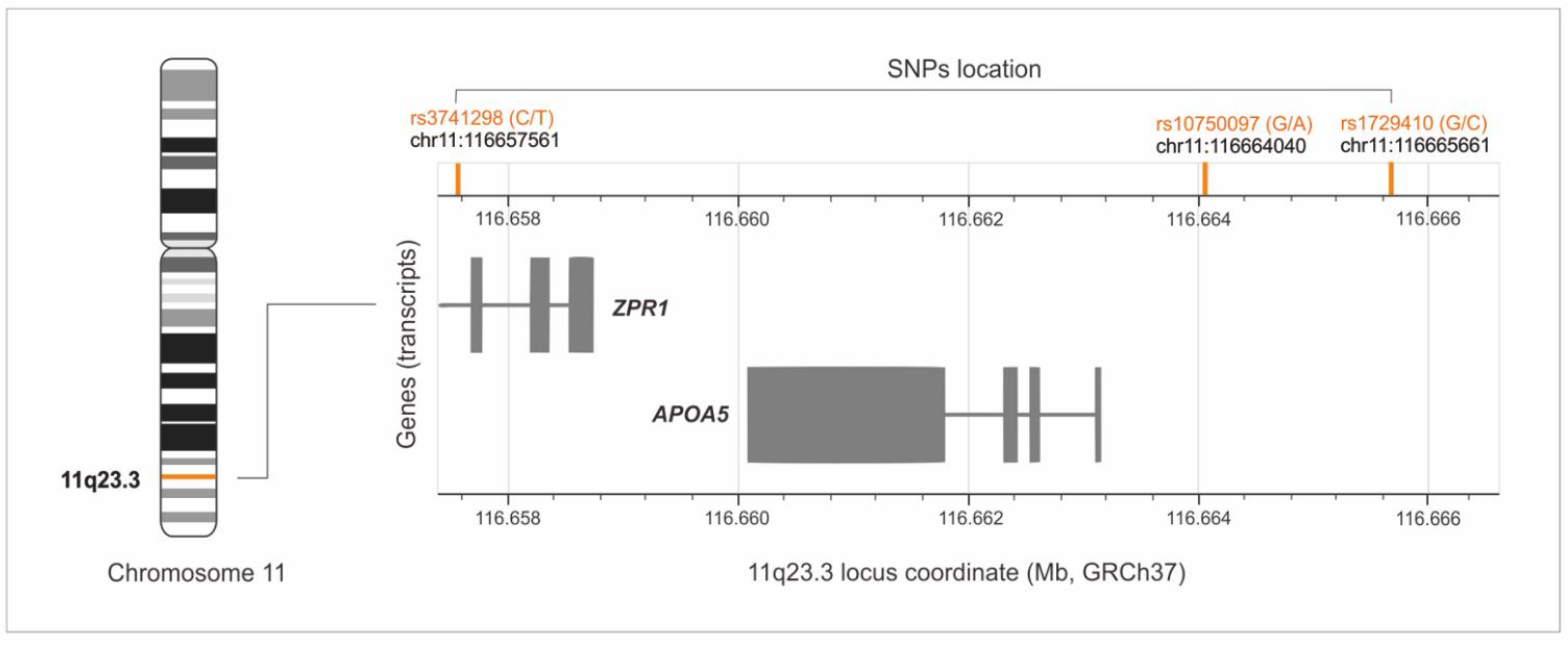
3.2. Analysis of the rs1729410, rs10750097, and rs3741298 Polymorphisms in CAD and Control Subjects
3.3. Analysis of Association between Polymorphisms and CAD Clinical Phenotypes
3.4. Analysis of Association between Polymorphisms and CAD Lipid Parameters
3.5. Biological Interactions between Genotypes of Analyzed Polymorphisms and Traditional Risk Factors of CAD
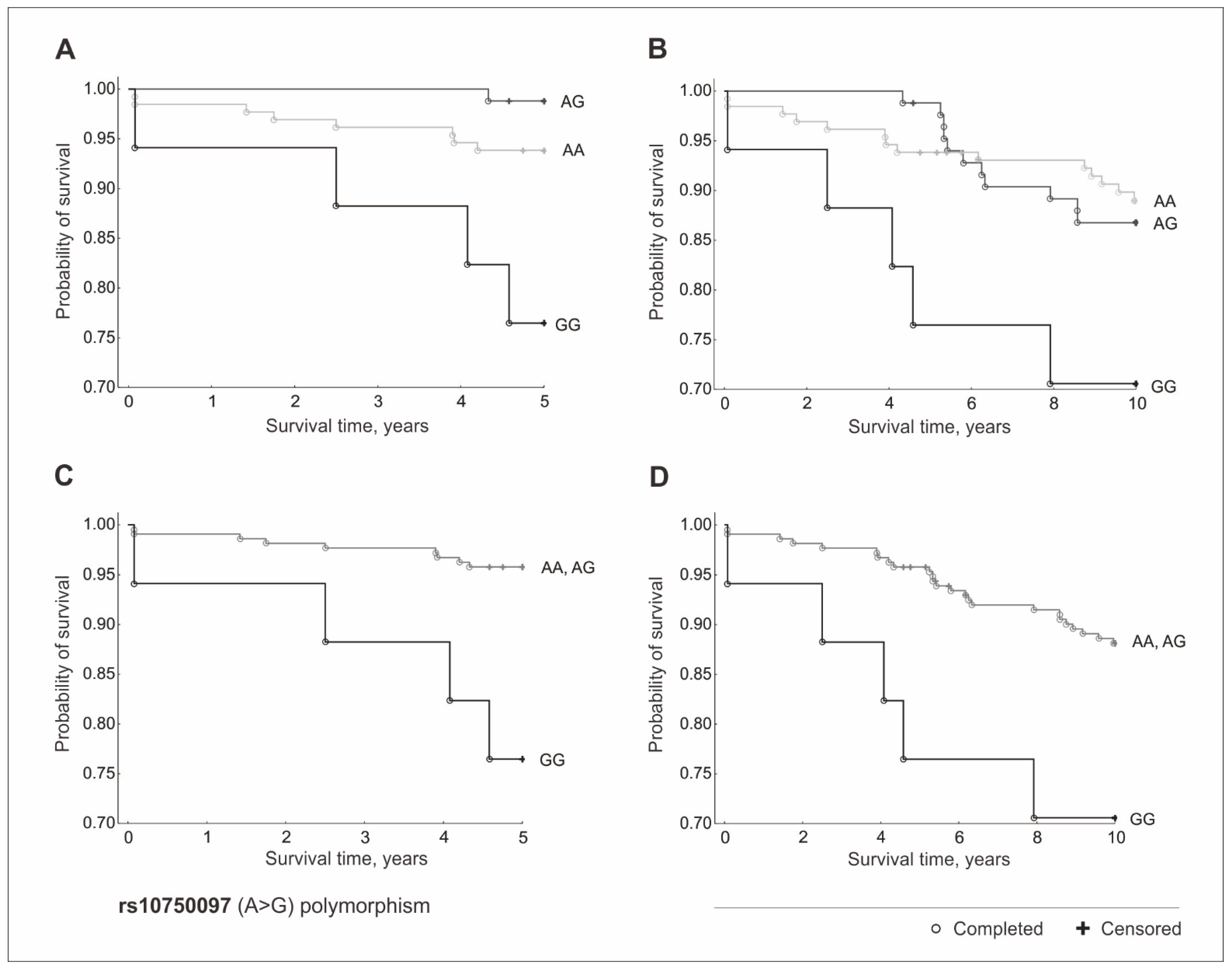
3.6. Survival and Mortality Analysis of Patients with Coronary Artery Disease
3.7. Polymorphisms of the 11q23.3 Locus and Mortality of CAD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Choy, P.C.; Siow, Y.L.; Mymin, D.; O, K. Lipids, and atherosclerosis. Biochem. Cell Biol. 2004, 82, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Kreisberg, R.A.; Oberman, A. Clinical review 141: Lipids and atherosclerosis: Lessons learned from randomized controlled trials of lipid lowering and other relevant studies. J. Clin. Endocrinol. Metab. 2002, 87, 423–437. [Google Scholar] [CrossRef] [PubMed]
- Pranav Chand, R.; Kumar, A.S.; Anuj, K.; Vishnupriya, S.; Mohan Reddy, B. Distinct Patterns of Association of Variants at 11q23.3 Chromosomal Region with Coronary Artery Disease and Dyslipidemia in the Population of Andhra Pradesh, India. PLoS ONE 2016, 11, e0153720. [Google Scholar] [CrossRef] [PubMed]
- López-Mejías, R.; Genre, F.; García-Bermúdez, M.; Castañeda, S.; González-Juanatey, C.; Llorca, J.; Corrales, A.; Miranda-Filloy, J.A.; Rueda-Gotor, J.; Gómez-Vaquero, C.; et al. The 11q23.3 genomic region-rs964184-is associated with cardiovascular disease in patients with rheumatoid arthritis. Tissue Antigens 2013, 82, 344–347. [Google Scholar] [CrossRef] [PubMed]
- López-Mejías, R.; Castañeda, S.; González-Juanatey, C.; Corrales, A.; Ferraz-Amaro, I.; Genre, F.; Remuzgo-Martínez, S.; Rodriguez-Rodriguez, L.; Blanco, R.; Llorca, J.; et al. Cardiovascular risk assessment in patients with rheumatoid arthritis: The relevance of clinical, genetic and serological markers. Autoimmun. Rev. 2016, 15, 1013–1030. [Google Scholar] [CrossRef] [Green Version]
- Brautbar, A.; Covarrubias, D.; Belmont, J.; Lara-Garduno, F.; Virani, S.S.; Jones, P.H.; Leal, S.M.; Ballantyne, C.M. Variants in the APOA5 gene region and the response to combination therapy with statins and fenofibric acid in a randomized clinical trial of individuals with mixed dyslipidemia. Atherosclerosis 2011, 219, 737–742. [Google Scholar] [CrossRef]
- Feitosa, M.F.; Wojczynski, M.K.; Straka, R.; Kammerer, C.M.; Lee, J.H.; Kraja, A.T.; Christensen, K.; Newman, A.B.; Province, M.A.; Borecki, I.B. Genetic analysis of long-lived families reveals novel variants influencing high density-lipoprotein cholesterol. Front. Genet. 2014, 5, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reilly, D.; Hao, K.; Jensen, M.K.; Girman, C.J.; Rimm, E.B. Use of systems biology approaches to analysis of genome-wide association studies of myocardial infarction and blood cholesterol in the nurses’ health study and health professionals’ follow-up study. PLoS ONE 2013, 8, e85369. [Google Scholar] [CrossRef] [Green Version]
- Pranavchand, R.; Kumar, A.S.; Reddy, B.M. Genetic determinants of clinical heterogeneity of the coronary artery disease in the population of Hyderabad, India. Hum. Genom. 2017, 11, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, C.Q.; Liu, B.; Cheung, B.M.; Lam, T.H.; Lin, J.M.; Li, J.Y.; Yue, X.J.; Ong, K.L.; Tam, S.; Wong, K.S.; et al. A single nucleotide polymorphism in APOA5 determines triglyceride levels in Hong Kong and Guangzhou Chinese. Eur. J. Hum. Genet. 2010, 18, 1255–1260. [Google Scholar] [CrossRef] [Green Version]
- Machiela, M.J.; Chanock, S.J. LDlink: A web-based application for exploring population-specific haplotype structure and linking correlated alleles of possible functional variants. Bioinformatics 2015, 31, 3555–3557. [Google Scholar] [CrossRef]
- Niemiec, P.; Zak, I.; Wita, K. The 242T variant of the CYBA gene polymorphism increases the risk of coronary artery disease associated with cigarette smoking and hypercholesterolemia. Coron. Artery Dis. 2007, 18, 339–346. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Horita, N.; Kaneko, T. Genetic model selection for a case-control study and a meta-analysis. Meta Gene 2015, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Knol, M.J.; VanderWeele, T.J.; Groenwold, R.H.; Klungel, O.H.; Rovers, M.M.; Grobbee, D.E. Estimating measures of interaction on an additive scale for preventive exposures. Eur. J. Epidemiol. 2011, 26, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Knol, M.J.; VanderWeele, T.J. Recommendations for presenting analyses of effect modification and interaction. Int. J. Epidemiol. 2012, 41, 514–520. [Google Scholar] [CrossRef] [Green Version]
- Zou, G.Y. On the estimation of additive interaction by use of the four-by-two table and beyond. Am. J. Epidemiol. 2008, 168, 212–224. [Google Scholar] [CrossRef]
- Wee, C.C.; Mukamal, K.J.; Huang, A.; Davis, R.B.; McCarth, E.P.; Mittleman, M.A. Obesity and C-reactive protein levels among white, black, and hispanic US adults. Obesity 2008, 16, 875–880. [Google Scholar] [CrossRef]
- Ryo, M.; Nakamura, T.; Kihara, S.; Kumada, M.; Shibazaki, S.; Takahashi, M.; Nagai, M.; Matsuzawa, Y.; Funahashi, T. Adiponectin as a biomarker of the metabolic syndrome. Circ. J. 2004, 68, 975–981. [Google Scholar] [CrossRef] [Green Version]
- Yudkin, J.S.; Kumari, M.; Humphries, S.E.; Mohamed-Ali, V. Inflammation, obesity, stress and coronary heart disease: Is interleukin-6 the link? Atherosclerosis 2000, 148, 209–214. [Google Scholar] [CrossRef]
- Keaney, J.F.; Larson, M.G.; Vasan, R.S.; Wilson, P.W.; Lipinska, I.; Corey, D.; Massaro, J.M.; Sutherland, P.; Vita, J.A.; Benjamin, E.J. Obesity and systemic oxidative stress: Clinical correlates of oxidative stress in the Framingham Study. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 434–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, W.; Long, J.; Cheng, Y.; Chen, Y.; Zhao, S. Elevated plasma lipoprotein(a) levels were associated with increased risk of cardiovascular events in Chinese patients with stable coronary artery disease. Sci. Rep. 2018, 8, 7726. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.K.; Hu, M.; Baum, L.; Thomas, G.N.; Tomlinson, B. Associations of polymorphisms in the apolipoprotein A1/C3/A4/A5 gene cluster with familial combined hyperlipidaemia in Hong Kong Chinese. Atherosclerosis 2010, 208, 427–432. [Google Scholar] [CrossRef]
- Shirts, B.H.; Howard, M.T.; Hasstedt, S.J.; Nanjee, M.N.; Knight, S.; Carlquist, J.F.; Anderson, J.L.; Hopkins, P.N.; Hunt, S.C. Vitamin D dependent effects of APOA5 polymorphisms on HDL cholesterol. Atherosclerosis 2012, 222, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Kassi, E.; Adamopoulos, C.; Basdra, E.K.; Papavassiliou, A.G. Role of vitamin D in atherosclerosis. Circulation 2013, 128, 2517–2531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elbers, C.C.; Guo, Y.; Tragante, V.; van Iperen, E.P.; Lanktree, M.B.; Castillo, B.A.; Chen, F.; Yanek, L.R.; Wojczynski, M.K.; Li, Y.R.; et al. Gene-centric meta-analysis of lipid traits in African, East Asian and Hispanic populations. PLoS ONE 2012, 7, e50198. [Google Scholar]
- Sidore, C.; Busonero, F.; Maschio, A.; Porcu, E.; Naitza, S.; Zoledziewska, M.; Mulas, A.; Pistis, G.; Steri, M.; Danjou, F.; et al. Genome sequencing elucidates Sardinian genetic architecture and augments association analyses for lipid and blood inflammatory markers. Nat. Genet. 2015, 47, 1272–1281. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, R.; Jahan, N.; Sun, Y.; Xue, H. Genetic association of lipid metabolism related SNPs with myocardial infarction in the Pakistani population. Mol. Biol. Rep. 2014, 41, 1545–1552. [Google Scholar] [CrossRef]
- Ong, K.L.; Jiang, C.Q.; Liu, B.; Jin, Y.L.; Tso, A.W.; Tam, S.; Wong, K.S.; Tomlinson, B.; Cheung, B.M.; Lin, J.M.; et al. Association of a genetic variant in the apolipoprotein A5 gene with the metabolic syndrome in Chinese. Clin. Endocrinol. 2011, 74, 206–213. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | CAD n = 248 | Controls n = 243 | OR * (95% CI) | p |
|---|---|---|---|---|
| Age (years), median (QD) | 45.00 (4.00) | 43.00 (4.00) | - | 0.06 |
| Male gender, n (%) | 165 (66.53) | 174 (71.60) | 0.79 (0.54–1.16) | 0.22 |
| TC (mmol/L), median (QD) | 5.71 (0.97) | 4.92 (0.74) | - | <10−6 |
| HDL (mmol/L), median (QD) | 1.04 (0.14) | 1.33 (0.39) | - | <10−6 |
| LDL (mmol/L), median (QD) | 3.81 (0.84) | 2.80 (0.77) | - | <10−6 |
| TG (mmol/L), median (QD) | 1.73 (0.52) | 1.29 (0.40) | - | <10−6 |
| BMI, mean (SD) | 26.60 (2.76) | 25.40 (2.27) | - | 0.02 |
| Cigarette smoking, n (%) | 140 (56.45) | 66 (27.16) | 3.48 (2.38–5.07) | <10−7 |
| SNPs | rs3741298 | rs10750097 | rs1729410 |
|---|---|---|---|
| rs3741298 | 1.000 | 0.314 | 0.006 |
| rs10750097 | 0.314 | 1.000 | 0.000 |
| rs1729410 | 0.006 | 0.000 | 1.000 |
| Genotype/ Allele | CAD n (%) | Controls n (%) | Inheritance Model | OR (95% CI) | p |
|---|---|---|---|---|---|
| rs1729410 | |||||
| GG | 57 (25.00) | 56 (23.63) | Dominant, vs. GC + CC | 1.07 (0.70–1.65) | 0.73 |
| GC | 121 (53.07) | 109 (45.99) | Additive, vs. GG | 1.09 (0.69–1.71) | 0.71 |
| CC | 50 (21.93) | 72 (30.38) | Additive, vs. GG | 0.68 (0.41–1.14) | 0.15 |
| GC + GG | 178 (78.07) | 165 (69.62) | Recessive, vs. CC | 1.55 (1.02–2.36) | 0.04 * |
| C | 221 (48.46) | 253 (53.38) | - | 0.82 (0.64–1.06) | 0.13 |
| G | 235 (51.54) | 221 (46.62) | - | 1.21 (0.94–1.57) | 0.13 |
| rs10750097 | |||||
| AA | 128 (56.64) | 143 (63.84) | Dominant, vs. AG + GG | 0.74 (0.51–1.08) | 0.12 |
| AG | 84 (37.17) | 68 (30.36) | Additive, vs. AA | 1.38 (0.93–2.06) | 0.11 |
| GG | 14 (6.19) | 13 (5.80) | Additive, vs. AA | 1.20 (0.54–2.65) | 0.65 |
| AG + AA | 212 (93.80) | 211 (94.20) | Recessive, vs. GG | 0.93 (0.43–2.03) | 0.86 |
| G | 112 (24.78) | 94 (20.98) | - | 1.24 (0.91–1.70) | 0.18 |
| A | 340 (75.22) | 354 (79.02) | - | 0.81 (0.59–1.10) | 0.18 |
| rs3741298 | |||||
| TT | 120 (54.05) | 145 (61.44) | Dominant, vs. TC + CC | 0.74 (0.51–1.07) | 0.10 |
| TC | 91 (40.99) | 78 (33.05) | Additive, vs. TT | 1.41 (0.96–2.08) | 0.08 |
| CC | 11 (4.96) | 13 (5.51) | Additive, vs. TT | 1.02 (0.44–2.36) | 0.96 |
| TC + TT | 211 (95.04) | 223 (94.50) | Recessive, vs. CC | 1.12 (0.49–2.55) | 0.79 |
| C | 113 (25.45) | 104 (22.03) | - | 1.21 (0.89–1.64) | 0.23 |
| T | 331 (74.55) | 368 (77.97) | - | 0.83 (0.61–1.12) | 0.23 |
| GG Genotype, rs10750097 | Cigarette Smoking | CAD | Controls | OR | 95% CI | |
|---|---|---|---|---|---|---|
| n | n | Lower Limit | Upper Limit | |||
| 0 | 0 | 85 | 151 | 1 | - | - |
| 0 | 1 | 123 | 59 | 3.70 | 2.46 | 5.57 |
| 1 | 0 | 2 | 11 | 0.32 | 0.07 | 1.49 |
| 1 | 1 | 12 | 2 | 10.66 | 2.33 | 48.75 |
| G Allele, rs1729410 | BMI ≥ 25 | CAD | Controls | OR | 95% CI | |
|---|---|---|---|---|---|---|
| n | n | Lower Limit | Upper Limit | |||
| 0 | 0 | 25 | 37 | 1 | - | - |
| 0 | 1 | 17 | 34 | 0.74 | 0.34 | 1.60 |
| 1 | 0 | 67 | 75 | 1.32 | 0.72 | 2.42 |
| 1 | 1 | 99 | 87 | 1.68 | 0.94 | 3.02 |
| GG Genotype, rs1729410 | TC ≥ 5 mmol/L | CAD | Controls | OR | 95% CI | |
|---|---|---|---|---|---|---|
| n | n | Lower Limit | Upper Limit | |||
| 0 | 0 | 57 | 98 | 1 | - | - |
| 0 | 1 | 100 | 71 | 2.19 | 1.43 | 3.35 |
| 1 | 0 | 7 | 29 | 0.42 | 0.17 | 1.01 |
| 1 | 1 | 46 | 27 | 2.95 | 1.67 | 5.23 |
| GG genotype, rs1729410 | LDL ≥ 3 mmol/L | CAD | Controls | OR | 95% CI | |
| n | n | Lower limit | Upper limit | |||
| 0 | 0 | 41 | 42 | 1 | - | - |
| 0 | 1 | 114 | 92 | 1.27 | 0.76 | 2.11 |
| 1 | 0 | 4 | 32 | 0.13 | 0.04 | 0.39 |
| 1 | 1 | 47 | 24 | 2.01 | 1.04 | 3.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwanicki, T.; Iwanicka, J.; Balcerzyk-Matić, A.; Nowak, T.; Mizia-Stec, K.; Bańka, P.; Filipecki, A.; Krauze, J.; Jarosz, A.; Górczyńska-Kosiorz, S.; et al. Polymorphisms of the 11q23.3 Locus Affect the Risk and Mortality of Coronary Artery Disease. J. Clin. Med. 2022, 11, 4532. https://doi.org/10.3390/jcm11154532
Iwanicki T, Iwanicka J, Balcerzyk-Matić A, Nowak T, Mizia-Stec K, Bańka P, Filipecki A, Krauze J, Jarosz A, Górczyńska-Kosiorz S, et al. Polymorphisms of the 11q23.3 Locus Affect the Risk and Mortality of Coronary Artery Disease. Journal of Clinical Medicine. 2022; 11(15):4532. https://doi.org/10.3390/jcm11154532
Chicago/Turabian StyleIwanicki, Tomasz, Joanna Iwanicka, Anna Balcerzyk-Matić, Tomasz Nowak, Katarzyna Mizia-Stec, Paweł Bańka, Artur Filipecki, Jolanta Krauze, Alicja Jarosz, Sylwia Górczyńska-Kosiorz, and et al. 2022. "Polymorphisms of the 11q23.3 Locus Affect the Risk and Mortality of Coronary Artery Disease" Journal of Clinical Medicine 11, no. 15: 4532. https://doi.org/10.3390/jcm11154532