
Effectiveness of a Multifaced Antibiotic Stewardship Program: A Pre-Post Study in Seven Italian ICUs

 ,
,  ,
,  , , , ,
, , , ,  , , , , and add
Show full author list
, , , , and add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participating Units
2.3. Study Population
2.4. Data Collection and Management
2.5. Phases of the Project
2.6. Outcomes
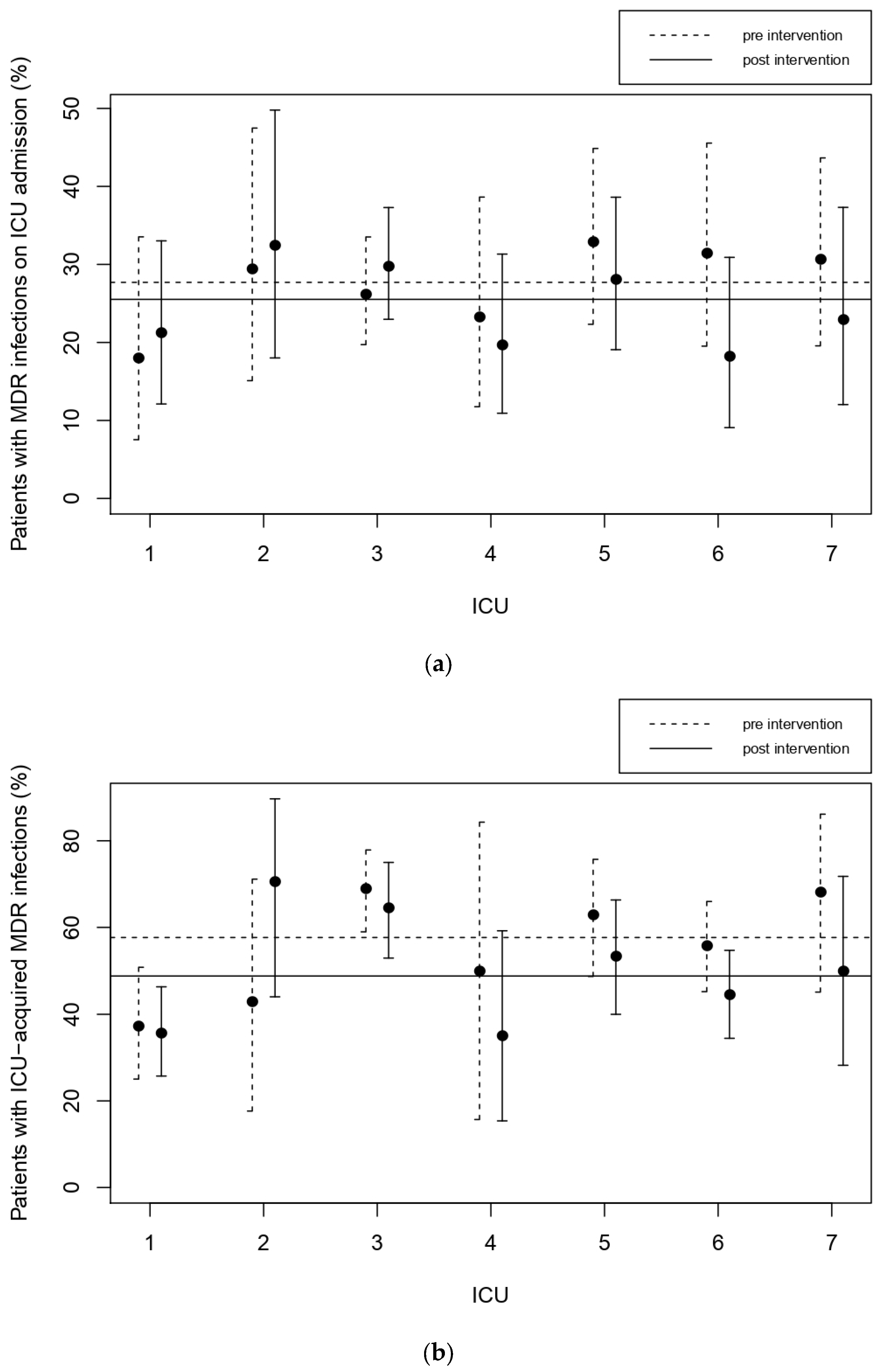
2.6.1. Frequency of Patients with MDR Infections
2.6.2. Median Duration of Empirical Therapy and Prophylaxis
2.6.3. Inappropriateness of Antibiotics by Penetration into the Site of Infection
2.6.4. Inappropriateness of Antibiotics by Microorganism Resistance Pattern
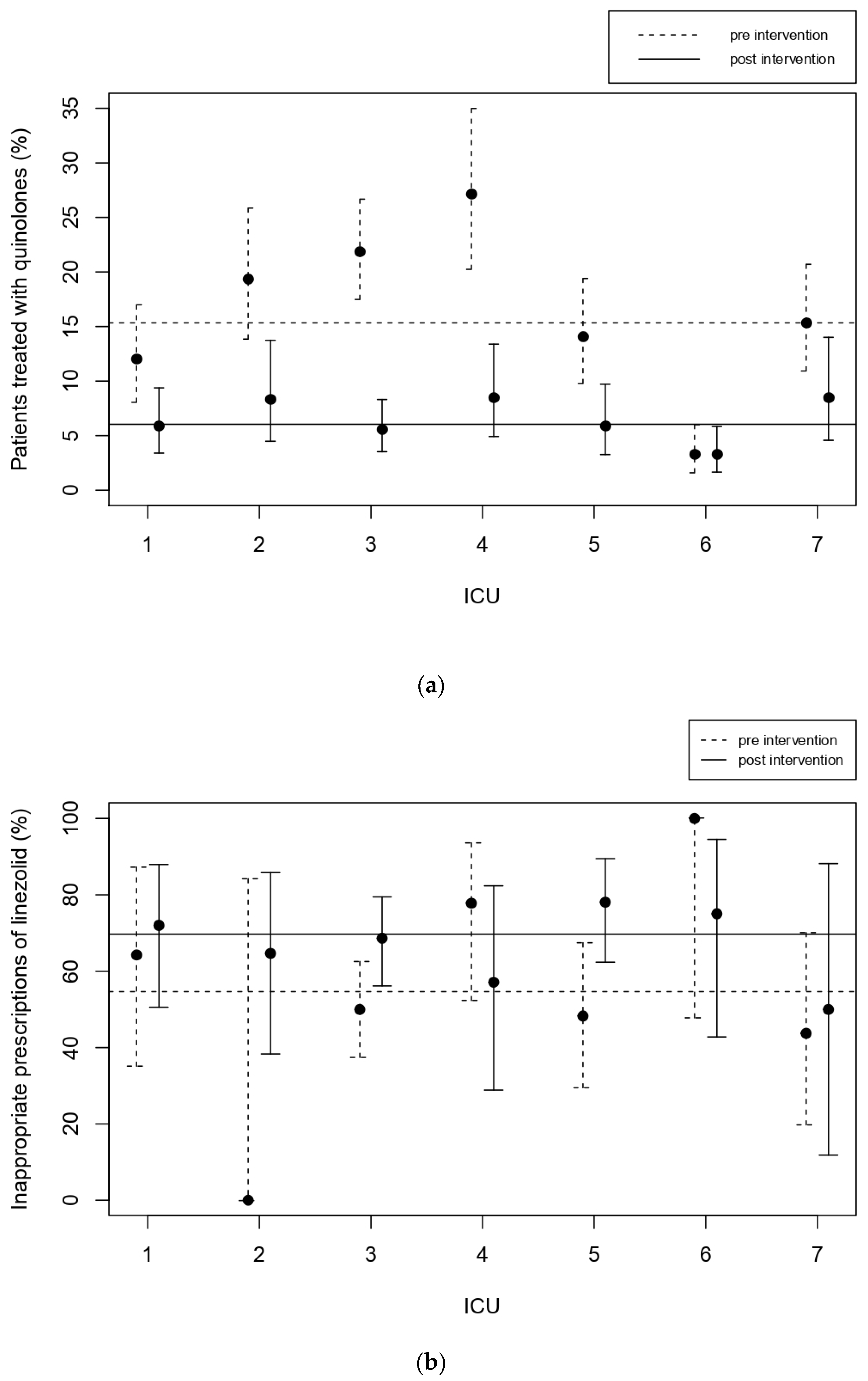
2.6.5. Use of Fluoroquinolone Antibiotics
2.6.6. Inappropriate Prescriptions of Carbapenems
2.6.7. Inappropriate Prescriptions of Colistin
2.6.8. Inappropriate Prescriptions of Linezolid
- -
- Antibiotic pressure: Proportion of days of ICU stay when patients received any antibiotic therapy.
- -
- Average ICU length of stay.
- -
- ICU mortality.
2.7. Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- French, G.L. Clinical Impact and Relevance of Antibiotic Resistance. Adv. Drug Deliv. Rev. 2005, 57, 1514–1527. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Report on Surveillance of Antibiotic Consumption: 2016–2018 Early Implementation; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Livermore, D.M. Minimising Antibiotic Resistance. Lancet Infect. Dis. 2005, 5, 450–459. [Google Scholar] [CrossRef]
- Davey, P.; Brown, E.; Charani, E.; Fenelon, L.; Gould, I.M.; Holmes, A.; Ramsay, C.R.; Wiffen, P.J.; Wilcox, M. Interventions to Improve Antibiotic Prescribing Practices for Hospital Inpatients. Cochrane Database Syst. Rev. 2013, 4, CD003543. [Google Scholar]
- Tamma, P.D.; Miller, M.A.; Cosgrove, S.E. Rethinking How Antibiotics Are Prescribed: Incorporating the 4 Moments of Antibiotic Decision Making into Clinical Practice. JAMA 2019, 321, 139–140. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Milkowska-Shibata, M.; Tseng, K.K.; Sharland, M.; Gandra, S.; Pulcini, C.; Laxminarayan, R. Assessment of WHO Antibiotic Consumption and Access Targets in 76 Countries, 2000–15: An Analysis of Pharmaceutical Sales Data. Lancet Infect. Dis. 2021, 21, 107–115. [Google Scholar] [CrossRef]
- Zhang, Y.-Z.; Singh, S. Antibiotic Stewardship Programmes in Intensive Care Units: Why, How, and Where Are They Leading Us. World J. Crit. Care Med. 2015, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Taggart, L.R.; Leung, E.; Muller, M.P.; Matukas, L.M.; Daneman, N. Differential Outcome of an Antimicrobial Stewardship Audit and Feedback Program in Two Intensive Care Units: A Controlled Interrupted Time Series Study. BMC Infect. Dis. 2015, 15, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Álvarez-Lerma, F.; Grau, S.; Echeverría-Esnal, D.; Martínez-Alonso, M.; Gracia-Arnillas, M.P.; Horcajada, J.P.; Masclans, J.R. A Before-and-after Study of the Effectiveness of an Antimicrobial Stewardship Program in Critical Care. Antimicrob. Agents Chemother. 2018, 62, e01825-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thursky, K.A.; Buising, K.L.; Bak, N.; Macgregor, L.; Street, A.C.; Macintyre, C.R.; Presneill, J.J.; Cade, J.F.; Brown, G.V. Reduction of Broad-Spectrum Antibiotic Use with Computerized Decision Support in an Intensive Care Unit. Int. J. Qual. Health Care 2006, 18, 224–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, V.; Gill, S.; Sauve, J.; Walker, K.; Stumpo, C.; Powis, J. Growing a “Positive Culture” of Antimicrobial Stewardship in a Community Hospital. Can. J. Hosp. Pharm. 2011, 64, 314. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; Beriault, D.; Schwartz, K.L.; Seah, J.; Pasic, M.D.; Cirone, R.; Chan, A.; Downing, M. A Real-World Assessment of Procalcitonin Combined with Antimicrobial Stewardship in a Community ICU. J. Crit. Care 2020, 57, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-Y.; Chiu, C.-H.; Huang, C.-T.; Cheng, C.-W.; Lin, Y.-J.; Hsu, Y.-J.; Chen, C.-H.; Deng, S.-T.; Leu, H.-S. Blood Culture-Guided de-Escalation of Empirical Antimicrobial Regimen for Critical Patients in an Online Antimicrobial Stewardship Programme. Int. J. Antimicrob. Agents 2014, 44, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Ramsamy, Y.; Muckart, D.J.J.; Han, K.S.S. Microbiological Surveillance and Antimicrobial Stewardship Minimise the Need for Ultrabroad-Spectrum Combination Therapy for Treatment of Nosocomial Infections in a Trauma Intensive Care Unit: An Audit of an Evidence-Based Empiric Antimicrobial Policy. S. Afr. Med. J. 2013, 103, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Doernberg, S.B.; Chambers, H.F. Antimicrobial Stewardship Approaches in the Intensive Care Unit. Infect. Dis. Clin. 2017, 31, 513–534. [Google Scholar] [CrossRef] [PubMed]
- De Waele, J.J.; Akova, M.; Antonelli, M.; Canton, R.; Carlet, J.; De Backer, D.; Dimopoulos, G.; Garnacho-Montero, J.; Kesecioglu, J.; Lipman, J. Antimicrobial Resistance and Antibiotic Stewardship Programs in the ICU: Insistence and Persistence in the Fight against Resistance. A Position Statement from ESICM/ESCMID/WAAAR Round Table on Multi-Drug Resistance. Intensive Care Med. 2018, 44, 189–196. [Google Scholar] [CrossRef]
- Finazzi, S.; Mandelli, G.; Garbero, E.; Mondini, M.; Trussardi, G.; Giardino, M.; Tavola, M.; Bertolini, G. Data Collection and Research with MargheritaTre. Physiol. Meas. 2018, 39, 084004. [Google Scholar] [CrossRef] [PubMed]
- Finazzi, S.; Luci, G.; Olivieri, C.; Langer, M.; Mandelli, G.; Gori, A.; Viaggi, B.; Di Paolo, A. Tissue penetration of antimicrobials in intensive care unit patients: A systematic review—Part II. Antibiotics 2022, 11. submitted. [Google Scholar]
- Leclercq, R.; Cantón, R.; Brown, D.F.; Giske, C.G.; Heisig, P.; MacGowan, A.P.; Mouton, J.W.; Nordmann, P.; Rodloff, A.C.; Rossolini, G.M. EUCAST Expert Rules in Antimicrobial Susceptibility Testing. Clin. Microbiol. Infect. 2013, 19, 141–160. [Google Scholar] [CrossRef] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 8.1. 2018. Available online: http://www.eucast.org/Clinical_breakpoints/ (accessed on 20 May 2020).
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 9.0. 2019. Available online: http://www.eucast.or/Clinical_breakpoints/ (accessed on 20 May 2020).
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 28th ed.; CLSI Supplement M100; Wayne, P.A., Ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 29th ed.; CLSI Supplement M100; Wayne, P.A., Ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2019. [Google Scholar]
- Carlet, J.; Ali, A.B.; Chalfine, A. Epidemiology and Control of Antibiotic Resistance in the Intensive Care Unit. Curr. Opin. Infect. Dis. 2004, 17, 309–316. [Google Scholar] [CrossRef]
- Apisarnthanarak, A.; Pinitchai, U.; Warachan, B.; Warren, D.K.; Khawcharoenporn, T.; Hayden, M.K. Effectiveness of Infection Prevention Measures Featuring Advanced Source Control and Environmental Cleaning to Limit Transmission of Extremely-Drug Resistant Acinetobacter Baumannii in a Thai Intensive Care Unit: An Analysis before and after Extensive Flooding. Am. J. Infect. Control 2014, 42, 116–121. [Google Scholar] [PubMed]
- Frattari, A.; Savini, V.; Polilli, E.; Di Marco, G.; Lucisano, G.; Corridoni, S.; Spina, T.; Costantini, A.; Nicolucci, A.; Fazii, P. Control of Gram-Negative Multi-Drug Resistant Microorganisms in an Italian ICU: Rapid Decline as a Result of a Multifaceted Intervention, Including Conservative Use of Antibiotics. Int. J. Infect. Dis. 2019, 84, 153–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, S.W.; Anderson, D.J.; May, D.B.; Drew, R.H. Utility of a Clinical Risk Factor Scoring Model in Predicting Infection with Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae on Hospital Admission. Infect. Control Hosp. Epidemiol. 2013, 34, 385–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tumbarello, M.; Trecarichi, E.M.; Bassetti, M.; De Rosa, F.G.; Spanu, T.; Di Meco, E.; Losito, A.R.; Parisini, A.; Pagani, N.; Cauda, R. Identifying Patients Harboring Extended-Spectrum-β-Lactamase-Producing Enterobacteriaceae on Hospital Admission: Derivation and Validation of a Scoring System. Antimicrob. Agents Chemother. 2011, 55, 3485–3490. [Google Scholar] [CrossRef] [Green Version]
- Tumbarello, M.; Trecarichi, E.M.; Tumietto, F.; Del Bono, V.; De Rosa, F.G.; Bassetti, M.; Losito, A.R.; Tedeschi, S.; Saffioti, C.; Corcione, S. Predictive Models for Identification of Hospitalized Patients Harboring KPC-Producing Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2014, 58, 3514–3520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Bij, A.K.; Pitout, J.D. The Role of International Travel in the Worldwide Spread of Multiresistant Enterobacteriaceae. J. Antimicrob. Chemother. 2012, 67, 2090–2100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassetti, M.; Carnelutti, A.; Peghin, M. Patient Specific Risk Stratification for Antimicrobial Resistance and Possible Treatment Strategies in Gram-Negative Bacterial Infections. Expert Rev. Anti-Infect. Ther. 2017, 15, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Mojica, M.F.; Rossi, M.-A.; Vila, A.J.; Bonomo, R.A. The Urgent Need for Metallo-β-Lactamase Inhibitors: An Unattended Global Threat. Lancet Infect. Dis. 2021, 22, e28–e34. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (6290) | Pre-Intervention (2901) | Post-Intervention (3389) | p-Value | ||
|---|---|---|---|---|---|
| Median Age (Q1, Q3) | 66 (51, 77) | 67 (52, 77) | 65 (51, 76) | 0.003 | *** |
| Male | 3816 (60.7%) | 1755 (60.5%) | 2061 (60.8%) | 0.80 | |
| ICU Outcome | 1011 (16.1%) | 471 (16.2%) | 540 (15.9%) | 0.75 | |
| Comorbidities | |||||
| Hypertension | 2818 (48.9%) | 1321 (48.4%) | 1497 (49.4%) | 0.48 | |
| Severe Obesity (BMI > 35) | 979 (17.0%) | 440 (16.1%) | 539 (17.8%) | 0.10 | |
| Arrythmia | 839 (14.6%) | 391 (14.3%) | 448 (14.8%) | 0.64 | |
| Type 2 Diabetes | 1018 (17.7%) | 460 (16.9%) | 558 (18.4%) | 0.13 | |
| BPCO | 840 (14.6%) | 401 (14.7%) | 439 (14.5%) | 0.81 | |
| Tumor | 683 (11.9%) | 348 (12.8%) | 335 (11.0%) | 0.05 | * |
| Myocardial Infarction | 531 (9.2%) | 241 (8.8%) | 290 (9.6%) | 0.34 | |
| Moderate/Severe Renal Failure | 450 (7.8%) | 193 (7.1%) | 257 (8.5%) | 0.05 | * |
| NYHA 2, 3 | 450 (7.8%) | 208 (7.6%) | 242 (8.0%) | 0.62 | |
| Vasculopathy | 409 (7.1%) | 239 (8.8%) | 170 (5.6%) | <0.001 | *** |
| No comorbidities | 1069 (18.6%) | 552 (20.2%) | 517 (17.1%) | 0.002 | ** |
| Infections on admission | |||||
| Pneumonia | 579 (9.7%) | 286 (10.6%) | 293 (9.0%) | 0.04 | * |
| Clinical sepsis | 226 (3.8%) | 98 (3.6%) | 128 (3.9%) | 0.56 | |
| Peritonitis | 241 (4.1%) | 118 (4.4%) | 123 (3.8%) | 0.24 | |
| Urinary tract infections | 116 (1.9%) | 50 (1.9%) | 66 (2.0%) | 0.64 | |
| Skin/soft-tissue Infection | 102 (1.7%) | 45 (1.7%) | 57 (1.8%) | 0.81 | |
| No infections | 4488 (75.4%) | 2009 (74.6%) | 2479 (76.1%) | 0.16 | |
| ICU acquired infections | |||||
| Pneumonia | 599 (9.5%) | 285 (9.8%) | 314 (9.3%) | 0.45 | |
| Lower respiratory tract infection | 211 (3.4%) | 103 (3.6%) | 108 (3.2%) | 0.43 | |
| Clinical Sepsis | 100 (1.6%) | 49 (1.7%) | 51 (1.5%) | 0.560 | |
| Primary bloodstream infection | 128 (2.0%) | 60 (2.1%) | 68 (2.0%) | 0.86 | |
| Urinary tract infection | 95 (1.5%) | 39 (1.3%) | 56 (1.7%) | 0.32 | |
| Pre-Intervention | Post-Intervention | p-Value | ||
|---|---|---|---|---|
| Frequency of patients with MDR infections (N/D) | 44.9% (315/701) | 39.5% (305/772) | 0.11 | |
| On admission (N/D) | 27.7% (131/473) | 25.5% (135/529 | 0.59 | |
| ICU acquired (N/D) | 57.7% (203/352) | 48.8% (189/387) | 0.09 | |
| Median (IQR) duration of empirical therapy (D) | 5.6 days (1275) | 4.6 days (1406) | <0.001 | *** |
| Median duration of prophylaxis (D) | 2.3 days (589) | 2.0 days (584) | 0.06 | |
| Inappropriateness of antibiotics by penetration into the site of infection (N/D) | 2.3% (49/2117) | 1.9% (49/2619) | 0.26 | |
| Inappropriateness of antibiotics by microorganism resistance pattern in empirical therapy (N/D) | 16.2% (57/351) | 17.3% (67/387) | 0.84 | |
| Inappropriateness of antibiotics by microorganism resistance pattern in targeted therapy (N/D) | 3.8% (19/507) | 4.8% (29/606) | 0.29 | |
| Use of quinolones (N/D) | 15.3% (251/1637) | 6.0% (105/1737) | <0.001 | *** |
| Inappropriate prescriptions of carbapenems in empirical therapy (N/D) | 45.2% (19/42) | 36.9% (24/65) | 0.51 | |
| Inappropriate prescriptions of carbapenems in targeted therapy (N/D) | 36.7% (18/49) | 55.3% (42/76) | 0.07 | |
| Inappropriate prescriptions of colistin in targeted therapy | 27.6% (8/29) | 40% (2/5) | 0.61 | |
| Inappropriate prescriptions of linezolid (N/D) | 54.9% (82/150) | 69.8% (127/182) | 0.01 | * |
| Average ICU Length of stay (D) | 5.5 days (2901) | 5.4 days (3389) | 0.07 | |
| ICU Mortality (N/D) | 16.2% (471/2901) | 15.9% (540/3389) | 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mandelli, G.; Dore, F.; Langer, M.; Garbero, E.; Alagna, L.; Bianchin, A.; Ciceri, R.; Di Paolo, A.; Giani, T.; Giugni, A.; et al. Effectiveness of a Multifaced Antibiotic Stewardship Program: A Pre-Post Study in Seven Italian ICUs. J. Clin. Med. 2022, 11, 4409. https://doi.org/10.3390/jcm11154409
Mandelli G, Dore F, Langer M, Garbero E, Alagna L, Bianchin A, Ciceri R, Di Paolo A, Giani T, Giugni A, et al. Effectiveness of a Multifaced Antibiotic Stewardship Program: A Pre-Post Study in Seven Italian ICUs. Journal of Clinical Medicine. 2022; 11(15):4409. https://doi.org/10.3390/jcm11154409
Chicago/Turabian StyleMandelli, Giulia, Francesca Dore, Martin Langer, Elena Garbero, Laura Alagna, Andrea Bianchin, Rita Ciceri, Antonello Di Paolo, Tommaso Giani, Aimone Giugni, and et al. 2022. "Effectiveness of a Multifaced Antibiotic Stewardship Program: A Pre-Post Study in Seven Italian ICUs" Journal of Clinical Medicine 11, no. 15: 4409. https://doi.org/10.3390/jcm11154409