
NT-proBNP Levels Influence the Prognostic Value of Mineral Metabolism Biomarkers in Coronary Artery Disease

 , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Study Design
2.3. Analytical and Biomarker Studies
2.4. Statistical Analysis
2.5. Ethics Statement
3. Results
3.1. Patients
3.2. Clinical Events
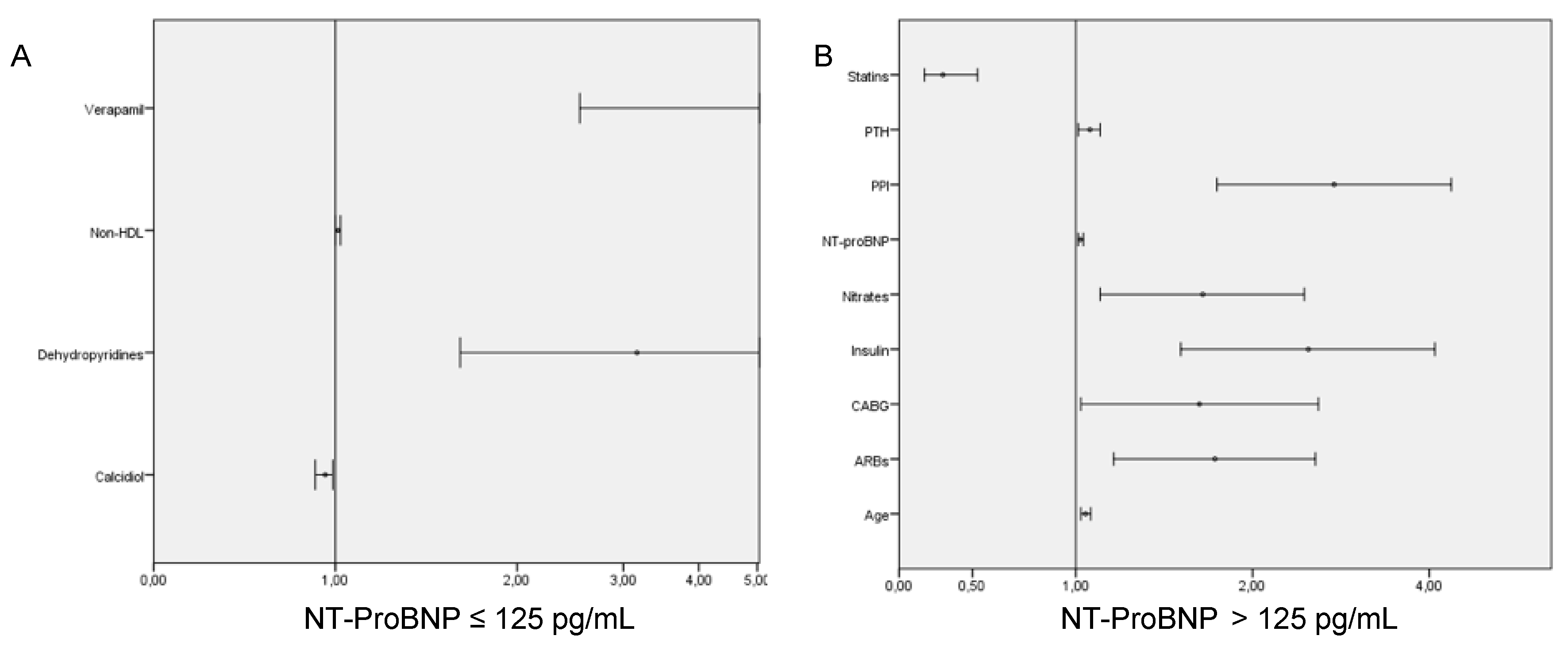
3.3. Prognostic Value of the Components of Mineral Metabolism According to NT-proBNP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martín-Ventura, J.L.; Blanco-Colio, L.M.; Tuñón, J.; Muñoz-García, B.; Madrigal-Matute, J.; Moreno, J.A.; de Ceniga, M.; Egido, J. Biomarkers in cardiovascular medicine. Rev. Esp. Cardiol. 2009, 62, 677–688. [Google Scholar] [CrossRef]
- Vasan, R.S. Biomarkers of cardiovascular disease. Circulation 2006, 113, 2335–2362. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.S.; Krishnaswamy, P.; Nowak, R.M.; Mccord, J.; Hollander, J.; Duc, P.; Omland, T.; Storrow, A.B.; Abraham, W.T.; Wu, A.H.; et al. Breathing not properly multinational study I. Rapid measurement of B-type natriuretic peptide in the emergencydiagnosis of heart failure. N. Engl. J. Med. 2002, 347, 161–167. [Google Scholar] [CrossRef]
- Tuñón, J.; Blanco-Colio, L.; Cristóbal, C.; Tarín, N.; Higueras, J.; Huelmos, A.; Alonso, J.; Egido, J.; Asensio, D.; Lorenzo, O.; et al. Usefulness of a combination of monocyte chemoattractant protein-1, Galectin-3, and N-Terminal probrain natriuretic peptide to predict cardiovascular events in patients with coronary artery disease. Am. J. Cardiol. 2014, 113, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Daniels, L.B.; Maisel, A.S. Natriuretic peptides. J. Am. Coll. Cardiol. 2007, 50, 2357–2368. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.-H.; Cao, Y.-X.; Jin, J.-L.; Guo, Y.-L.; Zhu, C.-G.; Wu, N.-Q.; Gao, Y.; Zhang, Y.; Xu, R.-X.; Dong, Q.; et al. Prognostic value of NT-proBNP in patients with chronic coronary syndrome and normal left ventricular systolic function according to glucose status: A prospective cohort study. Cardiovasc. Diabetol. 2021, 20, 84. [Google Scholar] [CrossRef]
- Ndrepepa, G.; Braun, S.; Niemöller, K.; Mehilli, J.; von Beckerath, N.; von Beckerath, O.; von Beckerath, N.; Vogt, W.; Schomig, A.; Kastrati, A. Prognostic value of N-Terminal pro–brain natriuretic peptide in patients with chronic stable angina. Circulation 2005, 112, 2102–2107. [Google Scholar] [CrossRef] [Green Version]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [Green Version]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Gardner, R.S.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contributio. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Gullestad, L.; Ueland, T.; Kjekshus, J.; Nymo, S.H.; Hulthe, J.; Muntendam, P.; Adourian, A.; Böhm, M.; van Veldhuisen, D.J.; Komajda, M.; et al. Galectin-3 predicts response to statin therapy in the controlled rosuvastatin multinational trial in heart failure (CORONA). Eur. Heart J. 2012, 33, 2290–2296. [Google Scholar] [CrossRef] [Green Version]
- Kestenbaum, B.; Katz, R.; de Boer, I.; Hoofnagle, A.; Sarnak, M.J.; Shlipak, M.G.; Jenny, N.S.; Siscovick, D.S. Vitamin D, parathyroid hormone, and cardiovascular events among older adults. J. Am. Coll. Cardiol. 2011, 58, 1433–1441. [Google Scholar] [CrossRef] [Green Version]
- Aceña, Á.; Pello, A.M.; Carda, R.; Lorenzo, Ó.; Gonzalez-Casaus, M.L.; Blanco-Colio, L.M.; Ventura, J.L.; Orejas, M.; Rabago, R.; Gonzalez-Parra, E.; et al. Parathormone levels are independently associated with the presence of left ventricular hypertrophy in patients with coronary artery disease. J. Nutr. Health Aging 2016, 20, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.C.; Hayen, A.; Macaskill, P.; Pellegrini, F.; Craig, J.C.; Elder, G.J.; Strippoli, G.F.M. Serum Levels of phosphorus, parathyroid hormone, and calcium and risks of death and cardiovascular disease in individuals with chronic kidney disease: A systematic review and meta-analysis. JAMA 2011, 305, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Welsh, P.; Papacosta, O.; Lennon, L.; Whincup, P.H.; Sattar, N. Elevated parathyroid hormone, but not vitamin D deficiency, is associated with increased risk of heart failure in older men with and without cardiovascular disease. Circ. Heart Fail. 2014, 7, 732–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Parra, E.; Rojas-Rivera, J.; Tuñón, J.; Praga, M.; Ortiz, A.; Egido, J. Vitamin D receptor activation and cardiovascular disease. Nephrol. Dial. Transpl. 2012, 27, iv17–iv21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, B.D.; Schurgers, L.J.; Brandenburg, V.M.; Christenson, R.H.; Vermeer, C.; Ketteler, M.; Shlipak, M.G.; Whooley, M.A. The associations of fibroblast growth factor 23 and uncarboxylated matrix gla protein with mortality in coronary artery disease: The heart and soul study. Ann. Intern Med. 2010, 152, 640–648. [Google Scholar] [CrossRef] [Green Version]
- Tuñón, J.; Cristóbal, C.; Tarín, N.; Aceña, Á.; González-Casaus, M.L.; Huelmos, A.; Alonso, J.; Lorenzo, Ó.; González-Parra, E.; Mahíllo-Fernández, I.; et al. Coexistence of low vitamin D and high fibroblast growth factor-23 plasma levels predicts an adverse outcome in patients with coronary artery disease. PLoS ONE 2014, 9, e95402. [Google Scholar] [CrossRef] [Green Version]
- Faul, C.; Amaral, A.P.; Oskouei, B.; Hu, M.-C.; Sloan, A.; Isakova, T.; Gutiérrez, O.M.; Aguillon-Prada, R.; Lincoln, J.; Hare, J.M.; et al. FGF23 induces left ventricular hypertrophy. J. Clin. Investig. 2011, 121, 4393–4408. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez-Landaluce, C.; Aceña, Á.; Pello, A.; Martínez-Milla, J.; González-Lorenzo, Ó.; Tarín, N.; Cristóbal, C.; Blanco-Colio, L.M.; Martín-Ventura, J.L.; Huelmos, A.; et al. Parathormone levels add prognostic ability to N-terminal pro-brain natriuretic peptide in stable coronary patients. ESC Heart Fail. 2021, 8, 2713–2722. [Google Scholar] [CrossRef]
- Mueller, C.; McDonald, K.; de Boer, R.A.; Maisel, A.; Cleland, J.G.F.; Kozhuharov, N.; Coats, A.J.; Metra, M.; Mebazza, A.; Kozhurov, N.; et al. Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations. Eur. J. Heart Fail. 2019, 21, 715–731. [Google Scholar] [CrossRef] [Green Version]
- Meijers, W.C.; Bayes-Genis, A.; Mebazaa, A.; Bauersachs, J.; Cleland, J.G.F.; Coats, A.J.S.; Januzzi, J.L.; Maisel, A.S.; McDonald, K.; Mueller, T.; et al. Circulating heart failure biomarkers beyond natriuretic peptides: Review from the Biomarker Study Group of the Heart Failure Association (HFA), European Society of Cardiology (ESC). Eur. J. Heart Fail. 2021, 23, 1610–1632. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.L.; Vanwoerkom, R.C.; Horne, B.D.; Bair, T.L.; May, H.T.; Lappé, D.L.; Muhleistein, J.B. Parathyroid hormone, vitamin D, renal dysfunction, and cardiovascular disease: Dependent or independent risk factors? Am. Heart J. 2011, 162, 331–339.e2. [Google Scholar] [CrossRef] [PubMed]
- Taylor, E.N.; Curhan, G.C.; Forman, J.P. Parathyroid hormone and the risk of incident hypertension. J. Hypertens. 2008, 26, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Kuroo, M.; Matsumura, Y.; Aizawa, H.; Kawaguchi, H.; Suga, T.; Utsugi, T.; Ohyama, Y.; Kurabayashi, M.; Kaname, T.; Kume, E.; et al. Mutation of the mouse klotho gene leads to a syndrome resembling ageing. Nature 1997, 390, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Higueras, J.; Martín-Ventura, J.L.; Blanco-Colio, L.; Cristóbal, C.; Tarín, N.; Huelmos, A.; Alonso, J.; Pello, A.; Aceña, Á.; Carda, R.; et al. Impacto de los niveles plasmáticos de pro-péptido natriurético tipo B aminoterminal, proteína quimiotáctica de monocitos-1 y galectina3 en la capacidad predictiva de eventos de la escala clínica LIPID en la enfermedad coronaria estable. Impact of plasma pro-B-type natriuretic peptide amino-terminal and galectin-3 levels on the predictive capacity of the LIPID Clinical Risk Scale in stable coronary disease. Clin. Investig. Arterioscler. 2015, 27, 57–63. [Google Scholar] [PubMed] [Green Version]
- Brøndum-Jacobsen, P.; Benn, M.; Jensen, G.B.; Nordestgaard, B.G. 25-Hydroxyvitamin D Levels and Risk of Ischemic Heart Disease, Myocardial Infarction, and Early Death. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2794–2802. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Moreno, J.M.; Herencia, C.; de Oca, A.M.; Muñoz-Castañeda, J.R.; Rodríguez-Ortiz, M.E.; Díaz-Tocados, J.M.; Peralbo-Santealla, E.; Camargo, A.; Canalejo, A.; Rodriguez, M.; et al. Vitamin D modulates tissue factor and protease-activated receptor 2 expression in vascular smooth muscle cells. FASEB J. 2016, 30, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Drüeke, T.B.; Massy, Z.A. Role of vitamin D in vascular calcification: Bad guy or good guy? Nephrol. Dial. Transpl. 2012, 27, 1704–1707. [Google Scholar] [CrossRef] [Green Version]
- Hsia, J.; Heiss, G.; Ren, H.; Allison, M.; Dolan, N.C.; Greenland, P.; Heckbert, S.R.; Johnson, K.C.; Manson, J.E.; Sidney, S.; et al. Calcium/Vitamin D Supplementation and Cardiovascular Events. Circulation 2007, 115, 846–854. [Google Scholar] [CrossRef] [Green Version]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A.; Sundus, S.; Bachuwa, G.; Alkotob, M.L.; et al. Vitamin D Supplementation and Cardiovascular Disease Risks in More Than 83,000 Individuals in 21 Randomized Clinical Trials: A Meta-analysis. JAMA Cardiol. 2019, 4, 765–776. [Google Scholar] [CrossRef]
- Bansal, N.; Zelnick, L.; Robinson-Cohen, C.; Hoofnagle, A.N.; Ix, J.H.; Lima, J.A.; Shoben, A.B.; Peralta, C.; Siscovick, D.S.; Kestenbaum, B.; et al. Serum parathyroid hormone and 25-hydroxyvitamin D concentrations and risk of incident heart failure: The Multi-Ethnic Study of Atherosclerosis. J. Am. Heart Assoc. 2014, 3, e001278. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | NT-ProBNP ≤ 125 N = 342 | NT-ProBNP > 125 N = 622 | p |
|---|---|---|---|
| Age (y) | 54.0 (48.0–61.0) | 65.0 (56.0–75.0) | <0.001 |
| Female (%) | 17.3 | 27.3 | <0.001 |
| Race: Caucasian (%) | 95.6 | 97.4 | 0.127 |
| Body mass index (kg/m2) | 28.4 (25.8–30.5) | 27.9 (25.6–30.8) | 0.359 |
| Smoker (%) | 19.3 | 10.9 | <0.001 |
| Hypertension (%) | 49.1 | 72.5 | <0.001 |
| Diabetes (%) | 20.8 | 25.9 | 0.075 |
| Dyslipidemia (%) | 71.9 | 73.0 | 0.734 |
| Peripheral artery disease (%) | 3.5 | 3.9 | 0.784 |
| Cerebrovascular disease (%) | 0.3 | 4.2 | <0.001 |
| Prior CABG (%) | 4.1 | 10.1 | 0.001 |
| LVEF < 40 (%) | 0.9 | 10.5 | <0.001 |
| Prior heart failure (%) | 2.9 | 16.4 | <0.001 |
| Atrial fibrillation (%) | 1.5 | 9.0 | <0.001 |
| TREATMENT | |||
| Aspirin (%) | 94.7 | 92.9 | 0.273 |
| P2Y12 antagonist (%) | 78.1 | 74.0 | 0.156 |
| Anticoagulant (%) | 1.8 | 7.6 | <0.001 |
| Statin (%) | 95.9 | 94.2 | 0.256 |
| High potency statin (%) | 59.4 | 57.7 | 0.621 |
| Ezetimibe (%) | 5.0 | 3.7 | 0.343 |
| Insulin (%) | 4.4 | 7.9 | 0.037 |
| Oral antidiabetic drug (%) | 15.5 | 18.0 | 0.322 |
| ACEI (%) | 59.4 | 64.3 | 0.129 |
| ARB (%) | 12.3 | 17.0 | 0.050 |
| Aldosterone antagonist (%) | 2.0 | 9.3 | <0.001 |
| Betablocker (%) | 73.4 | 82.2 | 0.001 |
| Diltiazem (%) | 3.2 | 2.4 | 0.461 |
| Verapamil (%) | 0.6 | 0.2 | 0.258 |
| Dihydropyridine (%) | 12.0 | 14.8 | 0.227 |
| Diuretic (%) | 12.6 | 22.2 | <0.001 |
| Nitrates (%) | 10.2 | 14.5 | 0.061 |
| PPI (%) | 67.5 | 69.9 | 0.442 |
| Digoxin (%) | 0.0 | 0.5 | 0.556 |
| Vitamin D | 1.5 | 1.3 | 0.779 |
| PREVIOUS ACUTE CORONARY SYNDROME | |||
| STEMI/Non-STEMI (%) | 39.2/60.8 | 55.3/44.7 | <0.001 |
| Number of vessels diseased | |||
| Revascularization method (%) | 0.064 | ||
| • No revascularization | 15.8 | 14.1 | |
| • Drug-eluting stent | 56.1 | 50.2 | |
| • Bare metal stent | 23.4 | 26.4 | |
| • Angioplasty | 1.8 | 3.4 | |
| • CABG | 2.9 | 5.9 | |
| ANALYTICS | |||
| Glucose (mg/dL) | 100.0 (91.0–114.25) | 101.0 (91.7–115.2) | 0.401 |
| Total cholesterol (mg/dL) | 145.5 (124.0–166.0) | 141.0 (124.7–161.0) | 0.110 |
| HDL cholesterol (mg/dL) | 39.0 (31.4–46.0) | 41.0 (35.0–47.0) | 0.029 |
| LDL cholesterol (mg/dL) | 79.0 (65.0–93.0) | 76.0 (64.0–92.0) | 0.240 |
| Non-HDL cholesterol (mg/dL) | 103.0 (85.0–122.2) | 99.0 (83.7–116) | 0.048 |
| Triglyceride (mg/dL) | 104.5 (77.5–152.0) | 100.0 (76.0–137.0) | 0.081 |
| eGFR (mL/min/1.73 m2) | 87.4 (75.8–97.9) | 75.2 (59.2–89.1) | <0.001 |
| HsCRP (mg/L) | 1.0 (0.3–2.6) | 1.1 (0.3–3.2) | 0.324 |
| Nt-ProBNP (ng/L) | 71.5 (47.2–95.8) | 305.0 (187.7–578.0) | <0.001 |
| HsTroponin (µg/L) | 0.0 (0.0–0.004) | 0.005 (0.001–0.014) | <0.001 |
| Phosphate (mmol/L) | 3.1 (2.7–3.5) | 3.2 (2.8–3.5) | 0.310 |
| Calcidiol (mmol/L) | 19.3 (14.5–25.7) | 19.1 (14.2–25.2) | 0.779 |
| FGF 23 (RU/mL) | 72.7 (56.3–94.9) | 82.0 (62.1–108.6) | <0.001 |
| Klotho (pg/mL) | 588.7 (496.1–730.0) | 555.6 (462.7–679.8) | 0.003 |
| PTH (ng/L) | 54.8 (42.1–70.3) | 59.8 (45.9–76.9) | 0.001 |
| MCP-1 (pg/mL) | 121.4 (95.2–155.0) | 114.7 (114.2–185.6) | <0.001 |
| Galectine-3 (ng/mL) | 7.2 (5.5–9.0) | 8.3 (6.3–108.6) | <0.001 |
| Variable | HR | p |
|---|---|---|
| (A) | ||
| Caucasian race | 0.36 | 0.093 |
| High blood pressure | 1.61 | 0.123 |
| Statins | 0.50 | 0.184 |
| Ezetimbe | 2.55 | 0.049 |
| MRA | 3.25 | 0.051 |
| Betablockers | 0.50 | 0.025 |
| Nitrates | 1.69 | 0.162 |
| Verapamil | 7.47 | 0.006 |
| Dehydropiridines | 2.71 | 0.002 |
| Cholesterol levels | 1.01 | 0.042 |
| LDL cholesterol | 1.01 | 0.048 |
| Non-HDL | 1.01 | 0.031 |
| Calcidiol | 0.95 | 0.018 |
| PTH | 1.01 | 0.023 |
| (B) | ||
| Age | 1.06 | 0.037 |
| Male sex | 0.75 | 0.102 |
| Smoking | 0.60 | 0.143 |
| High blood pressure | 2.15 | 0.001 |
| Cognitive impairment | 1.63 | 0.006 |
| Previous stroke | 1.91 | 0.049 |
| Previous CABG | 1.85 | 0.008 |
| Previous heart failure admission | 2.15 | 0.000 |
| Atrial Fibrillation | 1.97 | 0.004 |
| Left ventricular dysfunction | 1.56 | 0.060 |
| P2Y12 inhibitors | 0.75 | 0.104 |
| Anticoagulation | 2.13 | 0.002 |
| Statins | 0.32 | 0.000 |
| Insulin | 2.96 | 0.000 |
| Oral antidiabetic drugs | 28.16 | 0.002 |
| ACE inhibitors | 0.73 | 0.070 |
| ARB | 1.91 | 0.001 |
| MRA | 1.69 | 0.043 |
| Betablockers | 0.61 | 0.008 |
| Nitrates | 2.34 | 0,000 |
| Diltiazem | 2.71 | 0.006 |
| Verapamil | 0.71 | 0.050 |
| Dehydropiridines | 1.36 | 0.146 |
| Diuretics | 1.93 | 0.000 |
| PPI | 2.16 | 0.000 |
| Digoxin | 3.01 | 0.122 |
| Glucose levels | 1.00 | 0.014 |
| Cholesterol levels | 1.00 | 0.139 |
| Glomerular filtration rate | 0.98 | 0.000 |
| Non-HDL cholesterol | 1.00 | 0.162 |
| High sensitive troponin | 1.40 | 0.054 |
| Nt-ProBNP 1 | 1.02 | 0.000 |
| Calcidiol | 0.99 | 0.055 |
| MCP-1 | 1.01 | 0.004 |
| Galectin-3 | 1.05 | 0.001 |
| FGF23 | 1.00 | 0.000 |
| PTH 2 | 1.09 | 0.000 |
| Klotho | 0.99 | 0.073 |
| Variable | HR | CI | p |
|---|---|---|---|
| (A) | |||
| Verapamil | 11.28 | 2.54–50.00 | 0.001 |
| Dihydropyridines | 3.16 | 1.63–6.13 | 0.001 |
| Non-HDL cholesterol | 1.01 | 1.00–1.02 | 0.014 |
| Calcidiol | 0.96 | 0.92–0.99 | 0.045 |
| (B) | |||
| Age | 1.04 | 1.02–1.06 | <0.001 |
| CABG | 1.62 | 1.02–2.59 | 0.041 |
| Statins | 0.32 | 0.19–0.53 | <0.001 |
| Insulin | 2.49 | 1.51–4.09 | <0.001 |
| ARB | 1.73 | 1.16–2.56 | 0.007 |
| Nitrates | 1.65 | 1.10–2.45 | 0.014 |
| Proton pump inhibitors | 2.75 | 1.74–4.36 | <0.001 |
| Nt-ProBNP 1 | 1.02 | 1.01–1.03 | <0.001 |
| PTH 2 | 1.06 | 1.01–1.10 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Milla, J.; Aceña, Á.; Pello, A.; López-Castillo, M.; Gaebelt, H.P.; González-Lorenzo, Ó.; Tarín, N.; Cristóbal, C.; Blanco-Colio, L.M.; Martín-Ventura, J.L.; et al. NT-proBNP Levels Influence the Prognostic Value of Mineral Metabolism Biomarkers in Coronary Artery Disease. J. Clin. Med. 2022, 11, 4153. https://doi.org/10.3390/jcm11144153
Martínez-Milla J, Aceña Á, Pello A, López-Castillo M, Gaebelt HP, González-Lorenzo Ó, Tarín N, Cristóbal C, Blanco-Colio LM, Martín-Ventura JL, et al. NT-proBNP Levels Influence the Prognostic Value of Mineral Metabolism Biomarkers in Coronary Artery Disease. Journal of Clinical Medicine. 2022; 11(14):4153. https://doi.org/10.3390/jcm11144153
Chicago/Turabian StyleMartínez-Milla, Juan, Álvaro Aceña, Ana Pello, Marta López-Castillo, Hans Paul Gaebelt, Óscar González-Lorenzo, Nieves Tarín, Carmen Cristóbal, Luis M. Blanco-Colio, José Luis Martín-Ventura, and et al. 2022. "NT-proBNP Levels Influence the Prognostic Value of Mineral Metabolism Biomarkers in Coronary Artery Disease" Journal of Clinical Medicine 11, no. 14: 4153. https://doi.org/10.3390/jcm11144153