
The Use of Intravenous Lidocaine in Perioperative Medicine: Anaesthetic, Analgesic and Immune-Modulatory Aspects

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
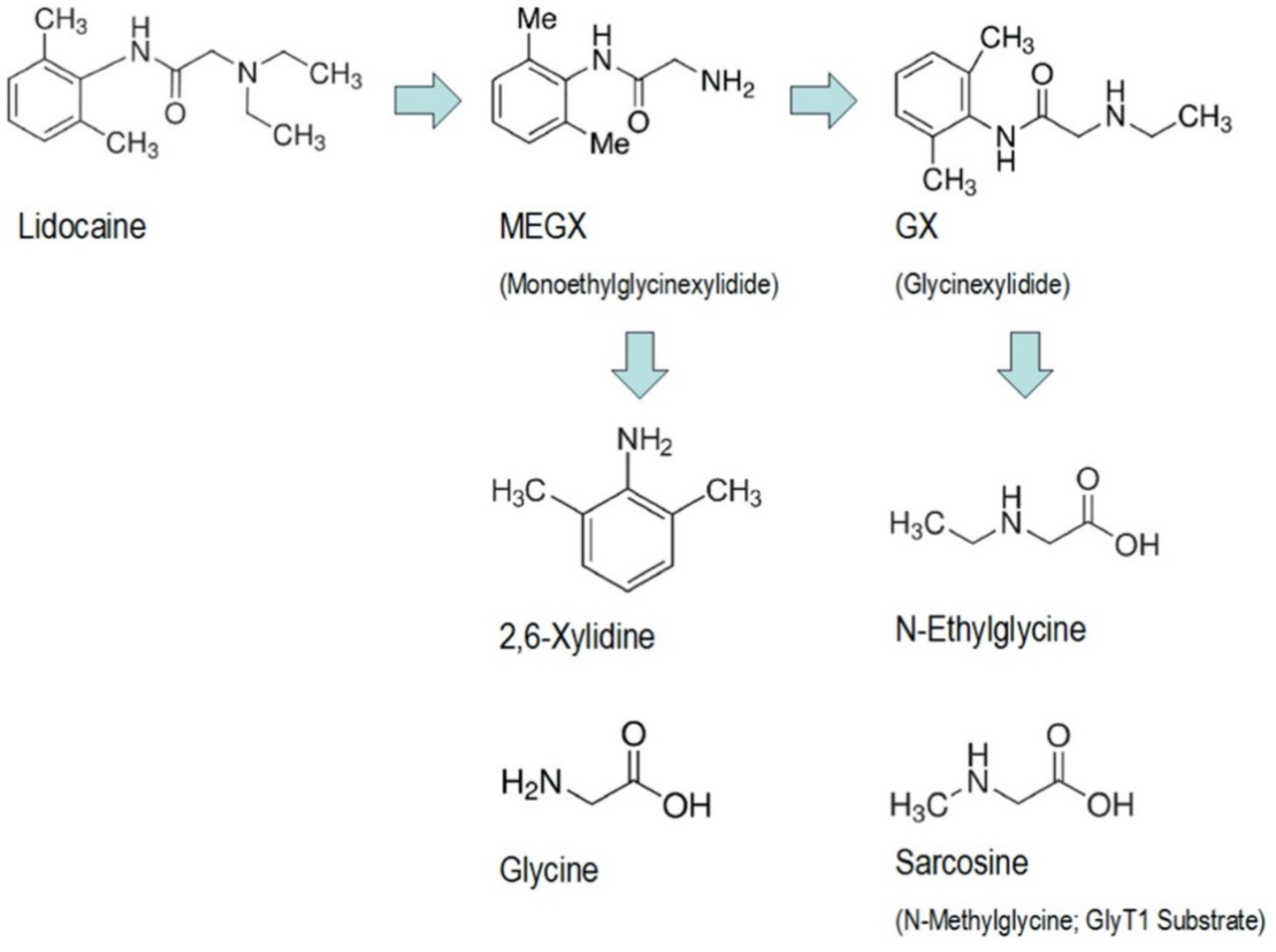
2. Pharmacology and Mechanism of Action
3. Intravenous Use
4. Clinical Properties of Lidocaine
4.1. Analgesic, Anti-Hyperalgesic and Anti-Nociceptive
4.2. Anti-Arrhythmic
4.3. Anti-Inflammatory
5. Evidence on Postoperative Outcome
5.1. Colorectal Surgery
5.2. Other Surgical Specialties
6. Immuno-Modulatory and Anti-Cancer Properties
7. Clinical Recommendations and Safety
8. Medico-Legal Implications and Licensing
9. Summary and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Löfgren, N. Studies on Local Anaesthetics: Xylocaine, a New Synthetic Drug. Ph.D. Thesis, Stockholm University, Stockholm, Sweden, 1948. [Google Scholar]
- World Health Organisation. Lidocaine. WHO Model Lists of Essential Medicine. Available online: https://list.essentialmeds.org/medicines/8 (accessed on 18 October 2021).
- World Health Organisation. WHO Model List of Essential Medicines. Available online: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2021.02 (accessed on 26 October 2021).
- National Institute for Health and Care Excellence. British National Formulary: Lidocaine. Available online: https://bnf.nice.org.uk/drug/lidocaine-hydrochloride.html (accessed on 18 October 2021).
- Beaussier, M.; Delbos, A.; Maurice-Szamburski, A.; Ecoffey, C.; Mercadal, L. Perioperative Use of Intravenous Lidocaine. Drugs 2018, 78, 1229–1246. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, C.R.; Hanson, I.R.; Brown, A.B.; Hingson, R.A. Intravenous use of xylocaine. Curr. Res. Anesth. Analg. 1951, 30, 301e13. [Google Scholar] [CrossRef]
- De Clive-Lowe, S.G.; Desmond, J.; North, J. Intravenous lignocaine anaesthesia. Anaesthesia 1958, 13, 138e46. [Google Scholar] [CrossRef]
- Bartlett, E.E.; Hutserani, O. Xylocaine for the relief of postoperative pain. Anesthesia Analg. 1961, 40, 296–304. [Google Scholar] [CrossRef]
- Hermanns, H.; Hollmann, M.W.; Stevens, M.F.; Lirk, P.; Brandenburger, T.; Piegeler, T.; Werdehausen, R. Molecular mechanisms of action of systemic lidocaine in acute and chronic pain: A narrative review. Br. J. Anaesth. 2019, 123, 335–349. [Google Scholar] [CrossRef]
- Bargetzi, M.J.; Aoyama, T.; Gonzalez, F.J.; A Meyer, U. Lidocaine metabolism in human liver microsomes by cytochrome P450IIIA4. Clin. Pharmacol. Ther. 1989, 46, 521–527. [Google Scholar] [CrossRef]
- Oellerich, M.; Burdelski, M.; Ringe, B.; Lamesch, P.; Gubernatis, G.; Bunzendahl, H.; Pichlmayr, R.; Herrmann, H. Lignocaine metabo- lite formation as a measure of pre-transplant liver function. Lancet 1989, 1, 640–642. [Google Scholar] [CrossRef]
- Thomson, A.H.; Elliott, H.L.; Kelman, A.W.; Meredith, P.A.; Whiting, B. The pharmacokinetics and pharmacodynamics of lignocaine and MEGX in healthy subjects. J. Pharmacokinet. Biopharm. 1987, 15, 101–115. [Google Scholar] [CrossRef]
- Eipe, N.; Gupta, S.; Penning, J. Intravenous lidocaine for acute pain: An evidence-based clinical update. BJA Educ. 2016, 16, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Estebe, J.P. Intravenous lidocaine. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 513–521. [Google Scholar] [CrossRef]
- Rowland, M.; Thomson, P.D.; Guichard, A.; Melmon, K.L. Disposition Kinetics of Lidocaine in Normal Subjects. Ann. N. Y. Acad. Sci. 1971, 179, 383–398. [Google Scholar] [CrossRef] [PubMed]
- Bennett, P.N.; Aarons, L.J.; Bending, M.R.; Steiner, J.A.; Rowland, M. Pharmacokinetics of lidocaine and its deethylated metabolite: Dose and time dependency studies in man. J. Pharmacokinet. Biopharm. 1982, 10, 265–281. [Google Scholar] [CrossRef] [PubMed]
- De Martin, S.; Orlando, R.; Bertoli, M.; Pegoraro, P.; Palatini, P. Differential effect of chronic renal failure on the pharmacokinetics of lidocaine in patients receiving and not receiving hemodialysis. Clin. Pharmacol. Ther. 2006, 80, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Abernethy, D.R.; Greenblatt, D.J. Impairment of Lidocaine Clearance in Elderly Male Subjects. J. Cardiovasc. Pharmacol. 1983, 5, 1093–1096. [Google Scholar] [CrossRef]
- Weinberg, L.; Peake, B.; Tan, C.; Nikfarjam, M. Pharmacokinetics and pharmacodynamics of lignocaine: A review. World J. Anesthesiol. 2015, 4, 17–29. [Google Scholar] [CrossRef]
- Nation, R.; Triggs, E.; Selig, M. Lignocaine kinetics in cardiac patients and aged subjects. Br. J. Clin. Pharmacol. 1977, 4, 439–448. [Google Scholar] [CrossRef]
- Oertel, R.; Arenz, N.; Zeitz, S.G.; Pietsch, J. Investigations into distribution of lidocaine in human autopsy material. Biomed. Chromatogr. 2015, 29, 1290–1296. [Google Scholar] [CrossRef]
- Hsu, Y.-W.; Somma, J.; Newman, M.F.; Mathew, J.P. Population Pharmacokinetics of Lidocaine Administered During and After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2011, 25, 931–936. [Google Scholar] [CrossRef] [Green Version]
- Foo, I.; Macfarlane, A.J.R.; Srivastava, D.; Bhaskar, A.; Barker, H.; Knaggs, R.; Eipe, N.; Smith, A.F. The use of intravenous lidocaine for postoperative pain and recovery: International consensus statement on efficacy and safety. Anaesthesia 2021, 76, 238–250. [Google Scholar] [CrossRef]
- Fassoulaki, A.; Melemeni, A.; Zotou, M.; Sarantopoulos, C. Systemic Ondansetron Antagonizes the Sensory Block Produced by Intrathecal Lidocaine. Anesth. Analg. 2005, 100, 1817–1821. [Google Scholar] [CrossRef]
- Kawamata, M.; Watanabe, H.; Nishikawa, K.; Takahashi, T.; Kozuka, Y.; Kawamata, T.; Omote, K.; Namiki, A. Different Mechanisms of Development and Maintenance of Experimental Incision-induced Hyperalgesia in Human Skin. Anesthesiology 2002, 97, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Holthusen, H.; Irsfeld, S.; Lipfert, P. Effect of pre- or post-traumatically applied i.v. lidocaine on primary and secondary hyperalgesia after experimental heat trauma in humans. Pain 2000, 88, 295–302. [Google Scholar] [CrossRef]
- Kawamata, M.; Takahashi, T.; Kozuka, Y.; Nawa, Y.; Nishikawa, K.; Narimatsu, E.; Watanabe, H.; Namiki, A. Experimental incision-induced pain in human skin: Effects of systemic lidocaine on flare formation and hyperalgesia. Pain 2002, 100, 77–89. [Google Scholar] [CrossRef]
- Fletcher, D.; Martinez, V. Opioid-induced hyperalgesia in patients after surgery: A systematic review and a meta-analysis. Br. J. Anaesth. 2014, 112, 991–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, W.; Li, Y.; Li, S.; Yang, W.; Jiang, J.; Han, S.; Li, J. Systemic Lidocaine Inhibits Remifentanil-induced Hyperalgesia via the Inhibition of cPKCgamma Membrane Translocation in Spinal Dorsal Horn of Rats. J. Neurosurg. Anesthesiol. 2009, 21, 318–325. [Google Scholar] [CrossRef] [Green Version]
- Tibbs, G.R.; Posson, D.J.; Goldstein, P.A. Voltage-gated ion channels in the PNS: Novel therapies for neuropathic pain? Trends Pharmacol. Sci. 2016, 37, 522e42. [Google Scholar] [CrossRef]
- Du, C.; Yu, M.; Volkow, N.D.; Koretsky, A.P.; Fowler, J.S.; Benveniste, H. Cocaine Increases the Intracellular Calcium Concentration in Brain Independently of Its Cerebrovascular Effects. J. Neurosci. 2006, 26, 11522–11531. [Google Scholar] [CrossRef]
- Fuchs, A.; Rigaud, M.; Hogan, Q.H. Painful nerve injury shortens the intracellular Ca 2þ signal in axotomized sensory neurons of rats. Anesthesiology 2007, 107, 106e16. [Google Scholar] [CrossRef] [Green Version]
- Francois, A.; Kerckhove, N.; Meleine, M.; Alloui, A.; Barrere, C.; Gelot, A.; Uebele, V.N.; Renger, J.J.; Eschalier, A.; Ardid, D.; et al. State-dependent properties of a new T-type calcium channel blocker enhance CaV3.2 selectivity and support analgesic effects. Pain 2013, 154, 283–293. [Google Scholar] [CrossRef]
- Soar, J.; Böttiger, B.W.; Carli, P.; Couper, K.; Deakin, C.D.; Djärv, T.; Lott, C.; Olasveengen, T.; Paal, P.; Pellis, T.; et al. European Resuscitation Council Guidelines 2021: Adult advanced life support. Resuscitation 2021, 161, 105–106. [Google Scholar] [CrossRef]
- Mitra, R.L.; Greenstein, S.A.; Epstein, L.M. An algorithm for managing QT prolongation in coronavirus disease 2019 (COVID-19) patients treated with either chloroquine or hydroxychloroquine in conjunction with azithromycin: Possible benefits of intravenous lidocaine. Heart Rhythm Case Rep. 2020, 6, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Fischer, L.G.; Bremer, M.; Coleman, E.J.; Conrad, B.; Krumm, B.; Gross, A.; Hollmann, M.W.; Mandell, G.; Durieux, M.E. Local Anesthetics Attenuate Lysophosphatidic Acid-Induced Priming in Human Neutrophils. Anesth. Analg. 2001, 92, 1041–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peck, S.L.; Johnston, R.B.; Horwitz, L. Reduced neutrophil superoxide anion release after prolonged infusions of lidocaine. J. Pharmacol. Exp. Ther. 1985, 235, 418–422. [Google Scholar] [PubMed]
- Sinclair, R.; Eriksson, A.S.; Gretzer, C.; Cassuto, J.; Thomsen, P. Inhibitory effects of amide local anaesthetics on stimulus-induced human leukocyte metabolic activation, LTB4release and IL-1 secretionin vitro. Acta Anaesthesiol. Scand. 1993, 37, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Yanagi, H.; Sankawa, H.; Saito, H.; Iikura, Y. Effect of lidocaine on histamine release and Ca2+ mobilization from mast cells and basophils. Acta Anaesthesiol. Scand. 1996, 40, 1138–1144. [Google Scholar] [CrossRef] [PubMed]
- Gallos, G.; Jones, D.R.; Nasr, S.H.; Emala, C.W.; Lee, H.T. Local Anesthetics Reduce Mortality and Protect against Renal and Hepatic Dysfunction in Murine Septic Peritonitis. Anesthesiology 2004, 101, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Herroeder, S.; Pecher, S.; Schönherr, M.E.; Kaulitz, G.; Hahnen- kamp, K.; Friess, H.; Böttiger, B.W.; Bauer, H.; Dijkgraaf, M.G.; Durieux, M.E.; et al. Systemic lidocaine shortens length of hospital stay after colorectal surgery: A double- blinded, randomized, placebo-controlled trial. Ann. Surg. 2007, 246, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Yardeni, I.Z.; Beilin, B.; Mayburd, E.; Levinson, Y.; Bessler, H. The Effect of Perioperative Intravenous Lidocaine on Postoperative Pain and Immune Function. Anesth. Analg. 2009, 109, 1464–1469. [Google Scholar] [CrossRef]
- Yon, J.H.; Choi, G.J.; Kang, H.; Park, J.M.; Yang, H.S. Intraoperative systemic lidocaine for pre-emptive analgesics in subtotal gas- trectomy: A prospective, randomized, double-blind, placebo- controlled study. Can. J. Surg. 2014, 57, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Weinschenk, S.; Weiss, C.; Benrath, J.; von Baehr, V.; Strowitzki, T.; Feißt, M. Anti-Inflammatory Characteristics of Local Anesthetics: Inhibition of TNF-α Secretion of Lipopolysaccharide-Stimulated Leucocytes in Human Blood Samples. Int. J. Mol. Sci. 2022, 23, 3283. [Google Scholar] [CrossRef]
- Centre for Healthcare Randomised Trials. ALLEGRO. Available online: https://w3.abdn.ac.uk/hsru/ALLEGRO/Public/Public/index.cshtml (accessed on 30 October 2021).
- Sun, Y.; Li, T.; Wang, N.; Yun, Y.; Gan, T.J. Perioperative Systemic Lidocaine for Postoperative Analgesia and Recovery after Abdominal Surgery: A meta-analysis of randomized controlled trials. Dis. Colon Rectum 2012, 55, 1183–1194. [Google Scholar] [CrossRef] [PubMed]
- Marret, E.; Rolin, M.; Beaussier, M.; Bonnet, F. Meta-analysis of intravenous lidocaine and postoperative recovery after abdominal surgery. Br. J. Surg. 2008, 95, 1331–1338. [Google Scholar] [CrossRef]
- Kranke, P.; Jokinen, J.; Pace, N.L.; Schnabel, A.; Hollmann, M.W.; Hahnenkamp, K.; Eberhart, L.H.; Poepping, D.M.; Weibel, S. Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery. Cochrane Database Syst. Rev. 2015, 7, CD009642. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, G.S., Jr.; Duncan, K.; Fitzgerald, P.; Nader, A.; Gould, R.W.; McCarthy, R.J. Systemic lidocaine to improve quality of recovery after laparoscopic bariatric surgery: A randomized double-blinded placebo-controlled trial. Obes. Surg. 2014, 24, 212–218. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, G.C.; Megalla, S.A.; Habib, A.S. Impact of intravenous lidocaine infusion on postoperative analgesia and recovery from surgery: A systematic review of randomized controlled trials. Drugs 2010, 70, 1149–1163. [Google Scholar] [CrossRef]
- Vigneault, L.; Turgeon, A.F.; Côté, D.; Lauzier, F.; Zarychanski, R.; Moore, L.; McIntyre, L.A.; Nicole, P.C.; Fergusson, D. Perioperative intravenous lidocaine infusion for postoperative pain control: A meta-analysis of randomized controlled trials. Can. J. Anaesth. 2011, 58, 22–37. [Google Scholar] [CrossRef] [PubMed]
- Weibel, S.; Jelting, Y.; Pace, N.L.; Helf, A.; Eberhart, L.H.; Hahnenkamp, K.; Hollmann, M.W.; Poepping, D.M.; Schnabel, A.; Kranke, P. Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery in adults. Cochrane Database Syst. Rev. 2018, 2018, CD009642. [Google Scholar] [CrossRef]
- Terkawi, A.S.; Tsang, S.; Kazemi, A.; Morton, S.; Luo, R.; Sanders, D.T.; Regali, L.A.; Columbano, H.; Kurtzeborn, N.Y.; Durieux, M.E. A clinical comparison of intravenous and epidural local anesthetic for major abdominal surgery. Reg. Anesth. Pain Med. 2016, 41, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Groudine, S.B.; Fisher, H.A.; Kaufman, R.P., Jr.; Patel, M.K.; Wilkins, L.J.; Mehta, S.A.; Lumb, P.D. Intravenous lidocaine speeds the return of bowel function, decreases postoperative pain, and shortens hospital stay in patients undergoing radical retropubic prostatectomy. Anesth. Analg. 1998, 86, 235–239. [Google Scholar] [CrossRef]
- Wuethrich, P.Y.; Romero, J.; Burkhard, F.C.; Curatolo, M. No benefit from perioperative intravenous lidocaine in laparoscopic renal surgery: A randomised, placebo-controlled study. Eur. J. Anaesthesiol. 2012, 29, 537–543. [Google Scholar] [CrossRef]
- Insler, S.R.; O’Connor, M.; Samonte, A.F.; Bazaral, M.G. Lidocaine and the inhibition of postoperative pain in coronary artery bypass patients. J. Cardiothorac. Vasc. Anesth. 1995, 9, 541–546. [Google Scholar] [CrossRef]
- Boswell, M.R.; Moman, R.N.; Burtoft, M.; Gerdes, H.; Martinez, J.; Gerberi, D.J.; Wittwer, E.; Murad, M.H.; Hooten, W.M. Lidocaine for postoperative pain after cardiac surgery: A systematic review. J. Cardiothorac. Surg. 2021, 16, 1–7. [Google Scholar] [CrossRef]
- Cui, W.; Li, Y.; Li, S.; Wang, R.; Li, J. Systemic administration of lidocaine reduces morphine requirements and postoperative pain of patients undergoing thoracic surgery after propofol-remifentanil-based anaesthesia. Eur. J. Anaesthesiol. 2010, 27, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Dunn, L.K.; Durieux, M. Perioperative Use of Intravenous Lidocaine. Anesthesiology 2017, 126, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Plass, F.; Nicolle, C.; Zamparini, M.; Al Issa, G.; Fiant, A.L.; Le Roux, Y.; Gérard, J.L.; Fischer, M.O.; Alvès, A.; Hanouz, J. Effect of intra-operative intravenous lidocaine on opioid consumption after bariatric surgery: A prospective, randomised, blinded, placebo-controlled study. Anaesthesia 2021, 76, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Terkawi, A.S.; Sharma, S.; Durieux, M.E.; Thammishetti, S.; Brenin, D.; Tiouririne, M. Perioperative lidocaine infusion reduces the incidence of post-mastectomy chronic pain: A double-blind, placebo-controlled randomized trial. Pain Physician 2015, 18, E139–E146. [Google Scholar]
- Wall, T.P.; Buggy, D.J. Perioperative Intravenous Lidocaine and Metastatic Cancer Recurrence—A Narrative Review. Front. Oncol. 2021, 11, 688896. [Google Scholar] [CrossRef]
- Dvorak, H.F. Tumors: Wounds that do not heal. Similarities between tumor stroma generation and wound healing. N. Engl. J. Med. 1986, 315, 1650–1659. [Google Scholar] [CrossRef]
- Alieva, M.; van Rheenen, J.; Broekman, M.L.D. Potential impact of invasive surgical procedures on primary tumor growth and metastasis. Clin. Exp. Metastasis 2018, 35, 319–331. [Google Scholar] [CrossRef] [Green Version]
- Chlebowski, R.T.; Block, J.B.; Cundiff, D.; Dietrich, M.F. Doxorubicin cytotoxicity enhanced by local anesthetics in a human melanoma cell line. Cancer Treat. Rep. 1982, 66, 121–125. [Google Scholar]
- D’Agostino, G.; Saporito, A.; Cecchinato, V.; Silvestri, Y.; Borgeat, A.; Anselmi, L.; Uguccioni, M. Lidocaine inhibits cytoskeletal remodelling and human breast cancer cell migration. Br. J. Anaesth. 2018, 121, 962–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Xiao, C.; Liu, H.; Huang, Y.; Dilger, J.P.; Lin, J. Effects of local anesthetics on breast cancer cell viability and migration. BMC Cancer 2018, 18, 666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.; Yang, J.; Han, X. Lidocaine Sensitizes the Cytotoxicity of Cisplatin in Breast Cancer Cells via Up-Regulation of RARβ2 and RASSF1A Demethylation. Int. J. Mol. Sci. 2014, 15, 23519–23536. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.W.Y.; Xie, J.X.J.; Liu, W.L.W.; Zhang, R.Z.R.; Huang, S.H.S.; Xing, Y.X.Y. Lidocaine sensitizes the cytotoxicity of 5-fluorouacil in melanoma cells via upregulation of microRNA-493. Pharmazie 2017, 72, 663–669. [Google Scholar] [CrossRef]
- Zhang, X.; Pang, W.; Liu, H.; Wang, J. Lidocine potentiates the cytotoxicity of 5-fluorouracil to choriocarcinoma cells by downregulating ABC transport proteins expression. J. Cell. Biochem. 2019, 120, 16533–16542. [Google Scholar] [CrossRef]
- Freeman, J.; Crowley, P.D.; Foley, A.G.; Gallagher, H.C.; Iwasaki, M.; Ma, D.; Buggy, D.J. Effect of Perioperative Lidocaine, Propofol and Steroids on Pulmonary Metastasis in a Murine Model of Breast Cancer Surgery. Cancers 2019, 11, 613. [Google Scholar] [CrossRef] [Green Version]
- Galoș, E.V.; Tat, T.-F.; Popa, R.; Efrimescu, C.-I.; Finnerty, D.; Buggy, D.J.; Ionescu, D.C.; Mihu, C.M. Neutrophil extracellular trapping and angiogenesis biomarkers after intravenous or inhalation anaesthesia with or without intravenous lidocaine for breast cancer surgery: A prospective, randomised trial. Br. J. Anaesth. 2020, 125, 712–721. [Google Scholar] [CrossRef]
- Johnson, M.; Crowley, P.; Foley, A.; Xue, C.; Gallagher, H.; Buggy, D. Does perioperative i.v. lidocaine infusion during tumour resection surgery reduce metastatic disease in the 4T1 mouse model of breast cancer? Br. J. Anaesth. 2018, 120, e1–e2. [Google Scholar] [CrossRef] [Green Version]
- Fraser, S.P.; Diss, J.K.; Chioni, A.M.; Mycielska, M.E.; Pan, H.; Yamaci, R.F. Voltage-gated sodium channel expression and potentiation of human breast cancer metas- tasis. Clin. Cancer Res. 2005, 11, 5381–5389. [Google Scholar] [CrossRef] [Green Version]
- Piegeler, T.; Schläpfer, M.; Dull, R.O.; Schwartz, D.E.; Borgeat, A.; Minshall, R.D.; Beck-Schimmer, B. Clinically relevant concentrations of lidocaine and ropivacaine inhibit TNFα-induced invasion of lung adenocarcinoma cells in vitro by blocking the activation of Akt and focal adhesion kinase. Br. J. Anaesth. 2015, 115, 784–791. [Google Scholar] [CrossRef] [Green Version]
- Akkuş, M.; Öner, E. Can local infiltration of lidocaine reduce the postoperative atrial fibrillation rate in patients undergoing lobectomy for lung cancer? Acta Chir. Belg. 2019, 23, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Xing, W.; Chen, D.-T.; Pan, J.-H.; Chen, Y.-H.; Yan, Y.; Li, Q.; Xue, R.-F.; Yuan, Y.-F.; Zeng, W.-A. Lidocaine Induces Apoptosis and Suppresses Tumor Growth in Human Hepatocellular Carcinoma Cells In Vitro and in a Xenograft Model In Vivo. Anesthesiology 2017, 126, 868–881. [Google Scholar] [CrossRef]
- Yang, X.; Zhao, L.; Li, M.; Yan, L.; Zhang, S.; Mi, Z.; Ren, L.; Xu, J. Lidocaine enhances the effects of chemotherapeutic drugs against bladder cancer. Sci. Rep. 2018, 8, 598. [Google Scholar] [CrossRef] [Green Version]
- Grandhi, R.K.; Perona, B. Mechanisms of Action by Which Local Anesthetics Reduce Cancer Recurrence: A Systematic Review. Pain Med. 2020, 21, 401–414. [Google Scholar] [CrossRef]
- Euasobhon, P.; Dej-Arkom, S.; Siriussawakul, A.; Muangman, S.; Sriraj, W.; Pattanittum, P.; Lumbiganon, P. Lidocaine for reducing propofol-induced pain on induction of anaesthesia in adults. Cochrane Database Syst. Rev. 2016, 2, CD007874. [Google Scholar] [CrossRef] [Green Version]
- E Silva, L.O.J.; Scherber, K.; Cabrera, D.; Motov, S.; Erwin, P.J.; West, C.P.; Murad, M.H.; Bellolio, M.F. Safety and efficacy of intravenous lidocaine for pain management in the emergency department: A systematic review. Ann. Emerg. Med. 2018, 72, 135–144. [Google Scholar] [CrossRef]
- Mooney, J.J.; Pagel, P.S.; Kundu, M.A. Safety, Tolerability, and Short-Term Efficacy of Intravenous Lidocaine Infusions for the Treatment of Chronic Pain in Adolescents and Young Adults: A Preliminary Report. Pain Med. 2014, 15, 820–825. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, A.J.R.; Gitman, M.; Bornstein, K.J.; El-Boghdadly, K.; Weinberg, G. Updates in our understanding of local anaesthetic systemic toxicity: A narrative review. Anaesthesia 2021, 76, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Dale, G.J.; Phillips, S.; Falk, G.L. The analgesic efficacy of intravenous lidocaine infusion after laparoscopic fundoplication: A prospective, randomized, double-blind, placebo-controlled trial. Local Reg. Anesth. 2016, 9, 87–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Illingworth, J.; Lambert, C.; Malik, J.W. Adult Intravenous Lidocaine (Lignocaine) Infusion for Perioperative Analgesia in Critical Care and Recovery. Available online: https://smh-gas.org.uk/wp-content/uploads/2021/03/Standard-operating-procedure-for-the-use-of-Adult-Intravenous-Lidocaine-Lignocaine-infusion-for-Perioperative-Analgesia-in-critical-care-and-recovery.docx.pdf (accessed on 7 June 2022).
- Shanthanna, H.; Weinberg, G. Intravenous lidocaine, regional blockade, or both: Considerations for multiple interventions involving local anaesthetics. Br. J. Anaesth. 2021, 127, 497–501. [Google Scholar] [CrossRef]
- Bailey, M.A.; Toner, A.J.; Corcoran, T.B. A survey of perioperative intravenous lidocaine use by anaesthetists in Australia and New Zealand. Anaesth. Intensiv. Care 2020, 48, 53e8. [Google Scholar] [CrossRef] [PubMed]
- Meaney, E.D.; Reid, L.; Srivastava, D. A survey on the use of intravenous lidocaine infusion for acute pain in Scottish Hospitals. Br. J. Pain 2020, 14, 98e103. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, A.; Dunn, L. Clinical Implications of IV Lidocaine Infusion in Preoperative/Acute Pain Settings. Available online: https://www.asra.com/guidelines-articles/original-articles/regional-anesthesia/regional-anesthesia/asra-news/2018/07/24/clinical-implications-of-iv-lidocaine-infusion-in-preoperative-acute-pain-settings (accessed on 13 June 2022).
- Pandit, J.J.; McGuire, N. Unlicensed intravenous lidocaine for postoperative pain: Always a safer ‘licence to stop’ than to start. Anaesthesia 2021, 76, 156–160. [Google Scholar] [CrossRef]
- Weibel, S.; Jokinen, J.; Pace, N.; Schnabel, A.; Hollmann, M.; Hahnenkamp, K.; Eberhart, L.; Poepping, D.; Afshari, A.; Kranke, P. Efficacy and safety of intravenous lidocaine for postoperative analgesia and recovery after surgery: A systematic review with trial sequential analysis. Br. J. Anaesth. 2016, 116, 770–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.W.-S.; Schraag, S. The Use of Intravenous Lidocaine in Perioperative Medicine: Anaesthetic, Analgesic and Immune-Modulatory Aspects. J. Clin. Med. 2022, 11, 3543. https://doi.org/10.3390/jcm11123543
Lee IW-S, Schraag S. The Use of Intravenous Lidocaine in Perioperative Medicine: Anaesthetic, Analgesic and Immune-Modulatory Aspects. Journal of Clinical Medicine. 2022; 11(12):3543. https://doi.org/10.3390/jcm11123543
Chicago/Turabian StyleLee, Ingrid Wing-Sum, and Stefan Schraag. 2022. "The Use of Intravenous Lidocaine in Perioperative Medicine: Anaesthetic, Analgesic and Immune-Modulatory Aspects" Journal of Clinical Medicine 11, no. 12: 3543. https://doi.org/10.3390/jcm11123543