
Serum Nardilysin as a Prognostic Biomarker in Pancreatic Ductal Adenocarcinoma

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Samples
2.2. Cell Lines
2.3. Measurement of Serum NRDC Levels
2.4. RNA Extraction and Quantitative Real-Time PCR (qRT-PCR)
2.5. Immunohistochemistry
2.6. Statistical Analysis
2.7. Gene Set Enrichment Analysis
2.8. Gene Ontology (GO), Kyoto Encyclopedia of Genes and Genomes (KEGG) Analysis, Heatmap, and Volcano Plots
2.9. Pan-Cancer Analysis
3. Results
3.1. Participants’ Characteristics
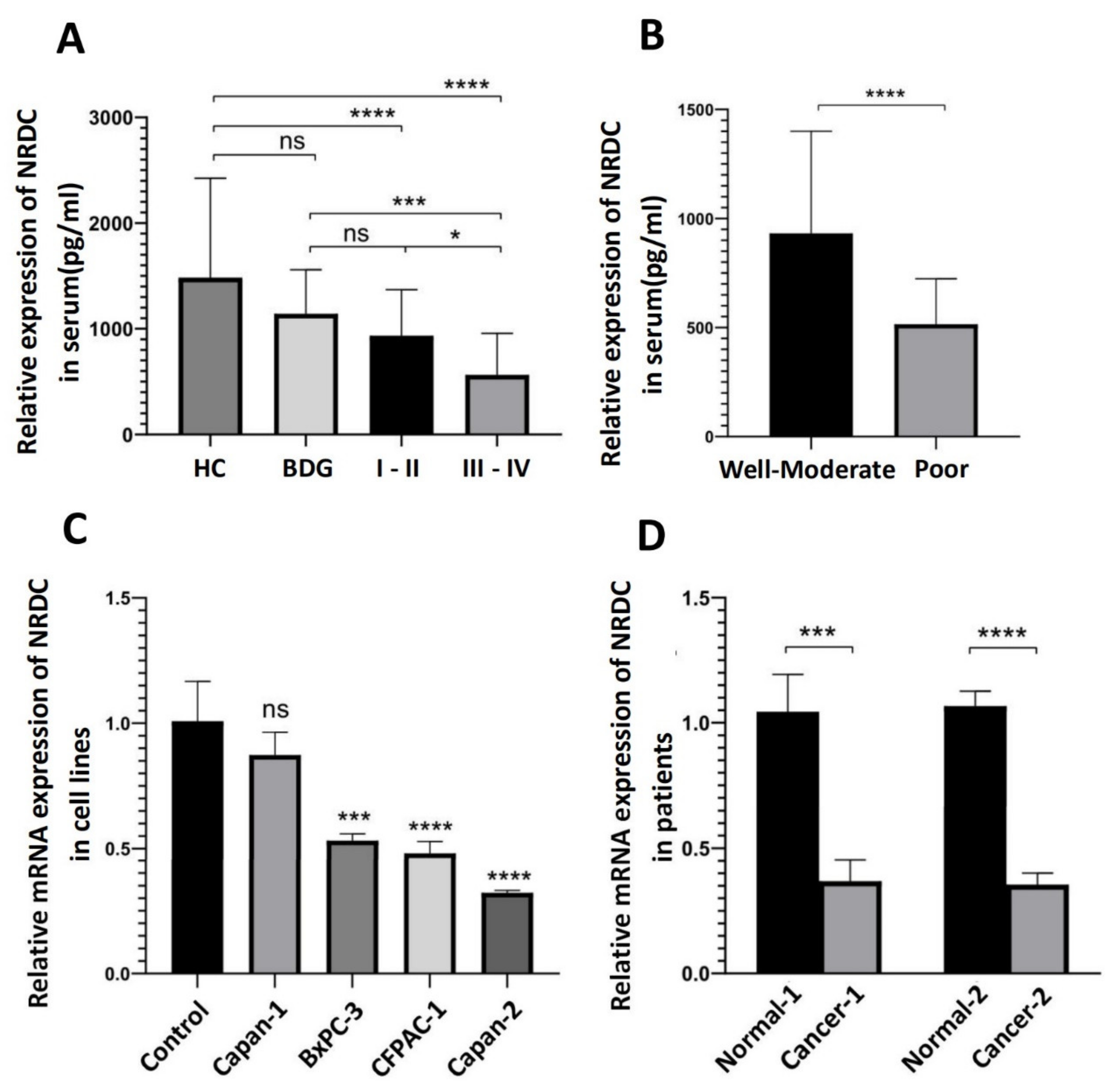
3.2. The Relative Level of NRDC Expression in Serum, Cell Lines or Pancreatic Ductal Adenocarcinoma Tissues
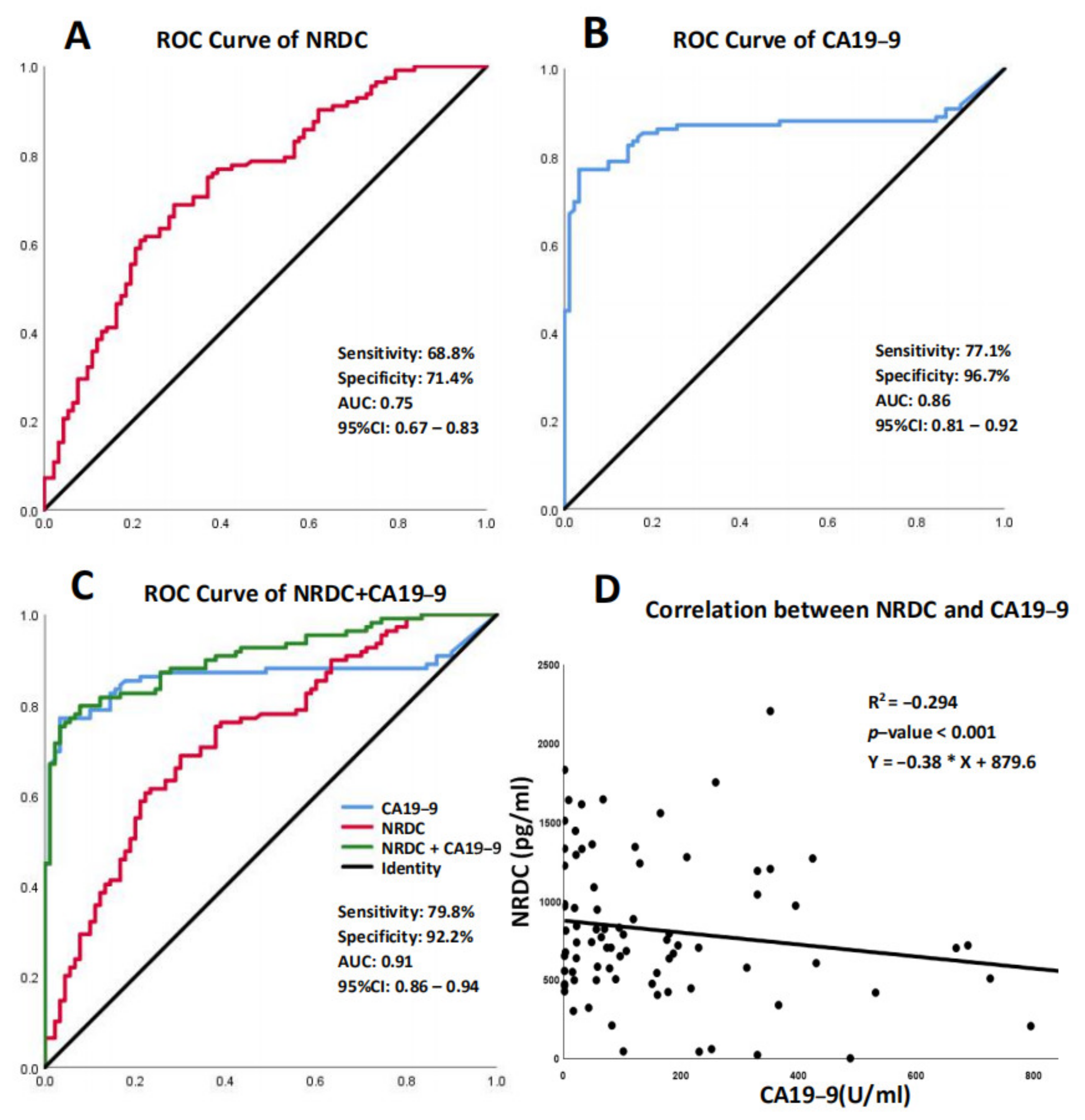
3.3. Diagnostic Value of Serum NRDC and CA19-9
3.4. Immunohistochemistry (IHC) Staining of NRDC and Hematoxylin-Eosin (H&E) Staining in Human Pancreatic Ductal Adenocarcinoma Tissues
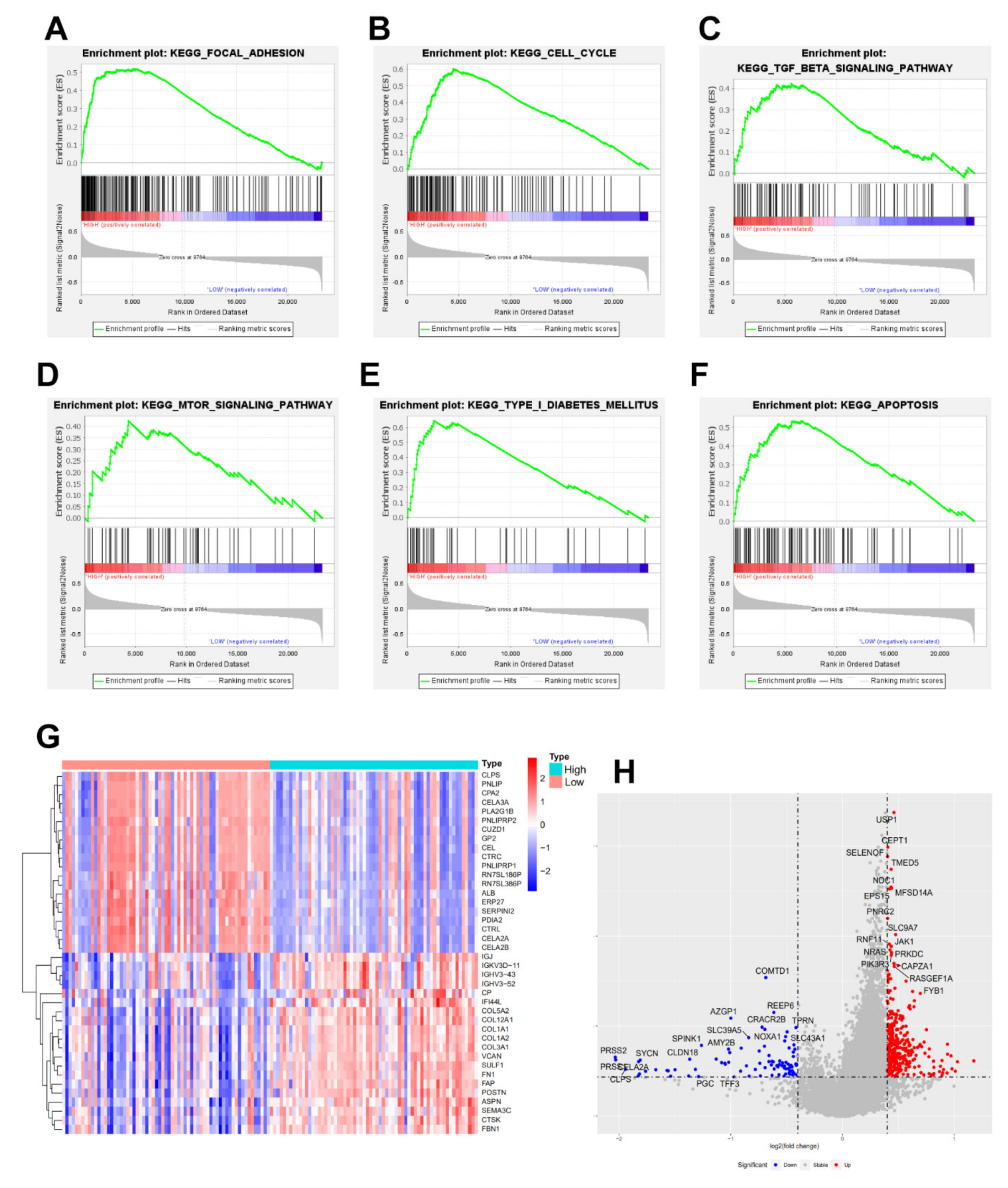
3.5. Gene Set Enrichment Analysis (GSEA), Heatmap and Volcano Plot
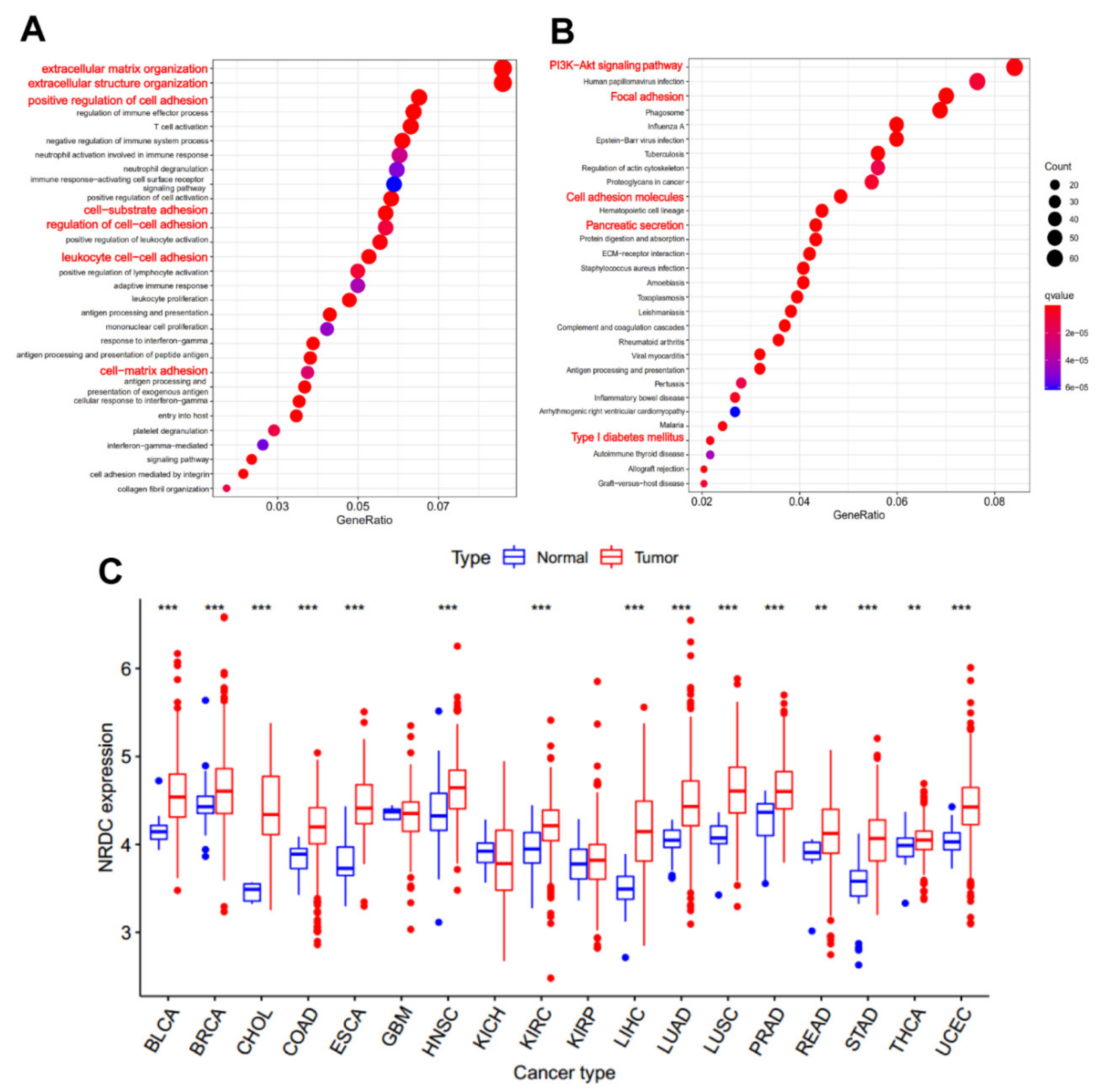
3.6. Gene Ontology (GO) Analysis, Kyoto Encyclopedia of Genes and Genomes (KEGG) Analysis, and Pan-Cancer Analysis of NRDC
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic cancer. Lancet 2020, 395, 2008–2020. [Google Scholar] [CrossRef]
- Peng, J.; Sun, B.F.; Chen, C.Y.; Zhou, J.Y.; Chen, Y.S.; Chen, H.; Liu, L.; Huang, D.; Jiang, J.; Cui, G.S.; et al. Single-cell RNA-seq highlights intra-tumoral heterogeneity and malignant progression in pancreatic ductal adenocarcinoma. Cell Res. 2019, 29, 725–738. [Google Scholar] [CrossRef]
- Yadav, D.; Lowenfels, A.B. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 2013, 144, 1252–1261. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Arnold, M.; Rutherford, M.J.; Bardot, A.; Ferlay, J.; Andersson, T.M.; Myklebust, T.A.; Tervonen, H.; Thursfield, V.; Ransom, D.; Shack, L.; et al. Progress in cancer survival, mortality, and incidence in seven high-income countries 1995–2014 (ICBP SURVMARK-2): A population-based study. Lancet Oncol. 2019, 20, 1493–1505. [Google Scholar] [CrossRef] [Green Version]
- Singhi, A.D.; Koay, E.J.; Chari, S.T.; Maitra, A. Early Detection of Pancreatic Cancer: Opportunities and Challenges. Gastroenterology 2019, 156, 2024–2040. [Google Scholar] [CrossRef] [Green Version]
- Strobel, O.; Neoptolemos, J.; Jager, D.; Buchler, M.W. Optimizing the outcomes of pancreatic cancer surgery. Nat. Rev. Clin. Oncol. 2019, 16, 11–26. [Google Scholar] [CrossRef]
- Zheng, X.; Carstens, J.L.; Kim, J.; Scheible, M.; Kaye, J.; Sugimoto, H.; Wu, C.C.; LeBleu, V.S.; Kalluri, R. Epithelial-to-mesenchymal transition is dispensable for metastasis but induces chemoresistance in pancreatic cancer. Nature 2015, 527, 525–530. [Google Scholar] [CrossRef] [Green Version]
- Ferlay, J.; Partensky, C.; Bray, F. More deaths from pancreatic cancer than breast cancer in the EU by 2017. Acta Oncol. 2016, 55, 1158–1160. [Google Scholar] [CrossRef]
- Chesneau, V.; Pierotti, A.R.; Barré, N.; Créminon, C.; Tougard, C.; Cohen, P. Isolation and characterization of a dibasic selective metalloendopeptidase from rat testes that cleaves at the amino terminus of arginine residues. J. Biol. Chem. 1994, 269, 2056–2061. [Google Scholar] [CrossRef]
- Yoh, T.; Hatano, E.; Kasai, Y.; Fuji, H.; Nishi, K.; Toriguchi, K.; Sueoka, H.; Ohno, M.; Seo, S.; Iwaisako, K.; et al. Serum Nardilysin, a Surrogate Marker for Epithelial-Mesenchymal Transition, Predicts Prognosis of Intrahepatic Cholangiocarcinoma after Surgical Resection. Clin. Cancer Res. 2019, 25, 619–628. [Google Scholar] [CrossRef] [Green Version]
- Chen, F.-H.; Wang, Y.; Jiang, Y.-X.; Zhang, G.-H.; Wang, Z.-M.; Yang, H. Clinical determination of serum nardilysin levels in predicting 30-day mortality among adults with malignant cerebral infarction. Clin. Chim. Acta 2019, 494, 8–13. [Google Scholar] [CrossRef]
- Uraoka, N.; Oue, N.; Sakamoto, N.; Sentani, K.; Oo, H.Z.; Naito, Y.; Noguchi, T.; Yasui, W. NRD1, which encodes nardilysin protein, promotes esophageal cancer cell invasion through induction of MMP2 and MMP3 expression. Cancer Sci. 2014, 105, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Kanda, K.; Komekado, H.; Sawabu, T.; Ishizu, S.; Nakanishi, Y.; Nakatsuji, M.; Akitake-Kawano, R.; Ohno, M.; Hiraoka, Y.; Kawada, M.; et al. Nardilysin and ADAM proteases promote gastric cancer cell growth by activating intrinsic cytokine signalling via enhanced ectodomain shedding of TNF-a. Embo Mol. Med. 2012, 4, 396–411. [Google Scholar] [CrossRef]
- Morita, Y.; Ohno, M.; Nishi, K.; Hiraoka, Y.; Saijo, S.; Matsuda, S.; Kita, T.; Kimura, T.; Nishi, E. Genome-wide profiling of nardilysin target genes reveals its role in epigenetic regulation and cell cycle progression. Sci. Rep. 2017, 7, 14801. [Google Scholar] [CrossRef] [Green Version]
- Yoon, W.H.; Sandoval, H.; Nagarkar-Jaiswal, S.; Jaiswal, M.; Yamamoto, S.; Haelterman, N.A.; Putluri, N.; Putluri, V.; Sreekumar, A.; Tos, T.; et al. Loss of Nardilysin, a Mitochondrial Co-chaperone for alpha-Ketoglutarate Dehydrogenase, Promotes mTORC1 Activation and Neurodegeneration. Neuron 2017, 93, 115–131. [Google Scholar] [CrossRef] [Green Version]
- Hospital, V.; Prat, A. Nardilysin, a basic residues specific metallopeptidase that mediates cell migration and proliferation. Protein Pept. Lett. 2004, 11, 501–508. [Google Scholar] [CrossRef]
- Nishi, K.; Sato, Y.; Ohno, M.; Hiraoka, Y.; Saijo, S.; Sakamoto, J.; Chen, P.-M.; Morita, Y.; Matsuda, S.; Iwasaki, K.; et al. Nardilysin Is Required for Maintaining Pancreatic beta-Cell Function. Diabetes 2016, 65, 3015–3027. [Google Scholar] [CrossRef] [Green Version]
- Ikuta, K.; Fukuda, A.; Ogawa, S.; Masuo, K.; Goto, N.; Hiramatsu, Y.; Tsuda, M.; Kimura, Y.; Matsumoto, Y.; Kimura, Y.; et al. Nardilysin inhibits pancreatitis and suppresses pancreatic ductal adenocarcinoma initiation in mice. Gut 2019, 68, 882–892. [Google Scholar] [CrossRef] [Green Version]
- Makohon-Moore, A.; Iacobuzio-Donahue, C.A. Pancreatic cancer biology and genetics from an evolutionary perspective. Nat. Rev. Cancer 2016, 16, 553–565. [Google Scholar] [CrossRef] [Green Version]
- Kleeff, J.; Korc, M.; Apte, M.; la Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic cancer. Nature reviews. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Kleeff, J.; Michl, P.; Costello, E.; Greenhalf, W.; Palmer, D.H. Therapeutic developments in pancreatic cancer: Current and future perspectives. Nature reviews. Gastroenterol. Hepatol. 2018, 15, 333–348. [Google Scholar]
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Riquelme, E.; Zhang, Y.; Zhang, L.; Montiel, M.; Zoltan, M.; Dong, W.; Quesada, P.; Sahin, I.; Chandra, V.; Lucas, A.S.; et al. Tumor Microbiome Diversity and Composition Influence Pancreatic Cancer Outcomes. Cell 2019, 178, 795–806.e12. [Google Scholar] [CrossRef]
- Hosein, A.N.; Brekken, R.A.; Maitra, A. Pancreatic cancer stroma: An update on therapeutic targeting strategies. Nature reviews. Gastroenterol. Hepatol. 2020, 17, 487–505. [Google Scholar]
- Yang, J.; Xu, R.; Wang, C.; Qiu, J.; Ren, B.; You, L. Early screening and diagnosis strategies of pancreatic cancer: A comprehensive review. Cancer Commun. 2021, 41, 1257–1274. [Google Scholar] [CrossRef]
- Huang, Z.; Li, Z.; Jiang, M.; Liu, R.; Lv, Y. Homogeneous Multiplex Immunoassay for One-Step Pancreatic Cancer Biomarker Evaluation. Anal. Chem. 2020, 92, 16105–16112. [Google Scholar] [CrossRef]
- Singh, S.; Tang, S.J.; Sreenarasimhaiah, J.; Lara, L.F.; Siddiqui, A. The clinical utility and limitations of serum carbohydrate antigen (CA19-9) as a diagnostic tool for pancreatic cancer and cholangiocarcinoma. Dig. Dis. Sci. 2011, 56, 2491–2496. [Google Scholar] [CrossRef]
- Fujimoto, Y.; Suehiro, Y.; Kaino, S.; Suenaga, S.; Tsuyama, T.; Matsui, H.; Higaki, S.; Fujii, I.; Suzuki, C.; Hoshida, T.; et al. Combination of CA19-9 and Blood Free-Circulating Methylated RUNX3 May Be Useful to Diagnose Stage I Pancreatic Cancer. Oncology 2021, 99, 234–239. [Google Scholar] [CrossRef]
- Ishizu-Higashi, S.; Seno, H.; Nishi, E.; Matsumoto, Y.; Ikuta, K.; Tsuda, M.; Kimura, Y.; Takada, Y.; Kimura, Y.; Nakanishi, Y.; et al. Deletion of Nardilysin Prevents the Development of Steatohepatitis and Liver Fibrotic Changes. PLoS ONE 2014, 9, e98017. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, Y.; Matsuoka, T.; Ohno, M.; Nakamura, K.; Saijo, S.; Matsumura, S.; Nishi, K.; Sakamoto, J.; Chen, P.-M.; Inoue, K.; et al. Critical roles of nardilysin in the maintenance of body temperature homoeostasis. Nat. Commun. 2014, 5, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Z.L.; Chow, K.M.; Yao, J.; Hersh, L.B. Nuclear shuttling of the peptidase nardilysin. Arch. Biochem. Biophys. 2004, 422, 153–160. [Google Scholar] [CrossRef]
- Agemy, L.; Kotamraju, V.R.; Friedmann-Morvinski, D.; Sharma, S.; Sugahara, K.N.; Ruoslahti, E. Proapoptotic peptide-mediated cancer therapy targeted to cell surface p32. Mol. Ther. 2013, 21, 2195–2204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Wang, L.; Zhan, Y.; Zeng, T.; Zhang, X.; Guan, X.Y.; Li, Y. Membrane Metalloendopeptidase (MME) Suppresses Metastasis of Esophageal Squamous Cell Carcinoma (ESCC) by Inhibiting FAK-RhoA Signaling Axis. Am. J. Pathol. 2019, 189, 1462–1472. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Miyake, M.; Lawton, A.; Goodison, S.; Rosser, C.J. Matrix metalloproteinase-10 promotes tumor progression through regulation of angiogenic and apoptotic pathways in cervical tumors. BMC Cancer 2014, 14, 310. [Google Scholar] [CrossRef] [Green Version]
- Gu, G.; Xia, H.; Hu, Q.; Liu, Z.; Jiang, M.; Kang, T.; Miao, D.; Tu, Y.; Pang, Z.; Song, Q.; et al. PEG-co-PCL nanoparticles modified with MMP-2/9 activatable low molecular weight protamine for enhanced targeted glioblastoma therapy. Biomaterials 2013, 34, 196–208. [Google Scholar] [CrossRef]
- Solimando, A.G.; Summa, S.; Vacca, A.; Ribatti, D. Cancer-Associated Angiogenesis: The Endothelial Cell as a Checkpoint for Immunological Patrolling. Cancers 2020, 12, 3380. [Google Scholar] [CrossRef]
- Xing, H.; Wang, J.; Wang, Y.; Tong, M.; Hu, H.; Huang, C.; Li, D. Diagnostic Value of CA 19-9 and Carcinoembryonic Antigen for Pancreatic Cancer: A Meta-Analysis. Gastroenterol Res. Pract. 2018, 2018, 8704751. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number | NRDC | χ2 | p-Value | |
|---|---|---|---|---|---|
| Low | High | ||||
| Age (years) | 0.913 | NS | |||
| <60 | 47 (42) | 30 (64) | 17 (36) | ||
| ≥60 | 65 (58) | 47 (72) | 18 (28) | ||
| Gender | 2.662 | NS | |||
| Male | 73 (57) | 54 (57) | 19 (43) | ||
| Female | 39 (43) | 23 (43) | 16 (57) | ||
| Smoke | 0.018 | NS | |||
| Yes | 67 (60) | 47 (70) | 20 (30) | ||
| No | 35 (40) | 25 (71) | 10 (29) | ||
| Drink | 0.492 | NS | |||
| Yes | 77 (75) | 55 (71) | 22 (29) | ||
| No | 25 (25) | 16 (64) | 9 (36) | ||
| Metastasis | 30.915 | <0.001 | |||
| Yes | 26 (25) | 23 (88) | 3 (12) | ||
| No | 76 (75) | 47 (62) | 29 (38) | ||
| Differentiation | 28.221 | <0.001 | |||
| Well-Moderate | 57 (51) | 32 (56) | 25 (44) | ||
| Poor Missing | 24 (21) | 23 (96) | 1 (4) | ||
| 31 (28) | |||||
| T stage | 26.958 | <0.001 | |||
| T1 | 4 (4) | 2 (50) | 2 (50) | ||
| T2 | 45 (40) | 30 (67) | 15 (33) | ||
| T3 | 1312) | 8 (62) | 5 (38) | ||
| T4 Missing | 40 (36) | 10 (25) | 30 (75) | ||
| 10 (8) | |||||
| TNM stage | 6.4 | =0.011 | |||
| I/II | 63 (56) | 37 (65) | 26 (35) | ||
| III/IV Missing | 48 (43) | 39 (81) | 9 (19) | ||
| 1 (1) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, Y.; Xiong, Q.; Yang, Y.; Weng, N.; Li, J.; Liu, J.; Yang, X.; Zeng, Z.; Zhang, Z.; Zhu, Q. Serum Nardilysin as a Prognostic Biomarker in Pancreatic Ductal Adenocarcinoma. J. Clin. Med. 2022, 11, 3101. https://doi.org/10.3390/jcm11113101
Xu Y, Xiong Q, Yang Y, Weng N, Li J, Liu J, Yang X, Zeng Z, Zhang Z, Zhu Q. Serum Nardilysin as a Prognostic Biomarker in Pancreatic Ductal Adenocarcinoma. Journal of Clinical Medicine. 2022; 11(11):3101. https://doi.org/10.3390/jcm11113101
Chicago/Turabian StyleXu, Yongfeng, Qunli Xiong, Yang Yang, Ningna Weng, Junjun Li, Jinlu Liu, Xiaojuan Yang, Zhu Zeng, Zhiwei Zhang, and Qing Zhu. 2022. "Serum Nardilysin as a Prognostic Biomarker in Pancreatic Ductal Adenocarcinoma" Journal of Clinical Medicine 11, no. 11: 3101. https://doi.org/10.3390/jcm11113101