
Structural Integrity and Functional Neural Activity Associated with Oral Language Function after Stroke


Abstract
:1. Introduction
2. Materials and Methods
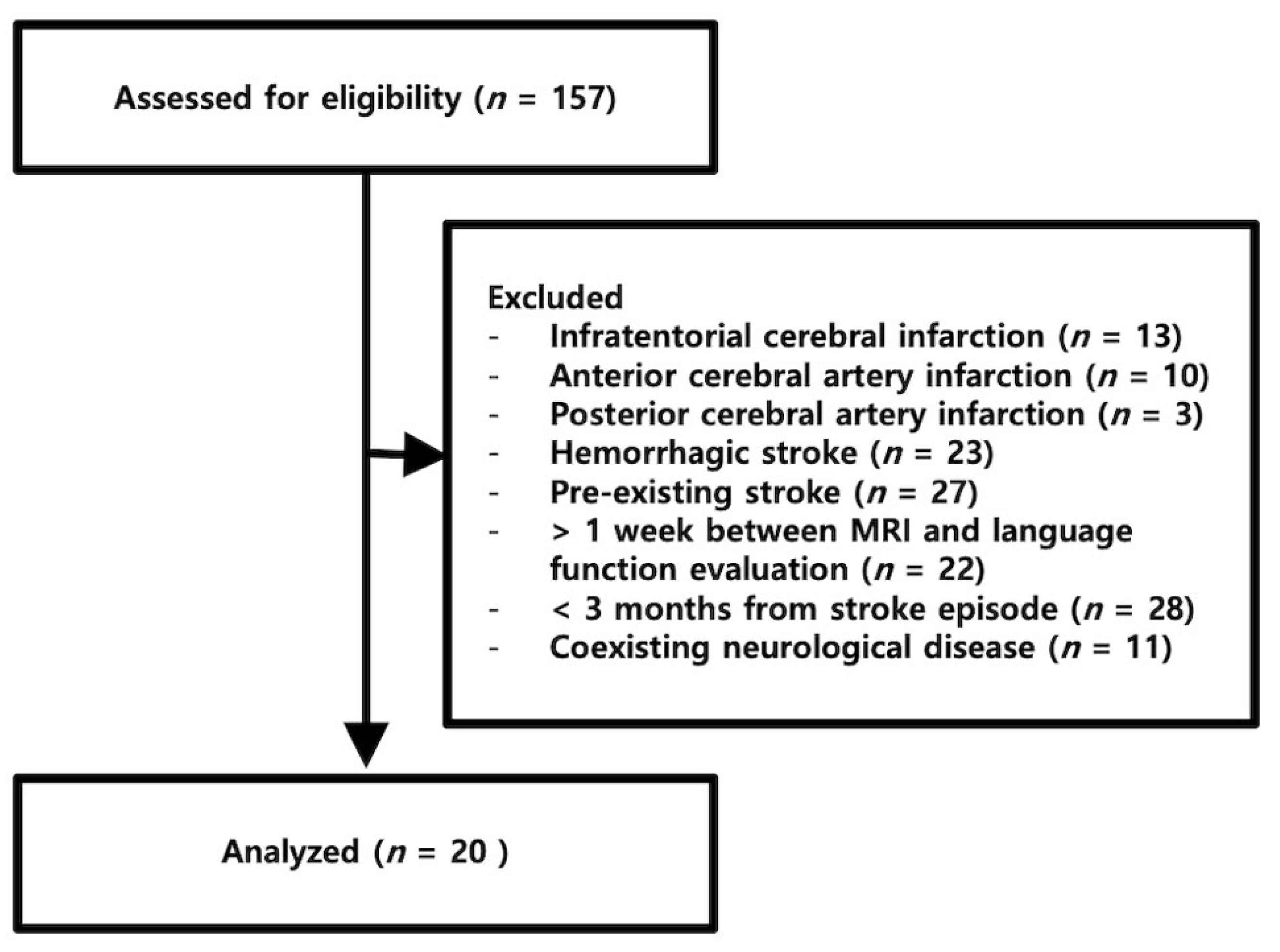
2.1. Patients
2.2. Language Evaluation
2.3. MRI Preprocessing
2.4. Statistical Analysis
3. Results
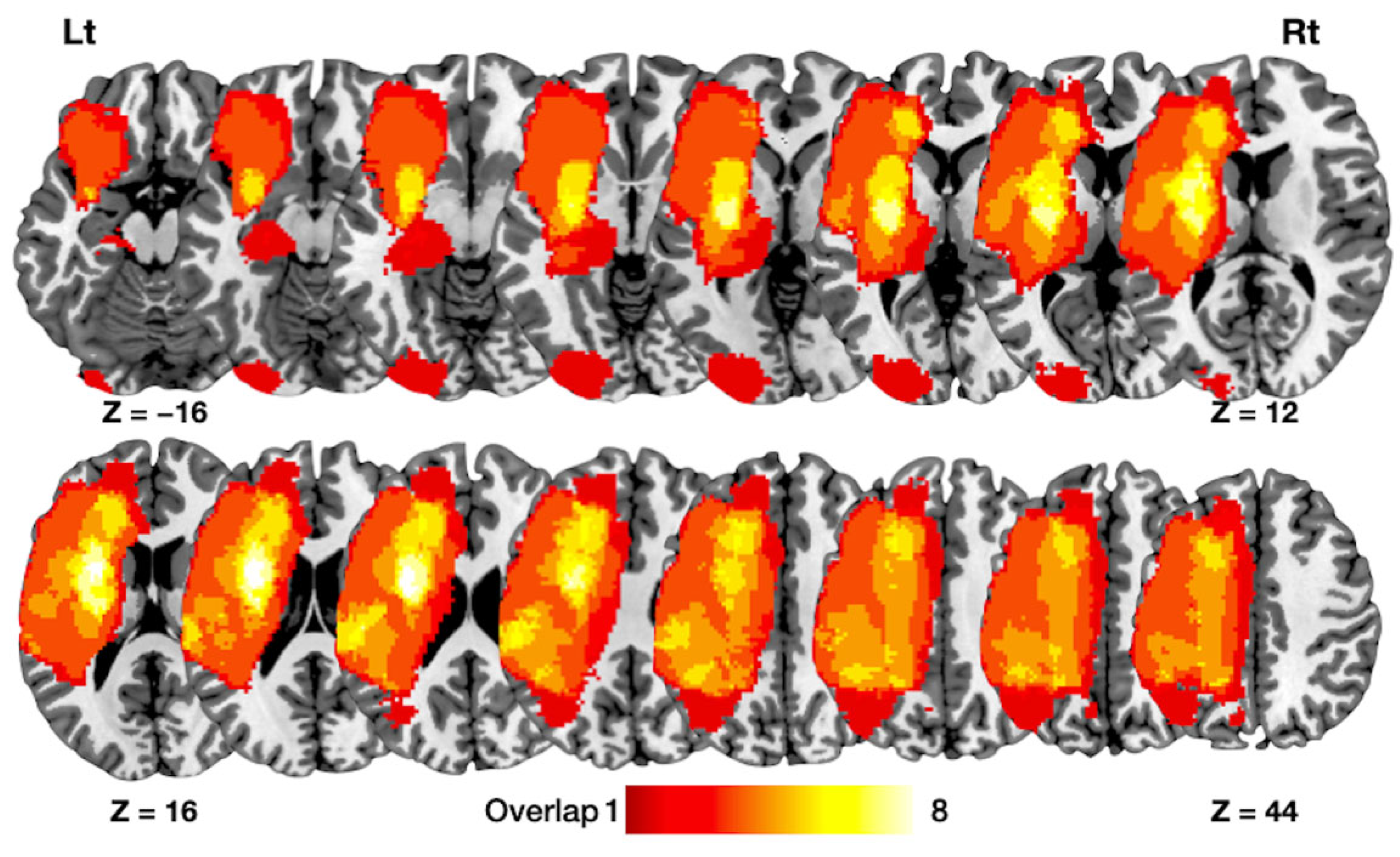
3.1. Patient Characteristics
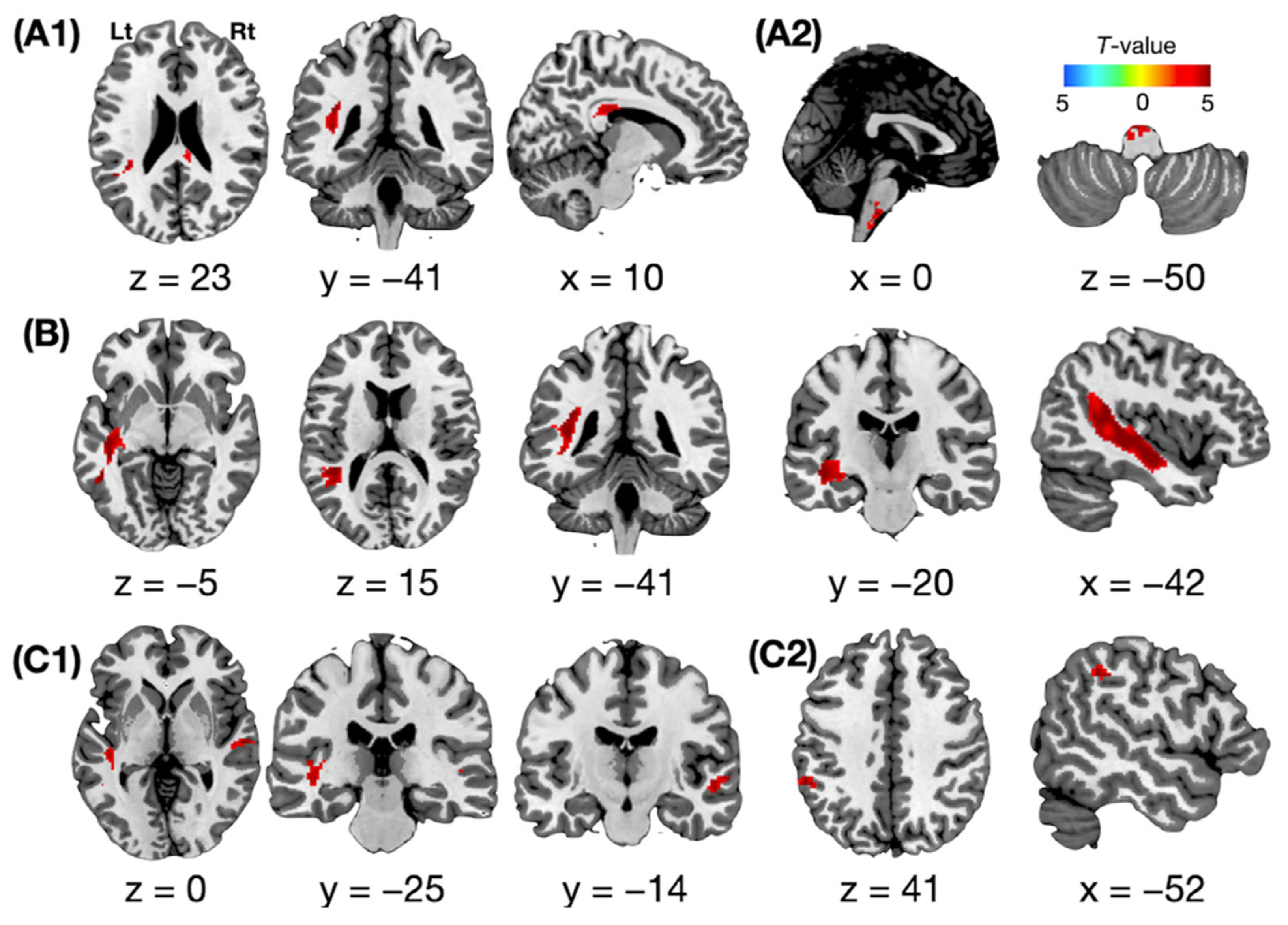
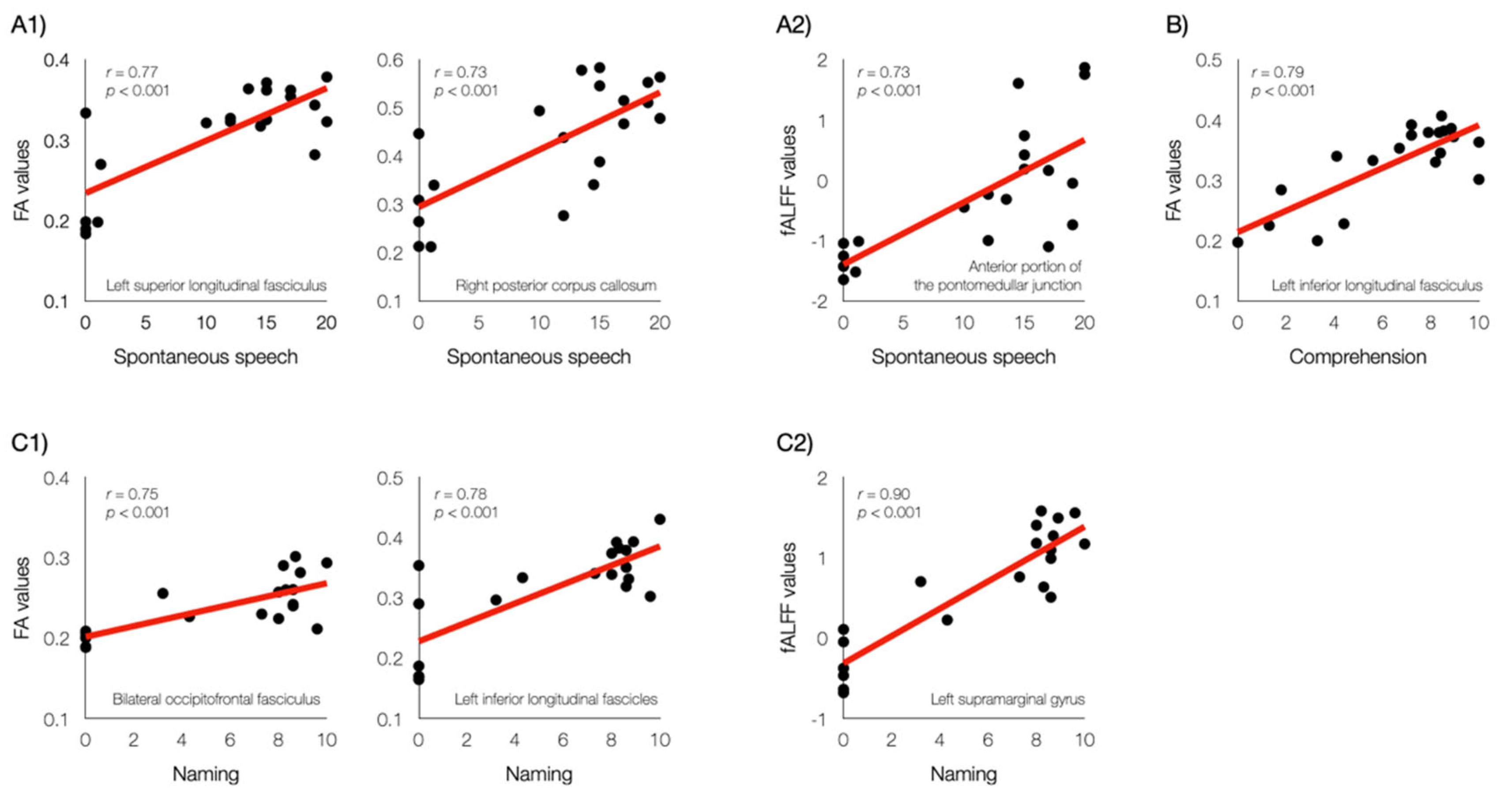
3.2. Structural Atrophy Associated with Language Function
3.3. Functional Neural Activity Associated with Language Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Watila, M.M.; Balarabe, S.A. Factors predicting post-stroke aphasia recovery. J. Neurol. Sci. 2015, 352, 12–18. [Google Scholar] [PubMed]
- Lwi, S.J.; Herron, T.J.; Curran, B.C.; Ivanova, M.V.; Schendel, K.; Dronkers, N.F.; Baldo, J.V. Auditory comprehension deficits in post-stroke aphasia: Neurologic and demographic correlates of outcome and recovery. Front Neurol. 2021, 12, 680248. [Google Scholar] [CrossRef] [PubMed]
- Flowers, H.L.; Skoretz, S.A.; Silver, F.L.; Rochon, E.; Fang, J.; Flamand-Roze, C.; Martino, R. Poststroke aphasia frequency, recovery, and outcomes: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2016, 97, 2188–2201.e2188. [Google Scholar] [CrossRef]
- Zhang, J.; Zhong, S.; Zhou, L.; Yu, Y.; Tan, X.; Wu, M.; Sun, P.; Zhang, W.; Li, J.; Cheng, R.; et al. Correlations between dual-pathway white matter alterations and language impairment in patients with aphasia: A systematic review and meta-analysis. Neuropsychol. Rev. 2021, 31, 402–418. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Chen, L.; Zheng, S.; Wang, H.; Dai, Y.; Chen, Z.; Huang, R. Disrupted brain connectivity networks in aphasia revealed by resting-state fmri. Front Aging Neurosci. 2021, 13, 666301. [Google Scholar]
- Kyeong, S.; Kang, H.; Kyeong, S.; Kim, D.H. Differences in brain areas affecting language function after stroke. Stroke 2019, 50, 2956–2959. [Google Scholar] [CrossRef]
- Saur, D.; Kreher, B.W.; Schnell, S.; Kummerer, D.; Kellmeyer, P.; Vry, M.S.; Umarova, R.; Musso, M.; Glauche, V.; Abel, S.; et al. Ventral and dorsal pathways for language. Proc. Natl. Acad. Sci. USA 2008, 105, 18035–18040. [Google Scholar] [CrossRef] [Green Version]
- Hickok, G.; Poeppel, D. Dorsal and ventral streams: A framework for understanding aspects of the functional anatomy of language. Cognition 2004, 92, 67–99. [Google Scholar] [CrossRef]
- Chang, E.F.; Raygor, K.P.; Berger, M.S. Contemporary model of language organization: An overview for neurosurgeons. J. Neurosurg. Feb. 2015, 122, 250–261. [Google Scholar] [CrossRef]
- Fridriksson, J.; Ouden, D.-B.D.; Hillis, A.E.; Hickok, G.; Rorden, C.; Basilakos, A.; Yourganov, G.; Bonilha, L. Anatomy of aphasia revisited. Brain 2018, 141, 848–862. [Google Scholar] [CrossRef]
- Saur, D.; Lange, R.; Baumgaertner, A.; Schraknepper, V.; Willmes, K.; Rijntjes, M.; Weiller, C. Dynamics of language reorganization after stroke. Brain 2006, 129, 1371–1384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stockert, A.; Wawrzyniak, M.; Klingbeil, J.; Wrede, K.; Kümmerer, D.; Hartwigsen, G.; Kaller, C.P.; Weiller, C.; Saur, D. Dynamics of language reorganization after left temporo-parietal and frontal stroke. Brain 2020, 143, 844–861. [Google Scholar] [CrossRef] [PubMed]
- Fridriksson, J.; Richardson, J.D.; Fillmore, P.; Cai, B. Left hemisphere plasticity and aphasia recovery. NeuroImage 2012, 60, 854–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffis, J.C.; Nenert, R.; Allendorfer, J.B.; Vannest, J.; Holland, S.; Dietz, A.; Szaflarski, J.P. The canonical semantic network supports residual language function in chronic post-stroke aphasia. Hum. Brain Mapp. 2017, 38, 1636–1658. [Google Scholar] [CrossRef] [Green Version]
- Thiel, A.; Hartmann, A.; Rubi-Fessen, I.; Anglade, C.; Kracht, L.; Weiduschat, N.; Kessler, J.; Rommel, T.; Heiss, W.D. Effects of noninvasive brain stimulation on language networks and recovery in early poststroke aphasia. Stroke 2013, 44, 2240–2246. [Google Scholar] [CrossRef] [Green Version]
- Tyler, L.K.; Wright, P.; Randall, B.; Marslen-Wilson, W.D.; Stamatakis, E.A. Reorganization of syntactic processing following left-hemisphere brain damage: Does right-hemisphere activity preserve function? Brain 2010, 133, 3396–3408. [Google Scholar] [CrossRef]
- Szaflarski, J.P.; Allendorfer, J.B.; Banks, C.; Vannest, J.; Holland, S.K. Recovered vs. Not-recovered from post-stroke aphasia: The contributions from the dominant and non-dominant hemispheres. Restor. Neurol. Neurosci. 2013, 31, 347–360. [Google Scholar] [CrossRef]
- Turkeltaub, P.E.; Coslett, H.B.; Thomas, A.L.; Faseyitan, O.; Benson, J.; Norise, C.; Hamilton, R.H. The right hemisphere is not unitary in its role in aphasia recovery. Cortex 2012, 48, 1179–1186. [Google Scholar] [CrossRef] [Green Version]
- Keser, Z.; Sebastian, R.; Hasan, K.M.; Hillis, A.E. Right hemispheric homologous language pathways negatively predicts poststroke naming recovery. Stroke 2020, 51, 1002–1005. [Google Scholar] [CrossRef]
- Schlaug, G.; Marchina, S.; Norton, A. Evidence for plasticity in white-matter tracts of patients with chronic broca’s aphasia undergoing intense intonation-based speech therapy. Ann. N. Y. Acad. Sci. 2009, 1169, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Na, D.L. Normative data on the korean version of the western aphasia battery. J. Clin. Exp. Neuropsychol. 2004, 26, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3d slicer as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, Q.-H.; Zhu, C.-Z.; Yang, Y.; Zuo, X.-N.; Long, X.-Y.; Cao, Q.-J.; Wang, Y.-F. An improved approach to detection of amplitude of low-frequency fluctuation (alff) for resting-state fmri: Fractional alff. J. Neurosci. Methods 2008, 172, 137–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flandin, G.; Friston, K.J. Analysis of family-wise error rates in statistical parametric mapping using random field theory. Hum. Brain Mapp. 2017, 40, 2052–2054. [Google Scholar] [CrossRef] [PubMed]
- Assaf, Y.; Pasternak, O. Diffusion tensor imaging (dti)-based white matter mapping in brain research: A review. J. Mol. Neurosci. 2008, 34, 51–61. [Google Scholar] [CrossRef]
- Klingbeil, J.; Wawrzyniak, M.; Stockert, A.; Saur, D. Resting-state functional connectivity: An emerging method for the study of language networks in post-stroke aphasia. Brain Cogn. 2019, 131, 22–33. [Google Scholar] [CrossRef]
- Zhao, Y.; Lambon Ralph, M.A.; Halai, A.D. Relating resting-state hemodynamic changes to the variable language profiles in post-stroke aphasia. Neuroimage Clin. 2018, 20, 611–619. [Google Scholar] [CrossRef]
- Sandberg, C.W. Hypoconnectivity of resting-state networks in persons with aphasia compared with healthy age-matched adults. Front. Hum. Neurosci. 2017, 11, 91. [Google Scholar] [CrossRef] [Green Version]
- Hofer, S.; Frahm, J. Topography of the human corpus callosum revisited--comprehensive fiber tractography using diffusion tensor magnetic resonance imaging. NeuroImage 2006, 32, 989–994. [Google Scholar] [CrossRef]
- Jaekl, P.; Pesquita, A.; Alsius, A.; Munhall, K.; Soto-Faraco, S. The contribution of dynamic visual cues to audiovisual speech perception. Neuropsychologia 2015, 75, 402–410. [Google Scholar] [CrossRef]
- Basirat, A.; Allart, É.; Brunellière, A.; Martin, Y. Audiovisual speech segmentation in post-stroke aphasia: A pilot study. Top Stroke Rehabil. 2019, 26, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.H. Neuroanatomy: Text and Atlas; McGraw-Hil: New York, NY, USA, 2012. [Google Scholar]
- Anglade, C.; Thiel, A.; Ansaldo, A.I. The complementary role of the cerebral hemispheres in recovery from aphasia after stroke: A critical review of literature. Brain Inj. 2014, 28, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Marcotte, K.; Adrover-Roig, D.; Damien, B.; de Préaumont, M.; Généreux, S.; Hubert, M.; Ansaldo, A.I. Therapy-induced neuroplasticity in chronic aphasia. Neuropsychologia 2012, 50, 1776–1786. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | T1-Weighed MRI | DTI | rsfMRI |
|---|---|---|---|
| Matrix | 256 × 256 | 112 × 112 | 64 × 64 |
| Field of view (mm2) | 230 × 230 | 224 × 224 | 192 × 192 |
| Repetition time (ms) | 1900 | 9700 | 2000 |
| Echo time (ms) | 2.57 | 92.00 | 30.00 |
| Slice thickness (mm) | 1 | 2 | 4.4 |
| Flip angle (°) | 9 | 9 | 9 |
| Directions | 30 | ||
| b values (s/mm2) | 1000 |
| (n = 20)/Mean ± SE/n (%) | |
|---|---|
| Demographic characteristics | |
| Age (years) | 71.9 ± 2.4 |
| Duration between stroke and performed MRI (days) | 1219.7 ± 432.6 |
| Language evaluation (K-WAB) | |
| Spontaneous speech (20) | 11.1 ± 1.7 |
| Comprehension (10) | 6.5 ± 0.7 |
| Repetition (10) | 6.0 ± 1.0 |
| Naming (10) | 5.5 ± 0.9 |
| Aphasia severity | |
| Mild | 6 (30.0%) |
| Mild to moderate | 6 (30.0%) |
| Moderate | 1 (5.0%) |
| Moderate to severe | 0 (0%) |
| Severe | 7 (35.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyeong, S.; Kang, H.; Kim, D.H. Structural Integrity and Functional Neural Activity Associated with Oral Language Function after Stroke. J. Clin. Med. 2022, 11, 3028. https://doi.org/10.3390/jcm11113028
Kyeong S, Kang H, Kim DH. Structural Integrity and Functional Neural Activity Associated with Oral Language Function after Stroke. Journal of Clinical Medicine. 2022; 11(11):3028. https://doi.org/10.3390/jcm11113028
Chicago/Turabian StyleKyeong, Sunghyon, Hyunkoo Kang, and Dae Hyun Kim. 2022. "Structural Integrity and Functional Neural Activity Associated with Oral Language Function after Stroke" Journal of Clinical Medicine 11, no. 11: 3028. https://doi.org/10.3390/jcm11113028