
Double Lateral Sliding Bridge Flap versus Laterally Closed Tunnel for the Treatment of Single Recessions in the Mandibular Anterior Teeth: A Pseudorandomized Clinical Trial

 ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Selection
2.2. Clinical Assessments
- Recession type (RT): the Miller [15] classification was used.
- Gingival recession depth (GRD), measured in millimeters as the distance from the cementoenamel junction to the gingival margin.
- Probing depth (PD), measured in millimeters from the free gingival margin to the most apical part of the gingival sulcus.
- Clinical attachment level (CAL): algebraic sum of the PD and GRD.
- Keratinized tissue width (KTW), measured in millimeters from the free gingival margin to the mucogingival junction (MGJ).
- Gingival thickness (GT), determined 2 mm apical to the new gingival margin using a K#10 endodontic file with rubber stop (transgingival probing) [17].
- The percentage of root coverage (RC) was calculated by the following formula: ([recession at baseline–recession at the final examination]/recession at baseline) × 100.
- Evaluation by an operator (N.Q.) of esthetic outcomes after root coverage using the root coverage esthetic score (RES) system, with reference to intraoral photos. The file with preoperative and postoperative images was provided, together with the data collection record for each clinical case, as per the RES instructions. Five variables were evaluated with the RES system after surgery: the level of the gingival margin, the marginal tissue contour, soft tissue texture, the position of the MGJ and gingival color [18]. The final esthetic score ranged from 0 to 10, the maximum score being 10. The score breakdown was as follows: between 0 and 6 points were allocated to the level of the gingival margin, and the marginal tissue contour, soft tissue texture, mucogingival junction and gingival color parameters received either 0 or 1 point each.
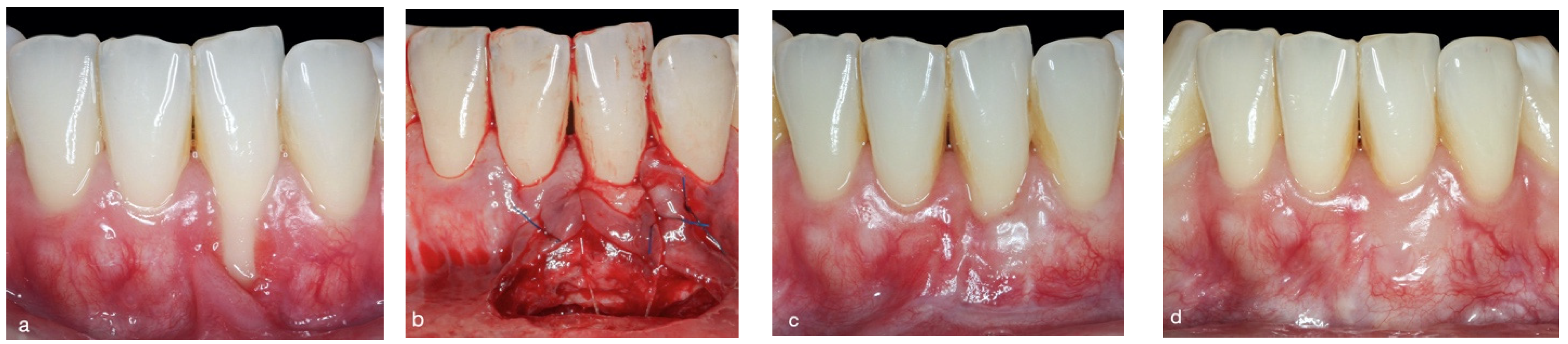
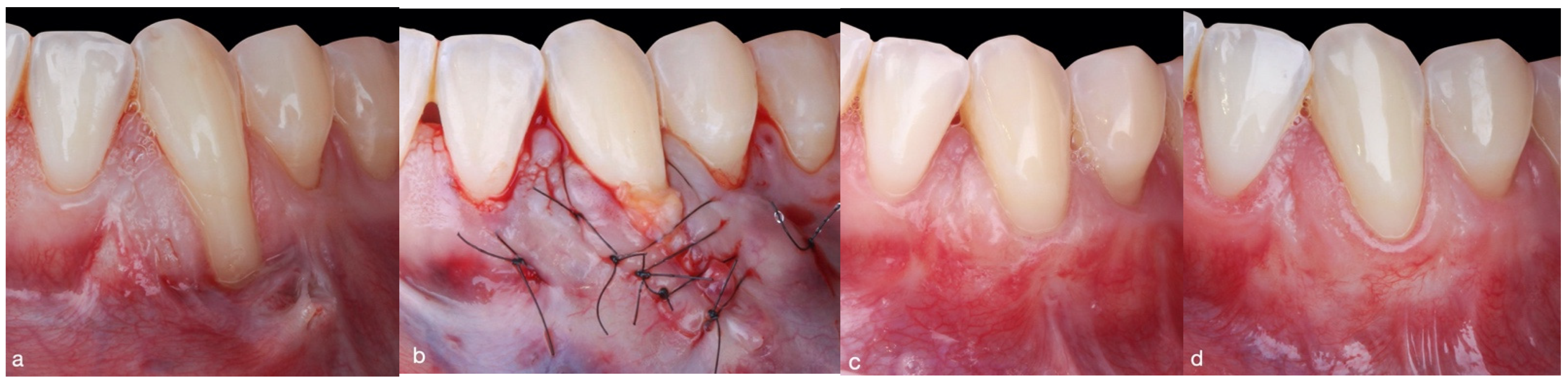
2.3. Surgical Approach
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DLSBF | Double lateral sliding bridge flap |
| LCT | Laterally closed tunnel |
| SCTG | Subepithelial connective tissue graft |
| GRD | Gingival recession depth |
| PD | Probing depth |
| CAL | Clinical attachment level |
| KTW | Keratinized tissue width |
| GT | Gingival thickness |
| MGJ | Mucogingival junction |
| RC | Root coverage |
| CRC | Complete root coverage |
| RES | Root coverage esthetic score |
References
- Cortellini, P.; Bissada, N.-F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J. Periodontol. 2018, 89, S204–S213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassab, M.-M.; Cohen, R.-E. The etiology and prevalence of gingival recession. J. Am. Dent. Assoc. 2003, 134, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Mandelaris, G.-A.; Neiva, R.; Chambrone, L. Cone-Beam Computed Tomography and Interdisciplinary Dentofacial Therapy: An American Academy of Periodontology Best Evidence Review Focusing on Risk Assessment of the Dentoalveolar Bone Changes Influenced by Tooth Movement. J. Periodontol. 2017, 88, 960–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebistorf, M.; Mijuskovic, M.; Pandis, N.; Fudalej, P.-S.; Katsaros, C. Gingival recession in orthodontic patients 10 to 15 years posttreatment: A retrospective cohort study. Am. J. Orthod. Dentofacial. Orthop. 2018, 153, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Charavet, C.; Vives, F.; Aroca, S.; Dridi, S.-M. “Wire Syndrome” Following Bonded Orthodontic Retainers: A Systematic Review of the Literature. Healthcare 2022, 10, 379. [Google Scholar] [CrossRef]
- Müller, H.-P.; Schaller, N.; Eger, T.; Heinecke, A. Thickness of masticatory mucosa. J. Clin. Periodontol. 2000, 27, 431–436. [Google Scholar] [CrossRef]
- Zuhr, O.; Rebele, S.-F.; Cheung, S.-L.; Hürzeler, M.-B. Research Group on Oral Soft Tissue Biology and Wound Healing. Surgery without papilla incision: Tunneling flap procedures in plastic periodontal and implant surgery. Periodontol. 2000 2018, 77, 123–149. [Google Scholar] [CrossRef]
- Zucchelli, G.; Marzadori, M.; Mounssif, I.; Mazzotti, C.; Stefanini, M. Coronally advanced flap + connective tissue graft techniques for the treatment of deep gingival recession in the lower incisors. A controlled randomized clinical trial. J. Clin. Periodontol. 2014, 41, 806–813. [Google Scholar] [CrossRef]
- Stefanini, M.; Mounssif, I.; Marzadori, M.; Mazzotti, C.; Mele, M.; Zucchelli, G. Vertically Coronally Advanced Flap (V-CAF) to Increase Vestibule Depth in Mandibular Incisors. Int. J. Periodontics Restor. Dent. 2021, 41, 325–333. [Google Scholar] [CrossRef]
- Sculean, A.; Allen, E.-P. The Laterally Closed Tunnel for the Treatment of Deep Isolated Mandibular Recessions: Surgical Technique and a Report of 24 Cases. Int. J. Periodontics Restor. Dent. 2018, 38, 479–487. [Google Scholar] [CrossRef]
- Allen, E.-P. Soft tissue grafting with the tunnel technique in the mandibular anterior: Myths and realities. J. Esthet. Restor. Dent. 2021, 33, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Quispe-López, N.; Castaño-Séiquer, A.; Pardal-Peláez, B.; Garrido-Martínez, P.; Gómez-Polo, C.; Mena-Álvarez, J.; Montero-Martín, J. Clinical Outcomes of the Double Lateral Sliding Bridge Flap Technique with Simultaneous Connective Tissue Graft in Sextant V Recessions: Three-Year Follow-Up Study. Appl. Sci. 2022, 12, 1038. [Google Scholar] [CrossRef]
- Chambrone, L.; Sukekava, F.; Araújo, M.-G.; Pustiglioni, F.-E.; Chambrone, L.-A.; Lima, L.-A. Root-coverage procedures for the treatment of localized recession-type defects: A Cochrane systematic review. J. Periodontol. 2010, 81, 452–478. [Google Scholar] [CrossRef] [PubMed]
- Bethaz, N.; Romano, F.; Ferrarotti, F.; Mariani, G.-M.; Aimetti, M. A mucogingival technique for the treatment of multiple recession defects in the mandibular anterior region: A case series with a 2-year follow-up. Int. J. Periodontics Restor. Dent. 2014, 34, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Miller, P.D., Jr. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- O’Leary, T.-J.; Drake, R.-B.; Naylor, J.-E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Ronay, V.; Sahrmann, P.; Bindl, A.; Attin, T.; Schmidlin, P.-R. Current status and perspectives of mucogingival soft tissue measurement methods. J. Esthet. Restor. Dent. 2011, 23, 146–156. [Google Scholar] [CrossRef]
- Cairo, F.; Nieri, M.; Cattabriga, M.; Cortellini, P.; De Paoli, S.; De Sanctis, M.; Fonzar, A.; Francetti, L.; Merli, M.; Rasperini, G.; et al. Root coverage esthetic score after treatment of gingival recession: An interrater agreement multicenter study. J. Periodontol. 2010, 81, 1752–1758. [Google Scholar] [CrossRef]
- Hurzeler, M.-B.; Weng, D. A single-incision technique to harvest subepithelial connective tissue grafts from the palate. Int. J. Periodontics Restor. Dent. 1999, 19, 279–287. [Google Scholar]
- Bouchard, P.; Malet, J.; Borghetti, A. Decision-making in aesthetics: Root coverage revisited. Periodontol. 2000 2001, 27, 97–120. [Google Scholar] [CrossRef] [Green Version]
- César-Neto, J.-B.; Cavalcanti, M.-C.; Sekiguchi, R.T.; Pannuti, C.-M.; Romito, G.-A.; Tatakis, D.-N. Root Coverage for Single Deep Gingival Recessions: Outcomes Based on a Decision-Making Algorithm. Int. J. Dent. 2019, 2019, 1830765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: An explorative and reliability study. J. Clin. Periodontol. 2011, 38, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Pannuti, C.-M.; Tu, Y.-K.; Chambrone, L.-A. Evidence-based periodontal plastic surgery. II. An individual data meta-analysis for evaluating factors in achieving complete root coverage. J Periodontol. 2012, 83, 477–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guldener, K.; Lanzrein, C.; Eliezer, M.; Katsaros, C.; Stähli, A.; Sculean, A. Treatment of single mandibular recessions with the modified coronally advanced tunnel or laterally closed tunnel, hyaluronic acid, and subepithelial connective tissue graft: A report of 12 cases. Quintessence Int. 2020, 51, 456–463. [Google Scholar] [CrossRef]
- Holtzman, L.P.; Blasi, G.; Rivera, E.; Herrero, F.; Downton, K.; Oates, T. Gingival Thickness and Outcome of Periodontal Plastic Surgery Procedures: A Meta-regression Analysis. JDR Clin. Trans. Res. 2021, 6, 295–310. [Google Scholar] [CrossRef]
- Nieri, M.; Pini-Prato, G.-P.; Giani, M.; Magnani, N.; Pagliaro, U.; Rotundo, R. Patient perceptions of buccal gingival recessions and requests for treatment. J. Clin. Periodontol. 2013, 40, 707–712. [Google Scholar] [CrossRef]
- Cairo, F.; Barootchi, S.; Tavelli, L.; Barbato, L.; Wang, H.-L.; Rasperini, G.; Graziani, F.; Tonetti, M. Aesthetic-And patient-related outcomes following root coverage procedures: A systematic review and network meta-analysis. J. Clin. Periodontol. 2020, 47, 1403–1415. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 14; 100%) | Double Lateral Sliding Bridge Flap Group (n = 7; 50%) | Laterally Closed Tunnel Group (n = 7; 50%) | Comparison | ||||
|---|---|---|---|---|---|---|---|
| Parameters | N | Mean ± SD | Range | Mean ± SD | Range | U Mann–Whitney | U Statistics p-Value |
| GRD (mm) | |||||||
| Baseline | 14 | 4.3 ± 1.2 | 3–6 | 4.9 ± 1.1 | 3–6 | 2.6 | 0.11 |
| Final follow-up | 14 | 0.6 ± 1.1 | 0–3 | 0.1 ± 0.4 | 0–1 | 0.4 | 0.52 |
| Pre–Post Difference | 14 | 3.7 ± 1.6 | 1–6 | 4.7 ± 1.2 | 3–6 | 2.6 | 0.11 |
| Wilcoxon Pre–Post comparison (p-value) | 0.0 (p = 0.018) * | 0.0 (p = 0.017) * | |||||
| PD (mm) | |||||||
| Baseline | 14 | 2.3 ± 0.8 | 1–3 | 3.7 ± 2.1 | 1–7 | 0.3 | 0.59 |
| Final follow-up | 14 | 2.7 ± 1.1 | 2–5 | 2.9 ± 0.9 | 2–4 | 0.3 | 0.59 |
| Pre–Post Difference | 14 | (−0.4) ± 1.1 | (−2)–1 | 0.9 ± 1.7 | (−1)–3 | 1.2 | 0.28 |
| Wilcoxon Pre–Post comparison (p-value) | 15.0 (p = 0.32) | 5.0 (p = 0.23) | |||||
| CAL (mm) | |||||||
| Baseline | 14 | 6.6 ± 1.4 | 5–9 | 8.4 ± 2.1 | 6–11 | 2.6 | 0.11 |
| Final follow-up | 14 | 3.3 ± 1.9 | 2–6 | 3.0 ± 0.8 | 5–9 | 0.0 | 1.0 |
| Pre–Post Difference | 14 | 3.3 ± 1.6 | 0–5 | 5.4 ± 1.8 | 3–8 | 2.8 | 0.09 |
| Wilcoxon Pre–Post comparison (p-value) | 0.0 (p = 0.026) * | 0.0 (p = 0.018) * | |||||
| KTW (mm) | |||||||
| Baseline | 14 | 0.4 ± 0.5 | 0–1 | 0.3 ± 0.5 | 0–1 | 0.3 | 0.58 |
| Final follow-up | 14 | 3.6 ± 1.5 | 1–5 | 3.7 ± 1.1 | 2–5 | 0.3 | 0.59 |
| Pre–Post Difference | 14 | 3.1 ± 1.3 | 1–5 | 3.4 ± 1.3 | 2–5 | 0.0 | 1.0 |
| Wilcoxon Pre-Post comparison (p-value) | 28.0 (p = 0.018) * | 28.0 (p = 0.017) * | |||||
| GT (mm) | |||||||
| Baseline | 14 | 0.0 ± 0.0 | 0–0 | 0.0 ± 0.0 | 0–0 | 0.0 | 1.0 |
| Final follow-up | 14 | 1.2 ± 0.2 | 1–1.5 | 1.0 ± 0.1 | 0.8–1.2 | 2.8 | 0.09 |
| Pre–Post Difference | 14 | 1.2 ± 0.2 | 1–1.5 | 1.0 ± 0.1 | 0.8–1.2 | 1.9 | 0.16 |
| Wilcoxon Pre–Post comparison (p-value) | 28.0 (p = 0.018) * | 21.0 (p = 0.027) * | |||||
| % RC | |||||||
| % Final follow-up | 14 | 86.9% ± 28.0% | 25–100 | 96.4% ± 9.4% | 75–100 | 28.0 | 0.53 |
| Double Lateral Sliding Bridge Flap Group (n = 7; 50%) | Laterally Closed Tunnel Group (n = 7; 50%) | Chi-Squared Comparison | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Parameters | NO | YES | NO | YES | X2 | p-Value | ||||
| N | % | N | % | N | % | N | % | |||
| Scar | 4 | 57.1 | 3 | 42.9 | 7 | 100 | 0 | 0 | 3.82 | 0.04 * |
| CRC | 2 | 28.6 | 5 | 71.4 | 1 | 14.3 | 6 | 85.7 | 0.42 | 0.52 |
| Double Lateral Sliding Bridge Flap Group (n = 7; 50%) | Laterally Closed Tunnel Group (n = 7; 50%) | Comparison | |
|---|---|---|---|
| RES Parameters | Mean ± SD | Mean ± SD | Mann–Whitney U (p-Value) |
| Gingival Margin level | 5.1 ± 1.5 | 5.6 ± 1.1 | 28.0 (p = 0.53) |
| Marginal Tissue Contour | 0.9 ± 0.4 | 0.9 ± 0.4 | 24.5 (1.0) |
| Soft Tissue Texture | 0.4 ± 0.5 | 0.9 ± 0.4 | 35.0 (0.11) |
| Mucogingival Junction | 0.9 ± 0.4 | 0.7 ± 0.5 | 21.0 (0.53) |
| Gingival Color | 0.9 ± 0.4 | 1.0 ± 0.0 | 28.0 (0.32) |
| Total Score (0–10) | 8.1 ± 2.5 | 9.0 ± 1.8 | 1.2 (p = 0.28) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quispe-López, N.; Sánchez-Santos, J.; Delgado-Gregori, J.; López-Malla Matute, J.; López-Valverde, N.; Zubizarreta-Macho, Á.; Flores-Fraile, J.; Gómez-Polo, C.; Montero, J. Double Lateral Sliding Bridge Flap versus Laterally Closed Tunnel for the Treatment of Single Recessions in the Mandibular Anterior Teeth: A Pseudorandomized Clinical Trial. J. Clin. Med. 2022, 11, 2918. https://doi.org/10.3390/jcm11102918
Quispe-López N, Sánchez-Santos J, Delgado-Gregori J, López-Malla Matute J, López-Valverde N, Zubizarreta-Macho Á, Flores-Fraile J, Gómez-Polo C, Montero J. Double Lateral Sliding Bridge Flap versus Laterally Closed Tunnel for the Treatment of Single Recessions in the Mandibular Anterior Teeth: A Pseudorandomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(10):2918. https://doi.org/10.3390/jcm11102918
Chicago/Turabian StyleQuispe-López, Norberto, Juan Sánchez-Santos, Joaquín Delgado-Gregori, Joaquín López-Malla Matute, Nansi López-Valverde, Álvaro Zubizarreta-Macho, Javier Flores-Fraile, Cristina Gómez-Polo, and Javier Montero. 2022. "Double Lateral Sliding Bridge Flap versus Laterally Closed Tunnel for the Treatment of Single Recessions in the Mandibular Anterior Teeth: A Pseudorandomized Clinical Trial" Journal of Clinical Medicine 11, no. 10: 2918. https://doi.org/10.3390/jcm11102918