
Effect of Combined Manual Therapy and Therapeutic Exercise Protocols on the Postural Stability of Patients with Non-Specific Chronic Neck Pain. A Secondary Analysis of Randomized Controlled Trial

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Sample Selection
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Interventions
2.5.1. Group 1: Manual Therapy
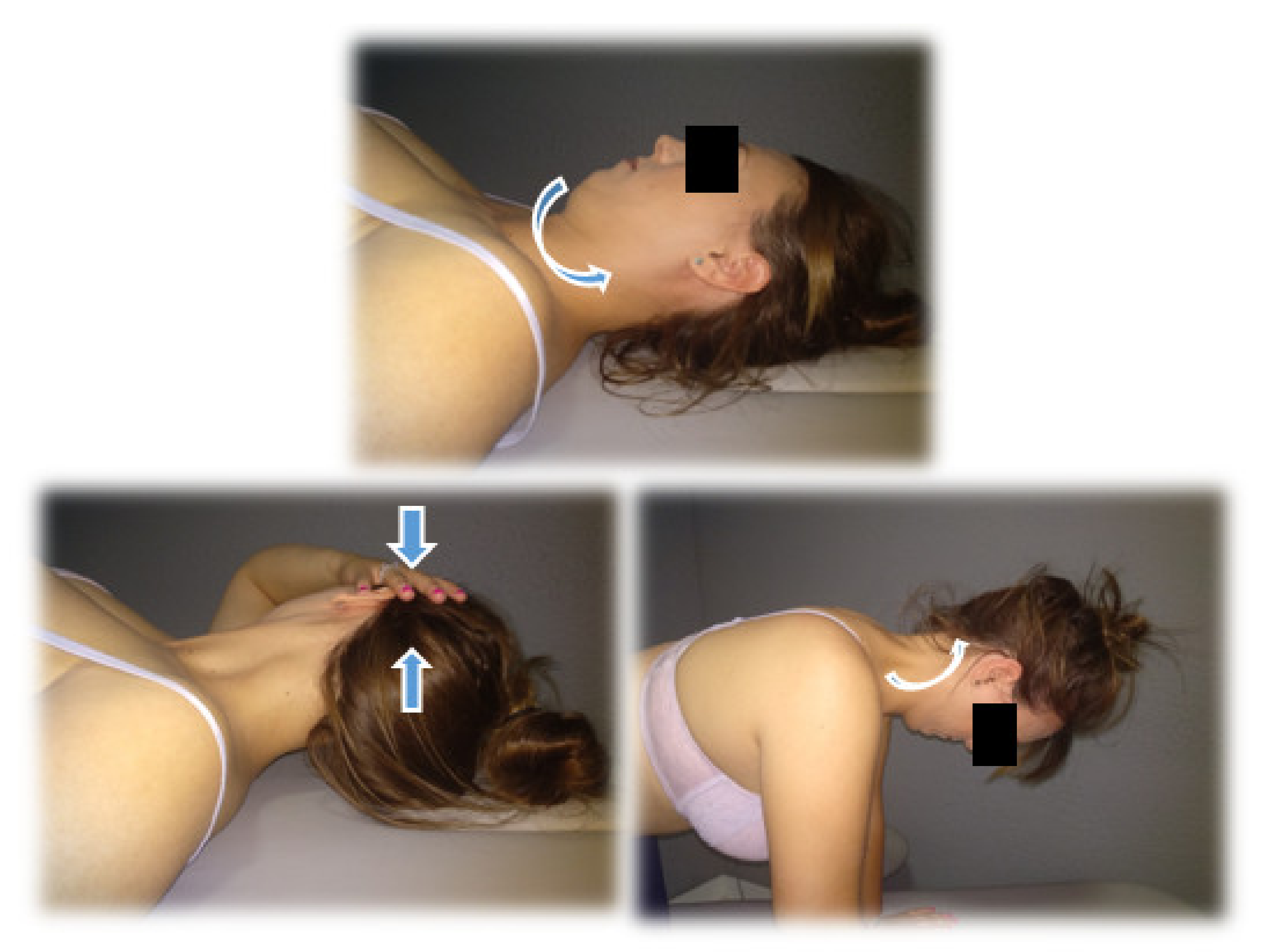
- High Thoracic Manipulation on T4. Patients are positioned supine with their arms crossed in a “V” shape over the chest. The therapist makes contact with the fist at the level of the spinous process of T4 and blocks the patient’s elbows with his chest; following this, he introduces flexion of the cervical spine until a slight tension is felt in the tissues the point of contact. Downward and cranial manipulation is applied. If cavitation is not achieved on the first attempt, the therapist repositions the patient and performs a second manipulation. A maximum of two attempts will be allowed in each patient [32].
- Cervical Articular Mobilization (2 Hz, 2 min × 3 series). The patient is placed on the stretcher prone, placing both hands under his forehead. The therapist makes contact with his two thumbs on the spinous process of the patient’s C2 vertebra and performs grade III posteroanterior impulses at a speed of 2 Hz and for two minutes. There are three mobilization intervals with a minute of rest between each one of them [33].
2.5.2. Group 2: Therapeutic Exercise
- Cranio-cervical flexion (CCF) in supine position with a towel in the posterior area of the neck. (three sets, 10 repetitions, 10 s of contraction each repetition, and 10 s of rest).
- CCF sitting. (three sets, 10 repetitions, 10 s of contraction each repetition with 10 s of rest).
- 3.
- Co-contraction of deep and superficial neck flexors in supine decubitus. (10 repetitions, 10 s of contraction with 10 s of rest).
- 4.
- Co-contraction flexors, rotators, and inclines. Patients will perform cranial nerve flexion while the physiotherapist asks them to tilt, rotate and look towards the same side while he opposes a resistance with his hand. (10 repetitions, 10 s of contraction with 10 s of rest).
- 5.
- Eccentric for extensors. The patient seated should perform cervical extension; then, they must complete a cranio-cervical flexion and finish doing a cervical flexion (10 repetitions).
- 6.
- Eccentric for flexors. The patient will be in a quadrupedal and neutral neck position, should perform neck flexion. They must complete a cranio-cervical flexion and maintain that posture extending the neck and then finally losing the cranio-cervical flexion (10 repetitions).
2.5.3. Group 3: Sham Treatment
2.6. Outcomes Measures
2.7. Sample Size Calculation
2.8. Randomization
2.9. Blinding
2.10. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beltran-Alacreu, H.; López-De-Uralde-Villanueva, I.; Lobo, C.C.; La-Touche, R.; de la Cuerda, R.C.; Gil-Martínez, A.; Fernandez-Ayuso, D.; Fernandez-Carnero, J. Prediction models of health-related quality of life in different neck pain conditions: A cross-sectional study. Patient Prefer. Adherence 2018, 12, 657–666. [Google Scholar] [CrossRef] [Green Version]
- Daffner, S.D.; Hilibrand, A.S.; Hanscom, B.S.; Brislin, B.T.; Vaccaro, A.R.; Albert, T.J. Impact of Neck and Arm Pain on Overall Health Status. Spine 2003, 28, 2030–2035. [Google Scholar] [CrossRef]
- Treleaven, J.; Jull, G.; Sterling, M. Dizziness and unsteadiness following whiplash injury: Characteristic features and relationship with cervical joint position error. J. Rehabil. Med. 2003, 35, 36–43. [Google Scholar] [CrossRef]
- Grande-Alonso, M.; Saiz, B.M.; Zuazo, A.M.; Lara, S.L.; La Touche, R. Biobehavioural analysis of the vestibular system and posture control in patients with cervicogenic dizziness. A cross-sectional study. Neurología 2018, 33, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Cuenca-Martínez, F.; Bartrina-Rodríguez, I.; Suso-Martí, L.; La Touche, R.; Ferrer-Peña, R. Association between somatosensory, motor and psychological variables by levels of disability in patients with cervicogenic dizziness. Somatosens. Mot. Res. 2018, 35, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Kristjansson, E.; Treleaven, J. Sensorimotor Function and Dizziness in Neck Pain: Implications for Assessment and Management. J. Orthop. Sports Phys. Ther. 2009, 39, 364–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.-H.; Chien, A.; Hsu, W.-L.; Yen, L.-W.; Lin, Y.-H.; Cheng, H.-Y.K. Changes of postural control and muscle activation pattern in response to external perturbations after neck flexor fatigue in young subjects with and without chronic neck pain. Gait Posture 2015, 41, 801–807. [Google Scholar] [CrossRef]
- Dutia, M. The muscles and joints of the neck: Their specialisation and role in head movement. Prog. Neurobiol. 1991, 37, 165–178. [Google Scholar] [CrossRef]
- Kulkarni, V.; Chandy, M.J.; Babu, K.S. Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurol. India 2001, 49, 355–359. [Google Scholar] [PubMed]
- Hsu, W.-L.; Chen, C.P.; Nikkhoo, M.; Lin, C.-F.; Ching, C.T.-S.; Niu, C.-C.; Cheng, C.-H. Fatigue changes neck muscle control and deteriorates postural stability during arm movement perturbations in patients with chronic neck pain. Spine J. 2020, 20, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Koskikmies, K.; Sutinen, P.; Aalto, H.; Starck, J.; Toppila, E.; Hirvonen, T.; Kaksonen, R.; Ishizaki, H.; Alaranta, H.; Pyykkö, I. Postural stability, neck propioception and tension neck. Acta Oto-Laryngol. 1997, 529, 95–97. [Google Scholar] [CrossRef] [PubMed]
- L’Heureux-Lebeau, B.; Godbout, A.; Berbiche, D.; Saliba, I. Evaluation of Paraclinical Tests in the Diagnosis of Cervicogenic Dizziness. Otol. Neurotol. 2014, 35, 1858–1865. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, Y.; Weber, B.R.; Grob, D.; Müntener, M. Fiber composition and fiber transformations in neck muscles of patients with dysfunction of the cervical spine. J. Orthop. Res. 1995, 13, 240–249. [Google Scholar] [CrossRef]
- McPartland, J.M.; Brodeur, R.R.; Hallgren, R.C. Chronic neck pain, standing balance, and suboccipital muscle atrophy—A pilot study. J. Manip. Physiol. Ther. 1997, 20, 24–29. [Google Scholar]
- Field, S.; Treleaven, J.; Jull, G. Standing balance: A comparison between idiopathic and whiplash-induced neck pain. Man. Ther. 2008, 13, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Jull, G.; Kristjansson, E.; Dall’Alba, P. Impairment in the cervical flexors: A comparison of whiplash and insiduous onser neck pain patients. Man. Ther. 2004, 9, 89–94. [Google Scholar] [CrossRef]
- Bigland-Ritchie, B.; Woods, J.J. Changes in muscle contractile properties and neural control during human muscular fatigue. Muscle Nerve 1984, 7, 691–699. [Google Scholar] [CrossRef]
- Taylor, J.; Butler, J.; Allen, G.M.; Gandevia, S. Changes in motor cortical excitability during human muscle fatigue. J. Physiol. 1996, 490, 519–528. [Google Scholar] [CrossRef]
- Schiepatti, M.; Nardone, A.; Schmid, M. Neck muscle fatigue afects postural control in man. Neuroscience 2003, 121, 277–285. [Google Scholar] [CrossRef]
- Flor, H. Cortical reorganisation and chronic pain: Implications for rehabilitation. J. Rehabil. Med. 2003, 35, 66–72. [Google Scholar] [CrossRef] [Green Version]
- Falla, D. Unravelling the complexity of muscle impairment in chronic neck pain. Man. Ther. 2004, 9, 125–133. [Google Scholar] [CrossRef]
- Boudreau, S.A.; Farina, D.; Falla, D. The role of motor learning and neuroplasticity in designing rehabilitation approaches for musculoskeletal pain disorders. Man. Ther. 2010, 15, 410–414. [Google Scholar] [CrossRef]
- Soliman, E.S.; Shousha, T.M.; Alayat, M.S. The effect of pain severity on postural stability and dynamic limits of stability in chronic low back pain. J. Back Musculoskelet. Rehabil. 2017, 30, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Benyamin, R.M.; Singh, V.; Parr, A.T.; Conn, A.; Diwan, S.; Abdi, S. Systematic review of the effectiveness of cervical epidurals in the management of chronic neck pain. Pain Physician 2009, 12, 137–157. [Google Scholar] [CrossRef] [PubMed]
- Abuín-Porras, V.; Clemente-Suárez, V.; Jaén-Crespo, G.; Navarro-Flores, E.; Pareja-Galeano, H.; Romero-Morales, C. Effect of Physiotherapy Treatment in the Autonomic Activation and Pain Perception in Male Patients with Non-Specific Subacute Low Back Pain. J. Clin. Med. 2021, 10, 1793. [Google Scholar] [CrossRef] [PubMed]
- De-La-Cruz-Torres, B.; Martínez-Jiménez, E.; Navarro-Flores, E.; Palomo-López, P.; Abuín-Porras, V.; Díaz-Meco-Conde, R.; López-López, D.; Romero-Morales, C. Heart Rate Variability Monitoring during Interferential Current Application in the Lower Back Area: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 3394. [Google Scholar] [CrossRef] [PubMed]
- Vincent, K.; Maigne, J.; Fischhoff, C.; Lanlo, O.; Dagenais, S. Systematic review of manual therapies for non-specific neck pain. Jt. Bone Spine 2013, 80, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.; Paquin, J.; Dupont, G.; Blanchette, S.; Lalonde, P.; Cristie, T.; Graham, N.; Kay, T.; Burnie, S.; Gelley, G.; et al. Exercises for mechanical neck disorders: A Cochrane review update. Man. Ther. 2016, 24, 25–45. [Google Scholar] [CrossRef]
- Miller, J.; Gross, A.; D’Sylva, J.; Burnie, S.J.; Goldsmith, C.H.; Graham, N.; Haines, T.; Brønfort, G.; Hoving, J.L. Manual therapy and exercise for neck pain: A systematic review. Man. Ther. 2010, 15, 334–354. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.; Rivett, D.A. Manual therapy treatment of cervicogenic dizziness: A systematic review. Man. Ther. 2005, 10, 4–13. [Google Scholar] [CrossRef]
- Holt, K.R.; Haavik, H.; Elley, C.R. The Effects of Manual Therapy on Balance and Falls: A Systematic Review. J. Manip. Physiol. Ther. 2012, 35, 227–234. [Google Scholar] [CrossRef]
- Saavedra-Hernández, M.; Arroyo-Morales, M.; Cantarero-Villanueva, I.; Fernández-Lao, C.; Castro-Sánchez, A.M.; Puentedura, E.; Fernández-De-Las-Peñas, C. Short-term effects of spinal thrust joint manipulation in patients with chronic neck pain: A randomized clinical trial. Clin. Rehabil. 2013, 27, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Lopez, A.; Perez, J.L.A.; Gutierez, J.L.G.; La Touche, R.; Lara, S.L.; Izquierdo, H.; Fernandez-Carnero, J. Mobilization versus manipulations versus sustain apophyseal natural glide techniques and interaction with psychological factors for patients with chronic neck pain: Randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2014, 51, 121–132. [Google Scholar] [PubMed]
- Jeong, E.-D.; Kim, C.-Y.; Kim, S.-M.; Lee, S.-J.; Kim, H.-D. Short-term effects of the suboccipital muscle inhibition technique and cranio-cervical flexion exercise on hamstring flexibility, cranio-vertebral angle, and range of motion of the cervical spine in subjects with neck pain: A randomized controlled trial. J. Back Musculoskelet. Rehabil. 2018, 31, 1025–1034. [Google Scholar] [CrossRef]
- Rizo, A.M.H.; Pascual-Vaca, Á.O.; Albornoz-Cabello, M.; Blanco, C.R.; Pozo, F.P.; Carrasco, A.L. Immediate Effects of the Suboccipital Muscle Inhibition Technique in Craniocervical Posture and Greater Occipital Nerve Mechanosensitivity in Subjects With a History of Orthodontia Use: A Randomized Trial. J. Manip. Physiol. Ther. 2012, 35, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Schomacher, J.; Falla, D. Function and structure of the deep cervical extensor muscles in patients with neck pain. Man. Ther. 2013, 18, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.M.; O’Leary, S.P.; Cagnie, B.; Durbridge, G.; Danneels, L.; Jull, G. Craniocervical Orientation Affects Muscle Activation When Exercising the Cervical Extensors in Healthy Subjects. Arch. Phys. Med. Rehabil. 2010, 91, 1418–1422. [Google Scholar] [CrossRef]
- Price, D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Abraira, V.; Royuela, A.; Corcoll, J.; Alegre, L.; Tomas, M.; Cano, A.; Muriel, A.; Zamora, J.; Del Real, M.T.; et al. Minimum detectable and minimal clinically important changes for pain in patients with non-specific neck pain. BMC Musculoskelet. Disord. 2008, 9, 43. [Google Scholar] [CrossRef] [Green Version]
- Parraca, J.A.; Olivares, P.R.; Carbonell-Baeza, A.; Aparicio, V.A.; Adsuar, J.C.; Gusi, N. Test-Retest reliability of Biodex Balance SD on physically active old people. J. Hum. Sport Exerc. 2011, 6, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Arnold, B.L.; Schmitz, R.J. Examination of balance measures produced by the biodex stability system. J. Athl. Train. 1998, 33, 323–327. [Google Scholar]
- Salavati, M.; Akhbari, B.; Ebrahimi-Takamjani, I.; Bagheri, H.; Ezzati, K.; Kahlaee, A.H. Effect of spinal stabilization exercise on dynamic postural control and visual dependency in subjects with chronic non-specific low back pain. J. Bodyw. Mov. Ther. 2016, 20, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Arifin, N.; Abu Osman, N.A.; Abas, W.A.B.W. Intrarater Test-Retest Reliability of Static and Dynamic Stability Indexes Measurement Using the Biodex Stability System During Unilateral Stance. J. Appl. Biomech. 2014, 30, 300–304. [Google Scholar] [CrossRef]
- Testa, M.; Rossettini, G. Enhance placebo, avoid nocebo: How contextual factors affect physiotherapy outcomes. Man. Ther. 2016, 24, 65–74. [Google Scholar] [CrossRef]
- Rossettini, G.; Carlino, E.; Testa, M. Clinical relevance of contextual factors as triggers of placebo and nocebo effects in musculoskeletal pain. BMC Musculoskelet. Disord. 2018, 19, 27. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.A.; Rivett, D.A.; Katekar, M.G.; Callister, R. Comparison of Mulligan Sustained Natural Apophyseal Glides and Maitland Mobilizations for Treatment of Cervicogenic Dizziness: A Randomized Controlled Trial. Phys. Ther. 2014, 94, 466–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, S.A.; Callister, R.; Snodgrass, S.; Katekar, M.G.; Rivett, D.A. Manual therapy for cervicogenic dizziness: Long-term outcomes of a randomised trial. Man. Ther. 2015, 20, 148–156. [Google Scholar] [CrossRef]
- Del Rey, R.R.; Hernández, M.S.; Blanco, C.R.; Del Cerro, L.P.; Rodríguez, R.A. Short-term effects of spinal thrust joint manipulation on postural sway in patients with chronic mechanical neck pain: A randomized controlled trial. Disabil. Rehabil. 2020, 1–7, epub ahead of print. [Google Scholar] [CrossRef]
- Minguez-Zuazo, A.; Grande-Alonso, M.; Saiz, B.M.; La Touche, R.; Lara, S.L. Therapeutic patient education and exercise therapy in patients with cervicogenic dizziness: A prospective case series clinical study. J. Exerc. Rehabil. 2016, 12, 216–225. [Google Scholar] [CrossRef]
- Bialosky, J.E.; Beneciuk, J.M.; Bishop, M.D.; Coronado, R.; Penza, C.W.; Simon, C.B.; George, S.Z. Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. J. Orthop. Sports Phys. Ther. 2018, 48, 8–18. [Google Scholar] [CrossRef]
- Bialosky, J.E.; George, S.Z.; Bishop, M.D. How Spinal Manipulative Therapy Works: Why Ask Why? J. Orthop. Sports Phys. Ther. 2008, 38, 293–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, A.; Brunner, F.; Wright, A.; Bachmann, L.M. Paradigm shift in manual therapy? Evidence for a central nervous system component in response to passive cervical joint mobilisation. Man. Ther. 2008, 13, 387–396. [Google Scholar] [CrossRef]
- Falla, D.; Hodges, P. Individualized Exercise Interventions for Spinal Pain. Exerc. Sport Sci. Rev. 2017, 45, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Pool, J.J.; Ostelo, R.W.; Knol, D.; Bouter, L.M.; de Vet, H.C. Are psychological factors prognostic indicators of outcome in patients with sub-acute neck pain? Man. Ther. 2010, 15, 111–116. [Google Scholar] [CrossRef] [Green Version]
- Bahat, H.S.; Weiss, P.L.; Sprecher, E.; Krasovsky, A.; Laufer, Y. Do neck kinematics correlate with pain intensity, neck disability or with fear of motion? Man. Ther. 2014, 19, 252–258. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VARIABLES | GROUP | Z | ||
|---|---|---|---|---|
| MT | TE | C | p | |
| Age (i) | 42.95 ± 2.89 | 36.78 ± 2.89 | 36.90 ± 2.89 | 0.312 b |
| Gender (ii) (male, female; %) | 23 (5/22); 77 (17/22) | 22 (5/23); 78 (18/23) | 29 (6/21); 71 (15/21) | 0.315 c |
| Body Mass Index (i) (Kg/m) | 24.67 ± 1.13 | 23.8 ± 0.72 | 24.75 ± 0.75 | 0.379 b |
| VAS (i) (mm) | 41.95 ± 4.03 | 48.17 ± 3.48 | 49.80 ± 3.53 | 0.237 b |
| OBI (i) | 6.34 ± 0.77 | 4.95 ± 0.59 | 5.47 ± 0.64 | 0.498 b |
| VAS Pre (i) | VAS Week 1 (i) | p | VAS Week 4 (i) | p | VAS Week 12 (i) | p | |
|---|---|---|---|---|---|---|---|
| MT | 41.95 ± 4.03 | 32.77 ± 3.14 | 0.007 * b | 15.82 ± 3.26 | 0.001 * b | 18.23 ± 4.33 | 0.002 * b |
| TE | 48.17 ± 3.48 | 35.83 ± 3.88 | 0.008 * a | 17.83± 3.42 | 0.001 * b | 24.43 ± 4.70 | 0.002 * b |
| C | 49.80 ± 3.53 | 49.25 ± 3.53 | 0.342 a | 50.55 ± 3.54 | 0.518 a | 48.75 ± 3.51 | 0.337 a |
| OBI Pre (i) |
OBI Week 1 (i) | p |
OBI Week 4 (i) | p |
OBI Week 12 (i) | p | |
|---|---|---|---|---|---|---|---|
| MT | 6.34 ±0.77 | 4.87 ± 0.64 | 0.001 * b | 4.01 ± 0.47 | 0.001 * b | 4.77 ± 0.65 | 0.003 * b |
| TE | 4.95 ±0.59 | 3.91 ± 0.41 | 0.017 * b | 4.06 ±0.73 | 0.013 * b | 3.83 ± 0.47 | 0.010 * b |
| C | 5.47 ±0.64 | 5.42 ± 0.62 | 0.808 b | 5.47 ± 0.66 | 0.745 b | 5.43 ± 0.62 | 0.579 b |
| VARIABLE | p | Post hoc | p | p | Post hoc | p | p | Post hoc | p |
|---|---|---|---|---|---|---|---|---|---|
| Week 1 | Week 4 | Week 12 | M and CI | ||||||
| VAS | 0.067 a | MT–C | 0.0329 c | 0.001 a | MT–C | 0.001 * c | 0.003 a | MT–C | 0.008 * c |
| 7.61 | 26.71 | 22.77 | |||||||
| [−3.92 to 19.14] | [12.30 to 41.11] | [4.79 to 40.76] | |||||||
| TE–C | 0.070 c | TE–C | 0.001 * c | TE–C | 0.007 * c | ||||
| 10.77 | 30.92 | 22.79 | |||||||
| [−0.64 to 22.19] | [16.67 to 45.17] | [5.00 to 40.58] | |||||||
| MT–TE | 1.000 c | MT–TE | 1.000 c | MT–TE | 1.000 c | ||||
| 3.17 | −4.21 | −0.01 | |||||||
| [−14.44 to 8.11] | [−18.29 to 9.87] | [−17.59 to 17.56] | |||||||
| OBI | 0.003 * b | MT–C | 0.001 * d | 0.001 * b | MT–C | 0.001 * d | 0.013 * b | MT–C | 0.006 * d |
| 1.41 | 2.30 | 1.53 | |||||||
| [0.32 to 2.50] | [0.98 to 3.63] | [0.22 to 2.83] | |||||||
| TE–C | 0.116 d | TE–C | 0.013 * d | TE–C | 0.028 * d | ||||
| 0.99 | 0.88 | 1.08 | |||||||
| [−0.09 to 2.06] | [−0.44 to 2.19] | [−0.21 to 2.38] | |||||||
| MT–TE | 0.261 d | MT–TE | 0.064 d | MT–TE | 0.420 d | ||||
| 0.42 | 1.43 | 0.44 | |||||||
| [−0.64 to 1.49] | [0.13 to 2.73] | [−0.84 to 1.72] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernal-Utrera, C.; Anarte-Lazo, E.; Gonzalez-Gerez, J.J.; Saavedra-Hernandez, M.; De-La-Barrera-Aranda, E.; Serrera-Figallo, M.A.; Gonzalez-Martin, M.; Rodriguez-Blanco, C. Effect of Combined Manual Therapy and Therapeutic Exercise Protocols on the Postural Stability of Patients with Non-Specific Chronic Neck Pain. A Secondary Analysis of Randomized Controlled Trial. J. Clin. Med. 2022, 11, 84. https://doi.org/10.3390/jcm11010084
Bernal-Utrera C, Anarte-Lazo E, Gonzalez-Gerez JJ, Saavedra-Hernandez M, De-La-Barrera-Aranda E, Serrera-Figallo MA, Gonzalez-Martin M, Rodriguez-Blanco C. Effect of Combined Manual Therapy and Therapeutic Exercise Protocols on the Postural Stability of Patients with Non-Specific Chronic Neck Pain. A Secondary Analysis of Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(1):84. https://doi.org/10.3390/jcm11010084
Chicago/Turabian StyleBernal-Utrera, Carlos, Ernesto Anarte-Lazo, Juan Jose Gonzalez-Gerez, Manuel Saavedra-Hernandez, Elena De-La-Barrera-Aranda, Maria Angeles Serrera-Figallo, Maribel Gonzalez-Martin, and Cleofas Rodriguez-Blanco. 2022. "Effect of Combined Manual Therapy and Therapeutic Exercise Protocols on the Postural Stability of Patients with Non-Specific Chronic Neck Pain. A Secondary Analysis of Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 1: 84. https://doi.org/10.3390/jcm11010084