
Defining a Synovial Fluid White Blood Cell Count Threshold to Predict Periprosthetic Infection after Shoulder Arthroplasty

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Blood Infection Markers
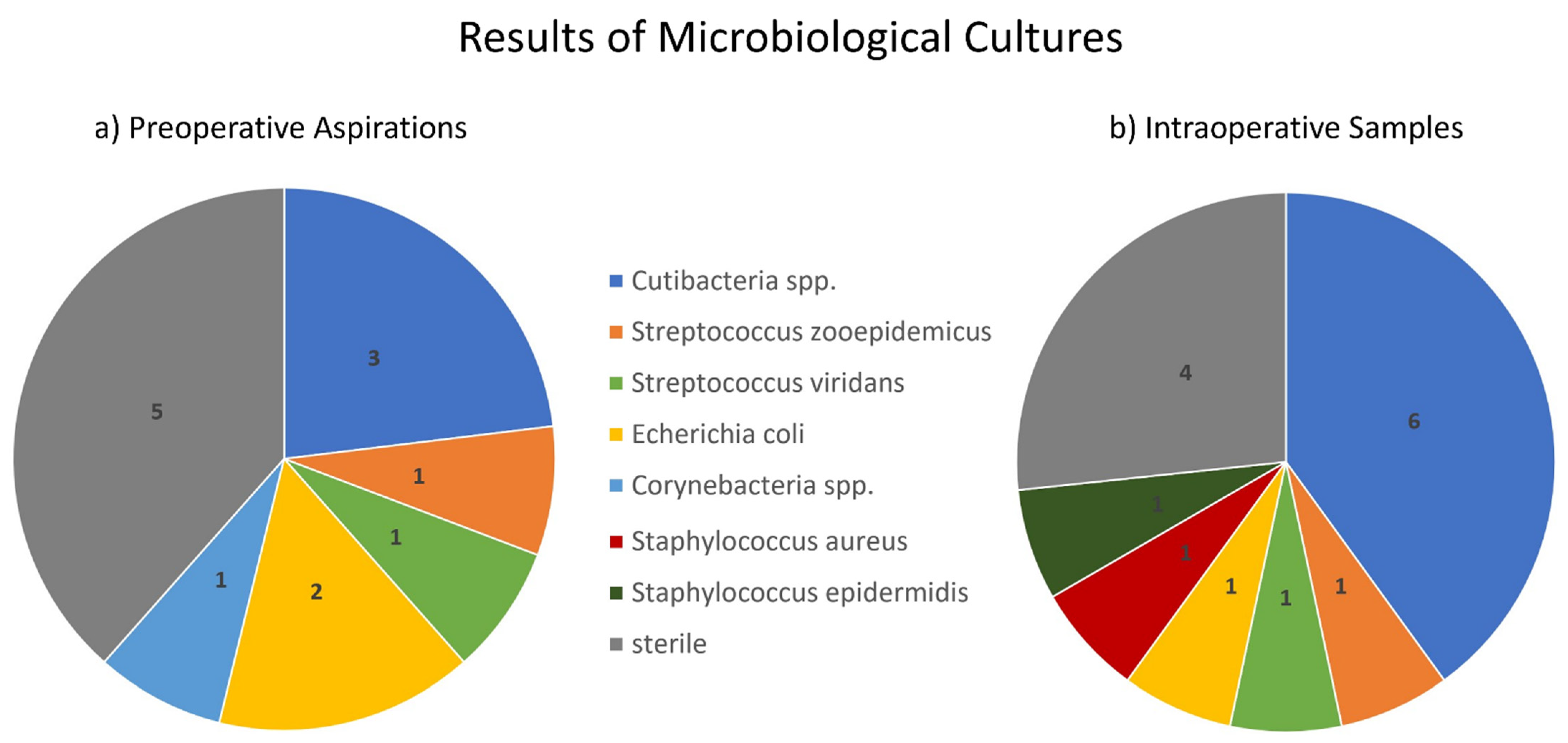
3.2. Microbiological Cultures
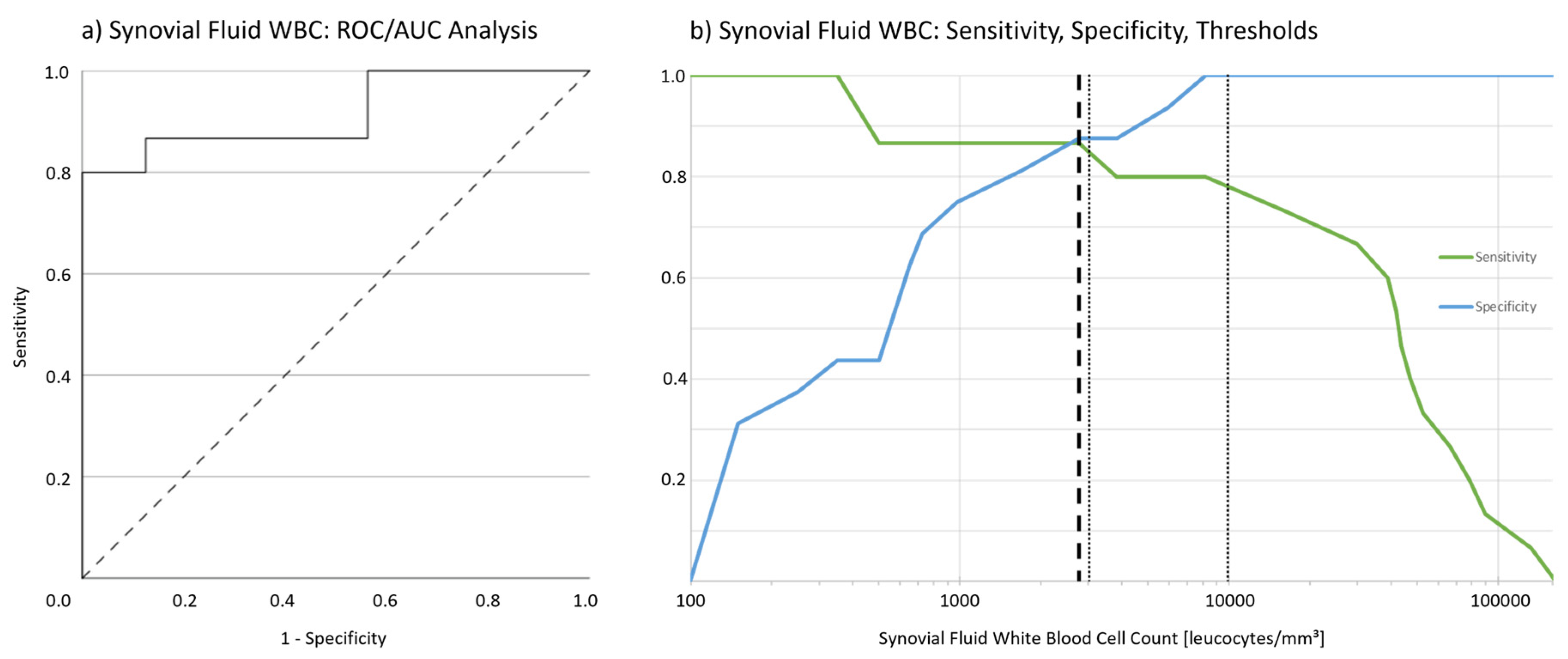
3.3. Synovial WBC in Preoperative Shoulder Joint Aspiration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CRP | c-reactive protein |
| ESR | erythrocyte sedimentation rate |
| ICM Philly | 2018s International consensus meeting on periprosthetic joint infections in Philadelphia |
| IDSA | Infectious Diseases Society of America |
| LR | Likelihood-Ratio |
| MSIS | MusculoSkeletal Infection Society |
| PA | preoperative joint aspiration |
| PSI | prosthetic shoulder infection |
| ROC | receiver operating curve |
| SD | standard deviation |
| WBC | white blood cell count |
References
- Bohsali, K.I.; Bois, A.J.; Wirth, M.A. Complications of Shoulder Arthroplasty. J. Bone Jt. Surg. Am. 2017, 99, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Zavala, J.A.; Clark, J.; Kissenberth, M.J.; Tolan, S.J.; Hawkins, R.J. Management of deep infection after reverse total shoulder arthroplasty: A case series. J. Shoulder Elb. Surg. 2012, 21, 1310–1315. [Google Scholar] [CrossRef]
- Sperling, J.W.; Kozak, T.K.; Hanssen, A.D.; Cofield, R.H. Infection After Shoulder Arthroplasty. Clin. Orthop. Relat. Res. 2001, 382, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Mook, W.R.; Garrigues, G.E. Diagnosis and Management of Periprosthetic Shoulder Infections. J. Bone Jt. Surg. Am. 2014, 96, 956–965. [Google Scholar] [CrossRef] [PubMed]
- Jauregui, J.J.; Tran, A.; Kaveeshwar, S.; Nadarajah, V.; Chaudhri, M.W.; Henn, R.F.; Gilotra, M.N.; Hasan, S.A. Diagnosing a periprosthetic shoulder infection: A systematic review. J. Orthop. 2021, 26, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.C.; Hasan, S.S. Is There a Role for Preoperative Joint Aspiration in the Evaluation of a Shoulder Arthroplasty for Periprosthetic Joint Infection (PJI)?: ICM Shoulder Q&A. ICM Philadelphia Shoulder Q&A. 2018, pp. 576–577. Available online: https://icmphilly.com/questions/is-there-a-role-for-preoperative-joint-aspiration-in-the-evaluation-of-a-shoulder-arthroplasty-for-periprosthetic-joint-infection-pji/ (accessed on 20 November 2021).
- Nodzo, S.R.; Boyle, K.K.; Bhimani, S.; Duquin, T.R.; Miller, A.O.; Westrich, G.H. Propionibacterium acnes Host Inflammatory Response During Periprosthetic Infection Is Joint Specific. HSS J. 2017, 13, 159–164. [Google Scholar] [CrossRef]
- Strahm, C.; Zdravkovic, V.; Egidy, C.; Jost, B. Accuracy of Synovial Leukocyte and Polymorphonuclear Cell Count in Patients with Shoulder Prosthetic Joint Infection. J. Bone Jt. Infect. 2018, 3, 245–248. [Google Scholar] [CrossRef]
- Cortes Jimenez, L.E. Is There a Role for Synovial Fluid White Blood Cell Count (WBC) and Differential in the Diagnosis of Shoulder Periprotsthetic Infection (PJI)?: Shoulder Q&A. ICM Philadelphia Shoulder Q&A. 2018. Available online: https://icmphilly.com/questions/is-there-a-role-for-synovial-fluid-white-blood-cell-wbc-count-and-differential-in-the-diagnosis-of-shoulder-periprosthetic-joint-infection-pji/ (accessed on 20 November 2021).
- Ince, A.; Seemann, K.; Frommelt, L.; Katzer, A.; Lohr, J.F. One-stage revision of shoulder arthroplasty in the case of periprosthetic infection. Z. Orthop. Ihre Grenzgeb. 2004, 142, 611–617. [Google Scholar] [CrossRef]
- Jacquot, A.; Sirveaux, F.; Roche, O.; Favard, L.; Clavert, P.; Molé, D. Surgical management of the infected reversed shoulder arthroplasty: A French multicenter study of reoperation in 32 patients. J. Shoulder Elb. Surg. 2015, 24, 1713–1722. [Google Scholar] [CrossRef]
- Strickland, J.P.; Sperling, J.W.; Cofield, R.H. The results of two-stage re-implantation for infected shoulder replacement. J. Bone Jt. Surg. Br. 2008, 90, 460–465. [Google Scholar] [CrossRef]
- Dilisio, M.F.; Miller, L.R.; Warner, J.J.; Higgins, L.D. Arthroscopic Tissue Culture for the Evaluation of Periprosthetic Shoulder Infection. J. Bone Jt. Surg. Am. Vol. 2014, 96, 1952–1958. [Google Scholar] [CrossRef] [Green Version]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R.; Infectious Diseases Society of America. Diagnosis and Management of Prosthetic Joint Infection: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [Green Version]
- Garrigues, G.E.; Green, A.; Zmistowski, B.; Hsu, J.; Ricchetti, E.; Namdari, S.; Frankle, M.; Gerber, C.; Tashjian, R.; Matsen, F. What are the Diagnostic Criteria of Shoulder Periprosthetic Joint Infection (PJI)?: ICM Shoulder Q&A. ICM Philadelphia Shoulder Q&A. 2018, pp. 558–565. Available online: https://icmphilly.com/questions/what-are-the-diagnostic-criteria-of-shoulder-periprosthetic-joint-infection-pji/ (accessed on 20 November 2021).
- Shohat, N.; Bauer, T.; Buttaro, M.; Budhiparama, N.; Cashman, J.; della Valle, C.J.; Drago, L.; Gehrke, T.; Gomes, L.S.M.; Goswami, K.; et al. What is the Definition of a Periprosthetic Joint Infection (PJI) of the Knee and the Hip? Can the Same Criteria be Used for Both Joints? ICM Philadelphia Hip and Knee Q&A. 2018, pp. 337–339. Available online: https://icmphilly.com/questions/what-is-the-definition-of-a-periprosthetic-joint-infection-pji-of-the-knee-and-the-hip-can-the-same-criteria-be-used-for-both-joints/ (accessed on 20 November 2021).
- Boelch, S.P.; Streck, L.E.; Plumhoff, P.; Konrads, C.; Gohlke, F.; Rueckl, K. Infection control and outcome of staged reverse shoulder arthroplasty for the management of shoulder infections. JSES Int. 2020, 4, 959–963. [Google Scholar] [CrossRef]
- Nelson, G.N.; Davis, D.E.; Namdari, S. Outcomes in the treatment of periprosthetic joint infection after shoulder arthroplasty: A systematic review. J. Shoulder Elb. Surg. 2016, 25, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Achermann, Y.; Goldstein, E.J.C.; Coenye, T.; Shirtliff, M.E. Propionibacterium acnes: From Commensal to Opportunistic Biofilm-Associated Implant Pathogen. Clin. Microbiol. Rev. 2014, 27, 419–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, L.R. Effect of Media on Transport and Recovery of Anaerobic Bacteria. Clin. Infect. Dis. 1997, 25, S134–S136. [Google Scholar] [CrossRef] [Green Version]
- Pottinger, P.; Butler-Wu, S.; Neradilek, M.B.; Merritt, A.; Bertelsen, A.; Jette, J.L.; Warme, W.J.; Matsen, F.A. Prognostic Factors for Bacterial Cultures Positive for Propionibacterium acnes and Other Organisms in a Large Series of Revision Shoulder Arthroplasties Performed for Stiffness, Pain, or Loosening. J. Bone Jt. Surg. Am. 2012, 94, 2075–2083. [Google Scholar] [CrossRef] [PubMed]
- Frangiamore, S.J.; Saleh, A.; Grosso, M.J.; Alolabi, B.; Bauer, T.W.; Iannotti, J.P.; Ricchetti, E.T. Early Versus Late Culture Growth of Propionibacterium acnes in Revision Shoulder Arthroplasty. J. Bone Jt. Surg. Am. 2015, 97, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Pulido, L.; Ghanem, E.; Joshi, A.; Purtill, J.J.; Parvizi, J. Periprosthetic Joint Infection: The Incidence, Timing, and Predisposing Factors. Clin. Orthop. Relat. Res. 2008, 466, 1710–1715. [Google Scholar] [CrossRef] [Green Version]
- Roerdink, R.L.; Huijbregts, H.J.T.A.M.; Van Lieshout, A.W.T.; Dietvorst, M.; Van Der Zwaard, B.C. The difference between native septic arthritis and prosthetic joint infections: A review of literature. J. Orthop. Surg. 2019, 27, 2309499019860468. [Google Scholar] [CrossRef]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef] [PubMed]
- Palan, J.; Nolan, C.; Sarantos, K.; Westerman, R.; King, R.; Foguet, P. Culture-negative periprosthetic joint infections. EFORT Open Rev. 2019, 4, 585–594. [Google Scholar] [CrossRef]
- Ottink, K.D.; Strahm, C.; Muller-Kobold, A.; Sendi, P.; Wouthuyzen-Bakker, M. Factors to Consider When Assessing the Diagnostic Accuracy of Synovial Leukocyte Count in Periprosthetic Joint Infection. J. Bone Jt. Infect. 2019, 4, 167–173. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Diagnosis | Number of Patients | Age | Sex |
|---|---|---|---|
| PSI | 15 | 72 years (range 55–84) | 7 male 8 female |
| Non-infection | Periprosthetic fracture: 2 Instability: 3 Aseptic component loosening: 5 Shoulder dislocation: 2 Rotator cuff insufficiency/superior escape: 4 | 70 years (range 45–90) | 3 male 13 female |
| Blood Infection Marker | PSI | Non-Infections | t-Test/U-Test | Correlation with Synovial WBC | ||||
|---|---|---|---|---|---|---|---|---|
| normal range | mean | SD | mean | SD | p | Pearson correlation | p | |
| CRP (mg/dl) | <0.8 | 5.3 | 4.7 | 1.0 | 1.1 | 0.004 * | 0.686 | <0.001 * |
| ESR (mm/h) | <25 | 40 | 21 | 16 | 12 | 0.002 * | 0.792 | <0.001 * |
| Blood WBC (leucocytes/mm3) | 4000–10,000 | 9900 | 3300 | 8600 | 3000 | 0.237 | 0.349 | 0.054 |
| WBC (Leucocytes/mm3) | 99 | 200 | 400 | 700 | 1000 | 1700 | 2800 | 3800 | 5900 | 8200 | 16,100 | 30,000 | 47,200 | 66,500 | 90,000 | 132,500 |
| Sensitivity | 1 | 1 | 1 | 0.867 | 0.867 | 0.867 | 0.867 | 0.800 | 0.800 | 0.800 | 0.733 | 0.667 | 0.400 | 0.267 | 0.133 | 0.067 |
| Specificity | 0 | 0.312 | 0.437 | 0.687 | 0.750 | 0.812 | 0.875 | 0.875 | 0.937 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Likelihood-Ratio | 1 | 1.5 | 1.8 | 2.8 | 3.5 | 4.6 | 6.9 | 6.4 | 12.7 | n/a | n/a | n/a | n/a | n/a | n/a | |
| Youden-Index | 0 | 0.312 | 0.437 | 0.554 | 0.617 | 0.679 | 0.742 | 0.675 | 0.737 | 0.800 | 0.733 | 0.667 | 0.400 | 0.267 | 0.133 | 0.067 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Streck, L.E.; Gaal, C.; Forster, J.; Konrads, C.; von Hertzberg-Boelch, S.P.; Rueckl, K. Defining a Synovial Fluid White Blood Cell Count Threshold to Predict Periprosthetic Infection after Shoulder Arthroplasty. J. Clin. Med. 2022, 11, 50. https://doi.org/10.3390/jcm11010050
Streck LE, Gaal C, Forster J, Konrads C, von Hertzberg-Boelch SP, Rueckl K. Defining a Synovial Fluid White Blood Cell Count Threshold to Predict Periprosthetic Infection after Shoulder Arthroplasty. Journal of Clinical Medicine. 2022; 11(1):50. https://doi.org/10.3390/jcm11010050
Chicago/Turabian StyleStreck, Laura Elisa, Chiara Gaal, Johannes Forster, Christian Konrads, Sebastian Philipp von Hertzberg-Boelch, and Kilian Rueckl. 2022. "Defining a Synovial Fluid White Blood Cell Count Threshold to Predict Periprosthetic Infection after Shoulder Arthroplasty" Journal of Clinical Medicine 11, no. 1: 50. https://doi.org/10.3390/jcm11010050