
Coronally Advanced Flap with Connective Tissue Graft for Treating Orthodontic-Associated Miller Class III Gingival Recession of the Lower Incisors: A One-Year Retrospective Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Initial Therapy
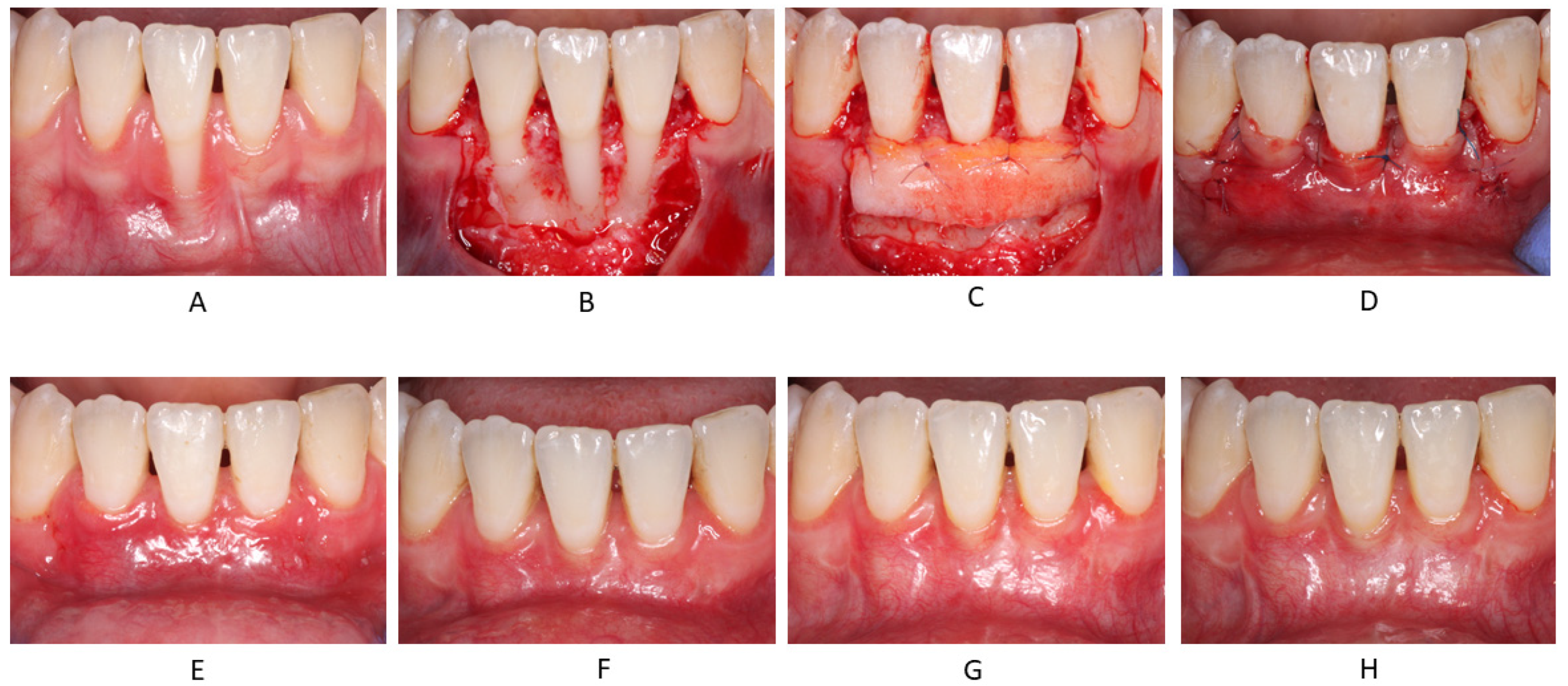
2.2. Surgical Procedures
2.3. Outcome Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prato, G.P.P. Mucogingival Deformities. Ann. Periodontol. 1999, 4, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Mounssif, I. Periodontal plastic surgery. Periodontol. 2000 2015, 68, 333–368. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Tatakis, D.N. Long-Term Outcomes of Untreated Buccal Gingival Recessions: A Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 796–808. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.-J.; Li, X.-D.; Fan, Q.; Liu, X.-J.; Yao, S.; Zhou, Z.; Yang, S.; Shen, Y. Prevalence of gingival recession after orthodontic treatment of infraversion and open bite. J. Orofac. Orthop. Fortschr. Der Kieferorthopädie 2018, 80, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Melsen, B.; Allais, D. Factors of importance for the development of dehiscences during labial movement of mandibular incisors: A retrospective study of adult orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, G.; Kjellsen, K.; Preus, H.; Vandevska-Radunovic, V.; Hansen, B.F. Prevalence and severity of vestibular recession in mandibular incisors after orthodontic treatment. Angle Orthod. 2011, 82, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Wennstrom, J.L.; Lindhe, J.; Sinclair, F.; Thilander, B. Some periodontal tissue reactions to orthodontic tooth movement in monkeys. J. Clin. Periodontol. 1987, 14, 121–129. [Google Scholar] [CrossRef]
- Steiner, G.G.; Pearson, J.K.; Ainamo, J. Changes of the Marginal Periodontium as a Result of Labial Tooth Movement in Monkeys. J. Periodontol. 1981, 52, 314–320. [Google Scholar] [CrossRef]
- Yared, K.F.G.; Zenobio, E.G.; Pacheco, W. Periodontal status of mandibular central incisors after orthodontic proclination in adults. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 6.e1. [Google Scholar] [CrossRef]
- Renkema, A.M.; Fudalej, P.S.; Renkema, A.A.; Abbas, F.; Bronkhorst, E.; Katsaros, C. Gingival labial recessions in orthodontically treated and untreated individuals: A case-control study. J. Clin. Periodontol. 2013, 40, 631–637. [Google Scholar] [CrossRef]
- Bin Bahar, B.S.; Alkhalidy, S.R.; Kaklamanos, E.G.; Athanasiou, A.E. Do orthodontic patients develop more gingival recession in anterior teeth compared to untreated individuals? A systematic review of controlled studies. Int. Orthod. 2019, 18, 1–9. [Google Scholar] [CrossRef]
- Dorfman, H.S. Mucogingival changes resulting from mandibular incisor tooth movement. Am. J. Orthod. 1978, 74, 286–297. [Google Scholar] [CrossRef]
- Pandis, N.; Vlahopoulos, K.; Madianos, P.; Eliades, T. Long-term periodontal status of patients with mandibular lingual fixed retention. Eur. J. Orthod. 2007, 29, 471–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beitlitum, I.; Barzilay, V.; Rayyan, F.; Sebaoun, A.; Sarig, R. Post-Orthodontic Lower Incisors Recessions: Combined Periodontic and Orthodontic Approach. Int. J. Environ. Res. Public Health 2020, 17, 8060. [Google Scholar] [CrossRef] [PubMed]
- Laursen, M.G.; Rylev, M.; Melsen, B. The role of orthodontics in the repair of gingival recessions. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 29–34. [Google Scholar] [CrossRef]
- Chaushu, S.; Stabholz, A. Orthodontic-associated localized gingival recession of lower incisors: Who should treat it? Compend. Contin Educ Dent 2013, 34, 6–12. [Google Scholar]
- Roccuzzo, M.; Bunino, M.; Needleman, I.; Sanz, M. Periodontal plastic surgery for treatment of localized gingival recessions: A systematic review. J. Clin. Periodontol. 2002, 29, 178–194. [Google Scholar] [CrossRef]
- Chambrone, L.; Sukekava, F.; Araújo, M.G.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Root-Coverage Procedures for the Treatment of Localized Recession-Type Defects: A Cochrane Systematic Review. J. Periodontol. 2010, 81, 452–478. [Google Scholar] [CrossRef] [PubMed]
- Sebaoun, A.; Nemcovsky, C.E.; Beitlitum, I.; Moses, O. Modified Tunnel Double Papilla Procedure for Root Coverage in the Anterior Mandible. Int. J. Periodontics Restor. Dent. 2019, 39, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Tatakis, D.N.; Chambrone, L.; Allen, E.P.; Langer, B.; McGuire, M.K.; Richardson, C.R.; Zabalegui, I.; Zadeh, H.H. Periodontal Soft Tissue Root Coverage Procedures: A Consensus Report From the AAP Regeneration Workshop. J. Periodontol. 2015, 86, S52–S55. [Google Scholar] [CrossRef] [Green Version]
- Miller, P.D. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- De Sanctis, M.; Zucchelli, G. Coronally advanced flap: A modified surgical approach for isolated recession-type defects: Three-year results. J. Clin. Periodontol. 2007, 34, 262–268. [Google Scholar] [CrossRef]
- Zucchelli, G.; Mele, M.; Stefanini, M.; Mazzotti, C.; Marzadori, M.; Montebugnoli, L.; de Sanctis, M. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: A comparative randomized-controlled clinical trial. J. Clin. Periodontol. 2010, 37, 728–738. [Google Scholar] [CrossRef]
- Zucchelli, G.; Marzadori, M.; Mounssif, I.; Mazzotti, C.; Stefanini, M. Coronally advanced flap + connective tissue graft techniques for the treatment of deep gingival recession in the lower incisors. A controlled randomized clinical trial. J. Clin. Periodontol. 2014, 41, 806–813. [Google Scholar] [CrossRef]
- Prato, G.P.P.; Baldi, C.; Nieri, M.; Franseschi, D.; Cortellini, P.; Clauser, C.; Rotundo, R.; Muzzi, L. Coronally Advanced Flap: The Post-Surgical Position of the Gingival Margin Is an Important Factor for Achieving Complete Root Coverage. J. Periodontol. 2005, 76, 713–722. [Google Scholar] [CrossRef]
- Landsberg, C.; Bender, O.; Weinreb, M.; Wigler, R.; Chackartchi, T.; Matalon, S.; Weinberg, E. Postextraction Ridge Width Alterations Following Socket Seal Surgery—A Retrospective Study. Appl. Sci. 2020, 11, 324. [Google Scholar] [CrossRef]
- Cairo, F.; Rotundo, R.; Miller, P.D.; Prato, G.P.P. Root Coverage Esthetic Score: A System to Evaluate the Esthetic Outcome of the Treatment of Gingival Recession Through Evaluation of Clinical Cases. J. Periodontol. 2009, 80, 705–710. [Google Scholar] [CrossRef]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: An explorative and reliability study. J. Clin. Periodontol. 2011, 38, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Nart, J.; Valles, C.; Mareque, S.; Santos, A.; Sanz-Moliner, J.; Pascual, A. Subepithelial connective tissue graft in combination with a coronally advanced flap for the treatment of Miller Class II and III gingival recessions in mandibular incisors: A case series. Int. J. Periodontics Restor. Dent. 2012, 32, 647–654. [Google Scholar]
- Nart, J.; Valles, C. Subepithelial Connective Tissue Graft in Combination with a Tunnel Technique for the Treatment of Miller Class II and III Gingival Recessions in Mandibular Incisors: Clinical and Esthetic Results. Int. J. Periodontics Restor. Dent. 2016, 36, 591–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercado, F.; Hamlet, S.; Ivanovski, S. Subepithelial connective tissue graft with or without enamel matrix derivative for the treatment of multiple Class III-IV recessions in lower anterior teeth: A 3-year randomized clinical trial. J. Periodontol. 2019, 91, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Barootchi, S.; Tavelli, L.; Barbato, L.; Wang, H.L.; Rasperini, G.; Graziani, F.; Tonetti, M. Aesthetic-And patient-related outcomes following root coverage procedures: A systematic review and network meta-analysis. J. Clin. Periodontol. 2020, 47, 1403–1415. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Pagliaro, U.; Nieri, M. Treatment of gingival recession with coronally advanced flap procedures: A systematic review. J. Clin. Periodontol. 2008, 35, 136–162. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Baseline Mean ± SD | 12 Months Mean ± SD | p Value Baseline vs. 12 Months | Mean Change from Baseline to 12 Months | |
|---|---|---|---|---|
| PD (mm) | 2.3 ± 1.3 | 1.0 ± 0.5 | 0.0001 | −1.3 |
| RD (mm) | 4.2 ± 1.7 | 0.7 ± 0.8 | 0.0001 | −3.5 |
| RW (mm) | 3.8 ± 0.8 | 1.7 ± 1.7 | 0.0001 | −2.1 |
| KTW (mm) | 0.7 ± 0.9 | 2.6 ± 0.8 | 0.0001 | 1.9 |
| 12 Months Mean ± SD | |
|---|---|
| Percentage of root coverage (%RC) | 83 ± 24% |
| Complete root coverage (CRC) | 10/21 (48%) |
| Mean ± SD | |
|---|---|
| GM | 4.4 ± 1.8 (out of 6) |
| MTC | 1.0 ± 0.2 (out of 1) |
| STT | 0.8 ± 0.4 (out of 1) |
| MGJ | 0.7 ± 0.5 (out of 1) |
| Gingival color | 0.4 ± 0.5 (out of 1) |
| RES | 7.1 ± 2.6 (out of 10) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weinberg, E.; Kolerman, R.; Kats, L.; Cohen, O.; Masri, D.; Sebaoun, A.; Slutzkey, G. Coronally Advanced Flap with Connective Tissue Graft for Treating Orthodontic-Associated Miller Class III Gingival Recession of the Lower Incisors: A One-Year Retrospective Study. J. Clin. Med. 2022, 11, 235. https://doi.org/10.3390/jcm11010235
Weinberg E, Kolerman R, Kats L, Cohen O, Masri D, Sebaoun A, Slutzkey G. Coronally Advanced Flap with Connective Tissue Graft for Treating Orthodontic-Associated Miller Class III Gingival Recession of the Lower Incisors: A One-Year Retrospective Study. Journal of Clinical Medicine. 2022; 11(1):235. https://doi.org/10.3390/jcm11010235
Chicago/Turabian StyleWeinberg, Evgeny, Roni Kolerman, Lazar Kats, Omer Cohen, Daya Masri, Alon Sebaoun, and Gil Slutzkey. 2022. "Coronally Advanced Flap with Connective Tissue Graft for Treating Orthodontic-Associated Miller Class III Gingival Recession of the Lower Incisors: A One-Year Retrospective Study" Journal of Clinical Medicine 11, no. 1: 235. https://doi.org/10.3390/jcm11010235