
Does Time to Theatre Affect the Ability to Achieve Fracture Reduction in Tibial Plateau Fractures?
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Radiographic Assessment
2.3. Patient-Reported Outcome Measures
2.4. Data Analysis
3. Results
3.1. Determinants of Fracture Reduction
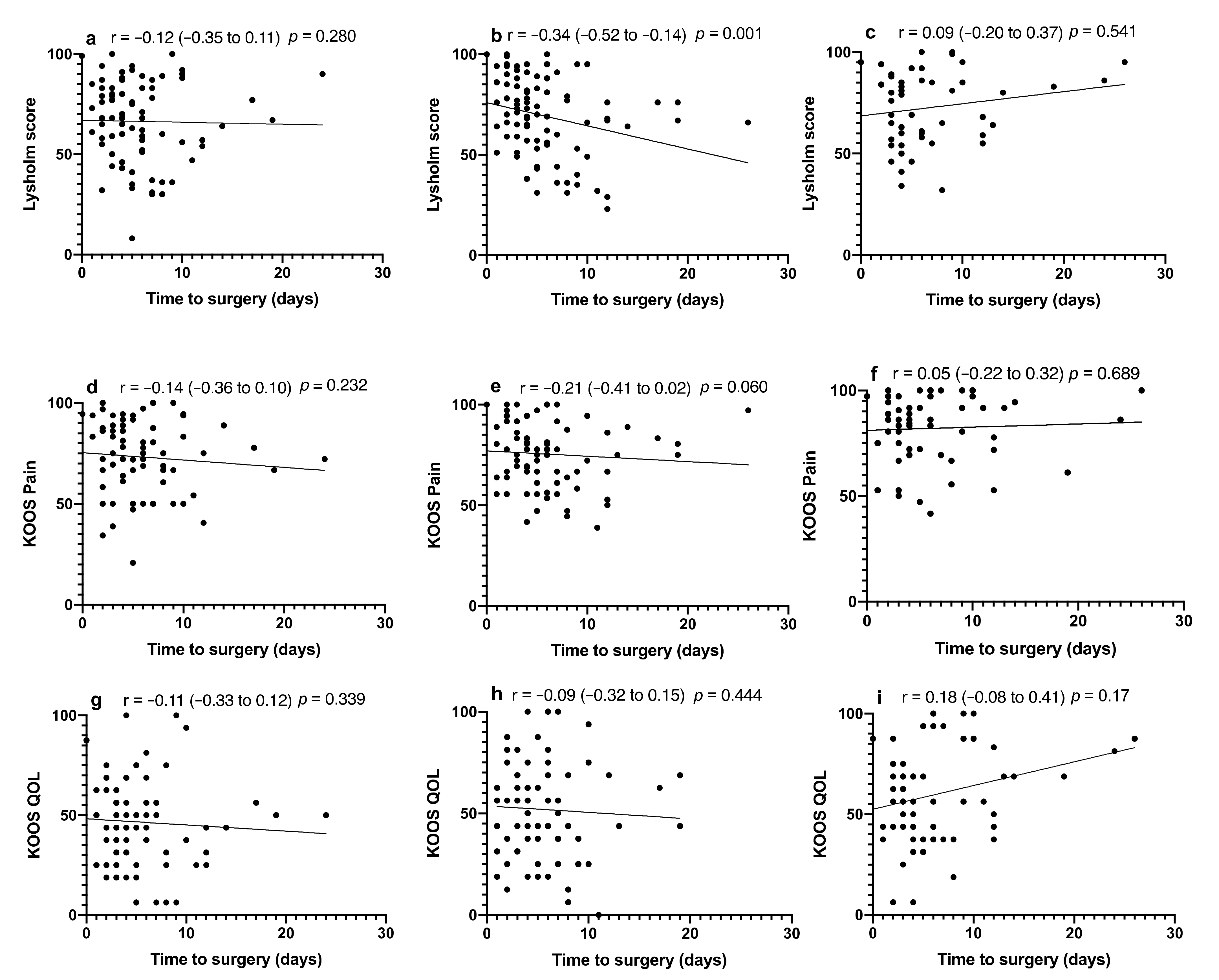
3.2. Influence of Fracture Reduction and Type on PROMs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dailey, S.K.; Phillips, C.T.; Radley, J.M.; Archdeacon, M.T. Achieving Anatomic acetabular fracture reduction—When is the best time to operate? J. Orthop. Trauma 2016, 30, 426–431. [Google Scholar] [CrossRef]
- Madhu, R.; Kotnis, R.; Al-Mousawi, A.; Barlow, N.; Deo, S.; Worlock, P.; Willett, K.; Penn, D.S.; Wasseem, M.; Stanley, J.K. Outcome of surgery for reconstruction of fractures of the acetabulum. The time dependent effect of delay. J. Bone Jt. Surg. Br. Vol. 2006, 88, 1197–1203. [Google Scholar] [CrossRef]
- Solomon, L.B.; Kitchen, D.; Anderson, P.H.; Yang, D.; Starczak, Y.; Kogawa, M.; Perilli, E.; Smitham, P.J.; Rickman, M.S.; Thewlis, D.; et al. Time dependent loss of trabecular bone in human tibial plateau fractures. J. Orthop. Res. 2018, 36, 2865–2875. [Google Scholar] [CrossRef] [PubMed]
- Krause, M.; Alm, L.; Berninger, M.; Domnick, C.; Fehske, K.; Frosch, K.-H.; Herbst, E.; Korthaus, A.; Raschke, M.; Hoffmann, R.; et al. Bone metabolism is a key factor for clinical outcome of tibial plateau fractures. Eur. J. Trauma Emerg. Surg. 2020, 46, 1227–1237. [Google Scholar] [CrossRef]
- Polat, B.; Gurpinar, T.; Polat, A.E.; Ozturkmen, Y. Factors influencing the functional outcomes of tibia plateau fractures after surgical fixation. Niger. J. Clin. Pract. 2019, 22, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, J.; Reul, M.; Nunes Cardozo, M.; Starovoyt, A.; Geusens, E.; Nijs, S.; Hoekstra, H. Functional outcome of intra-articular tibial plateau fractures: The impact of posterior column fractures. Int. Orthop. 2017, 41, 1865–1873. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, I.; McMillan, T.E.; Baliga, S.; Schemitsch, E.H. Primary and secondary total knee arthroplasty for tibial plateau fractures. J. Am. Acad. Orthop. Surg. 2018, 26, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Blokker, C.P.; Rorabeck, C.H.; Bourne, R.B. Tibial plateau fractures. An analysis of the results of treatment in 60 patients. Clin. Orthop. Relat. Res. 1984, 193–199. [Google Scholar] [CrossRef]
- Privalov, M.; Euler, F.; Keil, H.; Swartman, B.; Beisemann, N.; Franke, J.; Grützner, P.A.; Vetter, S.Y. Influence of reduction quality on functional outcome and quality of life in treatment of tibial plafond fractures: A retrospective cohort study. BMC Musculoskelet. Disord. 2019, 20, 534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochen, Y.; Peek, J.; McTague, M.F.; Weaver, M.J.; van der Velde, D.; Houwert, R.M.; Heng, M. Long-term outcomes after open reduction and internal fixation of bicondylar tibial plateau fractures. Injury 2020, 51, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- Schatzker, J.; McBroom, R.; Bruce, D. The tibial plateau fracture. The Toronto experience 1968–1975. Clin. Orthop. Relat. Res. 1979, 94–104. [Google Scholar]
- Civinini, R.; Carulli, C.; Matassi, F.; Villano, M.; Innocenti, M. Total knee arthroplasty after complex tibial plateau fractures. Musculoskelet. Surg. 2009, 93, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Solomon, L.B.; Boopalan, P.R.; Chakrabarty, A.; Callary, S.A. Can tibial plateau fractures be reduced and stabilised through an angiosome-sparing antero-lateral approach? Injury 2014, 45, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Maclean, J.; Kandemir, U. Surgical approaches for tibial plateau fractures. J. Knee Surg. 2014, 27, 021–030. [Google Scholar] [CrossRef] [Green Version]
- Goff, T.; Kanakaris, N.K.; Giannoudis, P.V. Use of bone graft substitutes in the management of tibial plateau fractures. Injury 2013, 44 (Suppl. S1), S86–S94. [Google Scholar] [CrossRef]
- Bachoura, A.; Guitton, T.G.; Smith, R.M.; Vrahas, M.S.; Zurakowski, D.; Ring, D. Infirmity and injury complexity are risk factors for surgical-site infection after operative fracture care. Clin. Orthop. Relat. Res. 2011, 469, 2621–2630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koval, K.J.; Helfet, D.L. Tibial plateau fractures: Evaluation and treatment. J. Am. Acad. Orthop. Surg. 1995, 3, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Colman, M.; Wright, A.; Gruen, G.; Siska, P.; Pape, H.-C.; Tarkin, I. Prolonged operative time increases infection rate in tibial plateau fractures. Injury 2013, 44, 249–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hap, D.X.F.; Kwek, E.B.K. Functional outcomes after surgical treatment of tibial plateau fractures. J. Clin. Orthop. Trauma 2019, 11 (Suppl. S1), S11–S15. [Google Scholar] [CrossRef]
- Eggli, S.; Hartel, M.; Kohl, S.; Haupt, U.; Exadaktylos, A.K.; Röder, C. Unstable Bicondylar Tibial Plateau Fractures: A Clinical Investigation. J. Orthop. Trauma 2008, 22, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Cahueque, M.; Martínez, M.; Cobar, A.; Bregni, M. Early reduction of acetabular fractures decreases the risk of post-traumatic hip osteoarthritis? J. Clin. Orthop. Trauma 2017, 8, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Unno, F.; Lefaivre, K.A.; Osterhoff, G.; Guy, P.; Broekhuyse, H.M.; Blachut, P.A.; O’Brien, P. Is early definitive fixation of bicondylar tibial plateau fractures safe? An observational cohort study. J. Orthop. Trauma 2017, 31, 151–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singleton, N.; Sahakian, V.; Muir, D. Outcome after tibial plateau fracture: How important is restoration of articular congruity? J. Orthop. Trauma 2017, 31, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Barei, D.P.; Nork, S.E.; Mills, W.J.; Coles, C.P.; Henley, M.B.; Benirschke, S.K. Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates. J. Bone Jt. Surg. 2006, 88, 1713–1721. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, P.S. Tibial condylar fractures. Impairment of knee joint stability as an indication for surgical treatment. J. Bone Jt. Surg. Am. 1973, 55, 1331–1350. [Google Scholar] [CrossRef]
- Duwelius, P.J.; Connolly, J.F. Closed reduction of tibial plateau fractures. A comparison of functional and roentgenographic end results. Clin. Orthop. Relat. Res. 1988, 230, 116–126. [Google Scholar] [CrossRef]
- Stevens, D.G.; Beharry, R.; McKee, M.D.; Waddell, J.P.; Schemitsch, E.H. The long-term functional outcome of operatively treated tibial plateau fractures. J. Orthop. Trauma 2001, 15, 312–320. [Google Scholar] [CrossRef]
- Lysholm, J.; Gillquist, J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am. J. Sports Med. 1982, 10, 150–154. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee injury and osteoarthritis outcome score (KOOS)—Development of a self-administered outcome measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Roos, E.M.; Lohmander, L.S. The Knee injury and osteoarthritis outcome score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [Green Version]
- Kraus, T.M.; Martetschläger, F.; Müller, D.; Braun, K.F.; Ahrens, P.; Siebenlist, S.; Stöckle, U.; Sandmann, G.H. Return to sports activity after tibial plateau fractures: 89 cases with minimum 24-month follow-up. Am. J. Sports Med. 2012, 40, 2845–2852. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Maso, G.; Gambato, M.; Belluzzi, E.; Pozzuoli, A.; Favero, M.; Vigo, M.; Ruggieri, P. Challenging surgical treatment of displaced articular tibial plateau fractures: Do early knee radiographic features have a predictive value of the mid-term clinical functional outcomes? Orthop. Surg. 2019, 11, 1149–1162. [Google Scholar] [CrossRef] [Green Version]
- Wasserstein, D.; Henry, P.; Paterson, J.M.; Kreder, H.J.; Jenkinson, R. Risk of total knee arthroplasty after operatively treated tibial plateau fracture: A matched-population-based cohort study. J. Bone Jt. Surg. 2014, 96, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Bott, A.; Odutola, A.; Halliday, R.; Acharya, M.R.; Ward, A.; Chesser, T.J.S. Long-term patient-reported functional outcome of polytraumatized patients with operatively treated pelvic fractures. J. Orthop. Trauma 2019, 33, 64–70. [Google Scholar] [CrossRef]
- Zelle, B.A.; Bhandari, M.; Sanchez, A.I.; Probst, C.; Pape, H.C. Loss of follow-up in orthopaedic trauma: Is 80% follow-up still acceptable? J. Orthop. Trauma 2013, 27, 177–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bäumlein, M.; Hanke, A.; Gueorguiev, B.; Nerlich, M.; Liodakis, E.; Perren, T.; Rillmann, P.; Ryf, C.; Loibl, M. Long-term outcome after surgical treatment of intra-articular tibial plateau fractures in skiers. Arch. Orthop. Trauma Surg. 2019, 139, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.; Tzioupis, C.; Papathanassopoulos, A.; Obakponovwe, O.; Roberts, C. Articular step-off and risk of post-traumatic osteoarthritis. Evidence today. Injury 2010, 41, 986–995. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic | Subcategory | Value (Range) | Mean Time to Theatre (SD, Range) (Days) | p Value |
|---|---|---|---|---|
| Age (years) Sex | 45.4 (21–78) | 0.388 | ||
| Male | 74 | 6.4 (5.0, 0–26) | 0.129 | |
| Female | 43 | 5.1 (3.5, 1–19) | ||
| Smoking status | Smoker | 25 | 7.1 (5.1, 1–26) | 0.114 |
| Nonsmoker | 92 | 5.6 (4.3, 0–24) | ||
| Diabetes status Schatzker type | Diabetic | 5 | 3.4 (1.9, 2–6) | 0.202 |
| Nondiabetic | 112 | 6.1 (4.6, 0–26) | ||
| I | 0 | 0.627 | ||
| II | 52 | 6.0 (4.7, 0–24) | ||
| III | 0 | |||
| IV | 4 | 3.8 (2.2, 1–6) | ||
| V | 0 | |||
| VI | 61 | 6.0 (4.6, 1–26) | ||
| Mechanism of injury | Low energy | 39 | 6.0 (5.1, 2–24) | 0.911 |
| High energy | 78 | 5.9 (4.3, 0–26) | ||
| Preoperative articular step (mm) | 8.1 (0.5–54) | 0.009 | ||
| Time to theatre (days) | 5.9 (0–26) |
| Demographic | Reduced | Unreduced | p Value | |
|---|---|---|---|---|
| Age (years) | 46.7 (21–78) | 43.9 (24–74) | 0.316 | |
| Sex | Male | 44 | 30 | 0.058 |
| Female | 33 | 10 | ||
| Smoking status | Smoker | 13 | 12 | 0.102 |
| Nonsmoker | 64 | 28 | ||
| Diabetic status | Diabetic | 4 | 1 | 0.498 |
| Nondiabetic | 73 | 39 | ||
| Schatzker type | II | 38 | 14 | 0.077 |
| IV | 4 | 0 | ||
| VI | 35 | 26 | ||
| Mechanism of injury | Low energy | 30 | 9 | 0.074 |
| High energy | 47 | 31 | ||
| Preoperative articular step (mm) | 7.57 (0.5–43) | 9.11 (1–54) | 0.344 | |
| Mean number of plates used for fixation | 1.56 (0–3) | 1.84 (0–5) | 0.166 | |
| Bone graft used | 48 | 24 | 0.848 |
| Exposure | Adjusted OR (95% CI) | p Value | |
|---|---|---|---|
| Time to theatre | Days | 0.83 (0.74, 0.93) | 0.002 |
| Age | 1.03 (0.99, 1.06) | 0.127 | |
| Sex | Male | 0.64 (0.21, 1.98) | 0.437 |
| Female | Reference | ||
| Smoking status | Smoker | 0.46 (0.16, 1.39) | 0.170 |
| Nonsmoker | Reference | ||
| Diabetes status | Diabetic | 0.64 (0.05, 7.64) | 0.722 |
| Nondiabetic | Reference | ||
| Schatzker type | II | Reference | 0.168 |
| IV | * | ||
| VI | 0.48 (0.17, 1.36) | ||
| Mechanism of injury | Low energy | Reference | 0.173 |
| High energy | 0.48 (0.16, 1.38) | ||
| Preoperative articular step | 0.98 (0.92, 1.04) | 0.468 | |
| Reduced | Unreduced | p Value | |
|---|---|---|---|
| 6-month Lysholm | 68.1 (30–100) | 62.8 (8–92) | 0.298 |
| 6-month KOOS pain | 75.0 (41–100) | 69.8 (21–94) | 0.230 |
| 6-month KOOS QOL | 48.9 (6–100) | 41.2 (6–94) | 0.151 |
| 1-year Lysholm | 70.3 (29–100) | 66.8 (23–100) | 0.438 |
| 1-year KOOS pain | 75.2 (39–100) | 76.1 (47–100) | 0.810 |
| 1-year KOOS QOL | 51.7 (0–100) | 52.3 (19–100) | 0.918 |
| Mid-term Lysholm | 73.0 (32–100) | 72.1 (34–99) | 0.875 |
| Mid-term KOOS pain | 81.6 (47–100) | 82.7 (42–100) | 0.801 |
| Mid-term KOOS QOL | 58.0 (6–100) | 62.8 (25–100) | 0.436 |
| Schatzker II | Schatzker VI | p Value | |
|---|---|---|---|
| 6-month Lysholm | 70.7 (8–100) | 60.7 (9–92) | 0.049 |
| 6-month KOOS pain | 74.1 (21–100) | 71.8 (34–97) | 0.600 |
| 6-month KOOS QOL | 51.1 (6–100) | 41.4 (6–94) | 0.067 |
| 1-year Lysholm | 70 (23–100) | 68.6 (29–100) | 0.745 |
| 1-year KOOS pain | 75.2 (42–100) | 75.4 (39–100) | 0.947 |
| 1-year KOOS QOL | 52.3 (19–100) | 50.2 (0–100) | 0.708 |
| Mid-term Lysholm | 72.6 (34–100) | 74.3 (32–99) | 0.734 |
| Mid-term KOOS pain | 84.5 (47–100) | 75.9 (56–100) | 0.105 |
| Mid-term KOOS QOL | 60.2 (6–100) | 51.0 (19–100) | 0.314 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitchen, D.S.; Richards, J.; Smitham, P.J.; Atkins, G.J.; Solomon, L.B. Does Time to Theatre Affect the Ability to Achieve Fracture Reduction in Tibial Plateau Fractures? J. Clin. Med. 2022, 11, 138. https://doi.org/10.3390/jcm11010138
Kitchen DS, Richards J, Smitham PJ, Atkins GJ, Solomon LB. Does Time to Theatre Affect the Ability to Achieve Fracture Reduction in Tibial Plateau Fractures? Journal of Clinical Medicine. 2022; 11(1):138. https://doi.org/10.3390/jcm11010138
Chicago/Turabian StyleKitchen, David Stuart, Jack Richards, Peter J. Smitham, Gerald J. Atkins, and Lucian B. Solomon. 2022. "Does Time to Theatre Affect the Ability to Achieve Fracture Reduction in Tibial Plateau Fractures?" Journal of Clinical Medicine 11, no. 1: 138. https://doi.org/10.3390/jcm11010138