
Caspase-Cleaved Keratin 18 Measurements Identified Ongoing Liver Injury after Bariatric Surgery

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgery
2.3. Data Acquisition
2.4. Quantification of Serum ccK18 Levels
2.5. Definition of Responders and Non-Responders to Bariatric Surgery
2.6. Proteome Profiling
2.7. Statistical Analysis
3. Results
3.1. Preoperative Assessment of the Study Population
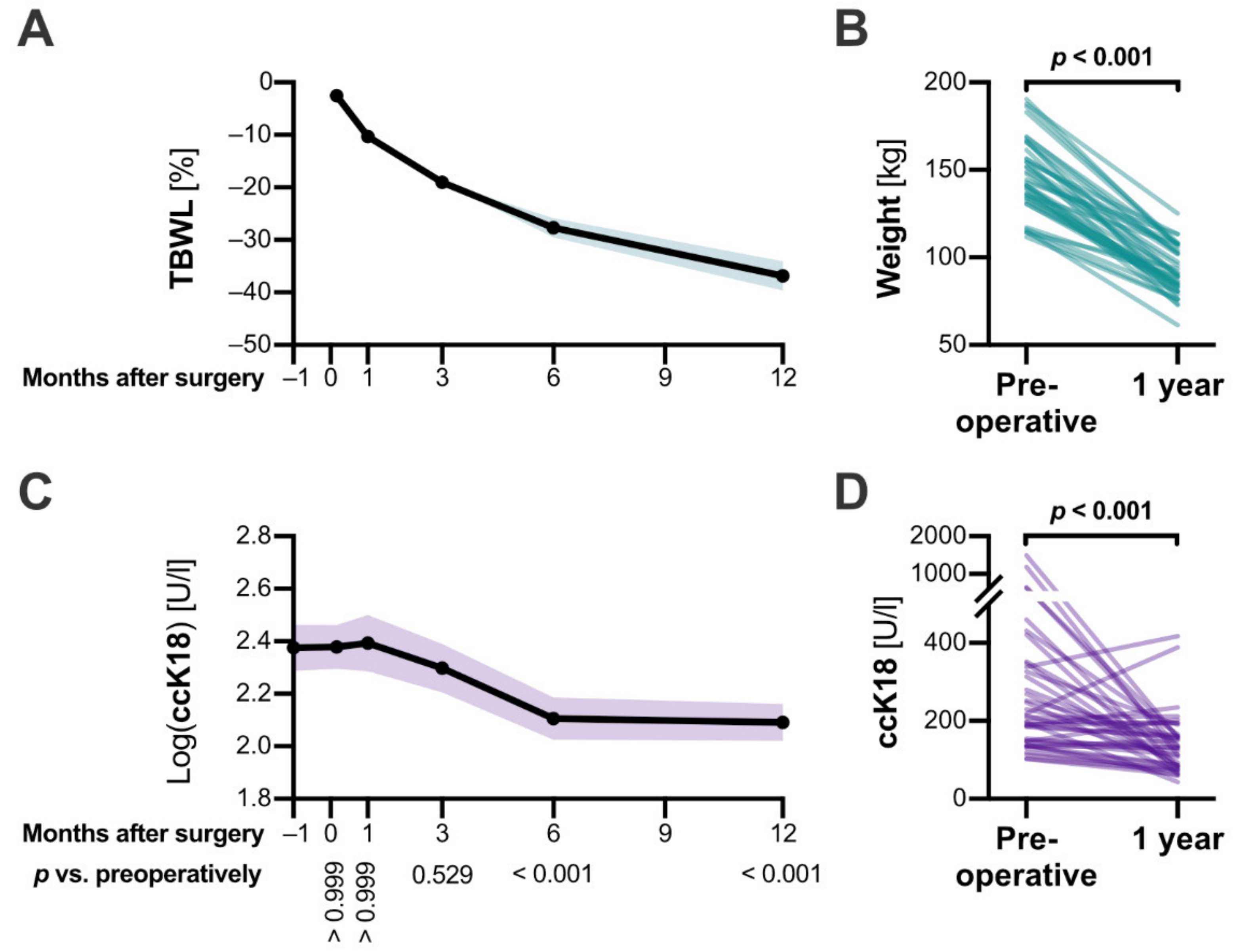
3.2. Roux-en-Y Gastric Bypass Induced Severe Weight Loss and Improved the Patient’s Metabolic State
3.3. ccK18 Levels Decreased within Six Months after Surgery
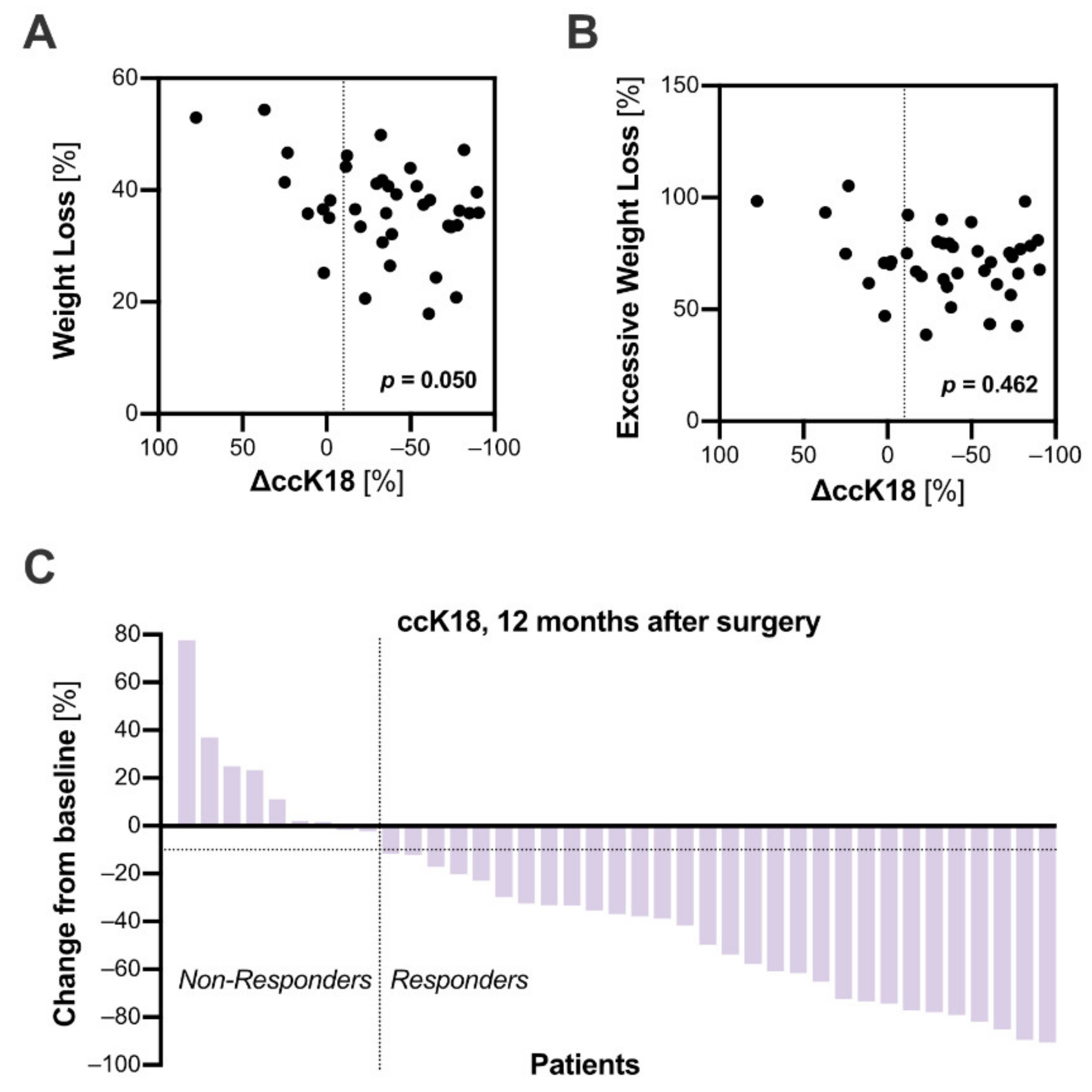
3.4. The Response to Bariatric Surgery Was Inconsistent among Patients
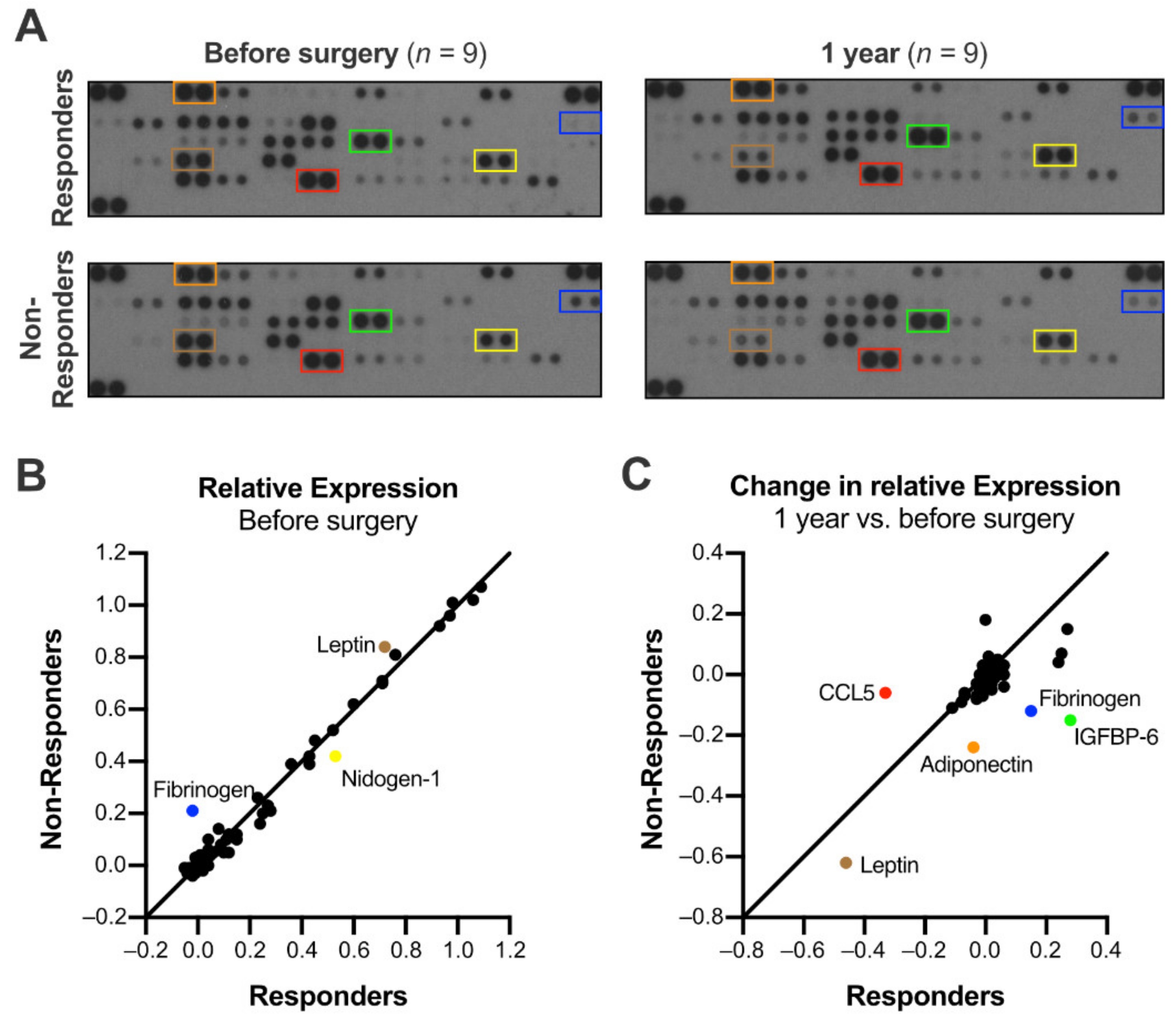
3.5. The Expression of Adipokines and Cytokines Distinguished Responders and Non-Responders
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Matteoni, C.A.; Younossi, Z.M.; Gramlich, T.; Boparai, N.; Liu, Y.C.; McCullough, A.J. Nonalcoholic fatty liver disease: A spectrum of clinical and pathological severity. Gastroenterology 1999, 116, 1413–1419. [Google Scholar] [CrossRef]
- Vernon, G.; Baranova, A.; Younossi, Z.M. Systematic review: The epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Tacke, F.; Arrese, M.; Chander Sharma, B.; Mostafa, I.; Bugianesi, E.; Wai-Sun Wong, V.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.M.; Marchesini, G.; Pinto-Cortez, H.; Petta, S. Epidemiology of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: Implications for Liver Transplantation. Transplantation 2019, 103, 22–27. [Google Scholar] [CrossRef]
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef]
- De Ridder, R.J.; Schoon, E.J.; Smulders, J.F.; van Hout, G.C.; Stockbrugger, R.W.; Koek, G.H. Review article: Non-alcoholic fatty liver disease in morbidly obese patients and the effect of bariatric surgery. Aliment. Pharmacol. Ther. 2007, 26, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Mummadi, R.R.; Kasturi, K.S.; Chennareddygari, S.; Sood, G.K. Effect of bariatric surgery on nonalcoholic fatty liver disease: Systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2008, 6, 1396–1402. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Doumouras, A.G.; Yu, J.; Brar, K.; Banfield, L.; Gmora, S.; Anvari, M.; Hong, D. Complete Resolution of Nonalcoholic Fatty Liver Disease After Bariatric Surgery: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2019, 17, 1040–1060. [Google Scholar] [CrossRef] [Green Version]
- Roeb, E.; Steffen, H.M.; Bantel, H.; Baumann, U.; Canbay, A.; Demir, M.; Drebber, U.; Geier, A.; Hampe, J.; Hellerbrand, C.; et al. S2k Guideline non-alcoholic fatty liver disease. Z. Gastroenterol. 2015, 53, 668–723. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver; European Association for the Study of Diabetes. Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Chitturi, S.; Wong, V.W.; Chan, W.K.; Wong, G.L.; Wong, S.K.; Sollano, J.; Ni, Y.H.; Liu, C.J.; Lin, Y.C.; Lesmana, L.A.; et al. The Asia-Pacific Working Party on Non-alcoholic Fatty Liver Disease guidelines 2017-Part 2: Management and special groups. J. Gastroenterol. Hepatol. 2018, 33, 86–98. [Google Scholar] [CrossRef] [Green Version]
- Kroh, M.; Liu, R.; Chand, B. Laparoscopic bariatric surgery: What else are we uncovering? Liver pathology and preoperative indicators of advanced liver disease in morbidly obese patients. Surg. Endosc. 2007, 21, 1957–1960. [Google Scholar] [CrossRef]
- Machado, M.; Marques-Vidal, P.; Cortez-Pinto, H. Hepatic histology in obese patients undergoing bariatric surgery. J. Hepatol. 2006, 45, 600–606. [Google Scholar] [CrossRef]
- Harnois, F.; Msika, S.; Sabate, J.M.; Mechler, C.; Jouet, P.; Barge, J.; Coffin, B. Prevalence and predictive factors of non-alcoholic steatohepatitis (NASH) in morbidly obese patients undergoing bariatric surgery. Obes. Surg. 2006, 16, 183–188. [Google Scholar] [CrossRef]
- Caulin, C.; Salvesen, G.S.; Oshima, R.G. Caspase cleavage of keratin 18 and reorganization of intermediate filaments during epithelial cell apoptosis. J. Cell Biol. 1997, 138, 1379–1394. [Google Scholar] [CrossRef]
- Bantel, H.; Ruck, P.; Gregor, M.; Schulze-Osthoff, K. Detection of elevated caspase activation and early apoptosis in liver diseases. Eur. J. Cell Biol. 2001, 80, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Bantel, H.; Lugering, A.; Heidemann, J.; Volkmann, X.; Poremba, C.; Strassburg, C.P.; Manns, M.P.; Schulze-Osthoff, K. Detection of apoptotic caspase activation in sera from patients with chronic HCV infection is associated with fibrotic liver injury. Hepatology 2004, 40, 1078–1087. [Google Scholar] [CrossRef]
- Kronenberger, B.; Wagner, M.; Herrmann, E.; Mihm, U.; Piiper, A.; Sarrazin, C.; Zeuzem, S. Apoptotic cytokeratin 18 neoepitopes in serum of patients with chronic hepatitis C. J. Viral. Hepat. 2005, 12, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, A.E.; Canbay, A.; Angulo, P.; Taniai, M.; Burgart, L.J.; Lindor, K.D.; Gores, G.J. Hepatocyte apoptosis and fas expression are prominent features of human nonalcoholic steatohepatitis. Gastroenterology 2003, 125, 437–443. [Google Scholar] [CrossRef]
- Wieckowska, A.; Zein, N.N.; Yerian, L.M.; Lopez, A.R.; McCullough, A.J.; Feldstein, A.E. In vivo assessment of liver cell apoptosis as a novel biomarker of disease severity in nonalcoholic fatty liver disease. Hepatology 2006, 44, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Jarrar, M.; Nugent, C.; Randhawa, M.; Afendy, M.; Stepanova, M.; Rafiq, N.; Goodman, Z.; Chandhoke, V.; Baranova, A. A novel diagnostic biomarker panel for obesity-related nonalcoholic steatohepatitis (NASH). Obes. Surg. 2008, 18, 1430–1437. [Google Scholar] [CrossRef]
- Diab, D.L.; Yerian, L.; Schauer, P.; Kashyap, S.R.; Lopez, R.; Hazen, S.L.; Feldstein, A.E. Cytokeratin 18 fragment levels as a noninvasive biomarker for nonalcoholic steatohepatitis in bariatric surgery patients. Clin. Gastroenterol. Hepatol. 2008, 6, 1249–1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldstein, A.E.; Wieckowska, A.; Lopez, A.R.; Liu, Y.C.; Zein, N.N.; McCullough, A.J. Cytokeratin-18 fragment levels as noninvasive biomarkers for nonalcoholic steatohepatitis: A multicenter validation study. Hepatology 2009, 50, 1072–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liebig, S.; Stoeckmann, N.; Geier, A.; Rau, M.; Schattenberg, J.M.; Bahr, M.J.; Manns, M.P.; Jaeckel, E.; Schulze-Osthoff, K.; Bantel, H. Multicenter Validation Study of a Diagnostic Algorithm to Detect NASH and Fibrosis in NAFLD Patients With Low NAFLD Fibrosis Score or Liver Stiffness. Clin. Transl. Gastroenterol. 2019, 10, e00066. [Google Scholar] [CrossRef]
- Bantel, H.; John, K.; Schulze-Osthoff, K. Robust detection of liver steatosis and staging of NAFLD by an improved ELISA for serum cytokeratin-18 fragments. Am. J. Gastroenterol. 2014, 109, 140–141. [Google Scholar] [CrossRef]
- Joka, D.; Wahl, K.; Moeller, S.; Schlue, J.; Vaske, B.; Bahr, M.J.; Manns, M.P.; Schulze-Osthoff, K.; Bantel, H. Prospective biopsy-controlled evaluation of cell death biomarkers for prediction of liver fibrosis and nonalcoholic steatohepatitis. Hepatology 2012, 55, 455–464. [Google Scholar] [CrossRef]
- Kwok, R.; Tse, Y.K.; Wong, G.L.; Ha, Y.; Lee, A.U.; Ngu, M.C.; Chan, H.L.; Wong, V.W. Systematic review with meta-analysis: Non-invasive assessment of non-alcoholic fatty liver disease--the role of transient elastography and plasma cytokeratin-18 fragments. Aliment. Pharmacol. Ther. 2014, 39, 254–269. [Google Scholar] [CrossRef]
- Musso, G.; Gambino, R.; Cassader, M.; Pagano, G. Meta-analysis: Natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasive tests for liver disease severity. Ann. Med. 2011, 43, 617–649. [Google Scholar] [CrossRef]
- Safarian, M.; Mohammadpour, S.; Shafiee, M.; Ganji, A.; Soleimani, A.; Nematy, M.; Bahari, A. Effect of diet-induced weight loss on cytokeratin-18 levels in overweight and obese patients with liver fibrosis. Diabetes Metab. Syndr. 2019, 13, 989–994. [Google Scholar] [CrossRef]
- Vuppalanchi, R.; Jain, A.K.; Deppe, R.; Yates, K.; Comerford, M.; Masuoka, H.C.; Neuschwander-Tetri, B.A.; Loomba, R.; Brunt, E.M.; Kleiner, D.E.; et al. Relationship between changes in serum levels of keratin 18 and changes in liver histology in children and adults with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2014, 12, 2121–2130. [Google Scholar] [CrossRef] [Green Version]
- Tsutsui, M.; Tanaka, N.; Kawakubo, M.; Sheena, Y.; Horiuchi, A.; Komatsu, M.; Nagaya, T.; Joshita, S.; Umemura, T.; Ichijo, T.; et al. Serum fragmented cytokeratin 18 levels reflect the histologic activity score of nonalcoholic fatty liver disease more accurately than serum alanine aminotransferase levels. J. Clin. Gastroenterol. 2010, 44, 440–447. [Google Scholar] [CrossRef]
- Hempel, F.; Roderfeld, M.; Savai, R.; Sydykov, A.; Irungbam, K.; Schermuly, R.; Voswinckel, R.; Kohler, K.; Churin, Y.; Kiss, L.; et al. Depletion of Bone Marrow-Derived Fibrocytes Attenuates TAA-Induced Liver Fibrosis in Mice. Cells 2019, 8, 1210. [Google Scholar] [CrossRef] [Green Version]
- Lin, Z.H.; Xin, Y.N.; Dong, Q.J.; Wang, Q.; Jiang, X.J.; Zhan, S.H.; Sun, Y.; Xuan, S.Y. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology 2011, 53, 726–736. [Google Scholar] [CrossRef] [PubMed]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Deng, L.; Zhang, Q.; Guo, J.; Zhou, J.; Song, W.; Yuan, F. Diagnostic Value of CK-18, FGF-21, and Related Biomarker Panel in Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2017, 2017, e9729107. [Google Scholar] [CrossRef]
- Cusi, K.; Chang, Z.; Harrison, S.; Lomonaco, R.; Bril, F.; Orsak, B.; Ortiz-Lopez, C.; Hecht, J.; Feldstein, A.E.; Webb, A.; et al. Limited value of plasma cytokeratin-18 as a biomarker for NASH and fibrosis in patients with non-alcoholic fatty liver disease. J. Hepatol. 2014, 60, 167–174. [Google Scholar] [CrossRef]
- Wong, V.W.; Adams, L.A.; de Ledinghen, V.; Wong, G.L.; Sookoian, S. Noninvasive biomarkers in NAFLD and NASH—Current progress and future promise. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 461–478. [Google Scholar] [CrossRef]
- Schwenger, K.J.P.; Fischer, S.E.; Jackson, T.; Okrainec, A.; Allard, J.P. In nonalcoholic fatty liver disease, Roux-en-Y gastric bypass improves liver histology while persistent disease is associated with lower improvements in waist circumference and glycemic control. Surg. Obes. Relat. Dis. 2018, 14, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Mathurin, P.; Gonzalez, F.; Kerdraon, O.; Leteurtre, E.; Arnalsteen, L.; Hollebecque, A.; Louvet, A.; Dharancy, S.; Cocq, P.; Jany, T.; et al. The evolution of severe steatosis after bariatric surgery is related to insulin resistance. Gastroenterology 2006, 130, 1617–1624. [Google Scholar] [CrossRef] [PubMed]
- Mathurin, P.; Hollebecque, A.; Arnalsteen, L.; Buob, D.; Leteurtre, E.; Caiazzo, R.; Pigeyre, M.; Verkindt, H.; Dharancy, S.; Louvet, A.; et al. Prospective study of the long-term effects of bariatric surgery on liver injury in patients without advanced disease. Gastroenterology 2009, 137, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Tuovila, M.; Erkinaro, T.; Koivukangas, V.; Savolainen, E.R.; Laurila, P.; Ohtonen, P.; Ala-Kokko, T. Thromboelastography Values Remain Hypercoagulative 6 Months After Obesity Surgery: A Pilot Study. Obes. Surg. 2018, 28, 3943–3949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyzos, S.A.; Aronis, K.N.; Kountouras, J.; Raptis, D.D.; Vasiloglou, M.F.; Mantzoros, C.S. Circulating leptin in non-alcoholic fatty liver disease: A systematic review and meta-analysis. Diabetologia 2016, 59, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Jarrar, M.H.; Baranova, A.; Collantes, R.; Ranard, B.; Stepanova, M.; Bennett, C.; Fang, Y.; Elariny, H.; Goodman, Z.; Chandhoke, V.; et al. Adipokines and cytokines in non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2008, 27, 412–421. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Toulis, K.A.; Goulis, D.G.; Zavos, C.; Kountouras, J. Serum total adiponectin in nonalcoholic fatty liver disease: A systematic review and meta-analysis. Metabolism 2011, 60, 313–326. [Google Scholar] [CrossRef]
- Balmer, M.L.; Joneli, J.; Schoepfer, A.; Stickel, F.; Thormann, W.; Dufour, J.F. Significance of serum adiponectin levels in patients with chronic liver disease. Clin. Sci. 2010, 119, 431–436. [Google Scholar] [CrossRef] [Green Version]
- Boutari, C.; Mantzoros, C.S. Adiponectin and leptin in the diagnosis and therapy of NAFLD. Metabolism 2020, 103, e154028. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Preoperative (n = 39) | 1 Year (n = 39) | p (Adjusted) | |
|---|---|---|---|
| Demographic | |||
| Age (year) | 39.44 (23 to 60) | ||
| Female sex | 35 (90%) | ||
| Anthropometric | |||
| BMI (kg/m2) | 51.94 (41.56 to 61.85) | 32.64 (17.88 to 54.37) | <0.001 |
| Body weight (kg) | 146.54 (111.7 to 190.5) | 91.84 (61.3 to 125) | <0.001 |
| Total Body Weight Loss (%) | 36.87 (17.88 to 54.37) | ||
| Excess Weight Loss † (%) | 71.89 (38.64 to 105.29) | ||
| Metabolism | |||
| HbA1c (%) | 6.19 (4.7 to 9.6) | 5.29 (4.5 to 6.7) | <0.001 |
| Diabetes mellitus | 10 (31%) | 2 (5%) | |
| LDL cholesterol (mg/dl) | 129.65 (53 to 233) | 91.92 (20 to 153) | <0.001 |
| HDL cholesterol (mg/dl) | 46.32 (27 to 87) | 50.79 (17 to 95) | 0.021 |
| Serum triglycerides (mg/dl) | 173.12 (58 to 751) | 88.1 (44 to 253) | <0.001 |
| CRP (mg/l) | 17.72 (2.09 to 146.61) | 1.87 (0.5 to 14.6) | 0.004 |
| Liver-related | |||
| Log ccK18 (U/l) | 2.37 (2.01 to 3.17) | 2.09 (1.64 to 2.62) | <0.001 |
| ccK18 > 200 U/l | 20 (51%) | 5 (13%) | |
| ALT (U/l) | 41.03 (11 to 126) | 36.15 (10 to 186) | 0.914 |
| AST (U/l) | 31.15 (10 to 136) | 23.44 (8 to 137) | 0.285 |
| Alkaline Phosphatase (U/l) | 77.44 (48 to 114) | 82.74 (43 to 270) | 0.836 |
| GGT (U/l) | 41 (9 to 162) | 23.26 (6 to 279) | 0.280 |
| Bilirubin (mg/dl) | 0.49 (0.3 to 1) | 0.58 (0.2 to 1.5) | 0.024 |
| Albumine (g/dl) | 4.29 (3.61 to 5.1) | 4.41 (3.92 to 5) | 0.213 |
| Significant fibrosis? | |||
| NFS | −0.24 (−3.01 to 2.78) | −2.36 (−5.44 to 0.4) | <0.001 |
| NFS > 0.676 | 8 (21%) | 0 | |
| APRI | 0.29 (0.06 to 0.99) | 0.24 (0.05 to 1.25) | 0.576 |
| APRI > 0.7 | 2 (5%) | 1 (3%) | |
| FIB-4 | 0.71 (0.23 to 1.67) | 0.63 (0.21 to 1.51) | 0.311 |
| FIB-4 > 3.25 | 0 | 0 |
| Preoperative | 1 Year | |||||
|---|---|---|---|---|---|---|
| Responders (n = 30) | Non-Responders (n = 9) | p (Adjusted) | Responders (n = 30) | Non-Responders (n = 9) | p (Adjusted) | |
| Demographic | ||||||
| Age (year) | 39.1 (23 to 60) | 40.56 (27 to 51) | >0.999 | |||
| Female sex | 27 (90%) | 8 (89%) | ||||
| Anthropometric | ||||||
| BMI (kg/m2) | 51.4 (41.56 to 61.85) | 53.72 (44.92 to 59.88) | >0.999 | 32.89 (25.4 to 42.52) | 31.81 (23.95 to 40.15) | >0.999 |
| Body weight (kg) | 145.51 (111.7 to 190.5) | 149.98 (115 to 183) | >0.999 | 92.79 (73.4 to 125) | 88.68 (61.3 to 108) | >0.999 |
| Metabolism | ||||||
| Diabetes mellitus | 8 (33%) | 2 (25%) | 1 (3%) | 1 (11%) | ||
| LDL cholesterol (mg/dl) | 128.15 (53 to 233) | 134.5 (90 to 165) | >0.999 | 90.63 (20 to 145) | 96.22 (65 to 153) | >0.999 |
| HDL cholesterol (mg/dl) | 44.5 (27 to 71) | 52.25 (31 to 87) | >0.999 | 49.3 (17 to 83) | 55.78 (38 to 95) | >0.999 |
| Serum triglycerides (mg/dl) | 183.08 (58 to 751) | 140.75 (98 to 189) | 0.036 | 90.53 (44 to 253) | 80 (44 to 120) | 0.962 |
| CRP (mg/l) | 15.25 (2.09 to 146.61) | 25.94 (8.12 to 110.89) | >0.999 | 1.26 (0.5 to 7.91) | 3.9 (0.5 to 14.6) | >0.999 |
| Liver-related | ||||||
| Log ccK18 (U/l) | 2.4 (2.01 to 3.17) | 2.27 (2.13 to 2.53) | >0.999 | 2.02 (1.64 to 2.28) | 2.34 (2.21 to 2.62) | >0.999 |
| ccK18 > 200 U/l | 17 (57%) | 3 (33%) | 0 | 5 (56%) | ||
| ALT (U/l) | 45.5 (11 to 126) | 26.11 (13 to 43) | 0.921 | 34.47 (10 to 186) | 41.78 (10 to 102) | >0.999 |
| AST (U/l) | 34.13 (10 to 136) | 21.22 (12 to 30) | >0.999 | 22.87 (8 to 137) | 25.33 (12 to 42) | >0.999 |
| Alkaline Phosphatase (U/l) | 76.87 (48 to 114) | 79.33 (50 to 114) | >0.999 | 78.27 (43 to 122) | 97.67 (60 to 270) | 0.194 |
| GGT (U/l) | 45.33 (9 to 162) | 26.56 (11 to 56) | 0.939 | 13.03 (6 to 40) | 57.33 (10 to 279) | < 0.001 |
| Bilirubin (mg/dl) | 0.49 (0.3 to 1) | 0.5 (0.3 to 0.7) | >0.999 | 0.59 (0.2 to 1.5) | 0.54 (0.3 to 0.9) | >0.999 |
| Albumine (g/dl) | 4.35 (3.8 to 5.1) | 4.09 (3.6 to 4.6) | >0.999 | 4.47 (4.03 to 5) | 4.24 (3.92 to 4.5) | >0.999 |
| Significant fibrosis? | ||||||
| NFS | −0.27 | −0.164 | >0.999 | −2.21 (−4.68 to 0.4) | −2.87 (−5.44 to −0.44) | >0.999 |
| NFS > 0.676 | 6 (20%) | 2 (22%) | 0 | 0 | ||
| APRI | 0.318 | 0.187 | >0.999 | 0.24 (0.05 to 1.25) | 0.23 (0.09 to 0.48) | >0.999 |
| APRI > 0.7 | 2 (7%) | 0 | 1 (3%) | 0 | ||
| FIB-4 | 0.74 | 0.594 | >0.999 | 0.64 (0.21 to 1.51) | 0.59 (0.36 to 1.33) | >0.999 |
| FIB-4 > 3.25 | 0 | 0 | 0 | 0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hempel, F.; Roderfeld, M.; Müntnich, L.J.; Albrecht, J.; Oruc, Z.; Arneth, B.; Karrasch, T.; Pons-Kühnemann, J.; Padberg, W.; Renz, H.; et al. Caspase-Cleaved Keratin 18 Measurements Identified Ongoing Liver Injury after Bariatric Surgery. J. Clin. Med. 2021, 10, 1233. https://doi.org/10.3390/jcm10061233
Hempel F, Roderfeld M, Müntnich LJ, Albrecht J, Oruc Z, Arneth B, Karrasch T, Pons-Kühnemann J, Padberg W, Renz H, et al. Caspase-Cleaved Keratin 18 Measurements Identified Ongoing Liver Injury after Bariatric Surgery. Journal of Clinical Medicine. 2021; 10(6):1233. https://doi.org/10.3390/jcm10061233
Chicago/Turabian StyleHempel, Felix, Martin Roderfeld, Lucas John Müntnich, Jens Albrecht, Ziya Oruc, Borros Arneth, Thomas Karrasch, Jörn Pons-Kühnemann, Winfried Padberg, Harald Renz, and et al. 2021. "Caspase-Cleaved Keratin 18 Measurements Identified Ongoing Liver Injury after Bariatric Surgery" Journal of Clinical Medicine 10, no. 6: 1233. https://doi.org/10.3390/jcm10061233