
Long-Term Patient-Related Quality of Life after Knee Periprosthetic Joint Infection

 ,
,
Abstract
:1. Introduction
2. Experimental Section
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rupp, M.; Lau, E.; Kurtz, S.M.; Alt, V. Projections of Primary TKA and THA in Germany from 2016 through 2040. Clin. Orthop. Relat. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kamath, A.F.; Ong, K.L.; Lau, E.; Chan, V.; Vail, T.P.; Rubash, H.E.; Berry, D.J.; Bozic, K.J. Quantifying the Burden of Revision Total Joint Arthroplasty for Periprosthetic Infection. J. Arthroplast. 2015, 30, 1492–1497. [Google Scholar] [CrossRef] [PubMed]
- Mallon, C.; Gooberman-Hill, R.; Blom, A.; Whitehouse, M.; Moore, A. Surgeons are deeply affected when patients are diagnosed with prosthetic joint infection. PLoS ONE 2018, 13, e0207260. [Google Scholar] [CrossRef]
- Alt, V.; Rupp, M.; Langer, M.; Baumann, F.; Trampuz, A. Can the oncology classification system be used for prosthetic joint infection: The PJI-TNM system. Bone Jt. Res. 2020, 9, 79–81. [Google Scholar] [CrossRef]
- Pellegrini, A.; Legnani, C.; Meani, E. A new perspective on current prosthetic joint infection classifications: Introducing topography as a key factor affecting treatment strategy. Arch. Orthop. Trauma Surg. 2019, 139, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-joint infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [Green Version]
- Wimmer, M.D.; Randau, T.M.; Petersdorf, S.; Pagenstert, G.I.; Weißkopf, M.; Wirtz, D.C.; Gravius, S. Evaluation of an interdisciplinary therapy algorithm in patients with prosthetic joint infections. Int. Orthop. 2013, 37, 2271–2278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, M.M.; Tan, T.L.; Manrique, J.; Deirmengian, G.K.; Parvizi, J. The Fate of Spacers in the Treatment of Periprosthetic Joint Infection. J. Bone Jt. Surg. Am. 2015, 97, 1495–1502. [Google Scholar] [CrossRef] [Green Version]
- Sousa, R.; Abreu, M.A. Treatment of Prosthetic Joint Infection with Debridement, Antibiotics and Irrigation with Implant Retention—A Narrative Review. J. Bone Jt. Infect. 2018, 3, 108–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pangaud, C.; Ollivier, M.; Argenson, J.N. Outcome of single-stage versus two-stage exchange for revision knee arthroplasty for chronic periprosthetic infection. EFORT Open Rev. 2019, 4, 495–502. [Google Scholar] [CrossRef]
- Tritt, K.; Von Heymann, F.; Zaudig, M.; Zacharias, I.; Söllner, W.; Loew, T. Development of the “ICD-10-Symptom-Rating”(ISR) questionnaire. Z. Psychosom. Med. Psychother. 2018, 54, 409–418. [Google Scholar] [CrossRef]
- Brooks, R. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]
- Claes, C.; Greiner, W.; Uber, A.; Graf von der Schulenburg, J.M. An interview-based comparison of the TTO and VAS values given to EuroQol states of health by the general German population. In EuroQol Plenary Meeting, 1–2 October 1998; Discussion papers; Greiner, W., Graf v.d. Schulenburg, J.-M., Piercy, J., Eds.; Centre for Health Economics and Health Systems Research, University of Hannover: Hannover, Germany, 1999; pp. 13–39. [Google Scholar]
- Bullinger, M.; Kirchberger, I.; Ware, J. The German SF-36 health survey translation and psychometric testing of a generic instrument for the assessment of health-related quality of life. J. Public Health 1995, 3, 21–36. [Google Scholar] [CrossRef]
- Ellert, U.; Kurth, B.M. Methodological views on the SF-36 summary scores based on the adult German population. Bundesgesundheitsblatt. Gesundheitsforschung. Gesundheitsschutz. 2004, 47, 1027–1032. [Google Scholar] [CrossRef]
- Szende, A.; Janssen, B.; Cabases, J. Self-Reported Population Health: An International Perspective Based on EQ-5D; Springer: Dordrecht, The Netherlands, 2014; pp. 20–22. [Google Scholar]
- Boonen, B.; Schotanus, M.G.M.; Kerens, B.; Van der Weegen, W.; Hoekstra, H.J.; Kort, N.P. No difference in clinical outcome between patient-matched positioning guides and conventional instrumented total knee arthroplasty two years post-operatively: A multicentre, double-blind, randomised controlled trial. Bone Jt. J. 2016, 98, 939–944. [Google Scholar] [CrossRef] [PubMed]
- Konopka, J.F.; Lee, Y.Y.; Su, E.P.; McLawhorn, A.S. Quality-Adjusted Life Years after Hip and Knee Arthroplasty: Health-Related Quality of Life after 12,782 Joint Replacements. JB JS Open Access 2018, 3, e0007. [Google Scholar] [CrossRef]
- Aboltins, C.; Dowsey, M.; Peel, T.; Lim, W.K.; Choong, P. Good quality of life outcomes after treatment of prosthetic joint infection with debridement and prosthesis retention. J. Orthop. Res. 2016, 34, 898–902. [Google Scholar] [CrossRef] [Green Version]
- Röhner, E.; Windisch, C.; Nuetzmann, K.; Rau, M.; Arnhold, M.; Matziolis, G. Unsatisfactory outcome of arthrodesis performed after septic failure of revision total knee arthroplasty. J. Bone Jt. Surg. Am. 2015, 97, 298–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orfanos, A.V.; Michael, R.J.; Keeney, B.J.; Moschetti, W.E. Patient-reported outcomes after above-knee amputation for prosthetic joint infection. Knee 2020, 27, 1101–1105. [Google Scholar] [CrossRef]
- Winkler, T.; Stuhlert, M.G.W.; Lieb, E.; Müller, M.; von Roth, P.; Preininger, B.; Trampuz, A.; Perka, C.F. Outcome of short versus long interval in two-stage exchange for periprosthetic joint infection: A prospective cohort study. Arch. Orthop. Trauma Surg. 2019, 139, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Hungerer, S.; Kiechle, M.; von Rüden, C.; Militz, M.; Beitzel, K.; Morgenstern, M. Knee arthrodesis versus above-the-knee amputation after septic failure of revision total knee arthroplasty: Comparison of functional outcome and complication rates. BMC Musculoskelet. Disord. 2017, 18, 443. [Google Scholar] [CrossRef] [PubMed]
- Preobrazhensky, P.M.; Bozhkova, S.A.; Kazemirsky, A.V.; Tikhilov, R.M.; Kulaba, T.A.; Kornilov, N.N. Functional outcome of two-stage reimplantation in patients with periprosthetic joint infection after primary total knee arthroplasty. Int. Orthop. 2019, 43, 2503–2509. [Google Scholar] [CrossRef]
- Cahill, J.L.; Shadbolt, B.; Scarvell, J.M.; Smith, P.N. Quality of life after infection in total joint replacement. J. Orthop. Surg. 2008, 16, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Helwig, P.; Morlock, J.; Oberst, M.; Hauschild, O.; Hübner, J.; Borde, J.; Südkamp, N.P.; Konstantinidis, L. Periprosthetic joint infection—Effect on quality of life. Int. Orthop. 2014, 38, 1077–1081. [Google Scholar] [CrossRef] [Green Version]
- Lum, Z.C.; Natsuhara, K.M.; Shelton, T.J.; Giordani, M.; Pereira, G.C.; Meehan, J.P. Mortality During Total Knee Periprosthetic Joint Infection. J. Arthroplast. 2018, 33, 3783–3788. [Google Scholar] [CrossRef]
- Moore, A.J.; Blom, A.W.; Whitehouse, M.R.; Gooberman-Hill, R. Deep prosthetic joint infection: A qualitative study of the impact on patients and their experiences of revision surgery. BMJ Open 2015, 5, e009495. [Google Scholar] [CrossRef] [Green Version]
- Knebel, C.; Menzemer, J.; Pohlig, F.; Herschbach, P.; Burgkart, R.; Obermeier, A.; von Eisenhart-Rothe, R.; Mühlhofer, H.M.L. Peri-Prosthetic Joint Infection of the Knee Causes High Levels of Psychosocial Distress: A Prospective Cohort Study. Surg. Infect. 2020, 21, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Beswick, A.D.; Peters, T.J.; Gooberman-Hill, R.; Whitehouse, M.R.; Blom, A.W.; Moore, A.J. Health Care Needs and Support for Patients Undergoing Treatment for Prosthetic Joint Infection following Hip or Knee Arthroplasty: A Systematic Review. PLoS ONE 2017, 12, e0169068. [Google Scholar] [CrossRef] [Green Version]
- Browne, J.A.; Sandberg, B.F.; D’Apuzzo, M.R.; Novicoff, W.M. Depression is associated with early postoperative outcomes following total joint arthroplasty: A nationwide database study. J. Arthroplast. 2014, 29, 481–483. [Google Scholar] [CrossRef] [PubMed]
- Rasouli, M.R.; Menendez, M.E.; Sayadipour, A.; Purtill, J.J.; Parvizi, J. Direct Cost and Complications Associated With Total Joint Arthroplasty in Patients With Preoperative Anxiety and Depression. J. Arthroplast. 2016, 31, 533–536. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | n = 36 |
|---|---|
| Gender | |
| Male | n = 19 (52.8%) |
| female | n = 17 (47.2%) |
| Age | 71.6 (10.7) years |
| BMI | 32.8 (8.3) kg/m2 |
| Smoking | |
| No | n = 15 (41.7%) |
| Currently | n = 4 (11.1%) |
| Formerly | n = 17 (47.2%) |
| Follow-up time | 4.9 (3.5) years |
| Revision rate | 2.9 (1.9) |
| Surgical procedure | |
| DAIR | n = 16 (44.4%) |
| One-stage exchange | n = 3 (8.3%) |
| Two-stage exchange | n = 8 (22.2%) |
| Arthrodesis | n = 9 (25.0%) |
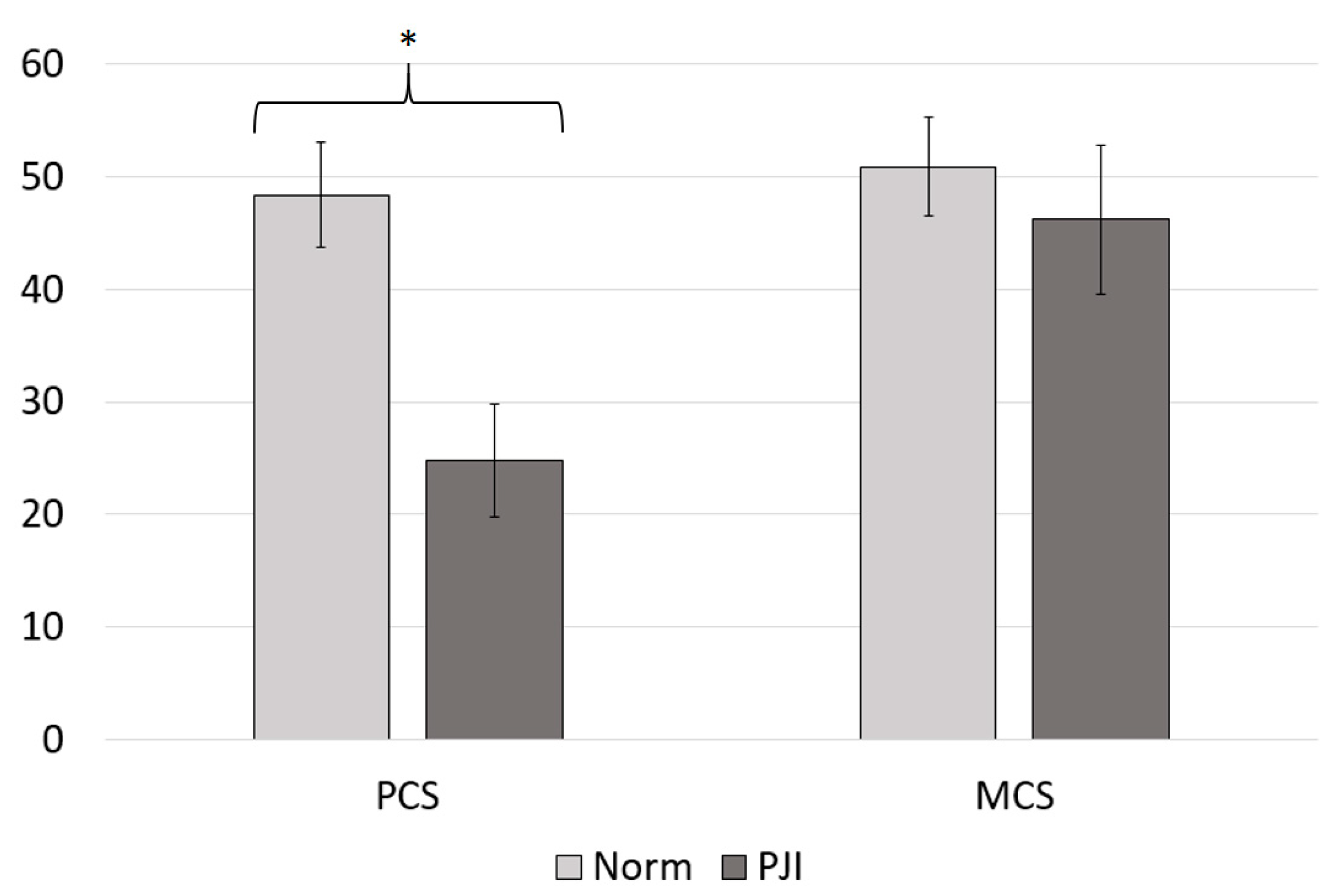
| SF-36 Outcomes | All Patients (n = 36) | Normative Data | Independent t-Test |
|---|---|---|---|
| Physical health component (PCS) | 24.82 (10.0) | 48.36 (9.4) | p < 0.001 |
| Mental health component (MCS) | 46.16 (13.3) | 50.87 (8.8) | p = 0.003 |
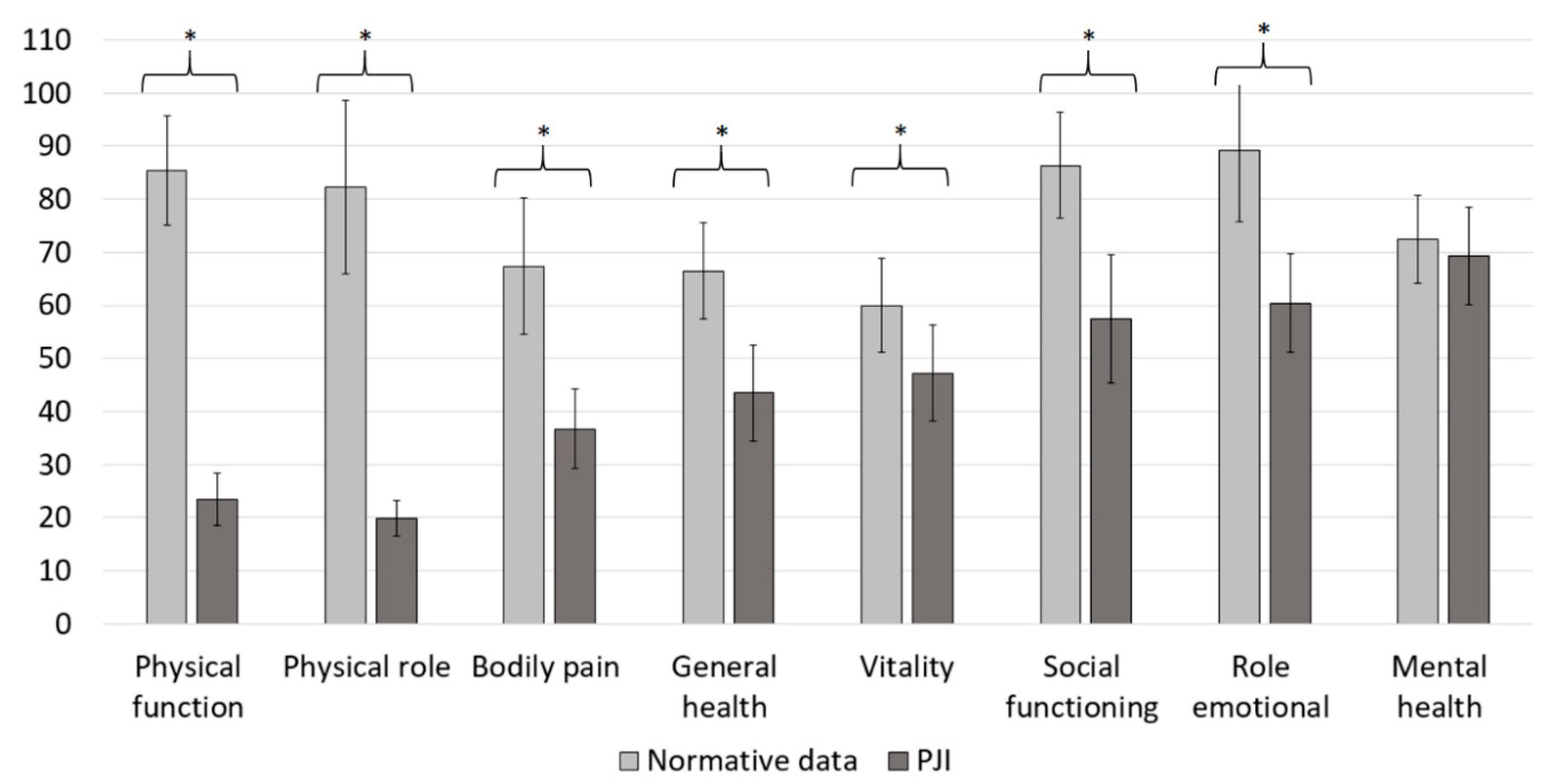
| Physical function | 23.4 (9.6) | 85.4 (20.7) | p < 0.001 |
| Physical role | 19.9 (6.7) | 82.36 (32.7) | p < 0.001 |
| Bodily pain | 36.7 (15.0) | 67.38 (25.9) | p < 0.001 |
| General health | 43.5 (18.3) | 66.42 (18.2) | p < 0.001 |
| Vitality | 47.2 (18.0 | 60.02 (17.8) | p < 0.001 |
| Social functioning | 57.5 (24.1) | 86.36 (19.9) | p < 0.001 |
| Emotional role | 60.4 (18.5) | 89.11 (26.7) | p < 0.001 |
| Mental health | 69.3 (18.5) | 72.46 (16.7) | p = 0.003 |
| SF-36 Outcomes | Patients Treated with Arthrodesis (n = 9) |
|---|---|
| Physical health component (PCS) | 23.0 (8.1) |
| Mental health component (MCS) | 42.6 (23.1 |
| Physical function | 18.3 (7.3) |
| Physical role | 5.6 (0.9 |
| Bodily pain | 35.1 (17.1) |
| General health | 42.0 (17.1) |
| Vitality | 43.3 (23.2) |
| Social functioning | 51.4 (28.4) |
| Emotional role | 45.8 (16.3 |
| Mental health | 66.4 (22.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walter, N.; Rupp, M.; Hierl, K.; Koch, M.; Kerschbaum, M.; Worlicek, M.; Alt, V. Long-Term Patient-Related Quality of Life after Knee Periprosthetic Joint Infection. J. Clin. Med. 2021, 10, 907. https://doi.org/10.3390/jcm10050907
Walter N, Rupp M, Hierl K, Koch M, Kerschbaum M, Worlicek M, Alt V. Long-Term Patient-Related Quality of Life after Knee Periprosthetic Joint Infection. Journal of Clinical Medicine. 2021; 10(5):907. https://doi.org/10.3390/jcm10050907
Chicago/Turabian StyleWalter, Nike, Markus Rupp, Katja Hierl, Matthias Koch, Maximilian Kerschbaum, Michael Worlicek, and Volker Alt. 2021. "Long-Term Patient-Related Quality of Life after Knee Periprosthetic Joint Infection" Journal of Clinical Medicine 10, no. 5: 907. https://doi.org/10.3390/jcm10050907