
Improvement of Arterial Stiffness One Month after Bariatric Surgery and Potential Mechanisms

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methods
2.1.1. Study Design and Patients
2.1.2. Procedures
Mobil-O-Graph® Device and Measurements
Renin-Angiotensin-Aldosterone System (RAAS) Components
Adipokines and Inflammatory Parameters
Surgical Techniques
2.1.3. Statistical Analyses
3. Results
3.1. Changes in Anthropometric and Hemodynamic Parameters
3.2. Changes in Glucose Metabolism, RAAS Components, Adipokines and Inflammatory Markers
3.3. Correlations
3.3.1. Correlations of Changes in Arterial Stiffness (AS) with Changes in Anthropometric Parameters, Glucose Metabolism, Adipokines and Inflammatory Markers
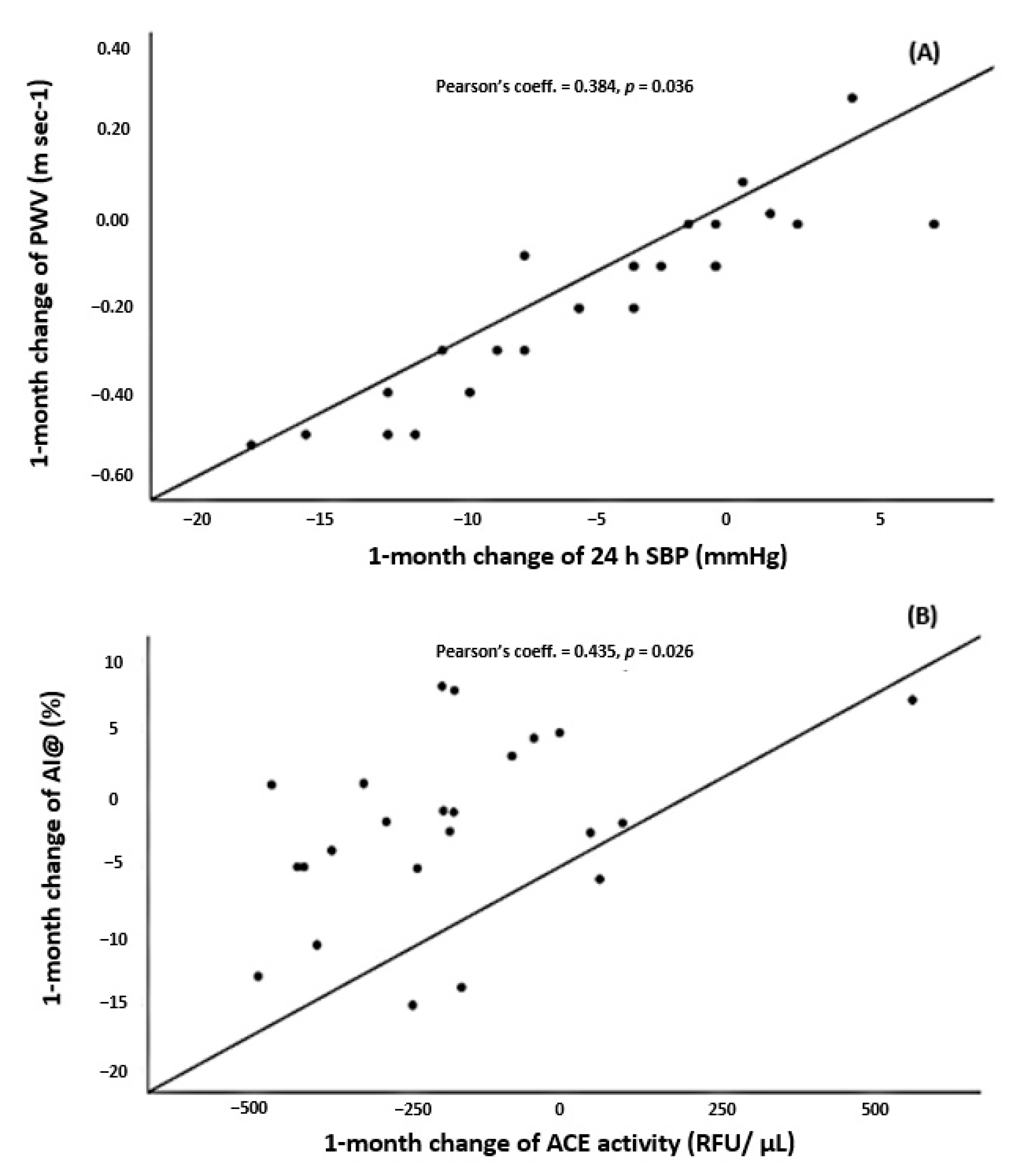
3.3.2. Correlations of Changes in AS with Changes in BP Estimates
3.3.3. Correlations of Changes in AS with Changes in the RAAS Components
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
A.1. Angiotensin-Converting Enzyme (ACE2) Enzymatic Assay
A.2. ACE Enzymatic Assay
Appendix B
Adipokines and Inflammatory Parameters
References
- World Health Organization. Obesity and Overweight. 2018. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 August 2020).
- Murphy, N.F.; MacIntyre, K.; Stewart, S.; Hart, C.L.; Hole, D.; McMurray, J.J. Long-term cardiovascular consequences of obesity: 20-year follow-up of more than 15 000 middle-aged men and women (the Renfrew-Paisley study). Eur. Heart J. 2006, 27, 96–106. [Google Scholar] [CrossRef]
- Khan, S.S.; Ning, H.; Wilkins, J.T.; Allen, N.; Carnethon, M.; Berry, J.D.; Sweis, R.N.; Lloyd-Jones, D.M. Association of Body Mass Index with Lifetime Risk of Cardiovascular Disease and Compression of Morbidity. JAMA Cardiol. 2018, 3, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Sjöström, L.; Gummesson, A.; Sjöström, C.D.; Narbro, K.; Peltonen, M.; Wedel, H.; Bengtsson, C.; Bouchard, C.; Carlsson, B.; Dahlgren, S.; et al. Swedish Obese Subjects Study. Effects of bariatric surgery on mortality in Swedish obese subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, T.D.; Gress, R.E.; Smith, S.C.; Halverson, R.C.; Simper, S.C.; Rosamond, W.D.; LaMonte, M.J.; Stroup, A.M.; Hunt, S.C. Long-term mortality after gastric bypass surgery. N. Engl. J. Med. 2007, 357, 753–761. [Google Scholar] [CrossRef] [Green Version]
- Safar, M.E. Arterial stiffness as a risk factor for clinical hypertension. Nat. Rev. Cardiol. 2018, 15, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Cecelja, M.; Chowienczyk, P. Role of arterial stiffness in cardiovascular disease. JRSM Cardiovasc. Dis. 2012, 1, 1–10. [Google Scholar] [CrossRef]
- Petersen, K.S.; Clifton, P.M.; Lister, N.; Keogh, J.B. Effect of weight loss induced by energy restriction on measures of arterial compliance: A systematic review and meta-analysis. Atherosclerosis 2016, 247, 7–20. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Shlomo, Y.; Spears, M.; Boustred, C.; May, M.; Anderson, S.G.; Benjamin, E.J.; Boutouyrie, P.; Cameron, J.; Chen, C.H.; Cruickshank, J.K.; et al. Aortic pulse wave velocity improves cardiovascular event prediction: An individual participant meta-analysis of prospective observational data from 17,635 subjects. J. Am. Coll. Cardiol. 2014, 63, 636–646. [Google Scholar] [CrossRef]
- Niiranen, T.J.; Kalesan, B.; Hamburg, N.M.; Benjamin, E.J.; Mitchell, G.F.; Vasan, R.S. Relative Contributions of Arterial Stiffness and Hypertension to Cardiovascular Disease: The Framingham Heart Study. J. Am. Heart Assoc. 2016, 5, e004271. [Google Scholar] [CrossRef]
- Wildman, R.P.; Mackey, R.H.; Bostom, A.; Thompson, T.; Sutton-Tyrrell, K. Measures of obesity are associated with vascular stiffness in young and older adults. Hypertension 2003, 42, 468–473. [Google Scholar] [CrossRef] [Green Version]
- Frey, S.; Jacobi, D.; Pichelin, M.; Cariou, B.; Mirallié, E.; Blanchard, C. Improvement in arterial stiffness (pOpmètre®) after bariatric surgery. Results from a prospective study. Ann. Endocrinol. 2020, 81, 44–50. [Google Scholar] [CrossRef]
- Cooper, J.N.; Buchanich, J.M.; Youk, A.; Brooks, M.M.; Barinas-Mitchell, E.; Conroy, M.B.; Sutton-Tyrrell, K. Reductions in arterial stiffness with weight loss in overweight and obese young adults: Potential mechanisms. Atherosclerosis 2012, 223, 485–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samaras, K.; Viardot, A.; Lee, P.N.; Jenkins, A.; Botelho, N.K.; Bakopanos, A.; Lord, R.V.; Hayward, C.S. Reduced arterial stiffness after weight loss in obese type 2 diabetes and impaired glucose tolerance: The role of immune cell activation and insulin resistance. Diab. Vasc. Dis. Res. 2013, 10, 40–48. [Google Scholar] [CrossRef]
- Petersen, K.S.; Blanch, N.; Keogh, J.B.; Clifton, P.M. Effect of weight loss on pulse wave velocity: Systematic review and meta-analysis. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 243–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordstrand, N.; Gjevestad, E.; Hertel, J.K.; Johnson, L.K.; Saltvedt, E.; Røislien, J.; Hjelmesaeth, J. Arterial stiffness, lifestyle intervention and a low-calorie diet in morbidly obese patients-a nonrandomized clinical trial. Obesity (Silver Spring) 2013, 21, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Oliveras, A.; Goday, A.; Sans, L.; Arias, C.E.; Vazquez, S.; Benaiges, D.; Ramon, J.M.; Pascual, J. Changes in Central 24-h Ambulatory Blood Pressure and Hemodynamics 12 Months After Bariatric Surgery: The Barihta Study. Obes. Surg. 2020, 30, 195–205. [Google Scholar] [CrossRef]
- Papaioannou, T.G.; Argyris, A.; Protogerou, A.D.; Vrachatis, D.; Nasothimiou, E.G.; Sfikakis, P.P.; Stergiou, G.S.; Stefanadis, C.I. Non-invasive 24 h ambulatory monitoring of aortic wave reflection and arterial stiffness by a novel oscillometric device: The first feasibility and reproducibility study. Int. J. Cardiol. 2013, 169, 57–61. [Google Scholar] [CrossRef]
- Hametner, B.; Wassertheurer, S.; Kropf, J.; Mayer, C.; Eber, B.; Weber, T. Oscillometric estimation of aortic pulse wave velocity: Comparison with intra-aortic catheter measurements. Blood Press. Monit. 2013, 18, 173–176. [Google Scholar] [CrossRef]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H. European Network for Non-invasive Investigation of Large Arteries. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S.; Marais, L.; Boutouyrie, P. The Noninvasive Assessment of Vascular Aging. Can. J. Cardiol. 2016, 32, 669–679. [Google Scholar] [CrossRef]
- Soler, M.J.; Riera, M.; Crespo, M.; Mir, M.; Márquez, E.; Pascual, M.J.; Pascual, J. Circulating angiotensin-converting enzyme 2 activity in kidney transplantation: A longitudinal pilot study. Nephron Clin. Pract. 2012, 121, c144–c150. [Google Scholar] [CrossRef]
- Tucker, O.N.; Szomstein, S.; Rosenthal, R.J. Indications for sleeve gastrectomy as a primary procedure for weight loss in the morbidly obese. J. Gastrointest. Surg. 2008, 12, 662–667. [Google Scholar] [CrossRef]
- Oliveras, A. Barcelona, Spain. Unpublished work. 2021. [Google Scholar]
- Weisbrod, R.M.; Shiang, T.; Al Sayah, L.; Fry, J.L.; Bajpai, S.; Reinhart-King, C.A.; Lob, H.E. Arterial stiffening precedes systolic hypertension in diet-induced obesity. Hypertension 2013, 62, 1105–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giudici, A.; Palombo, C.; Kozakova, M.; Morizzo, C.; Losso, L.; Nannipieri, M.; Berta, R.; Hughes, A.D. Weight Loss After Bariatric Surgery Significantly Improves Carotid and Cardiac Function in Apparently Healthy People with Morbid Obesity. Obes. Surg. 2020, 30, 3776–3783. [Google Scholar] [CrossRef]
- Rossi, G.P.; Maiolino, G. Excess Arterial Damage in Hyperaldosteronism. Hypertension 2019, 74, 502–504. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, I.; Mazarakis, A.; Papadopoulos, C.; Patsouras, N.; Kalfarentzos, F.; Lekakis, J.; Kremastinos, D.T.; Alexopoulos, D. Weight loss after bariatric surgery improves aortic elastic properties and left ventricular function in individuals with morbid obesity: A 3-year follow-up study. J. Hypertens. 2007, 25, 439–447. [Google Scholar] [CrossRef]
- Schütten, M.T.; Houben, A.J.; de Leeuw, P.W.; Stehouwer, C.D. The Link Between Adipose Tissue Renin-Angiotensin-Aldosterone System Signaling and Obesity-Associated Hypertension. Physiology (Bethesda) 2017, 32, 197–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, N.; Li, H. The role of perivascular adipose tissue in obesity-induced vascular dysfunction. Br. J. Pharmacol. 2017, 174, 3425–3442. [Google Scholar] [CrossRef] [Green Version]
- Chappell, M.C.; Marshall, A.C.; Alzayadneh, E.M.; Shaltout, H.A.; Diz, D.I. Update on the Angiotensin converting enzyme 2-Angiotensin (1-7)-MAS receptor axis: Fetal programing, sex differences, and intracellular pathways. Front. Endocrinol. 2014, 4, 201. [Google Scholar] [CrossRef] [Green Version]
- Lelis, D.F.; Freitas, D.F.; Machado, A.S.; Crespo, T.S.; Santos, S.H.S. Angiotensin-(1-7), Adipokines and Inflammation. Metabolism 2019, 95, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Salvi, P.; Furlanis, G.; Grillo, A.; Pini, A.; Salvi, L.; Marelli, S.; Rovina, M.; Moretti, F.; Gaetano, R.; Pintassilgo, I.; et al. Unreliable Estimation of Aortic Pulse Wave Velocity Provided by the Mobil-O-Graph Algorithm-Based System in Marfan Syndrome. J. Am. Heart Assoc. 2019, 8, e04028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, J.E.; Feig, P.U.; Izzo, J.L., Jr. Pulse Wave Velocities Derived From Cuff Ambulatory Pulse Wave Analysis. Hypertension 2019, 74, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Salvi, P.; Scalise, F.; Rovina, M.; Moretti, F.; Salvi, L.; Grillo, A.; Gao, L.; Baldi, C.; Faini, A.; Furlanis, G.; et al. Noninvasive Estimation of Aortic Stiffness Through Different Approaches. Hypertension 2019, 74, 117–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Age, year (mean ± SD) | 42.7 ± 9.4 |
| Sex, women, n (%) | 34 (72.3) |
| Body weight, kg (mean ± SD) | 118.1 ± 19.5 |
| Waist circumference, cm (mean ± SD) | 131.6 ± 10.7 |
| Body mas index, kg/m2 (mean ± SD) | 42.2 ± 5.4 |
| Race, Caucasian, n (%) | 45 (95.7) |
| Current smokers, n (%) | 10 (21.3) |
| Surgical procedure, n (%): | |
| Sleeve gastrectomy | 20 (42.6) |
| Roux-en-Y gastric bypass | 27 (57.4) |
| Hypertension, n (%) | 20 * (42.6) |
| T2-Diabetes Mellitus, n (%) | 4 (8.5) |
| Dyslipidemia, n (%) | 12 (25.5) |
| Previous major vascular event **, n (%) | 3 (6.4) |
| Sleep apnea syndrome, n (%) | 11 (23.4) |
| CPAP, n (%) | 9 (81.8) |
| All Patients (n = 47) | Patients without Antihypertensive Treatment at Baseline ** (n = 30) | |||||
|---|---|---|---|---|---|---|
| Parameter | Baseline Mean ± SD | 1-Month Mean ± SD | p | Baseline Mean ± SD | 1-Month Mean ± SD | p |
| Anthropometric parameters | ||||||
| Body weight, kg | 118.1 ± 19.5 | 104.5 ± 17.5 | <0.001 | 116.1 ± 17.7 | 102.5 ± 15.2 | <0.001 |
| Waist circumference, cm | 132.0 ± 12.0 | 122.4 ± 10.2 | <0.001 | 130.2 ± 10.6 | 120.2 ± 9.3 | <0.001 |
| Arterial stiffness | ||||||
| 24 h-PP, mmHg | 46.4 ± 7.5 | 44.2 ± 7.1 | 0.001 | 45.8 ± 6.9 | 43.1 ± 6.6 | 0.010 |
| 24 h-PWV, m/s | 6.64 ± 1.03 | 6.24 ± 0.97 | <0.001 | 6.2 ± 1.0 | 6.11 ± 0.99 | 0.001 |
| AIx@75, % | 26.4 ± 7.5 | 22.7 ± 7.1 | <0.001 | 24.8 ± 5.9 | 22.2 ± 6.0 | 0.028 |
| Blood pressure, heart rate and cardiac output | ||||||
| 24 h-SBP, mmHg | 120.0 ± 11.7 | 114.3 ± 9.9 | <0.001 | 118.6 ± 10.7 | 113.5 ± 9.7 | <0.001 |
| 24 h-DBP, mmHg | 73.7 ± 9.0 | 70.2 ± 6.9 | <0.001 | 72.1 ± 7.7 | 69.4 ± 6.8 | <0.001 |
| 24 h-HR, bpm | 73.2 ± 10.1 | 66.7 ± 8.8 | <0.001 | 75.2 ± 9.2 | 68.7 ± 7.6 | <0.001 |
| Cardiac output | 4.6 ± 0.6 | 4.5 ± 0.5 | <0.001 | 4.7 ± 0.5 | 4.5 ± 0.4 | 0.004 |
| Glucose metabolism parameters | ||||||
| Fasting glucose, mg/dL | 99.6 ± 19.1 | 86.5 ± 10.1 | <0.001 | 95.9 ± 12.9 | 85.7 ± 9.2 | <0.001 |
| Glycosylated hemoglobin, % | 5.7 ± 0.8 | 5.3 ± 0.6 | <0.001 | 5.7 ± 1.0 | 5.3 ± 0.6 | 0.001 |
| Fasting insulin *, mcU/mL | 12.0 [8.3; 17.3] | 6.8 [3.9; 9.4] | <0.001 | 11.7 [7.1; 17.3] | 6.3 [2.9; 9.2] | <0.001 |
| Insulin resistance (HOMA-IR) * | 54.5 [37.2; 87.1] | 23.8 [13.8; 39.3] | <0.001 | 50.4 [28.3; 82.2] | 23.3 [10.3; 39.3] | <0.001 |
| RAAS components | ||||||
| PRA *, ng/mL/h | 0.8 [0.3; 1.3] | 0.8 [0.5; 1.2] | 0.726 | 0.8 [0.4; 1.2] | 0.9 [0.5; 1.5] | 0.411 |
| Aldosterone *, ng/dL | 87.8 [56.8; 134.5] | 82.0 [61.4; 139.5] | 0.747 | 76.7 [59.3; 108.3] | 86.0 [65.8; 128.5] | 0.210 |
| ACE activity, RFU/µL | 1320.2 ± 385.8 | 1099.0 ± 293.7 | <0.001 | 1307.9 ± 337.4 | 1126.6 ± 258.0 | <0.001 |
| ACE2 activity *, RFU/µL/h | 7.9 [5.8; 10.8] | 6.0 [4.7; 7.8] | <0.001 | 7.6 [5.5; 9.4] | 5.8 [4.2; 7.8] | 0.001 |
| ACE act./ACE2 act. | 170.0 ± 82.0 | 194.1 ± 108.7 | 0.009 | 183.0 ± 93.3 | 207.4 ± 118.1 | 0.072 |
| Adipokines & Inflammatory Markers | ||||||
| Leptin *, ng/mL | 56.5 [28.8; 73.7] | 21.4 [12.1; 37.3] | <0.001 | 45.1 [24.3; 67.1] | 15.9 [9.5; 31.5] | <0.001 |
| Adiponectine *, μg/mL | 19.0 [12.5; 33.3] | 23.6 [12.9; 40.5] | 0.050 | 22.5 [16.0; 35.5] | 27.1 [16.8; 45.6] | 0.043 |
| Resistin, ng/mL | 36.8 ± 13.3 | 37.3 ± 14.9 | 0.822 | 35.9 ± 11.2 | 39.4 ± 12.7 | 0.106 |
| MCP-1, pg/mL | 544.9 ± 197.5 | 601.5 ± 249.4 | 0.041 | 530.0 ± 199.5 | 632.6 ± 274.7 | 0.014 |
| Angiopoietin2 *, pg/mL | 2676.2 [1815.4; 4067.0] | 4039.6 [2076.8; 5380.9] | 0.042 | 2721.4 [1815.4; 4655.1] | 4366.8 [2011.9; 5293.3] | 0.046 |
| hs-CRP *, mg/dL | 0.77 [0.43; 1.41] | 0.45 [0.24; 0.74] | 0.001 | 0.57 [0.32; 0.93] | 0.56 [0.25; 0.74] | 0.249 |
| Dep. Variable | B Coefficient | 95% (CI) | p | |
|---|---|---|---|---|
| Model 1 | 1-month 24 h PP | |||
| Age | ||||
| Sex | ||||
| Δ 24 h-SBP | 0.481 | 0.272–0.689 | 0.001 | |
| Δ body weight | ||||
| Δ cardiac output | ||||
| Baseline 24 h-PP | 0.996 | 0.771–1.220 | < 0.001 | |
| Δ ACE | ||||
| Model 2 | 1-month PWV | |||
| Age | ||||
| Sex | ||||
| Δ 24 h-SBP | 0.032 | 0.008–0.056 | 0.014 | |
| Δ body weight | ||||
| Δ cardiac output | ||||
| Baseline PWV | 0.651 | 0.416–0.886 | < 0.001 | |
| Δ aldosterone | −0.003 | −0.005–0.000 | 0.022 | |
| Model 3 | 1-month AI@75 | |||
| Age | ||||
| Sex | ||||
| Δ 24 h-SBP | ||||
| Δ body weight | ||||
| Δ cardiac output | ||||
| Baseline AI@75 | 0.326 | 0.013–0.639 | 0.043 | |
| Δ ACE/ACE2 | 0.036 | 0.005–0.006 | 0.024 | |
| Below Median Baseline 24 h-PWV (n = 21) | Above Median Baseline 24 h-PWV (n = 15) | Below Median Baseline 24 h AIx@75 (n = 18) | Above Median Baseline 24 h-AIx@75 (n = 18) | Below Median Baseline 24 h-PP (n = 18) | Above Median Baseline 24 h-PP (n = 18) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (95%CI) | p | Mean (95%CI) | p | Mean (95%CI) | p | Mean (95%CI) | p | Mean (95%CI) | p | Mean (95%CI) | p | |
| Δ 24 h-PWV | ||||||||||||
| 1 month | −0.18 (−0.25 to −0.10) | <0.001 | −0.31 (−0.64 to 0.02) | 0.060 | −0.18 (−0.28 to −0.08) | 0.002 | −0.29 (−0.55 to −0.03) | 0.034 | −0.16 (−0.28 to −0.04) | 0.013 | −0.31 (−0.56 to −0.05) | 0.020 |
| Δ 24 h-AIx@75 | ||||||||||||
| 1 month | −3.8 (−6.7 to −0.9) | 0.014 | −1.6 (−4.6 to 1.3) | 0.261 | −0.0 (−2.8 to 2.7) | 0.990 | −5.7 (−8.3 to −3.2) | <0.001 | −1.9 (−4.3 to 0.4) | 0.106 | −4.3 (−6.7 to −1.9) | 0.001 |
| Δ 24 h-PP | ||||||||||||
| 1 month | −3.4 (−5.5 to −1.3) | 0.003 | −2.3 (−5.1 to 0.4) | 0.563 | −2.0 (−5.0 to 1.0) | 0.177 | −2.7 (−4.8 to −0.6) | 0.015 | −2.1 (−5.1 to 0.8) | 0.149 | −3.6 (−6.7 to −0.6) | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveras, A.; Galceran, I.; Goday, A.; Vázquez, S.; Sans, L.; Riera, M.; Benaiges, D.; Pascual, J. Improvement of Arterial Stiffness One Month after Bariatric Surgery and Potential Mechanisms. J. Clin. Med. 2021, 10, 691. https://doi.org/10.3390/jcm10040691
Oliveras A, Galceran I, Goday A, Vázquez S, Sans L, Riera M, Benaiges D, Pascual J. Improvement of Arterial Stiffness One Month after Bariatric Surgery and Potential Mechanisms. Journal of Clinical Medicine. 2021; 10(4):691. https://doi.org/10.3390/jcm10040691
Chicago/Turabian StyleOliveras, Anna, Isabel Galceran, Albert Goday, Susana Vázquez, Laia Sans, Marta Riera, David Benaiges, and Julio Pascual. 2021. "Improvement of Arterial Stiffness One Month after Bariatric Surgery and Potential Mechanisms" Journal of Clinical Medicine 10, no. 4: 691. https://doi.org/10.3390/jcm10040691