
Do-(Not-)Mechanical-Circulatory-Support Orders: Should We Ask All Cardiac Surgery Patients for Informed Consent for Post-Cardiotomy Extracorporeal Life Circulatory Support?

 , , and
, , and
Abstract
:1. Introduction
2. Do-(not-)Mechanical-Circulatory-Support Orders?
3. Impact on Family and Patient
4. PC-ECLS and the Health Care System
5. Informed Consent and Patient Autonomy
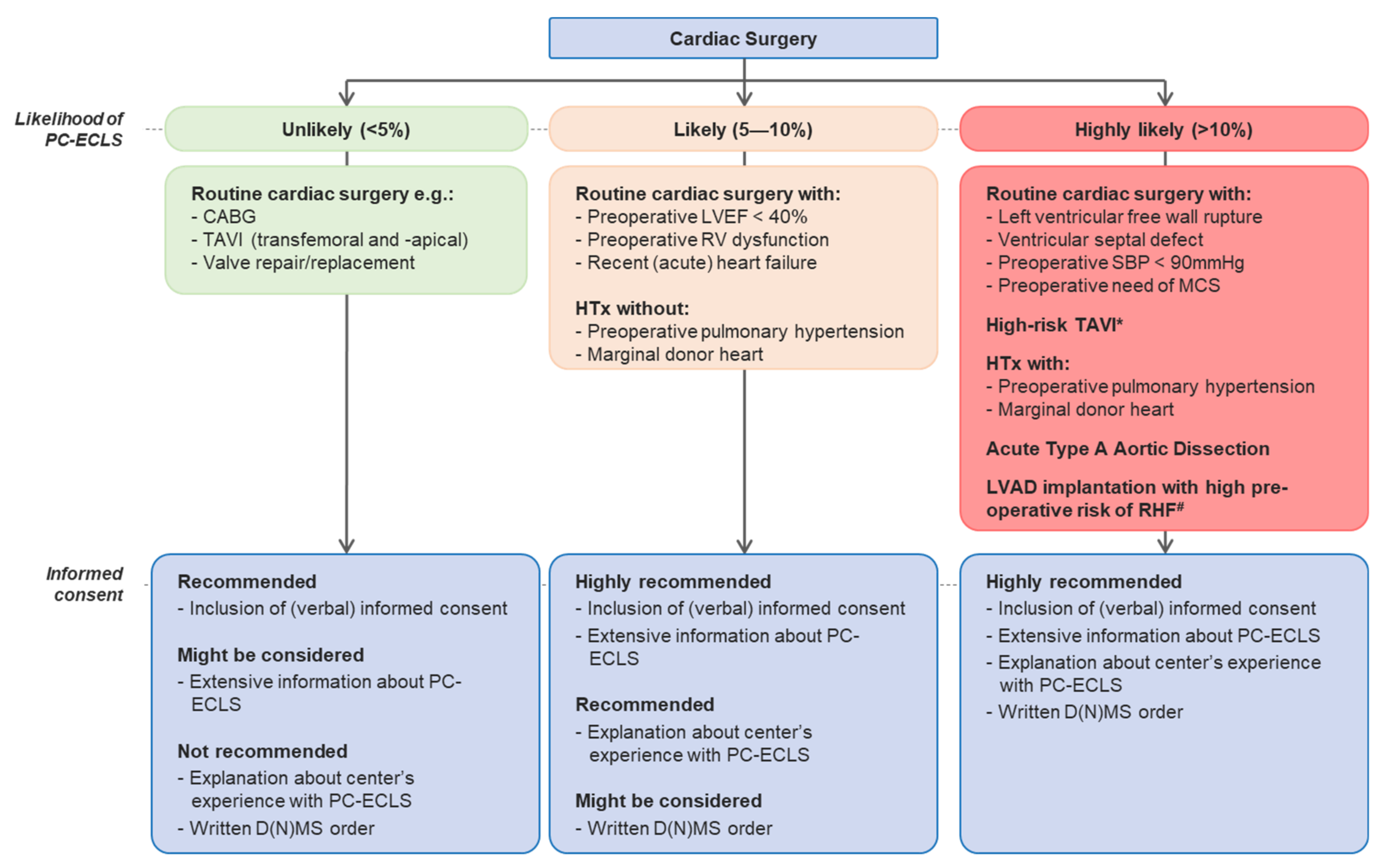
6. What Should the Informed Consent Look Like?
7. Likelihood of PC-ECLS
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hernandez, A.F.; Grab, J.D.; Gammie, J.S.; O’Brien, S.M.; Hammill, B.G.; Rogers, J.G.; Camacho, M.T.; Dullum, M.K.; Ferguson, T.B.; Peterson, E.D. A decade of short-term outcomes in post cardiac surgery ventricular assist device implantation: Data from the Society of Thoracic Surgeons’ National Cardiac Data-base. Circulation 2007, 116, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, R.; Raffa, G.M.; Kowalewski, M.; Alenizy, K.; Sluijpers, N.; Makhoul, M.; Brodie, D.; McMullan, M.; Wang, I.W.; Meani, F.; et al. Structured review of post-cardiotomy extracorporeal membrane oxygenation: Part 2—Pediatric patients. J. Heart Lung Transplant. 2019, 38, 1144–1161. [Google Scholar] [CrossRef] [PubMed]
- Doll, N.; Kiaii, B.; Borger, M.; Bucerius, J.; Krämer, K.; Schmitt, D.V.; Walther, T.; Mohr, F.W. Five-Year results of 219 consecutive patients treated with extracorporeal membrane oxygenation for refractory postoperative cardiogenic shock. Ann. Thorac. Surg. 2004, 77, 151–157. [Google Scholar] [CrossRef]
- Smith, C.; Bellomo, R.; Raman, J.S.; Matalanis, G.; Rosalion, A.; Buckmaster, J.; Hart, G.; Silvester, W.; Gutteridge, G.A.; Smith, B.; et al. An extracorporeal membrane oxygenation–based approach to cardiogenic shock in an older population. Ann. Thorac. Surg. 2001, 71, 1421–1427. [Google Scholar] [CrossRef]
- Lorusso, R.; Raffa, G.M.; Alenizy, K.; Sluijpers, N.; Makhoul, M.; Brodie, D.; McMullan, M.; Wang, I.W.; Meani, F.; MacLaren, G.; et al. Structured review of post-cardiotomy extracorporeal membrane oxygenation: Part 1—Adult patients. J. Heart Lung Transplant. 2019, 38, 1125–1143. [Google Scholar] [CrossRef]
- Den Uil, C.A.; Akin, S.; Jewbali, L.S.; Dos Reis Miranda, D.; Brugts, J.J.; Constantinescu, A.A.; Kappetein, A.P.; Caliskan, K. Short-term mechanical circulatory support as a bridge to durable left ventricular assist device implantation in refractory cardiogenic shock: A systematic review and meta-analysis. Eur. J. Cardiothorac. Surg. 2017, 52, 14–25. [Google Scholar] [CrossRef] [Green Version]
- Whitman, G.J. Extracorporeal membrane oxygenation for the treatment of postcardiotomy shock. J. Thorac. Cardiovasc. Surg. 2017, 153, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Sauer, C.M.; Yuh, D.D.; Bonde, P. Extracorporeal Membrane Oxygenation Use Has Increased by 433% in Adults in the United States from 2006 to 2011. ASAIO J. 2015, 61, 31–36. [Google Scholar] [CrossRef]
- Cheng, R.; Hachamovitch, R.; Kittleson, M.; Patel, J.; Arabia, F.; Moriguchi, J.; Esmailian, F.; Azarbal, B. Complications of Extracorporeal Membrane Oxygenation for Treatment of Cardiogenic Shock and Cardiac Arrest: A Meta-Analysis of 1, 866 Adult Patients. Ann. Thorac. Surg. 2014, 97, 610–616. [Google Scholar] [CrossRef]
- Raffa, G.M.; Gelsomino, S.; Sluijpers, N.; Meani, P.; Alenizy, K.; Natour, E.; Elham, B.; Daniel, M.J.; Maged, M.; Samuel, H.; et al. In-hospital outcome of post-cardiotomy extracor-poreal life support in adult patients: The 2007–2017 Maastricht experience. Crit. Care Resusc. 2017, 19 (Suppl. 1), 53–61. [Google Scholar]
- Lo Coco, V.; Lorusso, R.; Raffa, G.M.; Malvindi, P.G.; Pilato, M.; Martucci, G.; Arcadipane, A.; Zieliński, K.; Suwalski, P.; Kowalewski, M.; et al. Clinical complications during veno-arterial extra-corporeal membrane oxigenation in post-cardiotomy and non post-cardiotomy shock: Still the achille’s heel. J. Thorac. Dis. 2018, 10, 6993–7004. [Google Scholar] [CrossRef] [PubMed]
- Rabkin, M.T.; Gillerman, G.; Rice, N.R. Orders Not to Resuscitate. N. Engl. J. Med. 1976, 295, 364–366. [Google Scholar] [CrossRef] [PubMed]
- Loertscher, L.; Reed, D.A.; Bannon, M.P.; Mueller, P.S. Cardiopulmonary Resuscitation and Do-Not-Resuscitate Orders: A Guide for Clinicians. Am. J. Med. 2010, 123, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, A.J.O.; Malyon, A.C.; Fritz, Z.B.M. Themes and variations: An exploratory international investigation into resuscitation decisionmaking. Resuscitation 2016, 103, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Brouwers, C.; Denollet, J.; de Jonge, N.; Caliskan, K.; Kealy, J.; Pedersen, S.S. Patient-reported outcomes in left ventricular assist de-vice therapy: A systematic review and recommendations for clinical research and practice. Circ. Heart Fail. 2011, 4, 714–723. [Google Scholar] [CrossRef] [Green Version]
- Morgan, C.K.; Varas, G.M.; Pedroza, C.; Almoosa, K.F. Defining the practice of “no escalation of care” in the ICU. Crit. Care Med. 2014, 42, 357–361. [Google Scholar] [CrossRef]
- Tramm, R.; Ilic, D.; Murphy, K.; Sheldrake, J.; Pellegrino, V.; Hodgson, C. Experience and needs of family members of patients treated with extracorporeal membrane oxygenation. J. Clin. Nurs. 2017, 26, 1657–1668. [Google Scholar] [CrossRef]
- Harris-Fox, S. The experience of being an ‘extracorporeal membrane oxygenation’ relative within the CESAR trial. Nurs. Crit. Care 2011, 17, 9–18. [Google Scholar] [CrossRef]
- Cameron, J.I.; Chu, L.M.; Matte, A.; Tomlinson, G.; Chan, L.; Thomas, C.; Friedrich, J.O.; Mehta, S.; Lamontagne, F.; Levasseur, M.; et al. One-Year Outcomes in Caregivers of Critically Ill Patients. N. Engl. J. Med. 2016, 374, 1831–1841. [Google Scholar] [CrossRef]
- Ramos-Lima, M.J.M.; Brasileiro, I.C.; Lima, T.L.; Braga-Neto, P. Quality of life after stroke: Impact of clinical and sociodemographic factors. Clinics 2018, 73, e418. [Google Scholar] [CrossRef]
- Savas, H.; Koken, Z.O.; Celik, S.S. Experiences of adult extracorporeal membrane oxygenation patients following discharge: A mixed methods study. Heart Lung 2020, 49, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.; Ipsen, T.; Doherty, P.; Langberg, H. Physical and social factors determining quality of life for veterans with low-er-limb amputation(s): A systematic review. Disabil. Rehabil. 2016, 38, 2345–2353. [Google Scholar] [CrossRef] [PubMed]
- Grzebień, A.; Chabowski, M.; Malinowski, M.; Uchmanowicz, I.; Milan, M.; Janczak, D. Analysis of selected factors determining quality of life in patients after lower limb amputation- a review article. Pol. J. Surg. 2017, 89, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Dowdy, D.W.; Eid, M.P.; Sedrakyan, A.; Mendez-Tellez, P.A.; Pronovost, P.J.; Herridge, M.S.; Needham, D.M. Quality of life in adult survivors of critical illness: A systematic review of the literature. Intensive Care Med. 2005, 31, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Muller, G.; Flecher, E.; Lebreton, G.; Luyt, C.-E.; Trouillet, J.-L.; Bréchot, N.; Schmidt, M.; Mastroianni, C.; Chastre, J.; Leprince, P.; et al. The ENCOURAGE mortality risk score and analysis of long-term outcomes after VA-ECMO for acute myocardial infarction with cardiogenic shock. Intensive Care Med. 2016, 42, 370–378. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.D.; Sandsmark, D.K.; Palakshappa, J.A.; Mikkelsen, M.E.; Anderson, B.J.; Gutsche, J.T. Long-Term Outcomes After Ex-tracorporeal Life Support for Acute Respiratory Failure. J. Cardiothorac. Vasc. Anesth. 2019, 33, 72–79. [Google Scholar] [CrossRef]
- Wilcox, M.E.; Jaramillo-Rocha, V.; Hodgson, C.; Taglione, M.S.; Ferguson, N.D.; Fan, E. Long-Term Quality of Life After Extracorpo-real Membrane Oxygenation in ARDS Survivors: Systematic Review and Meta-Analysis. J. Intensive Care Med. 2020, 35, 233–243. [Google Scholar] [CrossRef]
- Wang, Z.-Y.; Li, T.; Wang, C.-T.; Xu, L.; Gao, X.-J. Assessment of 1-year Outcomes in Survivors of Severe Acute Respiratory Distress Syndrome Receiving Extracorporeal Membrane Oxygenation or Mechanical Ventilation: A Prospective Observational Study. Chin. Med. J. 2017, 130, 1161–1168. [Google Scholar] [CrossRef]
- Schmidt, M.; Zogheib, E.; Rozé, H.; Repesse, X.; Lebreton, G.; Luyt, C.-E.; Trouillet, J.-L.; Bréchot, N.; Nieszkowska, A.; Dupont, H.; et al. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med. 2013, 39, 1704–1713. [Google Scholar] [CrossRef]
- O’Brien, S.G.; Carton, E.G.; Fealy, G.M. Long-Term Health-Related Quality of Life after Venovenous Extracorporeal Membrane Oxygenation. ASAIO J. 2020, 66, 580–585. [Google Scholar] [CrossRef]
- Orbo, M.C.; Karlsen, S.F.; Pedersen, E.P.; Hermansen, S.E.; Ronning, P.B.; Nergaard, K.A.; Næsheim, T.; Myrmel, T. Health-related quality of life after ex-tracorporeal membrane oxygenation: A single centre’s experience. ESC Heart Fail. 2019, 6, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Tramm, R.; Hodgson, C.; Ilic, D.; Sheldrake, J.; Pellegrino, V. Identification and prevalence of PTSD risk factors in ECMO patients: A single centre study. Aust. Crit. Care. 2015, 28, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Davydow, D.S.; Zatzick, D.; Hough, C.L.; Katon, W.J. A longitudinal investigation of posttraumatic stress and depressive symp-toms over the course of the year following medical-surgical intensive care unit admission. Gen. Hosp. Psychiatry 2013, 35, 226–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbaro, R.P.; Odetola, F.O.; Kidwell, K.M.; Paden, M.L.; Bartlett, R.H.; Davis, M.M.; Annich, G.M. Association of hospital-level volume of ex-tracorporeal membrane oxygenation cases and mortality. Analysis of the extracorporeal life support organization registry. Am. J. Respir. Crit. Care Med. 2015, 191, 894–901. [Google Scholar] [CrossRef] [Green Version]
- Shah, P.; Thornton, I.; Turrin, D.; Hipskind, J.E. Informed Consent; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Beauchamp, T.L.; Childress, J. Principles of Biomedical Ethics: Marking Its Fortieth Anniversary. Am. J. Bioeth. 2019, 19, 9–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varelius, J. The value of autonomy in medical ethics. Med. Health Care Philos. 2006, 9, 377–388. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.Y.; Chen, L.; Kao, Y.H.; Chu, T.S.; Huang, T.S.; Ko, W.J. The over-optimistic portrayal of life-supporting treatments in news-papers and on the Internet: A cross-sectional study using extra-corporeal membrane oxygenation as an example. BMC Med. Ethics 2014, 15, 59. [Google Scholar] [CrossRef] [Green Version]
- MacLaren, G. When to initiate ECMO with low likelihood of success. Crit. Care 2018, 22, 217. [Google Scholar] [CrossRef] [Green Version]
- Mulaikal Teresa, A.; Nakagawa, S.; Prager Kenneth, M. Extracorporeal Membrane Oxygenation Bridge to No Recovery. Circulation 2019, 139, 428–430. [Google Scholar] [CrossRef]
- Wang, J.G.; Han, J.; Jia, Y.X.; Zeng, W.; Hou, X.T.; Meng, X. Outcome of veno-arterial extracorporeal membrane oxygenation for patients undergoing valvular surgery. PLoS ONE 2013, 8, e63924. [Google Scholar] [CrossRef] [Green Version]
- Hsu, P.-S.; Chen, J.-L.; Hong, G.-J.; Tsai, Y.-T.; Lin, C.-Y.; Lee, C.-Y.; Chen, Y.-G.; Tsai, C.-S. Extracorporeal membrane oxygenation for refractory cardiogenic shock after cardiac surgery: Predictors of early mortality and outcome from 51 adult patients. Eur. J. Cardio-Thorac. Surg. 2009, 37, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Ting, P.C.; Wu, V.C.; Liao, C.C.; Chou, A.H.; Tsai, F.C.; Lin, P.J.; Chen, C.Y.; Chen, H.W. Preoperative Right Ventricular Dysfunction Indicates High Vasoactive Support Needed After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2019, 33, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Biancari, F.; Dalén, M.; Perrotti, A.; Fiore, A.; Reichart, D.; Khodabandeh, S.; Gulbins, H.; Zipfel, S.; Al Shakaki, M.; Welp, H.; et al. Venoarterial extracorporeal membrane oxygenation after coronary artery bypass grafting: Results of a multicenter study. Int. J. Cardiol. 2017, 241, 109–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raffa, G.M.; Kowalewski, M.; Meani, P.; Follis, F.; Martucci, G.; Arcadipane, A.; Pilato, M.; Maessen, J.; Maessen, L. In-hospital outcomes after emergency or prophylactic veno-arterial extracorporeal membrane oxygenation during transcatheter aortic valve implantation: A comprehensive review of the literature. Perfusion 2019, 34, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Trenkwalder, T.; Pellegrini, C.; Holzamer, A.; Philipp, A.; Rheude, T.; Michel, J.; Kasel, A.M.; Kastrati, A.; Schunkert, H.; Endemann, D.; et al. Emergency extracorporeal membrane oxygenation in transcatheter aortic valve implantation: A two-center experience of incidence, outcome and temporal trends from 2010 to 2015. Catheter. Cardiovasc. Interv. 2018, 92, 149–156. [Google Scholar] [CrossRef]
- Mäkikallio, T.H.; Jalava, M.P.; Husso, A.; Virtanen, M.; Laakso, T.; Ahvenvaara, T.; Tauriainen, T.; Maaranen, P.; Kinnunen, E.-M.; Dahlbacka, S.; et al. Ten-year experience with transcatheter and surgical aortic valve replacement in Finland. Ann. Med. 2019, 51, 270–279. [Google Scholar] [CrossRef] [Green Version]
- Jalava, M.P.; Laakso, T.; Virtanen, M.; Niemelä, M.; Ahvenvaara, T.; Tauriainen, T.; Maaranen, P.; Husso, A.; Kinnunen, E.-M.; Dahlbacka, S.; et al. Transcatheter and Surgical Aortic Valve Replacement in Patients with Recent Acute Heart Failure. Ann. Thorac. Surg. 2019, 109, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Phan, K.; Luc, J.G.Y.; Xu, J.; Maltais, S.; Stulak, J.M.; Yan, T.D.; Tchantchaleishvili, V. Utilization and Outcomes of Temporary Mechanical Circulatory Support for Graft Dysfunction After Heart Transplantation. ASAIO J. 2017, 63, 695–703. [Google Scholar] [CrossRef]
- Huang, S.-M.; Huang, S.-C.; Wang, C.-H.; Wu, I.H.; Chi, N.-H.; Yu, H.-Y.; Hsu, R.-B.; Chang, C.-I.; Wang, S.-S.; Chen, Y.-S. Risk factors and outcome analysis after surgical man-agement of ventricular septal rupture complicating acute myocardial infarction: A retrospective analysis. J. Cardiothorac. Surg. 2015, 10, 66. [Google Scholar] [CrossRef] [Green Version]
- Listijono, D.R.; Watson, A.; Pye, R.; Keogh, A.M.; Kotlyar, E.; Spratt, P.; Granger, E.K.; Dhital, K.; Jansz, P.; Macdonald, P.S.; et al. Usefulness of extracorporeal membrane oxygenation for early cardiac allograft dysfunction. J. Heart Lung Transplant. 2011, 30, 783–789. [Google Scholar] [CrossRef]
- Formica, F.; Mariani, S.; Singh, G.; D’Alessandro, S.; Messina, L.A.; Jones, N.; Bamodu, O.A.; Sangalli, F.; Paolini, G. Postinfarction left ventricular free wall rupture: A 17-year single-centre experience. Eur. J. Cardio-Thorac. Surg. 2018, 53, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, T.-W.; Tsai, M.-T.; Hu, Y.-N.; Lin, W.-H.; Wang, W.-M.; Luo, C.-Y.; Roan, J.-N. Postoperative Extracorporeal Membrane Oxygenation Support for Acute Type A Aortic Dissection. Ann. Thorac. Surg. 2017, 104, 827–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Piao, H.; Li, B.; Wang, W.; Huang, M.; Zhu, Z.; Li, D.; Wang, T.; Liu, K. Extracorporeal Membrane Oxygenation in Stanford Type A Aortic Dissection. Int. Heart J. 2019, 60, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Riebandt, J.; Haberl, T.; Wiedemann, D.; Moayedifar, R.; Schloeglhofer, T.; Mahr, S.; Dimitrov, K.; Angleitner, P.; Laufer, G.; Zimpfer, D. Extracorporeal membrane oxygenation support for right ventricular failure after left ventricular assist device implantation. Eur. J. Cardiothorac. Surg. 2018, 53, 590–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Outcome | Author (Reference) | ECLS-Mode | Main Indication | Total Patients, N | Median Time to ECLS, Years | Prevalence, % |
|---|---|---|---|---|---|---|
| Clinically significant anxiety (HADS) | Muller et al. [25] | VA | AMI | 41 | 2.7 | 34 |
| McDonald et al. [26] | VV | ARF | 42 | 1.2 | 48 | |
| Schmidt et al. [29] | VV (95%) | ARDS | 67 | 1.4 | 34 | |
| O’brien et al. [30] | VV | ARF | 13 | 3.0 | 54 | |
| Orbo et al. [31] | VA (75%) | C (60%), P (25%) ECPR (15%) | 20 | 6.5 (mean) | 15 | |
| Anxiety/depression (EQ-5D) | Wang et al. [28] | VV | ARDS | 24 | 1.0 | None: 58 Moderate: 21 Extreme: 21 |
| Depression (HADS ) | Muller et al. [25] | VA | AMI | 41 | 2.7 | 20 |
| McDonald et al. [26] | VV | ARF | 42 | 1.2 | 26 | |
| Schmidt et al. [29] | VV (95%) | ARDS | 67 | 1.4 | 25 | |
| O’brien et al. [30] | VV | ARF | 13 | 3.0 | 15 | |
| Orbo et al. [31] | VA (75%) | C (60%), P (25%) CPR (15%) | 20 | 6.5 (mean) | 0 | |
| At risk for PTSD (IES(-R)) | Muller et al. [25] | VA | AMI | 41 | 2.7 | 5 |
| Schmidt et al. [29] | VV (95%) | ARDS | 67 | 1.4 | 16 | |
| O’brien et al. [30] | VV | ARF | 13 | 3.0 | 23 | |
| Pain/discomfort (EQ-5D) | Wang et al. [28] | VV | ARDS | 24 | 1.0 | None: 71 Moderate: 29 Extreme: 0 |
| Katz ADL and Lawton IADL | McDonald et al. [26] | VV | ARF | 42 | 1.2 | No deficiencies: 62 Mild/moderate: 19 Severe: 19 |
| Return to work | Orbo et al. [31] | VA (75%) | C (60%), P (25%) CPR (15%) | 20 | 6.5 (mean) | 50 |
| Preoperative Informed Consent for PC-ECLS and D(N)CS Orders | |
|---|---|
| Increasing Knowledge of the Patient | |
|
|
| Timing of D(N)MCS order | |
| |
| Procedure | Author (Reference)— Year of Publication | Total Patients, N | Prevalence of PC-ECLS Use, % | In-Hospital Mortality, % |
|---|---|---|---|---|
| Unlikely (<5%) | ||||
| CABG (isolated) | Biancari et al. [44]—2017 | 24,527 | VA-ECMO: 0.6 | 64.2 |
| Raffa et al. [45]—2019 | 5115 | Emergency VA-ECMO: 1.3 (TF and TA) | ||
| TAVI | Trenkwalder et al. [46]—2017 Trenkwalder et al. [46]—2017 | 1424 370 | Emergency VA-ECMO, TF: 1.5 Emergency VA-ECMO, TA: 3.0 | 39 Overall: 45.5 |
| SAVR | ||||
| Non-differentiated | Mäkikallio et al. [47]—2019 | 4333 | ECMO/IABP: 1.8 | N/A |
| Without recent AHF | Jalava et al. [48]—2019 | 3757 | ECMO/IABP: 1.3 | N/A |
| Likely (5–10%) | ||||
| SAVR (with recent AHF) | Jalava et al. [48]—2019 | 484 | ECMO/IABP: 5.6 | N/A |
| HTx | Phan et al. [49]—2017 | 11,555 | Overall MCS: 6.0 | VA-ECMO: 44.4 |
| VA-ECMO: 4.8 | ||||
| RVAD: 0.7 | RVAD: 62.1 | |||
| BiVAD: 0.5 | BiVAD: 14.3 | |||
| LVAD: 0.1 | LVAD: 37.5 | |||
| Highly likely (>10%) | ||||
| Ventricular septal defect | Huang et al. [50]—2015 | 47 | Preoperative IABP: 72.3 Preoperative VA-ECMO: 12.8 | N/A N/A |
| HTx (marginal donor heart; LVEF < 45) | Listijono et al. [51]—2011 | 9 | VA-ECMO: 89 | 12 |
| Post-MI LVFWR | Formica et al. [52]—2017 | 35 | Overall ECLS: 60 IABP: 28.6 VA-ECMO: 31.4 | Overall: 43 IABP: 30 VA-ECMO: 50 |
| aTAAD | Lin et al. [53]—2017 Wang et al. [54]–2019 | 162 246 | VA-ECMO: 12.3 VA-ECMO: 2.8 | 65 14.3 |
| LVAD implantation (isolated) | Riebandt et al. [55]—2017 | 154 | VA-ECMO: 21 | 25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simons, J.; Suverein, M.; van Mook, W.; Caliskan, K.; Soliman, O.; van de Poll, M.; Delnoij, T.; Maessen, J.; Mees, B.; Lorusso, R. Do-(Not-)Mechanical-Circulatory-Support Orders: Should We Ask All Cardiac Surgery Patients for Informed Consent for Post-Cardiotomy Extracorporeal Life Circulatory Support? J. Clin. Med. 2021, 10, 383. https://doi.org/10.3390/jcm10030383
Simons J, Suverein M, van Mook W, Caliskan K, Soliman O, van de Poll M, Delnoij T, Maessen J, Mees B, Lorusso R. Do-(Not-)Mechanical-Circulatory-Support Orders: Should We Ask All Cardiac Surgery Patients for Informed Consent for Post-Cardiotomy Extracorporeal Life Circulatory Support? Journal of Clinical Medicine. 2021; 10(3):383. https://doi.org/10.3390/jcm10030383
Chicago/Turabian StyleSimons, Jorik, Martje Suverein, Walther van Mook, Kadir Caliskan, Osama Soliman, Marcel van de Poll, Thijs Delnoij, Jos Maessen, Barend Mees, and Roberto Lorusso. 2021. "Do-(Not-)Mechanical-Circulatory-Support Orders: Should We Ask All Cardiac Surgery Patients for Informed Consent for Post-Cardiotomy Extracorporeal Life Circulatory Support?" Journal of Clinical Medicine 10, no. 3: 383. https://doi.org/10.3390/jcm10030383