
A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome

 , , ,
, , , 
Abstract
:1. Introduction
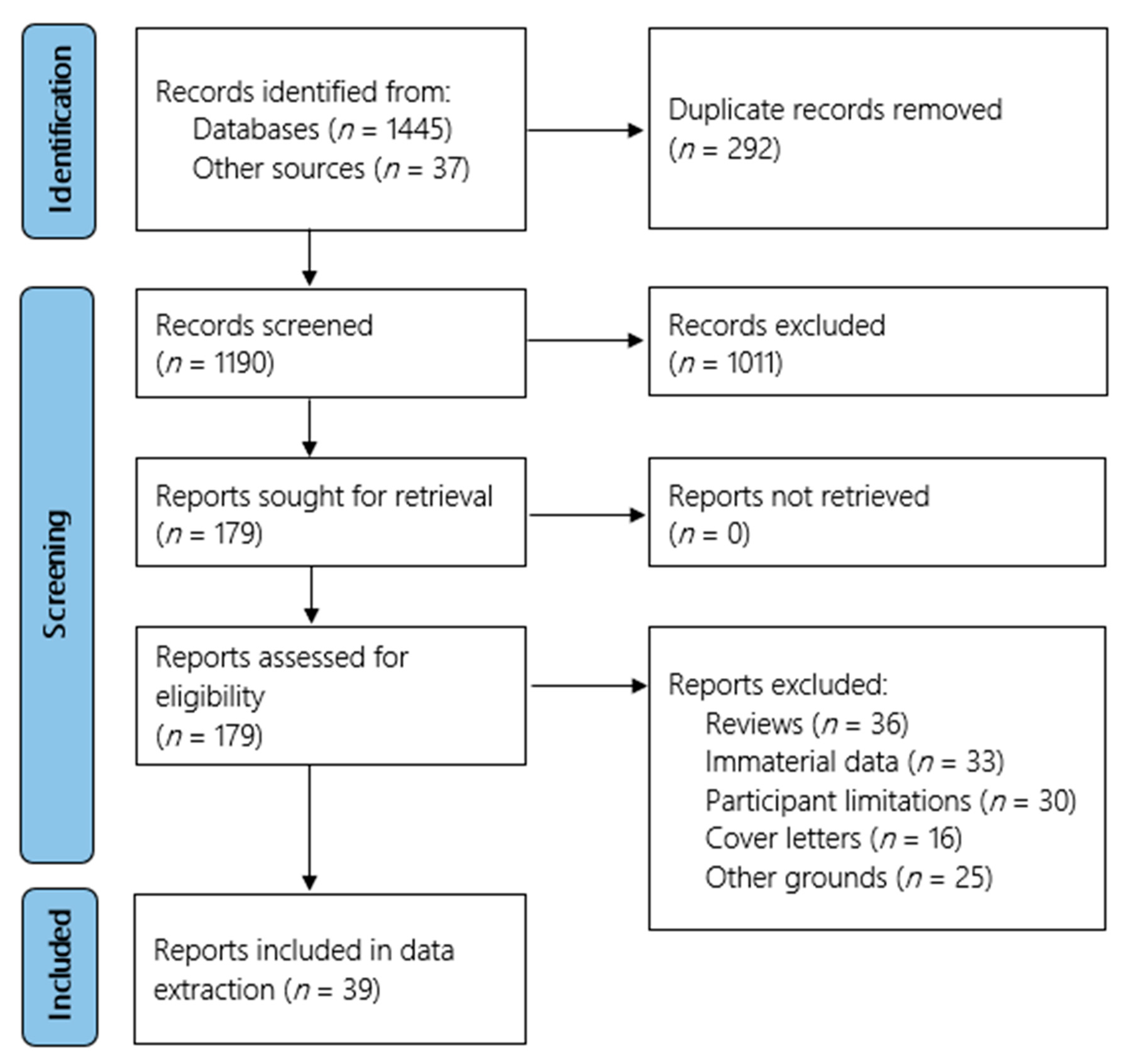
2. Methods and Materials
2.1. Protocol Registration
2.2. Search Strategy
2.3. Eligibility Criteria and Study Selection
2.4. Data Extraction
2.5. Quality Appraisal and Risk of Bias
3. Results
3.1. Description of Included Studies
3.2. Quality Appraisal and Risk of Bias
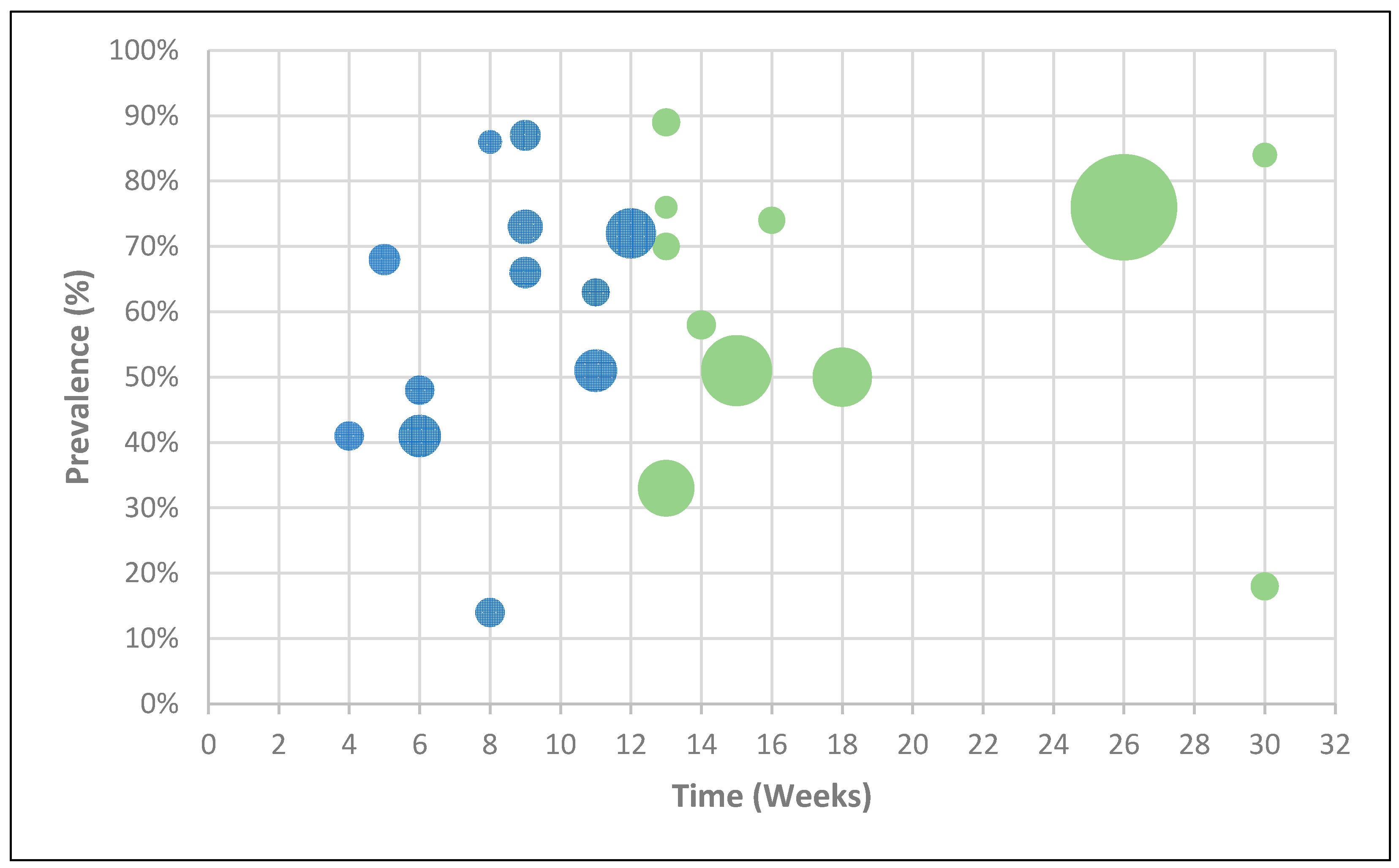
3.3. Ongoing Symptomatic COVID-19 and Post-COVID-19 Syndrome
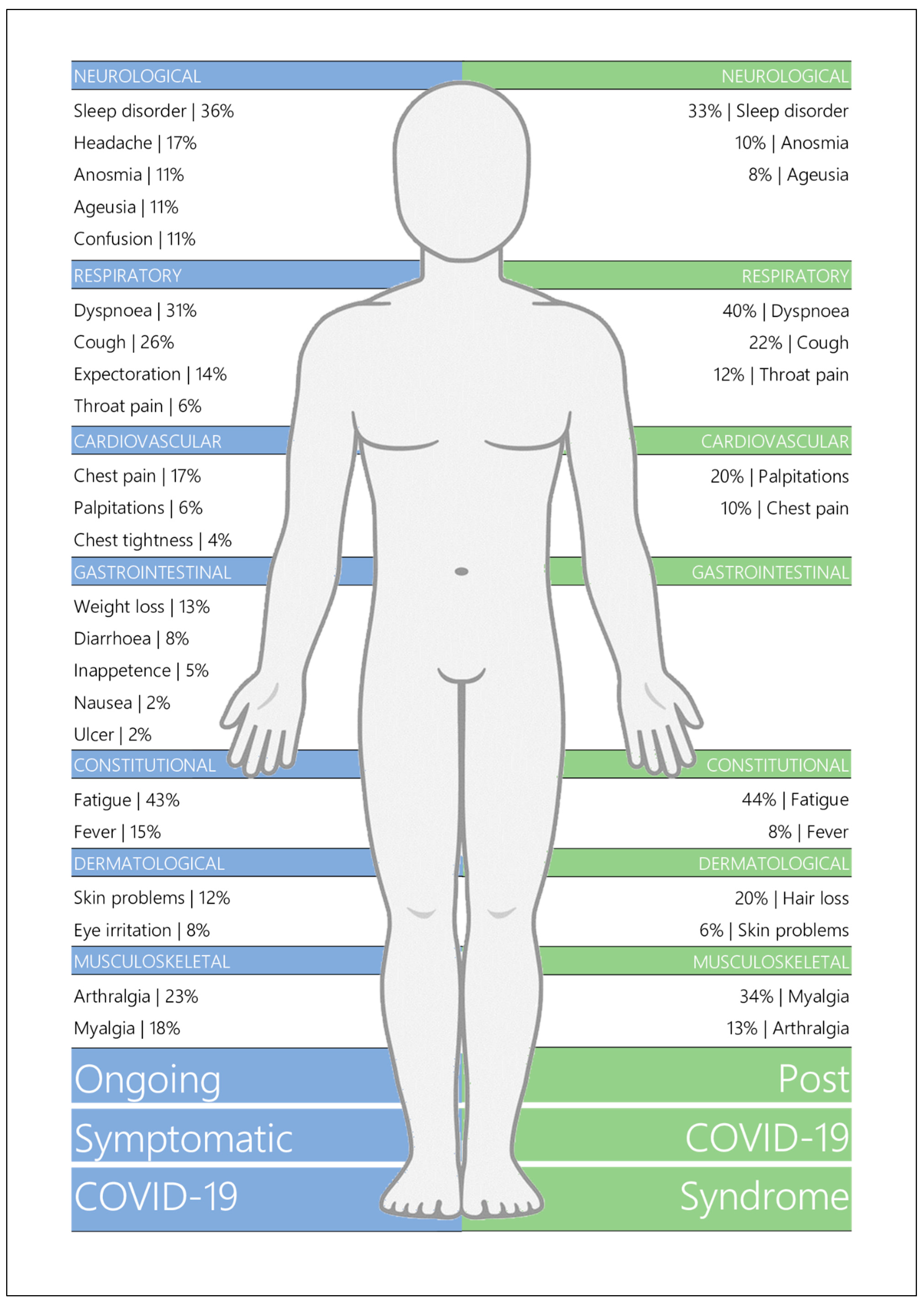
3.4. Symptomatology
3.4.1. Ongoing Symptomatic COVID-19
3.4.2. Post-COVID-19 Syndrome
3.5. Respiratory Functioning
3.5.1. Pulmonary Functioning
3.5.2. Lung Imaging
3.6. Cognitive Functioning
3.7. Mental Health & Quality of Life
4. Discussion
4.1. Statement of Principal Findings
4.2. Strengths and Weaknesses of the Study
4.3. Strengths and Weaknesses in Relation to Other Studies
4.4. Meaning of the Study
4.5. Unanswered Questions and Future Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. WHO Coronavirus (COVID-19) Dashboard: World Health Organisation. 2021. Available online: https://covid19.who.int/ (accessed on 5 December 2021).
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The Prevalence of Symptoms in 24,410 Adults Infected by the Novel Coronavirus (SARS-CoV-2; COVID-19): A Systematic Review and Meta-Analysis of 148 Studies from 9 Countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef]
- Pijls, B.G.; Jolani, S.; Atherley, A.; Derckx, R.T.; Dijkstra, J.I.R.; Franssen, G.H.L.; Hendriks, S.; Richters, A.; Venemans-Jellema, A.; Zalpuri, S.; et al. Demographic Risk Factors for COVID-19 Infection, Severity, ICU Admission and Death: A Meta-Analysis of 59 Studies. BMJ Open 2021, 11, e044640. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. COVID-19 Rapid Guideline: Managing COVID-19; NICE: London, UK, 2021. [Google Scholar]
- Amin-Chowdhury, Z.; Ladhani, S.N. Causation or Confounding: Why Controls Are Critical for Characterizing Long COVID. Nat. Med. 2021, 27, 1129–1130. [Google Scholar] [CrossRef]
- Jennings, G.; Romero-Ortuño, R.; Monaghan, A.; Xue, F. Long COVID: A Systematic Review of Chronic Fatigue and Other Persistent Symptoms Following Acute Phase Recovery: PROSPERO. 2021. Available online: www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021247846 (accessed on 1 March 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downes, M.J.; Brennan, M.; Williams, H.C.; Dean, R. Development of a Critical Appraisal Tool to Assess the Quality of Cross-Sectional Studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient Outcomes after Hospitalisation with COVID-19 and Implications for Follow-up: Results from a Prospective UK Cohort. Thorax 2020, 76, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Soddu, D.; Balbo, P.E.; Baricich, A.; Zeppegno, P.; Avanzi, G.C.; Baldon, G.; Bartolomei, G.; Battaglia, M.; Battistini, S.; et al. Respiratory and Psychophysical Sequelae among Patients with COVID-19 Four Months after Hospital Discharge. JAMA Netw. Open 2021, 4, e2036142. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K.; et al. Follow-up of Adults with Noncritical COVID-19 Two Months after Symptom Onset. Clin. Microbiol. Infect. 2020, 27, 258–263. [Google Scholar] [CrossRef]
- Cheng, D.; Calderwood, C.; Skyllberg, E.; Ainley, A. Clinical Characteristics and Outcomes of Adult Patients Admitted with COVID-19 in East London: A Retrospective Cohort Analysis. BMJ Open Respir. Res. 2021, 8, e000813. [Google Scholar] [CrossRef] [PubMed]
- Chopra, V.; Flanders, S.A.; O’Malley, M.; Malani, A.N.; Prescott, H.C. Sixty-Day Outcomes among Patients Hospitalized with COVID-19. Ann. Intern. Med. 2021, 174, 576–578. [Google Scholar] [CrossRef]
- Cortés-Telles, A.; López-Romero, S.; Figueroa-Hurtado, E.; Pou-Aguilar, Y.N.; Wong, A.W.; Milne, K.M.; Ryerson, C.J.; Guenette, J.A. Pulmonary Function and Functional Capacity in COVID-19 Survivors with Persistent Dyspnoea. Respir. Physiol. Neurobiol. 2021, 288, 103644. [Google Scholar] [CrossRef] [PubMed]
- Daher, A.; Balfanz, P.; Cornelissen, C.; Müller, A.; Bergs, I.; Marx, N.; Müller-Wieland, D.; Hartmann, B.; Dreher, M.; Müller, T. Follow up of Patients with Severe Coronavirus Disease 2019 (COVID-19): Pulmonary and Extrapulmonary Disease Sequelae. Respir. Med. 2020, 174, 106197. [Google Scholar] [CrossRef]
- D’Cruz, R.F.; Waller, M.D.; Perrin, F.; Periselneris, J.; Norton, S.; Smith, L.-J.; Patrick, T.; Walder, D.; Heitmann, A.; Lee, K.; et al. Chest Radiography Is a Poor Predictor of Respiratory Symptoms and Functional Impairment in Survivors of Severe COVID-19 Pneumonia. ERJ Open Res. 2020, 7, 00655-2020. [Google Scholar] [CrossRef]
- De Lorenzo, R.; Conte, C.; Lanzani, C.; Benedetti, F.; Roveri, L.; Mazza, M.G.; Brioni, E.; Giacalone, G.; Canti, V.; Sofia, V.; et al. Residual Clinical Damage after COVID-19: A Retrospective and Prospective Observational Cohort Study. PLoS ONE 2020, 15, e0239570. [Google Scholar] [CrossRef] [PubMed]
- Froidure, A.; Mahsouli, A.; Liistro, G.; De Greef, J.; Belkhir, L.; Gérard, L.; Bertrand, A.; Koenig, S.; Pothen, L.; Yildiz, H.; et al. Integrative Respiratory Follow-up of Severe COVID-19 Reveals Common Functional and Lung Imaging Sequelae. Respir. Med. 2021, 181, 106383. [Google Scholar] [CrossRef] [PubMed]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-Discharge Persistent Symptoms and Health-Related Quality of Life after Hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge Symptoms and Rehabilitation Needs in Survivors of COVID-19 Infection: A Cross-Sectional Evaluation. J. Med. Virol. 2020, 93, 1013–1022. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Huang, Y.; Tan, C.; Wu, J.; Chen, M.; Wang, Z.; Luo, L.; Zhou, X.; Liu, X.; Huang, X.; Yuan, S.; et al. Impact of Coronavirus Disease 2019 on Pulmonary Function in Early Convalescence Phase. Respir. Res. 2020, 21, 163. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, A.; Iqbal, K.; Ali, S.A.; Azim, D.; Farid, E.; Baig, M.D.; Bin Arif, T.; Raza, M. The COVID-19 Sequelae: A Cross-Sectional Evaluation of Post-recovery Symptoms and the Need for Rehabilitation of COVID-19 Survivors. Cureus 2021, 13, e13080. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, L.G.; Paleoudis, E.G.; Bari, D.L.-D.; Nyirenda, T.; Friedman, T.; Gupta, A.; Rasouli, L.; Zetkulic, M.; Balani, B.; Ogedegbe, C.; et al. Persistence of Symptoms and Quality of Life at 35 Days after Hospitalization for COVID-19 Infection. PLoS ONE 2020, 15, e0243882. [Google Scholar] [CrossRef]
- Lerum, T.V.; Aaløkken, T.M.; Brønstad, E.; Aarli, B.; Ikdahl, E.; Lund, K.M.A.; Durheim, M.T.; Rodriguez, J.R.; Meltzer, C.; Tonby, K.; et al. Dyspnoea, Lung Function and CT Findings Three Months after Hospital Admission for COVID-19. Eur. Respir. J. 2020, 57, 2003448. [Google Scholar] [CrossRef]
- Liang, L.; Yang, B.; Jiang, N.; Fu, W.; He, X.; Zhou, Y.; Ma, W.-L.; Wang, X. Three-Month Follow-Up Study of Survivors of Coronavirus Disease 2019 after Discharge. J. Korean Med. Sci. 2020, 35, e418. [Google Scholar] [CrossRef] [PubMed]
- Loerinc, L.B.; Scheel, A.M.; Evans, S.T.; Shabto, J.M.; O’Keefe, G.A.; O’Keefe, J.B. Discharge Characteristics and Care Transitions of Hospitalized Patients with COVID-19. Healthcare 2021, 9, 100512. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; Jarvis, H.C.; et al. ‘Long-COVID’: A Cross-Sectional Study of Persisting Symptoms, Biomarker and Imaging Abnormalities Following Hosptalisation for COVID-19. Thorax 2020, 76, 396–398. [Google Scholar] [CrossRef]
- Miyazato, Y.; Morioka, S.; Tsuzuki, S.; Akashi, M.; Osanai, Y.; Tanaka, K.; Terada, M.; Suzuki, M.; Kutsuna, S.; Saito, S.; et al. Prolonged and Late-Onset Symptoms of Coronavirus Disease 2019. Open Forum Infect. Dis. 2020, 7, ofaa507. [Google Scholar] [CrossRef]
- Mo, X.; Jian, W.; Su, Z.; Chen, M.; Peng, H.; Peng, P.; Lei, C.; Chen, R.; Zhong, N.; Li, S. Abnormal Pulmonary Function in COVID-19 Patients at Time of Hospital Discharge. Eur. Respir. J. 2020, 55, 2001217. [Google Scholar] [CrossRef]
- Moreno-Pérez, O.; Merino, E.; Leon-Ramirez, J.-M.; Andres, M.; Ramos, J.M.; Arenas-Jiménez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-Acute COVID-19 Syndrome. Incidence and Risk Factors: A Mediterranean Cohort Study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef]
- Osikomaiya, B.; Erinoso, O.; Wright, K.O.; Odusola, A.O.; Thomas, B.; Adeyemi, O.; Bowale, A.; Adejumo, O.; Falana, A.; Abdus-salam, I.; et al. ‘Long COVID’: Persistent COVID-19 Symptoms in Survivors Managed in Lagos State, Nigeria. BMC Infect. Dis. 2021, 21, 304. [Google Scholar] [CrossRef]
- Prieto, M.A.; Prieto, O.; Castro, H.M. Long COVID: Cross-Sectional Study. Rev. Fac. Cien. Med. Univ. Nac. Cordoba. 2021, 78, 33–36. [Google Scholar]
- Raman, B.; Cassar, M.P.; Tunnicliffe, E.M.; Filippini, N.; Griffanti, L.; Alfaro-Almagro, F.; Okell, T.; Sheerin, F.; Xie, C.; Mahmod, M.; et al. Medium-Term Effects of SARS-CoV-2 Infection on Multiple Vital Organs, Exercise Capacity, Cognition, Quality of Life and Mental Health, Post-Hospital Discharge. EClinicalMedicine 2021, 31, e100683. [Google Scholar] [CrossRef]
- Rosales-Castillo, A.; García de Los Ríos, C.; Mediavilla García, J.D. Persistent Symptoms after Acute COVID-19 Infection: Importance of Follow-up. Med. Clin. 2021, 156, 35–36. [Google Scholar] [CrossRef]
- Shah, A.S.; Wong, A.W.; Hague, C.J.; Murphy, D.T.; Johnston, J.C.; Ryerson, C.J.; Carlsten, C. A Prospective Study of 12-Week Respiratory Outcomes in COVID-19-Related Hospitalisations. Thorax 2020, 76, 402–404. [Google Scholar] [CrossRef]
- Simani, L.; Ramezani, M.; Darazam, I.A.; Sagharichi, M.; Aalipour, M.A.; Ghorbani, F.; Pakdaman, H. Prevalence and Correlates of Chronic Fatigue Syndrome and Post-Traumatic Stress Disorder after the Outbreak of the COVID-19. J. Neurovirol. 2021, 27, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Sykes, D.L.; Holdsworth, L.; Jawad, N.; Gunasekera, P.; Morice, A.H.; Crooks, M.G. Post-COVID-19 Symptom Burden: What Is Long-COVID and How Should We Manage It? Lung 2021, 199, 113–119. [Google Scholar] [CrossRef]
- Taboada, M.; Moreno, E.; Cariñena, A.; Rey, T.; Pita-Romero, R.; Leal, S.; Sanduende, Y.; Rodríguez, A.; Nieto, C.; Vilas, E.; et al. Quality of Life, Functional Status, and Persistent Symptoms after Intensive Care of COVID-19 Patients. Br. J. Anaesth. 2020, 126, e110–e113. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent Fatigue Following SARS-CoV-2 Infection Is Common and Independent of Severity of Initial Infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef]
- Venturelli, S.; Benatti, S.V.; Casati, M.; Binda, F.; Zuglian, G.; Imeri, G.; Conti, C.; Biffi, A.M.; Spada, M.S.; Bondi, E.; et al. Surviving COVID-19 in Bergamo Province: A Post-Acute Outpatient Re-Evaluation. Epidemiol. Infect. 2021, 149, E32. [Google Scholar] [CrossRef] [PubMed]
- Walle-Hansen, M.M.; Ranhoff, A.H.; Mellingsæter, M.; Wang-Hansen, M.S.; Myrstad, M. Health-Related Quality of Life, Functional Decline, and Long-Term Mortality in Older Patients Following Hospitalisation Due to COVID-19. BMC Geriatr. 2021, 21, 199. [Google Scholar] [CrossRef]
- Wang, X.; Xu, H.; Jiang, H.; Wang, L.; Lu, C.; Wei, X.; Liu, J.; Xu, S. Clinical Features and Outcomes of Discharged Coronavirus Disease 2019 Patients: A Prospective Cohort Study. QJM 2020, 113, 657–665. [Google Scholar] [CrossRef]
- Wong, A.W.; Shah, A.S.; Johnston, J.C.; Carlsten, C.; Ryerson, C.J. Patient-Reported Outcome Measures after COVID-19: A Prospective Cohort Study. Eur. Respir. J. 2020, 56, 2003276. [Google Scholar] [CrossRef]
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y.; Dong, W. Clinical Sequelae of COVID-19 Survivors in Wuhan, China: A Single-Centre Longitudinal Study. Clin. Microbiol. Infect. 2020, 27, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Liu, Y.; Xu, D.; Zhang, R.; Lan, L.; Xu, H. Prediction of the Development of Pulmonary Fibrosis Using Serial Thin-Section CT and Clinical Features in Patients Discharged after Treatment for COVID-19 Pneumonia. Korean J. Radiol. 2020, 21, 746–755. [Google Scholar] [CrossRef]
- Halpin, S.; O’Connor, R.; Sivan, M. Long COVID and Chronic COVID Syndromes. J. Med. Virol. 2020, 93, 1242–1243. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and Preliminary Testing of the New Five-Level Version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sleep, C.E.; Petty, J.A.; Wygant, D.B. Framing the Results: Assessment of Response Bias through Select Self-Report Measures in Psychological Injury Evaluations. Psychol. Inj. Law 2015, 8, 27–39. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-Acute COVID-19 Syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Mendelson, M.; Nel, J.; Blumberg, L.; Madhi, S.A.; Dryden, M.; Stevens, W.; Venter, F.W.D. Long-COVID: An Evolving Problem with an Extensive Impact. S. Afr. Med. J. 2020, 111, 10–12. [Google Scholar] [CrossRef]
- Rudroff, T.; Fietsam, A.C.; Deters, J.R.; Bryant, A.D.; Kamholz, J. Post-COVID-19 Fatigue: Potential Contributing Factors. Brain Sci. 2020, 10, 1012. [Google Scholar] [CrossRef]
- Mahase, E. Long Covid Could Be Four Different Syndromes, Review Suggests. BMJ 2020, 371, m3981. [Google Scholar] [CrossRef]
- Oronsky, B.; Larson, C.; Hammond, T.C.; Oronsky, A.; Kesari, S.; Lybeck, M.; Reid, T.R. A Review of Persistent Post-COVID Syndrome (PPCS). Clin. Rev. Allergy Immunol. 2021, 20, 1–9. [Google Scholar] [CrossRef]
- Cares-Marambio, K.; Montenegro-Jiménez, Y.; Torres-Castro, R.; Vera-Uribe, R.; Torralba, Y.; Alsina-Restoy, X.; Vasconcello-Castillo, L.; Vilaró, J. Prevalence of Potential Respiratory Symptoms in Survivors of Hospital Admission after Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis. Chronic Respir. Dis. 2021, 18. [Google Scholar] [CrossRef]
- Tancheva, L.; Petralia, M.C.; Miteva, S.; Dragomanova, S.; Solak, A.; Kalfin, R.; Lazarova, M.; Yarkov, D.; Ciurleo, R.; Cavalli, E.; et al. Emerging Neurological and Psychobiological Aspects of COVID-19 Infection. Brain Sci. 2020, 10, 852. [Google Scholar] [CrossRef]
- Rahman, A.; Niloofa, R.; De Zoysa, I.M.; Cooray, A.D.; Kariyawasam, J.; Seneviratne, S.L. Neurological Manifestations in COVID-19: A Narrative Review. SAGE Open Med. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Jarrahi, A.; Ahluwalia, M.; Khodadadi, H.; da Silva Lopes Salles, E.; Kolhe, R.; Hess, D.C.; Vale, F.; Kumar, M.; Baban, B.; Vaibhav, K.; et al. Neurological Consequences of COVID-19: What Have We Learned and Where Do We Go from Here? J. Neuroinflammation 2020, 17, 286. [Google Scholar] [CrossRef]
- Hadshiew, I.M.; Foitzik, K.; Arck, P.C.; Paus, R. Burden of Hair Loss: Stress and the Underestimated Psychosocial Impact of Telogen Effluvium and Androgenetic Alopecia. J. Investig. Dermatol. 2004, 123, 455–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Mill, J.G.; Hoogendijk, W.J.; Vogelzangs, N.; van Dyck, R.; Penninx, B.W. Insomnia and Sleep Duration in a Large Cohort of Patients with Major Depressive Disorder and Anxiety Disorders. J. Clin. Psychiatry 2010, 71, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Aguado, A.; García Del Álamo, M. Gastrointestinal Comorbidity and Symptoms Associated with Depression in Patients Aged over 60 Years. Semergen 2020, 46, 27–32. [Google Scholar] [CrossRef]
- Jowett, S.; Shevlin, M.; Hyland, P.; Karatzias, T. Posttraumatic Stress Disorder and Persistent Somatic Symptoms during the COVID-19 Pandemic: The Role of Sense of Threat. Psychosom. Med. 2020, 83, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Nehme, M.; Braillard, O.; Chappuis, F.; Courvoisier, D.S.; Guessous, I. Prevalence of Symptoms More Than Seven Months after Diagnosis of Symptomatic COVID-19 in an Outpatient Setting. Ann. Intern. Med. 2021, 174, 1252–1260. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Study Topic | Studies with participant data concerning long COVID symptomatology and/or general post-acute COVID-19 functioning. | N/A |
| Study Design | Cross-sectional studies, cohort studies, randomised control trials, and case-control studies. | Meta-analyses, systematic reviews, narrative reviews, clinical trials, case studies and series, opinion pieces, and non-peer reviewed publications. |
| Condition of Participants | Participants who tested positive for SARS-CoV-2 infection or were suspected of SARS-CoV-2 infection. | Participants recovered from acute COVID-19 (denoted as ≥4 weeks following symptom onset or hospital admission; immediately following discharge from hospital; or indicated as “recovered” by the respective researchers). |
| Sample Size | N/A | Studies with less than 30 participants. |
| Participant Age | N/A | Participants younger than 18 years of age |
| Participant Gender | N/A | Studies with a gender imbalance greater than 80:20%. |
| Other | N/A | Entire participant cohorts with a specific characteristic (e.g., only patients with anosmia). |
| First Author | Date | Country | N | Age (Years) | Gender (% Female) | Participant Hospital Status | Weeks from COVID Onset |
|---|---|---|---|---|---|---|---|
| Arnold [10] | 21 April | United Kingdom | 110 | M = 60 | 38% | Inpatient | 16 |
| Bellan [11] | 21 January | Italy | 238 | M = 61 | 40% | Inpatient (+ICU) | 21 |
| Carfi [12] | 20 July | Italy | 143 | = 57 | 37% | Inpatient (+ICU) | 9 |
| Carvalho-Schneider [13] | 20 October | France | 150 | = 49 | 56% | Mixed (−ICU) | 5|9 |
| Cheng [14] | 21 January | United Kingdom | 113 | M = 73 | 44% | Inpatient (+ICU) | 13 |
| Chopra [15] | 20 November | America | 488 | M = 62 | 48% | Inpatient (+ICU) | 13 |
| Cortés-Telles [16] | 20 June | Mexico | 186 | = 47 | 39% | Mixed | 9 |
| Daher [17] | 20 October | Germany | 33 | = 64 | 33% | Inpatient | 12 |
| D’Cruz [18] | 21 January | United Kingdom | 119 | = 59 | 38% | Inpatient (+ICU) | 13 |
| De Lorenzo [19] | 20 October | Italy | 185 | M = 57 | 34% | Mixed | 7 |
| Froidure [20] | 21 April | Belgium | 134 | M = 60 | 41% | Inpatient (+ICU) | 18 |
| Garrigues [21] | 20 August | France | 120 | = 63 | 37% | Mixed | 16 |
| Halpin [22] | 21 February | United Kingdom | 100 | R = 20–84 | 46% | Mixed | 11 |
| Huang [23] | 21 January | China | 1733 | M = 57 | 48% | Inpatient (+ICU) | 26 |
| Huang [24] | 20 June | China | 57 | = 47 | 54% | Inpatient | 8 |
| Iqbal [25] | 21 February | Pakistan | 158 | = 32 | 55% | Mixed | 7 |
| Jacobs [26] | 20 December | America | 183 | M = 57 | 38% | Inpatient | 4|6|7|9 |
| Lerum [27] | 21 April | Norway | 103 | M = 59 | 48% | Mixed | 12 |
| Liang [28] | 20 October | China | 76 | M = 41 | 72% | Inpatient (+ICU) | 5|13|17 |
| Loerinc [29] | 21 March | America | 310 | M = 58 | 51% | Inpatient (+ICU) | 4 |
| Mandal [30] | 20 September | United Kingdom | 384 | = 60 | 38% | Inpatient (+ICU) | 12 |
| Miyazato [31] | 20 October | Japan | 63 | = 48 | 33% | Inpatient | 9|17 |
| Mo [32] | 20 June | China | 110 | = 49 | 50% | Inpatient | 4 |
| Moreno-Perez [33] | 21 March | Spain | 277 | M = 62 | 47% | Mixed | 11 |
| Osikomaiya [34] | 21 March | Nigeria | 274 | = 42 | 34% | Outpatient | 6 |
| Prieto [35] | 21 March | Argentina | 85 | = 43 | 45% | Mixed | 8 |
| Raman [36] | 20 November | United Kingdom | 58 | = 55 | 41% | Inpatient (+ICU) | 10 |
| Rosales-Castillo [37] | 21 January | Spain | 118 | = 60 | 44% | Inpatient | 11 |
| Shah [38] | 21 March | Canada | 60 | M = 67 | 32% | Inpatient | 12 |
| Simani [39] | 21 February | Iran | 120 | = 55 | 33% | Inpatient (+ICU) | 30 |
| Sykes [40] | 21 April | United Kingdom | 134 | M = 58 | 34% | Mixed | 13|17|20|25 |
| Taboada [41] | 20 Decenber | Spain | 91 | = 66 | 35% | ICU | 30 |
| Townsend [42] | 20 November | Ireland | 128 | = 50 | 54% | Mixed | 14 |
| Venturelli [43] | 21 January | Italy | 767 | = 63 | 33% | Inpatient (+ICU) | 15 |
| Walle-Hansen [44] | 21 March | Norway | 106 | = 74 | 43% | Inpatient (+ICU) | 31 |
| Wang [45] | 20 May | China | 131 | M = 49 | 55% | Inpatient | 4|6|8 |
| Wong [46] | 20 November | Canada | 78 | = 62 | 36% | Inpatient | 13 |
| Xiong [47] | 20 September | China | 538 | M = 52 | 55% | Inpatient | 18 |
| Yu [48] | 20 March | China | 32 | M = 44 | 31% | Inpatient (+ICU) | 5 |
| Arnold et al. [10] | Bellan et al. [11] | Carfi et al. [12] | Carvalho-Schneider et al. [13] | Cheng et al. [14] | Chopra et al. [15] | Cortés-Telles et al. [16] | Daher et al. [17] | D’Cruz et al. [18] | De Lorenzo et al. [19] | Froidure et al. [20] | Garrigues et al. [21] | Halpin et al. [22] | Huang et al. [23] | Huang et al. [24] | Iqbal et al. [25] | Jacobs et al. [26] | Lerum et al. [27] | Liang et al. [28] | Loerinc et al. [29] | Mandal et al. [30] | Miyazato et al. [31] | Mo et al. [32] | Moreno-Perez et al. [33] | Osikomaiya et al. [34] | Prieto et al. [35] | Raman et al. [36] | Rosales-Castillo et al. [37] | Shah et al. [38] | Simani et al. [39] | Sykes et al. [40] | Taboada et al. [41] | Townsend et al. [42] | Venturelli et al. [43] | Walle-Hansen et al. [44] | Wang et al. [45] | Wong et al. [46] | Xiong et al. [47] | Yu et al. [48] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | N | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | Y | N | N | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | N | Y | N | Y | Y | N | Y | Y | Y | Y | Y |
| Q2 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q3 | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | Y | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| Q4 | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q5 | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q6 | Y | Y | Y | Y | Y | N | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q7 | Y | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | N | Y | N | N | N | N | N | Y | Y | Y | Y | Y | Y | N | Y | Y | N |
| Q8 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q9 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q10 | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | Y | Y | N | Y | Y |
| Q11 | Y | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q12 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q13 | N | N | N | N | N | N | Y | Y | N | N | N | N | N | N | N | Y | Y | Y | N | N | N | N | N | N | Y | Y | Y | Y | Y | Y | N | N | N | N | N | N | N | N | Y |
| Q14 | Y | Y | Y | Y | Y | Y | N | N | Y | N | Y | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | N | Y | N | N | N | N | N | Y | N | Y | Y | Y | Y | Y | Y | Y | N |
| Q15 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q16 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q17 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Q18 | Y | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y |
| Q19 | N | Y | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | Y | N | N | N | N | N | N | N | N | N | N | N |
| Q20 | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y |
| Ongoing Symptomatic COVID-19 | Post-COVID-19 Syndrome | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| SD | N | Min. | Max. | SD | N | Min. | Max. | |||
| Constitutional | ||||||||||
| Fatigue | 43% | 24 | 19 | 5% | 83% | 44% | 19 | 16 | 10% | 71% |
| Fever | 14% | 18 | 8 | 1% | 51% | 8% | 8 | 7 | 1% | 20% |
| Respiratory | ||||||||||
| Dyspnoea | 31% | 19 | 25 | 2% | 64% | 40% | 21 | 15 | 6% | 73% |
| Cough | 26% | 13 | 19 | 5% | 45% | 22% | 16 | 16 | 3% | 59% |
| Expectoration | 13% | 8 | 7 | 1% | 25% | - | - | - | - | - |
| Throat pain | 6% | 6 | 7 | 1% | 17% | 12% | 9 | 6 | 3% | 29% |
| Neurological | ||||||||||
| Sleep disorder | 36% | 25 | 5 | 10% | 69% | 33% | 13 | 11 | 18% | 57% |
| Headache | 17% | 8 | 10 | 4% | 36% | - | - | - | - | - |
| Anosmia | 11% | 7 | 9 | 2% | 21% | 10% | 3 | 8 | 5% | 13% |
| Ageusia | 11% | 9 | 8 | 1% | 25% | 8% | 4 | 7 | 2% | 15% |
| Confusion | 11% | 3 | 3 | 9% | 14% | - | - | - | - | - |
| Cardiovascular | ||||||||||
| Chest pain | 17% | 11 | 9 | 3% | 35% | 10% | 6 | 11 | 1% | 22% |
| Palpitations | 6% | 4 | 5 | 2% | 11% | 20% | 28 | 4 | 4% | 62% |
| Chest tightness | 4% | 3 | 3 | 1% | 6% | - | - | - | - | - |
| Gastrointestinal | ||||||||||
| Weight loss | 13% | 6 | 3 | 6% | 17% | - | - | - | - | - |
| Diarrhoea | 8% | 5 | 10 | 1% | 18% | - | - | - | - | - |
| Inappetence | 5% | 4 | 4 | 1% | 9% | - | - | - | - | - |
| Nausea | 2% | 2 | 5 | 1% | 6% | - | - | - | - | - |
| Ulcer | 2% | 1 | 3 | 1% | 3% | - | - | - | - | - |
| Musculoskeletal | ||||||||||
| Arthralgia | 23% | 13 | 7 | 10% | 48% | 13% | 11 | 4 | 6% | 29% |
| Myalgia | 18% | 10 | 9 | 1% | 32% | 34% | 31 | 9 | 2% | 86% |
| Dermatological | ||||||||||
| Skin problems | 12% | 4 | 3 | 8% | 15% | 6% | 4 | 4 | 3% | 12% |
| Eye irritation | 8% | 3 | 4 | 4% | 11% | - | - | - | - | - |
| Hair loss | - | - | - | - | - | 20% | 9 | 5 | 6% | 29% |
| Ongoing Symptomatic COVID-19 | Post-COVID-19 Syndrome | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| SD | N | Min. | Max. | SD | N | Min. | Max. | |||
| Pulmonary Functioning | ||||||||||
| FEV1 < 80% predicted | 15% | 5 | 5 | 9% | 21% | 11% | 6 | 4 | 5% | 17% |
| FVC < 80% predicted | 12% | 5 | 5 | 7% | 21% | 11% | 9 | 4 | 1% | 19% |
| FEV1/FVC < 0.7 | 6% | 4 | 4 | 1% | 11% | 7% | 1 | 3 | 6% | 8% |
| DLCO < 80% predicted | 44% | 14 | 4 | 24% | 53% | 32% | 11 | 4 | 20% | 46% |
| Chest Imaging | ||||||||||
| Abnormal pattern(s) | 34% | 25 | 5 | 2% | 60% | 28% | 17 | 5 | 13% | 53% |
| Ground-glass opacity | 28% | 29 | 3 | 1% | 59% | 24% | 26 | 6 | 2% | 67% |
| Fibrosis | 19% | 22 | 3 | 5% | 44% | 7% | 9 | 4 | 2% | 20% |
| Reticulation | - | - | - | - | - | 11% | 12 | 3 | 1% | 24% |
| Consolidation | - | - | - | - | - | 3% | 3 | 3 | 1% | 7% |
| Cognitive Impairments | ||||||||||
| Cognitive impairment | 20% | 11 | 5 | 2% | 28% | 15% | 6 | 5 | 5% | 22% |
| Concentration issues/Attention issues | - | - | - | - | - | 30% | 9 | 5 | 21% | 43% |
| Memory impairment | - | - | - | - | - | 35% | 16 | 6 | 6% | 48% |
| Psychological Disorder | ||||||||||
| Anxiety | 28% | 18 | 4 | 14% | 53% | 34% | 21 | 8 | 6% | 62% |
| Depression | 25% | 15 | 3 | 15% | 42% | 32% | 24 | 9 | 4% | 76% |
| Post-traumatic stress | - | - | - | - | - | 18% | 12 | 3 | 6% | 31% |
| Quality of Life | ||||||||||
| Decreased quality of life | 40% | 15 | 3 | 23% | 53% | 57% | 9 | 3 | 51% | 67% |
| Decrease in usual activities | - | - | - | - | - | 23% | 17 | 4 | 2% | 37% |
| Mobility issues | 51% | 15 | 3 | 37% | 67% | 32% | 25 | 3 | 7% | 56% |
| Pain or discomfort | - | - | - | - | - | 36% | 11 | 3 | 27% | 48% |
| Depression/Anxiety | - | - | - | - | - | 27% | 14 | 4 | 14% | 46% |
| Issues with self-care | - | - | - | - | - | 10% | 7 | 4 | 1% | 17% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jennings, G.; Monaghan, A.; Xue, F.; Mockler, D.; Romero-Ortuño, R. A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome. J. Clin. Med. 2021, 10, 5913. https://doi.org/10.3390/jcm10245913
Jennings G, Monaghan A, Xue F, Mockler D, Romero-Ortuño R. A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome. Journal of Clinical Medicine. 2021; 10(24):5913. https://doi.org/10.3390/jcm10245913
Chicago/Turabian StyleJennings, Glenn, Ann Monaghan, Feng Xue, David Mockler, and Román Romero-Ortuño. 2021. "A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome" Journal of Clinical Medicine 10, no. 24: 5913. https://doi.org/10.3390/jcm10245913