
Facilitators and Strategies for Breaking the News of an Intrauterine Death—A Mixed Methods Study among Obstetricians


Abstract
:1. Introduction
2. Materials and Methods
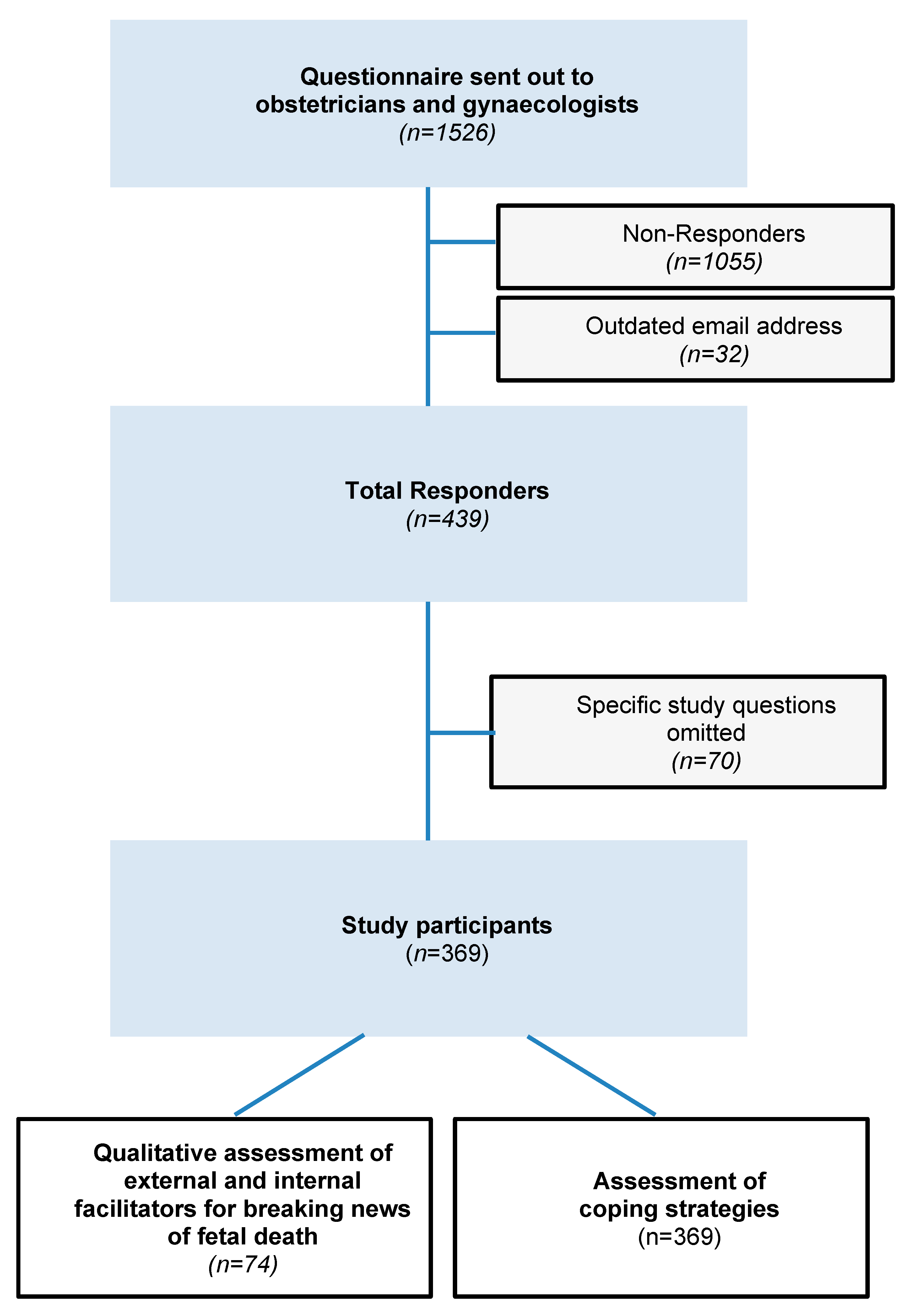
2.1. Data Collection
2.2. Measures
- Demographics
- Experience
- Stress Perception
- Coping Strategies
- Open Responses
2.3. Definitions
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Main Parameters
3.2.1. Experience
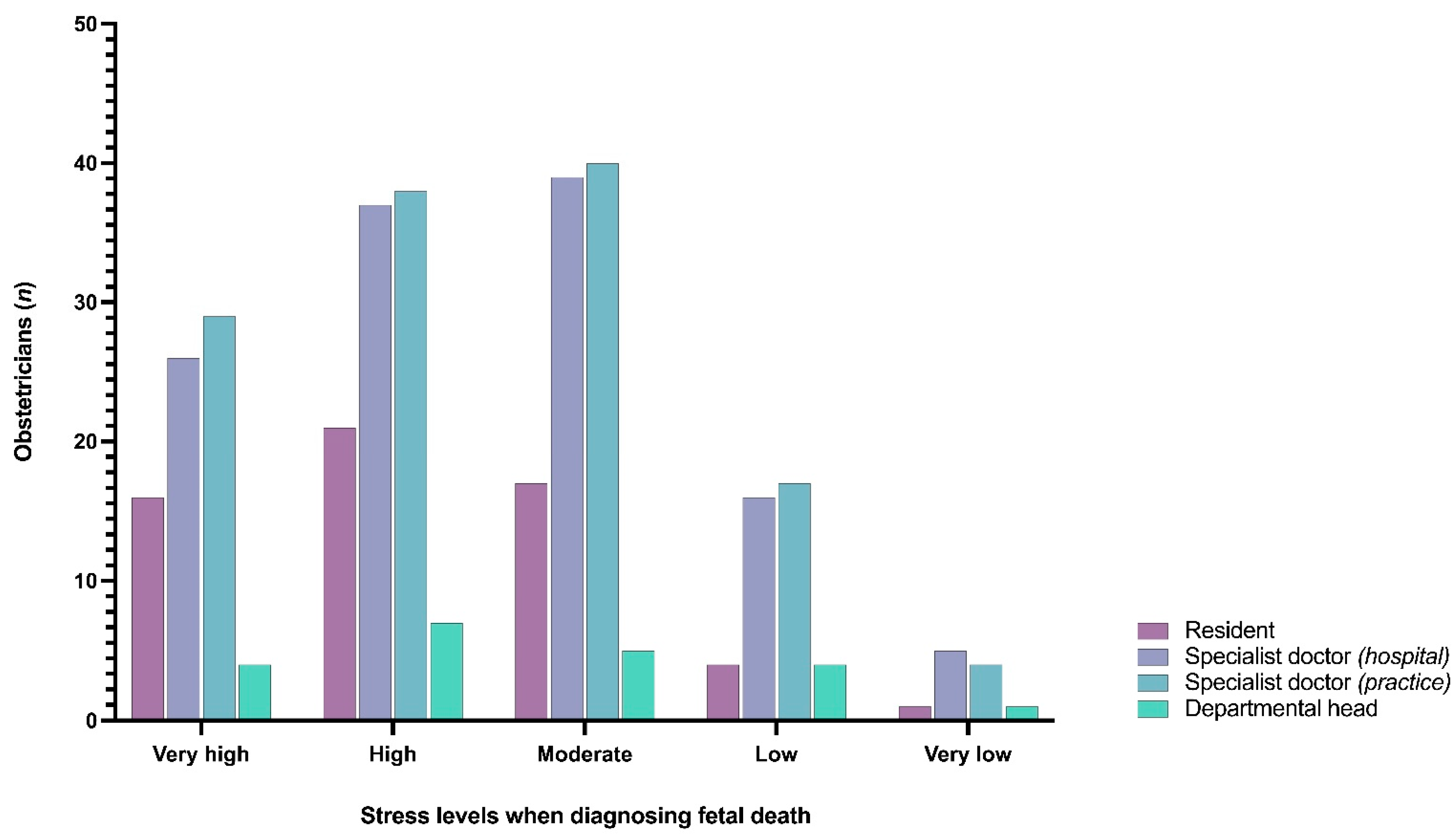
3.2.2. Stress
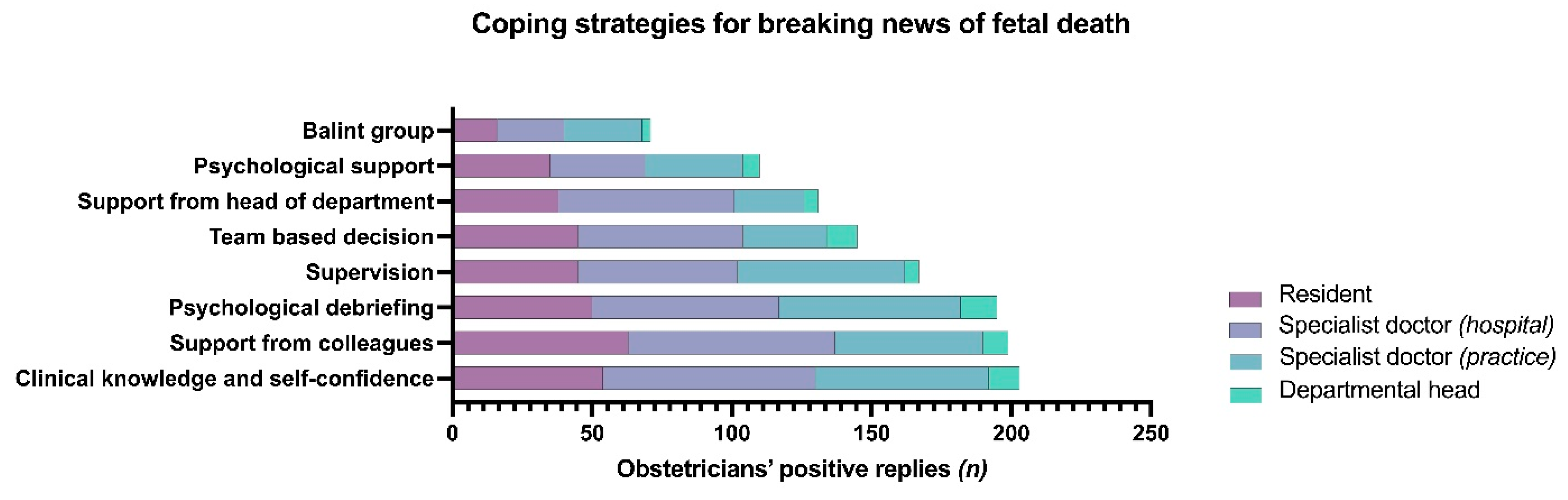
3.2.3. Coping Strategies for Breaking News of Fetal Death
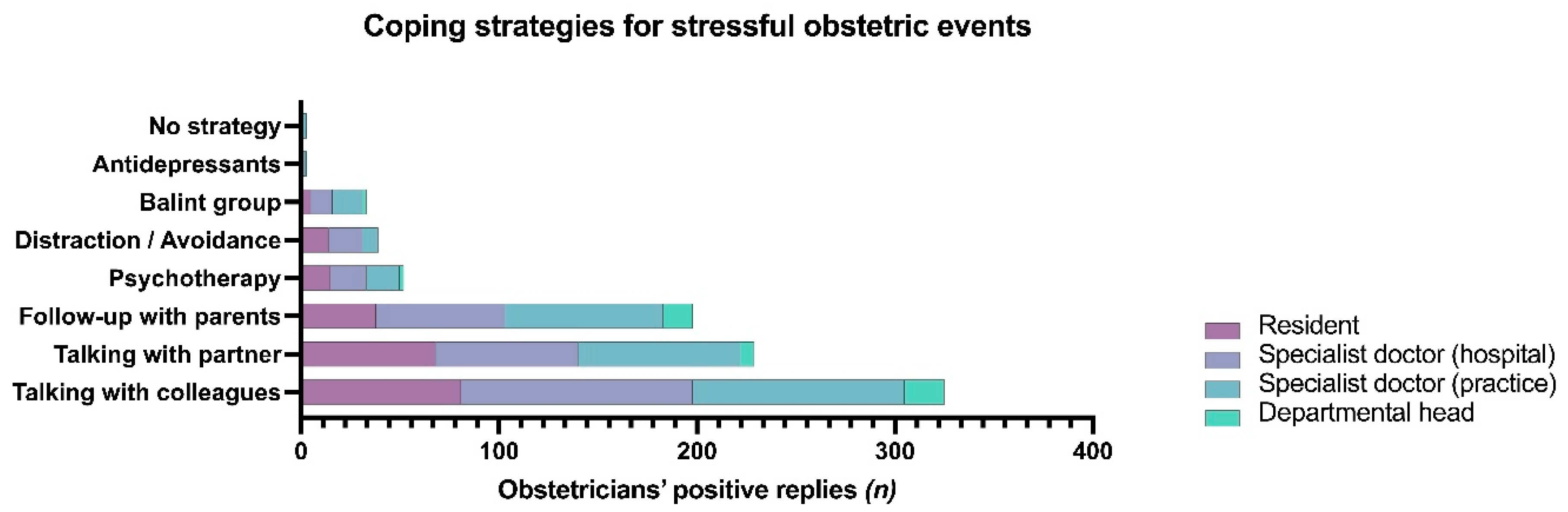
3.2.4. Coping Strategies in Stressful Obstetrical Events
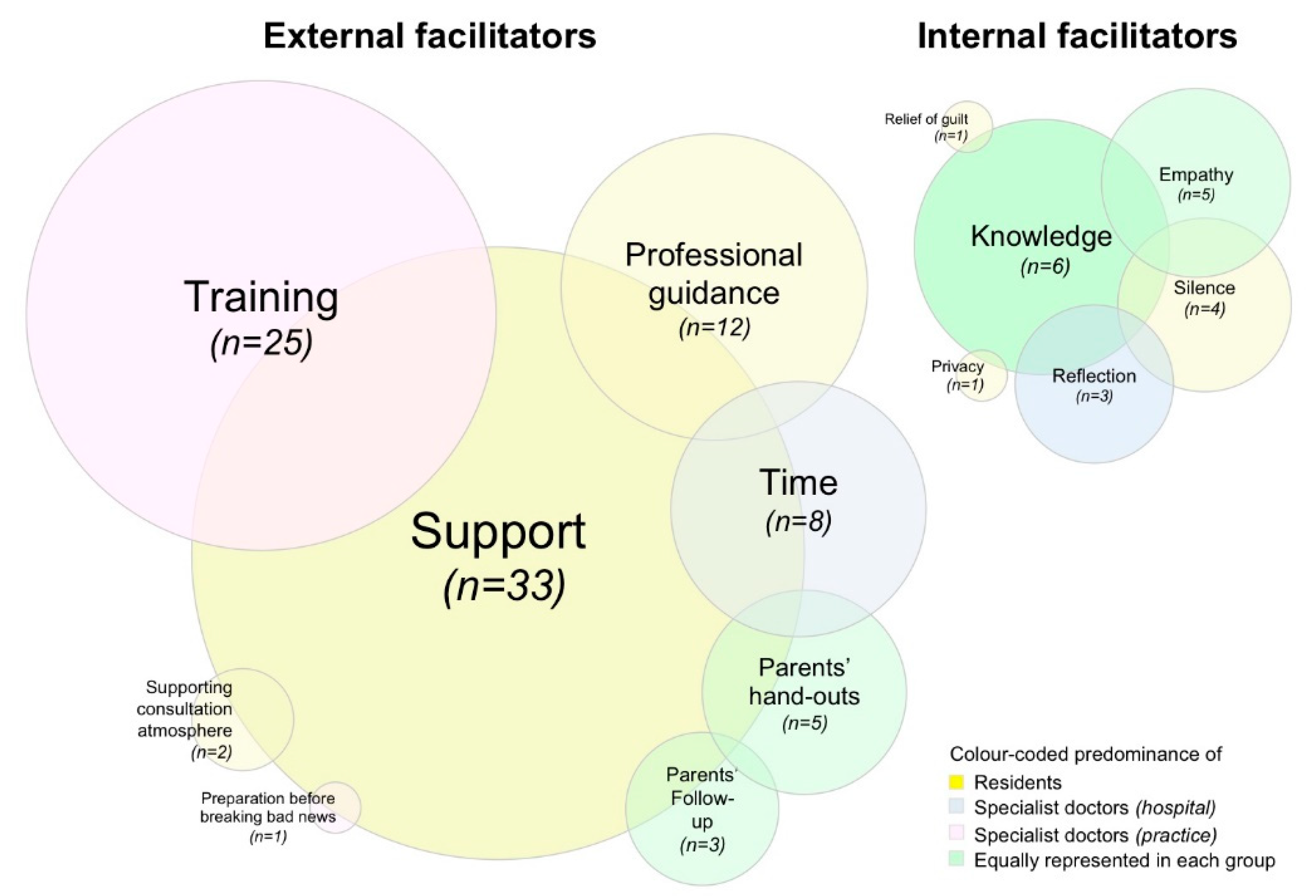
3.2.5. Facilitators for Delivering News of Fetal Death
4. Discussion
4.1. Main Findings
4.2. Results in the Context of What Is Known
4.3. Clinical Implications
4.4. Research Implications
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mohangoo, A.D.; Buitendijk, S.E.; Szamotulska, K.; Chalmers, J.; Irgens, L.M.; Bolumar, F.; Nijhuis, J.G.; Zeitlin, J. Gestational age patterns of fetal and neonatal mortality in Europe: Results from the Euro-Peristat project. PLoS ONE 2011, 6, e24727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuzum, D.; Meaney, S.; O’Donoghue, K. The impact of stillbirth on bereaved parents: A qualitative study. PLoS ONE 2018, 13, e0191635. [Google Scholar] [CrossRef]
- Nuzum, D.; Meaney, S.; O’Donoghue, K. The impact of stillbirth on consultant obstetrician gynaecologists: A qualitative study. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 1020–1028. [Google Scholar] [CrossRef]
- Nuzum, D.; Meaney, S.; O’Donoghue, K. The Place of Faith for Consultant Obstetricians Following Stillbirth: A Qualitative Exploratory Study. J. Relig. Health 2016, 55, 1519–1528. [Google Scholar] [CrossRef]
- Korteweg, F.J.; Gordijn, S.J.; Timmer, A.; Erwich, J.J.; Bergman, K.A.; Bouman, K.; Ravise, J.M.; Heringa, M.P.; Holm, J.P. The Tulip classification of perinatal mortality: Introduction and multidisciplinary inter-rater agreement. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Sharp, I.; Adeyeye, T.; Peacock, L.; Mahdi, A.; Farrant, K.; Sharp, A.N.; Greenwood, S.L.; Heazell, A.E.P. Investigation of the outcome of pregnancies complicated by increased fetal movements and their relation to underlying causes—A prospective cohort study. Acta Obstet. Et Gynecol. Scand. 2021, 100, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Ter Kuile, M.; Erwich, J.; Heazell, A.E.P. Stillbirths preceded by reduced fetal movements are more frequently associated with placental insufficiency: A retrospective cohort study. J. Perinat. Med. 2021. [Google Scholar] [CrossRef]
- Heazell, A.E.; McLaughlin, M.J.; Schmidt, E.B.; Cox, P.; Flenady, V.; Khong, T.Y.; Downe, S. A difficult conversation? The views and experiences of parents and professionals on the consent process for perinatal postmortem after stillbirth. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 987–997. [Google Scholar] [CrossRef] [PubMed]
- Gaab, J.; Rohleder, N.; Nater, U.M.; Ehlert, U. Psychological determinants of the cortisol stress response: The role of anticipatory cognitive appraisal. Psychoneuroendocrinology 2005, 30, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, C. Mental stress follows mental rules. J. Clin. Endocrinol. Metab. 1999, 84, 4292. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.H. A Multidimensional Approach to Individual Differences in Empathy. JSAS Cat. Sel. Doc. Psychol. 1980, 10, 85–104. [Google Scholar]
- Jakoby, N.J. Messung von internen und externen Kontrollüberzeugungen in allgemeinen Bevölkerungsumfragen. ZUMA Nachr. 1999, 23, 61–71. [Google Scholar]
- Rotter, J.B. Generalized expectancies for internal versus external control of reinforcement. Psychol. Monogr. 1966, 80, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkel, A.F.; Robinson, A.; Jones, A.A.; Squires, A.P. Physician resilience: A grounded theory study of obstetrics and gynaecology residents. Med. Educ. 2019, 53, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. What can “thematic analysis” offer health and wellbeing researchers? Int. J. Qual. Stud. Health Well-Being 2014, 9, 26152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Novel insights into patients’ life-worlds: The value of qualitative research. Lancet Psychiatry 2019, 6, 720–721. [Google Scholar] [CrossRef] [Green Version]
- Kelley, M.C.; Trinidad, S.B. Silent loss and the clinical encounter: Parents’ and physicians’ experiences of stillbirth-a qualitative analysis. BMC Pregnancy Childbirth 2012, 12, 137. [Google Scholar] [CrossRef] [Green Version]
- Nuzum, D.; Meaney, S.; O’Donohue, K. Communication skills in Obstetrics: What can we learn from bereaved parents? Ir. Med. J. 2017, 110, 512. [Google Scholar]
- Farrow, V.A.; Goldenberg, R.L.; Fretts, R.; Schulkin, J. Psychological impact of stillbirths on obstetricians. J. Matern.-Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obs. 2013, 26, 748–752. [Google Scholar] [CrossRef]
- Gold, K.J.; Kuznia, A.L.; Hayward, R.A. How physicians cope with stillbirth or neonatal death: A national survey of obstetricians. Obstet. Gynecol. 2008, 112, 29–34. [Google Scholar] [CrossRef]
- World Health Organization. Sexual and Reproductive Health and Research Including the Special Programme HRP. 2021. Available online: www.who.int/teams/sexual-and-reproductive-health-and-research/areas-of-work/maternal-and-perinatal-health/antenatal-care (accessed on 28 August 2021).
- Gardiner, P.A.; Kent, A.L.; Rodriguez, V.; Wojcieszek, A.M.; Ellwood, D.; Gordon, A.; Wilson, P.A.; Bond, D.M.; Charles, A.; Arbuckle, S.; et al. Evaluation of an international educational programme for health care professionals on best practice in the management of a perinatal death: IMproving Perinatal mortality Review and Outcomes Via Education (IMPROVE). BMC Pregnancy Childbirth 2016, 16, 376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frippiat, M. Les enquêtes par Internet en sciences sociales: Un état des lieux. Population 2010, 65, 309–338. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 369) | Resident (n = 88) | Specialist Doctor in Hospital (n = 129) | Departmental Head (n = 21) | Specialist Doctor in Private/Public Practice (n = 131) | p-Value | ||
|---|---|---|---|---|---|---|---|
| Age (n = 351) | (Median; min-max; in years) | 44 (24–67) | 31 (24–42) | 43 (26–66) | 57 (45–64) | 52 (26–67) | |
| Sex (n = 369) | Female | 282 (76.4%) | 80 (90.9%) | 99 (76.7%) | 5 (23.8%) | 98 (74.8%) | |
| Male | 87 (23.6%) | 8 (9.1%) | 30 (23.3%) | 16 (76.2%) | 33 (25.2%) | ||
| Marital status (n = 364) | Single | 52 (14.3%) | 17 (19.5%) | 24 (19.2%) | 2 (9.5%) | 9 (6.9%) | |
| Coupled | 71 (19.5%) | 34 (39.1%) | 19 (15.2%) | 1 (4.8%) | 17 (13%) | ||
| Married | 228 (62.6%) | 35 (40.2%) | 77 (61.6%) | 18 (85.7%) | 98 (74.8%) | ||
| Divorced | 13 (3.6%) | 1 (1.1%) | 5 (4.0%) | 0 (0.0%) | 7 (5.3%) | ||
| Parent (n = 367) | Yes | 253 (68.9%) | 31 (35.2%) | 97 (75.8%) | 19 (90.5%) | 106 (81.5%) | |
| No | 114 (31.1%) | 57 (64.8%) | 31 (24.2%) | 2 (9.5%) | 24 (18.5%) | ||
| Diagnosed IUFD (n) | 0 | 39 (10.6%) | 27 (30.7%) | 7 (5.4%) | 0 (0.0%) | 5 (3.8%) | χ2 (12; N = 369) = 114.821; p < 0.001 |
| <5 | 164 (44.4%) | 51 (58%) | 51 (39.5%) | 3 (14.3%) | 59 (45.0%) | ||
| 6–10 | 76 (20.6%) | 9 (10.2%) | 31 (24%) | 1 (4.8%) | 35 (26.7%) | ||
| 11–30 | 53 (14.4%) | 1 (1.1%) | 22 (17.1%) | 9 (42.9%) | 21 (16%) | ||
| >31 | 37 (10%) | 0 (0%) | 18 (14%) | 8 (38.1%) | 11 (8.4%) | ||
| Delivered diagnoses of IUFD (n) | 0 | 42 (11.4%) | 34 (38.6%) | 5 (3.9%) | 0 (0.0%) | 3 (2.3%) | χ2 (12; N = 369) = 147.043; p < 0.001 |
| <5 | 151 (40.9%) | 45 (51.1%) | 47 (36.4%) | 2 (9.5%) | 57 (43.5%) | ||
| 6–10 | 82 (22.2%) | 7 (8.0%) | 36 (27.9%) | 2 (9.5%) | 37 (28.2%) | ||
| 11–30 | 53 (14.4%) | 2 (2.3%) | 21 (16.3%) | 8 (38.1%) | 22 (16.8%) | ||
| >31 | 41 (11.1%) | 0 (0.0%) | 20 (15.5%) | 9 (42.9%) | 12 (9.2%) |
| External Facilitator (Listed per Frequency) | Exemplar Quotes (Translated from German to English) |
|---|---|
| Support | “To have the opportunity to talk to my colleagues regarding this situation” (Female resident, 24 y/o, single, diagnosed IUFDs < 5 times) |
| “To have support from experienced colleagues and professionals dealing with crisis-intervention” (Female 3rd year resident, 34 y/o, single, never diagnosed IUFD) | |
| “To know within the team what and how to break the bad news (with all residents, specialist doctors, midwives) and also debrief in this team after the consultation” (Female specialist doctor in private practice, 53 y/o, coupled; diagnosed IUFDs 6–10 times) | |
| Training | “To have continuous trainings and skills-and-drills simulation practice” (Female specialist doctor in private practice, 45 y/o, married; diagnosed IUFDs 11–30 times) |
| “This situation will always be terrible, whatever the circumstance. However, frequent courses help and foster reflective practice” (Female specialist doctor in public practice, 42 y/o; married, diagnosed IUFDs < 5 times) | |
| “To gain knowledge on how to handle these consultations by learning from experienced colleagues, psychologists, etc. You will never feel good during these consultations. It would be advisable to have predefined intern standards, on what needs to be checked post-mortem” (Male specialist doctor in public practice, 50 y/o, coupled; diagnosed IUFDs < 5 times) | |
| Professional guidance | “It would be helpful to have a short guidance or checklist with all points that have to be raised within such consultation and what needs to be considered” (Female 1st year resident, married, never diagnosed IUFD) |
| Time | “To have time during clinics, to be there for the patient and also for oneself to debrief after such consultation” (Female consultant, diagnosed IUFDs > 31 times) |
| Parents’ handouts | “Professional handouts and leaflets for the parents” (Female specialist doctor in pubic practice, 43 y/o; divorced, diagnosed IUFDs 6–19 times) |
| Parents’ follow-up | “It would be helpful to receive feedback from affected women to understand what went well or not so well during these consultations, and what they wished to be different next time” (Female consultant, 55 y/o; married, diagnosed IUFDs < 5 times) |
| Supporting consultation atmosphere | “To lead this consultation with another colleague, to be stronger together” (Female 6th year resident, 35 y/o; married, diagnosed IUFDs 6–10 times) |
| Preparation | “Briefing and debriefing: Being mentally and verbally prepared what to say and how to act” (Female specialist doctor in public practice, 35 y/o; married, diagnosed IUFDs 6–10 times) |
| Internal Facilitator (Listed per Frequency) | Exemplar Quotes (Translated from German to English) |
|---|---|
| Knowledge | “To know and understand what needs to be done after fetal death (e.g., genetic testing), to know what, when and how to take all necessary samples and tissues. To know how to advice and consult parents after the diagnosis.” (Female 2nd year resident, 31 y/o; coupled, diagnosed IUFDs < 5 times) |
| Empathy | “To be fully empathetic with the patient and be medically well trained and skilled” (Male specialist doctor in private practice, 62 y/o; married, diagnosed IUFDs 11–30 times) |
| Silence | “Time, silence and willingness to reflect for oneself after such event. Be centered and mindful.” (Female specialist doctor in public practice, 42 y/o; married, diagnosed IUFDs < 5 times) |
| Reflection | “This situation will always be terrible; regular training and reflection are helpful” (Female consultant, 42 y/o; married, diagnosed IUFDs 6–10 times) |
| Privacy | “Privacy; to have my other half by my side” (Female 1st year resident, 26 y/o; Single, diagnosed IUFDs < 5 times) |
| Relief of professional guilt | “Somebody to tell me that I am not responsible for the adverse outcome” (Female consultant, 38 y/o; coupled, diagnosed IUFDs > 31 times) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muin, D.A.; Erlacher, J.S.; Leutgeb, S.; Felnhofer, A. Facilitators and Strategies for Breaking the News of an Intrauterine Death—A Mixed Methods Study among Obstetricians. J. Clin. Med. 2021, 10, 5347. https://doi.org/10.3390/jcm10225347
Muin DA, Erlacher JS, Leutgeb S, Felnhofer A. Facilitators and Strategies for Breaking the News of an Intrauterine Death—A Mixed Methods Study among Obstetricians. Journal of Clinical Medicine. 2021; 10(22):5347. https://doi.org/10.3390/jcm10225347
Chicago/Turabian StyleMuin, Dana Anais, Janina Sophie Erlacher, Stephanie Leutgeb, and Anna Felnhofer. 2021. "Facilitators and Strategies for Breaking the News of an Intrauterine Death—A Mixed Methods Study among Obstetricians" Journal of Clinical Medicine 10, no. 22: 5347. https://doi.org/10.3390/jcm10225347