
Gender Disparities in Vascular Access and One-Year Mortality among Incident Hemodialysis Patients: An Epidemiological Study in Lazio Region, Italy

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Source of the Data
2.2. Study Population
2.3. Outcome and Follow-Up
2.4. Exposure
2.5. Co-Variates
2.5.1. Socio-Demographic and Clinical Variables
2.5.2. Care-Related Variables
2.5.3. Laboratory Findings
2.6. Statistical Analysis
2.6.1. Association between Gender and Type of Vascular Access
2.6.2. Association between Gender and 1-Year Mortality
3. Results
3.1. Association between Gender and Type of Vascular Access
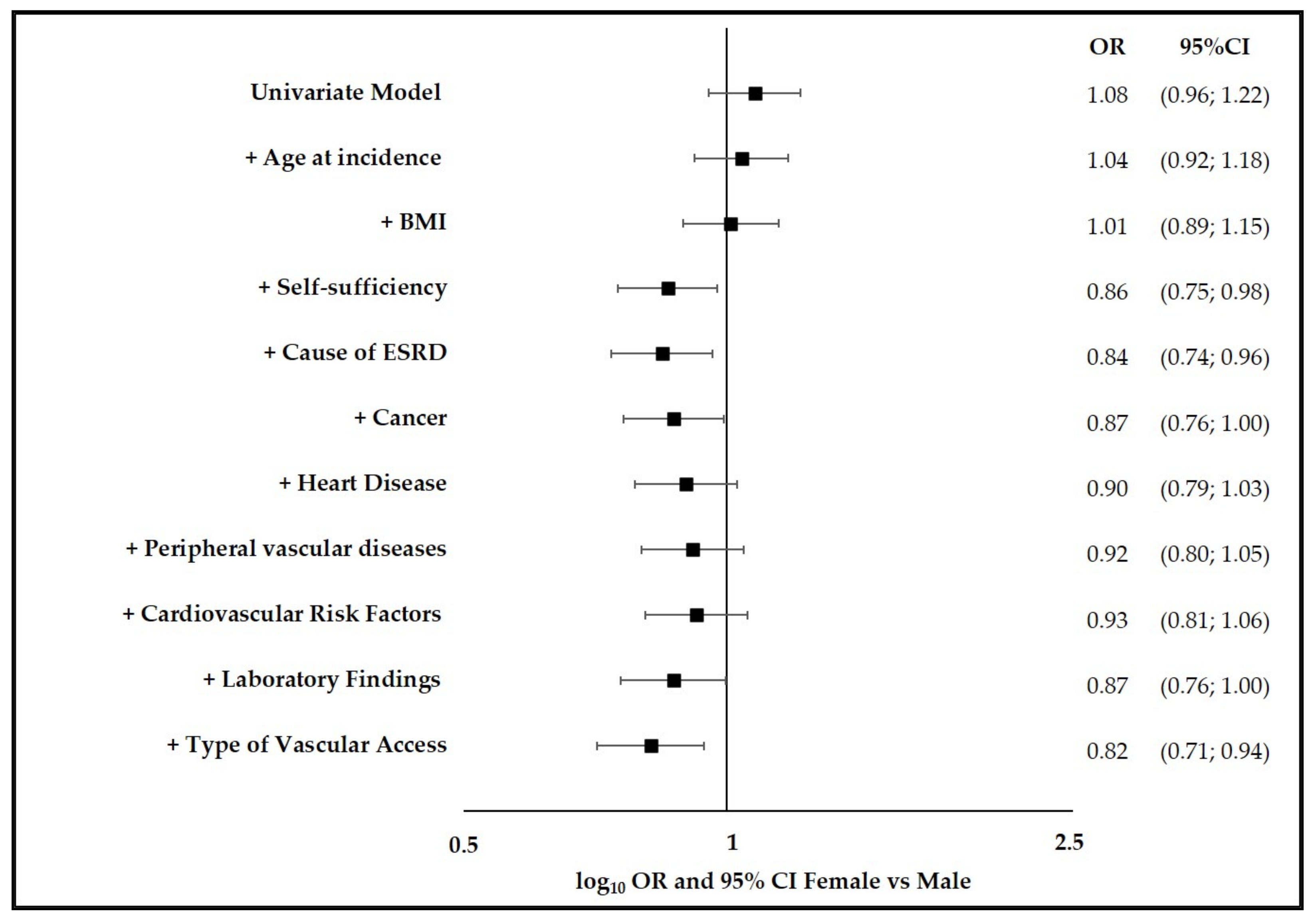
3.2. Association between Gender and 1-Year Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Saran, R.; Robinson, B.; Abbott, K.C.; Bragg-Gresham, J.; Chen, X.; Gipson, D.; Gu, H.; Hirth, R.A.; Hutton, D.; Jin, Y.; et al. US Renal Data System 2019 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2020, 75, A6–A7. [Google Scholar] [CrossRef] [PubMed]
- Marino, C.; Ferraro, P.M.; Bargagli, M.; Cascini, S.; Agabiti, N.; Gambaro, G.; Davoli, M. Prevalence of chronic kidney disease in the Lazio region, Italy: A clas-sification algorithm based on health information systems. BMC Nephrol. 2020, 21, 23. [Google Scholar] [CrossRef] [PubMed]
- Van De Luijtgaarden, M.W.; Jager, K.J.; Segelmark, M.; Pascual, J.; Collart, F.; Hemke, A.C.; Remón, C.; Metcalfe, W.; Miguel, A.; Kramar, R.; et al. Trends in dialysis modality choice and related patient survival in the ERA-EDTA Registry over a 20-year period. Nephrol. Dial. Transplant. 2015, 31, 120–128. [Google Scholar] [CrossRef] [Green Version]
- Cobo, G.; Hecking, M.; Port, F.K.; Exner, I.; Lindholm, B.; Stenvinkel, P.; Carrero, J.J. Sex and gender differences in chronic kidney disease: Progression to end-stage renal disease and haemodialysis. Clin. Sci. 2016, 130, 1147–1163. [Google Scholar] [CrossRef] [PubMed]
- Huxley, V.H. Sex and the cardiovascular system: The intriguing tale of how women and men regulate cardio-vascular function differently. Adv. Physiol. Educ. 2007, 31, 17–22. [Google Scholar] [CrossRef]
- Safford, M.M.; Brown, T.M.; Muntner, P.M.; Durant, R.W.; Glasser, S.P.; Halanych, J.H.; Shikany, J.M.; Prineas, R.J.; Samdarshi, T.E.; Bittner, V.A.; et al. Association of Race and Sex with Risk of Incident Acute Coronary Heart Disease Events. JAMA 2012, 308, 1768–1774. [Google Scholar] [CrossRef] [Green Version]
- Hecking, M.; Bieber, B.; Ethier, J.; Kautzky-Willer, A.; Sunder-Plassmann, G.; Säemann, M.D.; Ramirez, S.P.B.; Gillespie, B.W.; Pisoni, R.L.; Robinson, B.M.; et al. Sex-Specific Differences in Hemodialysis Prevalence and Practices and the Male-to-Female Mortality Rate: The Dialysis Outcomes and Practice Patterns Study (DOPPS). PLoS Med. 2014, 11, e1001750. [Google Scholar] [CrossRef] [Green Version]
- Carrero, J.J.; Hecking, M.; Chesnaye, N.C.; Jager, K.J. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 151–164. [Google Scholar] [CrossRef]
- Turin, T.C.; Tonelli, M.; Manns, B.J.; Ravani, P.; Ahmed, S.B.; Hemmelgarn, B.R. Chronic kidney disease and life expectancy. Nephrol. Dial. Transplant. 2012, 27, 3182–3186. [Google Scholar] [CrossRef] [Green Version]
- Stevens, L.A.; Coresh, J.; Greene, T.; Levey, A.S. Assessing kidney function—Measured and estimated glomerular filtration rate. N. Engl. J. Med. 2006, 354, 2473–2483. [Google Scholar] [CrossRef] [Green Version]
- Neugarten, J.; Acharya, A.; Silbiger, S.R. Effect of gender on the progression of nondiabetic renal disease: A meta-analysis. J. Am. Soc. Nephrol. 2000, 11, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, B.; Ingebretsen, O. The progression of chronic kidney disease: A 10-year population-based study of the effects of gender and age. Kidney Int. 2006, 69, 375–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halbesma, N.; Brantsma, A.H.; Bakker, S.J.; Jansen, D.F.; Stolk, R.P.; De Zeeuw, D.; De Jong, P.E.; Gansevoort, R.T.; for the PREVEND study group. Gender differences in predictors of the decline of renal function in the general population. Kidney Int. 2008, 74, 505–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crews, D.C.; Kuczmarski, M.F.; Miller, E.R., III.; Zonderman, A.B.; Evans, M.K.; Powe, N.R. Dietary habits, poverty, and chronic kidney disease in an urban population. J. Ren. Nutr. 2015, 25, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Ellam, T.; Fotheringham, J.; Kawar, B. Differential scaling of glomerular filtration rate and ingested metabolic burden: Implications for gender differences in chronic kidney disease outcomes. Nephrol. Dial. Transplant. 2014, 29, 1186–1194. [Google Scholar] [CrossRef] [Green Version]
- Nitsch, D. Is there a difference in metabolic burden between men and women? Nephrol. Dial. Transplant. 2014, 29, 1110–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitsch, D.; Grams, M.; Sang, Y.; Black, C.; Cirillo, M.; Djurdjev, O.; Iseki, K.; Jassal, S.K.; Kimm, H.; Kronenberg, F.; et al. Associations of estimated glomerular filtration rate and albuminuria with mortality and renal failure by sex: A meta-analysis. BMJ 2013, 346, f324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrero, J.J.; de Jager, D.J.; Verduijn, M.; Ravani, P.; De Meester, J.; Heaf, J.G.; Finne, P.; Hoitsma, A.J.; Pascual, J.; Jarraya, F.; et al. Cardiovascular and noncardiovascular mortality among men and women starting dialysis. Clin. J. Am. Soc. Nephrol. 2011, 6, 1722–1730. [Google Scholar] [CrossRef] [Green Version]
- Lok, C.E.; Huber, T.S.; Lee, T.; Shenoy, S.; Yevzlin, A.S.; Abreo, K.; Allon, M.; Asif, A.; Astor, B.C.; Glickman, M.H.; et al. KDOQI Vascular Access Guideline Work Group. KDOQI clinical practice guideline for vascular access: 2019 update. Am. J. Kidney Dis. 2020, 75 (Suppl. 2), S1–S164. [Google Scholar] [CrossRef] [Green Version]
- Caplin, N.; Sedlacek, M.; Teodorescu, V.; Falk, A.; Uribarri, J. Venous access: Women are equal. Am. J. Kidney Dis. 2003, 41, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Markell, M.; Brar, A.; Stefanov, D.G.; Salifu, M.O. Gender disparity in fistula use at initiation of hemodialysis varies markedly across ESRD networks-Analysis of USRDS data. Hemodial. Int. 2017, 22, 168–175. [Google Scholar] [CrossRef]
- Foley, R.N.; Chen, S.-C.; Collins, A.J. Hemodialysis access at initiation in the United States, 2005 to 2007: Still “Catheter First”. Hemodial. Int. 2009, 13, 533–542. [Google Scholar] [CrossRef] [PubMed]
- DeSilva, R.N.; Sandhu, G.S.; Garg, J.; Goldfarb-Rumyantzev, A.S. Association between initial type of hemodialysis access used in the elderly and mortality. Hemodial. Int. 2012, 16, 233–241. [Google Scholar] [CrossRef]
- Ravani, P.; Palmer, S.C.; Oliver, M.J.; Quinn, R.R.; MacRae, J.; Tai, D.J.; Pannu, N.I.; Thomas, C.; Hemmelgarn, B.R.; Craig, J.; et al. Associations between Hemodialysis Access Type and Clinical Outcomes: A Systematic Review. J. Am. Soc. Nephrol. 2013, 24, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.R.; Wasse, H.; Armistead, N.C.; McClellan, W.M. Achieving the goal of the Fistula First breakthrough initiative for prevalent maintenance hemodialysis patients. Am. J. Kidney Dis. 2011, 57, 78–89. [Google Scholar] [CrossRef] [Green Version]
- NKF-K/DOQI. Clinical Practice Guidelines for Vascular Access: Update 2000. Am. J. Kidney Dis. 2001, 37 (Suppl. 1), S137–S181. [Google Scholar] [CrossRef]
- Lok, C.E. Fistula First Initiative: Advantages and Pitfalls. Clin. J. Am. Soc. Nephrol. 2007, 2, 1043–1053. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Leonard, A.C.; Meganathan, K.; Christianson, A.L.; Thakar, C.V. Gender and Racial Disparities in Initial Hemodialysis Access and Outcomes in Incident End-Stage Renal Disease Patients. Am. J. Nephrol. 2018, 48, 4–14. [Google Scholar] [CrossRef]
- Zarkowsky, D.S.; Arhuidese, I.J.; Hicks, C.W.; Canner, J.K.; Qazi, U.; Obeid, T.; Schneider, E.; Abularrage, C.J.; Freischlag, J.A.; Malas, M.B. Racial/Ethnic Disparities Associated with Initial Hemodialysis Access. JAMA Surg. 2015, 150, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Registro Regionale Dialisi e Trapianto Lazio—RRDTL. Available online: https://www.deplazio.net/it/registro-dialisi-e-trapianto (accessed on 10 February 2020).
- Ifudu, O.; Paul, H.R.; Homel, P.; Friedman, E.A. Predictive value of functional status for mortality in patients on maintenance hemodialysis. Am. J. Nephrol. 1998, 18, 109–116. [Google Scholar] [CrossRef]
- Bossola, M.; On behalf of the Dialysis and Transplant Lazio Region Registry Scientific Committee; Marino, C.; Di Napoli, A.; Agabiti, N.; Tazza, L.; Davoli, M. Functional impairment and risk of mortality in patients on chronic hemodialysis: Results of the Lazio Dialysis Registry. J. Nephrol. 2018, 31, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Reddan, D.; Klassen, P.; Frankenfield, D.L.; Szczech, L.; Schwab, S.; Coladonato, J.; Rocco, M.; Lowrie, E.G.; Owen, W.F.; For the National ESRD CPM Work Group. National profile of practice patterns for hemodialysis vascular access in the United States. J. Am. Soc. Nephrol. 2002, 13, 2117–2124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Port, F.K.; Pisoni, R.L.; Bragg-Gresham, J.L.; Satayathum, S.S.; Young, E.W.; Wolfe, R.A.; Held, P.J. DOPPS Estimates of Patient Life Years Attributable to Modifiable Hemodialysis Practices in the United States. Blood Purif. 2004, 22, 175–180. [Google Scholar] [CrossRef]
- Tazza, L.; Angelici, L.; Marino, C.; Di Napoli, A.; Bossola, M.; De Cicco, C.; Davoli, M.; Agabiti, N. Determinants of venous catheter hemodialysis onset and subsequent switch to arteriovenous fistula: An epidemiological study in Lazio region. J. Vasc. Access 2021, 22, 749–758. [Google Scholar] [CrossRef]
- Sidawy, A.N.; Spergel, L.M.; Besarab, A.; Allon, M.; Jennings, W.C.; Padberg, F.T., Jr.; Murad, M.H.; Montori, V.; O’Hare, A.M.; Calligaro, K.D.; et al. The Society for Vascular Surgery: Clinical practice guidelines for the surgical placement and maintenance of arteriovenous hemodialysis access. J. Vasc. Surg. 2008, 48, S2–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidli, J.; Widmer, M.K.; Basile, C.; de Donato, G.; Gallieni, M.; Gibbons, C.P.; Haage, P.; Hamilton, G.; Hedin, U.; Kamper, L.; et al. Vascular access: 2018 clinical practice guidelines of the European society for vascular surgery (ESVS). Eur. J. Vasc. Endovasc Surg. 2018, 55, 757–818. [Google Scholar]
- Gameiro, J.; Ibeas, J. Factors affecting arteriovenous fistula dysfunction: A narrative review. J. Vasc. Access 2019, 21, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Pirozzi, N.; Mancianti, N.; Scrivano, J.; Fazzari, L.; Pirozzi, R.; Tozzi, M. Monitoring the Patient Following Radio-Cephalic Arteriovenous Fistula Creation: Current Perspectives. Vasc. Health Risk Manag. 2021, 17, 111–121. [Google Scholar] [CrossRef]
- Lee, T.; Barker, J.; Allon, M. Associations with predialysis vascular access management. Am. J. Kidney Dis. 2004, 43, 1008–1013. [Google Scholar] [CrossRef]
- Miller, C.D.; Robbin, M.L.; Allon, M. Gender differences in outcomes of arteriovenous fistulas in hemodialysis patients. Kidney Int. 2003, 63, 346–352. [Google Scholar] [CrossRef] [Green Version]
- Wachterman, M.W.; O’Hare, A.M.; Rahman, O.-K.; Lorenz, K.A.; Marcantonio, E.R.; Alicante, G.K.; Kelley, A.S. One-Year Mortality After Dialysis Initiation Among Older Adults. JAMA Intern. Med. 2019, 179, 987–990. [Google Scholar] [CrossRef]
- Saeed, F.; Arrigain, S.; Schold, J.D.; Nally, J.V., Jr.; Navaneethan, S.D. What are the Risk Factors for One-Year Mortality in Older Patients with Chronic Kidney Disease? An Analysis of the Cleveland Clinic CKD Registry. Nephron 2018, 141, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Mauri, J.M.; Clèries, M.; Vela, E.; Catalan Renal Registry. Design and validation of a model to predict early mortality in haemodialysis patients. Nephrol. Dial. Transplant. 2008, 23, 1690–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradbury, B.D.; Fissell, R.B.; Albert, J.; Anthony, M.S.; Critchlow, C.W.; Pisoni, R.L.; Port, F.K.; Gillespie, B.W. Predictors of Early Mortality among Incident US Hemodialysis Patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Clin. J. Am. Soc. Nephrol. 2006, 2, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Leonard, A.C.; Meganathan, K.; Christianson, A.L.; Thakar, C.V. Temporal Trends in Incident Mortality in Dialysis Patients: Focus on Sex and Racial Disparities. Am. J. Nephrol. 2019, 49, 241–253. [Google Scholar] [CrossRef]
- Brown, R.S.; Patibandla, B.K.; Goldfarb-Rumyantzev, A.S. The Survival Benefit of “Fistula First, Catheter Last” in Hemodialysis Is Primarily Due to Patient Factors. J. Am. Soc. Nephrol. 2016, 28, 645–652. [Google Scholar] [CrossRef] [Green Version]
- Mills, K.T.; Xu, Y.; Zhang, W.; Bundy, J.; Chen, C.-S.; Kelly, T.N.; Chen, J.; He, J. A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int. 2015, 88, 950–957. [Google Scholar] [CrossRef] [Green Version]
- Veronesi, G.; Ferrario, M.M.; Chambless, L.E.; Sega, R.; Mancia, G.; Corrao, G.; Fornari, C.; Cesana, G. Gender differences in the association between education and the incidence of cardiovascular events in Northern Italy. Eur. J. Public Health 2010, 21, 762–767. [Google Scholar] [CrossRef]
- Kausz, A.T.; Obrador, G.; Arora, P.; Ruthazer, R.; Levey, A.S.; Pereira, B.J.G. Late Initiation of Dialysis among Women and Ethnic Minorities in the United States. J. Am. Soc. Nephrol. 2000, 11, 2351–2357. [Google Scholar] [CrossRef]
- Tokars, J.I.; Light, P.; Anderson, J.; Miller, E.R.; Parrish, J.; Armistead, N.; Jarvis, W.R.; Gehr, T. A prospective study of vascular access infections at seven outpatient hemodialysis centers. Am. J. Kidney Dis. 2001, 37, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- De Nicola, L.; Donfrancesco, C.; Minutolo, R.; Lo Noce, C.; Palmieri, L.; De Curtis, A.; Iacoviello, L.; Zoccali, C.; Gesualdo, L.; Conte, G.; et al. Prevalence and cardiovascular risk profile of chronic kidney disease in Italy: Results of the 2008-12 National Health Examination Survey. Nephrol. Dial. Transplant. 2015, 30, 806–814. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| GENDER | |||||||
|---|---|---|---|---|---|---|---|
| MALE | FEMALE | Total | p-Value * | ||||
| n | % | n | % | n | |||
| Total | 5868 | 100.0 | 3200 | 100.0 | 9068 | ||
| Age class | (years) | 0.003 | |||||
| 18–49 | 714 | 12.2 | 380 | 11.9 | 1094 | ||
| 50–64 | 1260 | 21.5 | 674 | 21.1 | 1934 | ||
| 65–74 | 1595 | 27.2 | 793 | 24.8 | 2388 | ||
| 75–84 | 1816 | 31.0 | 1021 | 31.9 | 2837 | ||
| 85+ | 483 | 8.2 | 332 | 10.4 | 815 | ||
| Age (years) mean ± std | 5868 | 68.1 ± 14.1 | 3200 | 68.5 ± 14.7 | 9068 | 0.124 | |
| Education qualification | <0.001 | ||||||
| No qualifications/Elementary School/Middle School | 3627 | 61.8 | 2353 | 73.5 | 5980 | ||
| High School/Degree and more | 2241 | 38.2 | >847 | >26.5 | >3088 | ||
| Body Mass Index | <0.001 | ||||||
| Underweight (BMI < 18.0) | 208 | 3.5 | 283 | 8.8 | 491 | ||
| Normal weight (18.0 ≤ BMI < 25.0) | 3071 | 52.3 | 1561 | 48.8 | 4632 | ||
| Overweight (25.0 ≤ BMI < 30.0) | 1884 | 32.1 | 797 | 24.9 | 2681 | ||
| Obese (BMI ≥ 30.0) | >705 | >12.0 | >559 | >17.5 | >1264 | ||
| Self-sufficient | <0.001 | ||||||
| Complete | 2955 | 50.4 | 1289 | 40.3 | 4244 | ||
| Little self-sufficient | 1692 | 28.8 | 943 | 29.5 | 2635 | ||
| Not self-sufficient | 1221 | 20.8 | 968 | 30.3 | 2189 | ||
| Comorbidities | |||||||
| Heart disease | 2313 | 39.4 | 980 | 30.6 | 3293 | <0.001 | |
| Peripheral vascular diseases | 988 | 16.8 | 335 | 10.5 | 1323 | <0.001 | |
| Cerebrovascular disease | 866 | 14.8 | 385 | 12.0 | 1251 | <0.001 | |
| Chronic obstructive pulmonary disease | 915 | 15.6 | 372 | 11.6 | 1287 | <0.001 | |
| Cancer | 770 | 13.1 | 336 | 10.5 | 1106 | <0.001 | |
| Lipid metabolism’s alteration | 392 | 6.7 | 226 | 7.1 | 618 | 0.490 | |
| Neurological disease | 159 | 2.7 | 126 | 3.9 | 285 | 0.001 | |
| Cardiovascular Risk Factors (Hypertension, Obesity, Diabetes) | 4516 | 77.0 | 2545 | 79.5 | 7061 | 0.005 | |
| Vascular access | <0.001 | ||||||
| AVF | 3078 | 52.5 | 1344 | 42.0 | 4422 | ||
| CVC | >2790 | >47.6 | >1856 | >58.0 | >4646 | ||
| Type of dialysis unit | 0.653 | ||||||
| Public | 2201 | 37.5 | 1185 | 37.0 | 3386 | ||
| Private | 3667 | 62.5 | 2015 | 63.0 | 5682 | ||
| Pre-dialysis counselling | 0.052 | ||||||
| Yes | 4386 | 74.7 | 2448 | 76.5 | 6834 | ||
| No | 1482 | 25.3 | 750 | 23.4 | 2232 | ||
| Laboratory findings, mean ± std | n | mean ± std | n | mean ± std | Total | p-value | |
| Serum creatinine (mg/dL) | 5849 | 7.0 ± 2.3 | 3195 | 6.2 ± 2.0 | 9044 | <0.001 | |
| Hb (g/dL) | 5865 | 10.3 ± 1.4 | 3198 | 10.1 ± 1.4 | 9063 | <0.001 | |
| CPK (U/L) | 5868 | 8.7 ± 0.8 | 3200 | 8.7 ± 0.8 | 9068 | 0.009 | |
| Serum phosphate level (mg/dL) | 5822 | 5.0 ± 1.4 | 3169 | 5.0 ± 1.4 | 8991 | 0.023 | |
| Serum albumin (g/L) | 5840 | 3.6 ± 0.5 | 3185 | 3.5 ± 0.5 | 9025 | <0.001 | |
| AVF | CVC | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | N (%) | N (%) | Univariable Model | Multivariable Model * | |||||||
| Gender | Estimate | 95% CI | p-Value | Estimate | 95% CI | p-Value | |||||
| Male | 5868 | 3078 (52.5) | 2790 (47.6) | _ | _ | _ | _ | _ | _ | _ | _ |
| Female | 3200 | 1344 (42.0) | 1856 (58.0) | 0.656 | 0.602 | 0.716 | <0.001 | 0.667 | 0.606 | 0.733 | <0.001 |
| 1 YEAR DEATH | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Dead | Alive | Total | p-Value * | ||||||
| n | %col | %row | n | %col | %row | n | |||
| Total | 1354 | 100 | 16.5 | 6861 | 100 | 83.5 | 8215 | ||
| Gender | 0.2205 | ||||||||
| Males | 855 | 63.2 | 16.1 | 4452 | 64.9 | 83.9 | 5307 | ||
| Females | 499 | 36.9 | 17.2 | 2409 | 35.1 | 82.8 | 2908 | ||
| Age (years) mean ± std | 1354 | 74.8 ± 10.9 | 6861 | 67.0 ± 14.5 | 8215 | ||||
| Age class | (years) | <0.001 | |||||||
| 19–49 | 45 | 3.3 | 4.6 | 939 | 13.7 | 95.4 | 984 | ||
| 50–64 | 172 | 12.7 | 9.8 | 1576 | 23 | 90.2 | 1748 | ||
| 65–74 | 327 | 24.2 | 15.1 | 1835 | 26.8 | 84.9 | 2162 | ||
| 75–84 | 583 | 43.1 | 22.4 | 2019 | 29.4 | 77.6 | 2602 | ||
| 85+ | 227 | 16.8 | 31.6 | 492 | 7.2 | 68.4 | 719 | ||
| Education qualification | <0.001 | ||||||||
| No qualifications/Elementary School/Middle School | 992 | 73.3 | 18.2 | 4446 | 64.8 | 81.8 | 5438 | ||
| High School/Degree and more | 362 | 26.7 | 13 | 2415 | 35.2 | 87 | 2777 | ||
| Body Mass Index | <0.001 | ||||||||
| Underweight (BMI < 18.0) | 118 | 8.7 | 26.8 | 323 | 4.7 | 73.2 | 441 | ||
| Normal weight (18.0 ≤ BMI < 25.0) | 743 | 54.9 | 17.7 | 3449 | 50.3 | 82.3 | 4192 | ||
| Overweight (25.0 ≤ BMI < 30.0) | 357 | 26.4 | 14.7 | 2079 | 30.3 | 85.3 | 2436 | ||
| Obese (BMI ≥ 30.0) | 136 | 10 | 11.9 | 1010 | 14.7 | 88.1 | 1146 | ||
| Self-sufficient | <0.001 | ||||||||
| Complete | 247 | 18.2 | 6.6 | 3510 | 51.2 | 93.4 | 3757 | ||
| Little self-sufficient | 397 | 29.3 | 16.2 | 2049 | 29.9 | 83.8 | 2446 | ||
| Not self-sufficient | 710 | 52.4 | 35.3 | 1302 | 19 | 64.7 | 2012 | ||
| Cause of ESRD | <0.001 | ||||||||
| Unknown | 388 | 28.7 | 18.9 | 1668 | 24.3 | 81.1 | 2056 | ||
| Diabetic nephropathy | 318 | 23.5 | 17.1 | 1542 | 22.5 | 82.9 | 1860 | ||
| Renal vascular disease | 320 | 23.6 | 16.4 | 1629 | 23.7 | 83.6 | 1949 | ||
| Glomerulonephritis | 45 | 3.3 | 7 | 602 | 8.8 | 93 | 647 | ||
| Interstitial nephritis, toxic/pyelonephritis | 94 | 6.9 | 20.1 | 374 | 5.5 | 79.9 | 468 | ||
| Other nephropathies | 74 | 5.5 | 20.7 | 284 | 4.1 | 79.3 | 358 | ||
| Systemic disease | 83 | 6.1 | 28.5 | 208 | 3 | 71.5 | 291 | ||
| Cystic renal disease/familial nephropathy | 28 | 2.1 | 5.1 | 523 | 7.6 | 94.9 | 551 | ||
| Renal malformation | 4 | 0.3 | 11.4 | 31 | 0.5 | 88.6 | 35 | ||
| Comorbidities | |||||||||
| Heart disease | 683 | 50.4 | 22.7 | 2326 | 33.9 | 77.3 | 3009 | <0.001 | |
| Peripheral vascular diseases | 242 | 17.9 | 25.9 | 692 | 10.1 | 74.1 | 934 | <0.001 | |
| Cerebrovascular disease | 157 | 11.6 | 24.7 | 478 | 7 | 75.3 | 635 | <0.001 | |
| Chronic obstructive pulmonary disease | 289 | 21.3 | 24.7 | 882 | 12.9 | 75.3 | 1171 | <0.001 | |
| Cancer | 274 | 20.2 | 28.1 | 702 | 10.2 | 71.9 | 976 | <0.001 | |
| Lipid metabolism’s alteration | 71 | 5.2 | 12.8 | 484 | 7.1 | 87.2 | 555 | 0.0153 | |
| Neurological disease | 79 | 5.8 | 30 | 184 | 2.7 | 70 | 263 | <0.001 | |
| Cardiovascular Risk Factors (Hypertension, Obesity, Diabetes) | 944 | 69.7 | 14.9 | 5414 | 78.9 | 85.2 | 6358 | <0.001 | |
| Vascular access | <0.001 | ||||||||
| FAV | 1043 | 77 | 25.1 | 3115 | 45.4 | 74.9 | 4158 | ||
| CVC | 311 | 23 | 7.7 | 3746 | 54.6 | 92.3 | 4057 | ||
| Type of dialysis unit | 0.2191 | ||||||||
| Public hospital | 524 | 38.7 | 17.1 | 2534 | 36.9 | 82.9 | 3058 | ||
| Private clinic | 830 | 61.3 | 16.1 | 4327 | 63.1 | 83.9 | 5157 | ||
| Pre-dialysis counselling | 0.0003 | ||||||||
| Yes | 975 | 72 | 15.7 | 5257 | 76.6 | 84.4 | 6232 | ||
| No | 379 | 28 | 19.1 | 1604 | 23.4 | 80.9 | 1983 | ||
| Laboratory findings, mean ± std | n | mean ± std | n | mean ± std | Total | p-value | |||
| Serum creatinine (mg/dL) | 1349 | 6.0 ± 2.1 | 6845 | 6.9 ± 2.3 | 8194 | <0.001 | |||
| Hb (g/dL) | 1352 | 9.9 ± 1.3 | 6859 | 10.3 ± 1.4 | 8211 | <0.001 | |||
| CPK (U/L) | 1354 | 8.6 ± 0.8 | 6861 | 8.7 ± 0.8 | 8215 | <0.001 | |||
| Serum phosphate level (mg/dL) | 1338 | 4.7 ± 1.4 | 6809 | 5.0 ± 1.4 | 8147 | <0.001 | |||
| Serum albumin (g/L) | 1344 | 3.4 ± 0.5 | 6833 | 3.6 ± 0.5 | 8177 | <0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelici, L.; Marino, C.; Umbro, I.; Bossola, M.; Calandrini, E.; Tazza, L.; Agabiti, N.; Davoli, M.; on behalf of the Regional Registry Dialysis and Transplant Lazio Region. Gender Disparities in Vascular Access and One-Year Mortality among Incident Hemodialysis Patients: An Epidemiological Study in Lazio Region, Italy. J. Clin. Med. 2021, 10, 5116. https://doi.org/10.3390/jcm10215116
Angelici L, Marino C, Umbro I, Bossola M, Calandrini E, Tazza L, Agabiti N, Davoli M, on behalf of the Regional Registry Dialysis and Transplant Lazio Region. Gender Disparities in Vascular Access and One-Year Mortality among Incident Hemodialysis Patients: An Epidemiological Study in Lazio Region, Italy. Journal of Clinical Medicine. 2021; 10(21):5116. https://doi.org/10.3390/jcm10215116
Chicago/Turabian StyleAngelici, Laura, Claudia Marino, Ilaria Umbro, Maurizio Bossola, Enrico Calandrini, Luigi Tazza, Nera Agabiti, Marina Davoli, and on behalf of the Regional Registry Dialysis and Transplant Lazio Region. 2021. "Gender Disparities in Vascular Access and One-Year Mortality among Incident Hemodialysis Patients: An Epidemiological Study in Lazio Region, Italy" Journal of Clinical Medicine 10, no. 21: 5116. https://doi.org/10.3390/jcm10215116