
Long-Term Weight Outcomes after Bariatric Surgery: A Single Center Saudi Arabian Cohort Experience

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Subjects
2.2. Calculated Variables
2.3. Statistical Analysis
3. Results
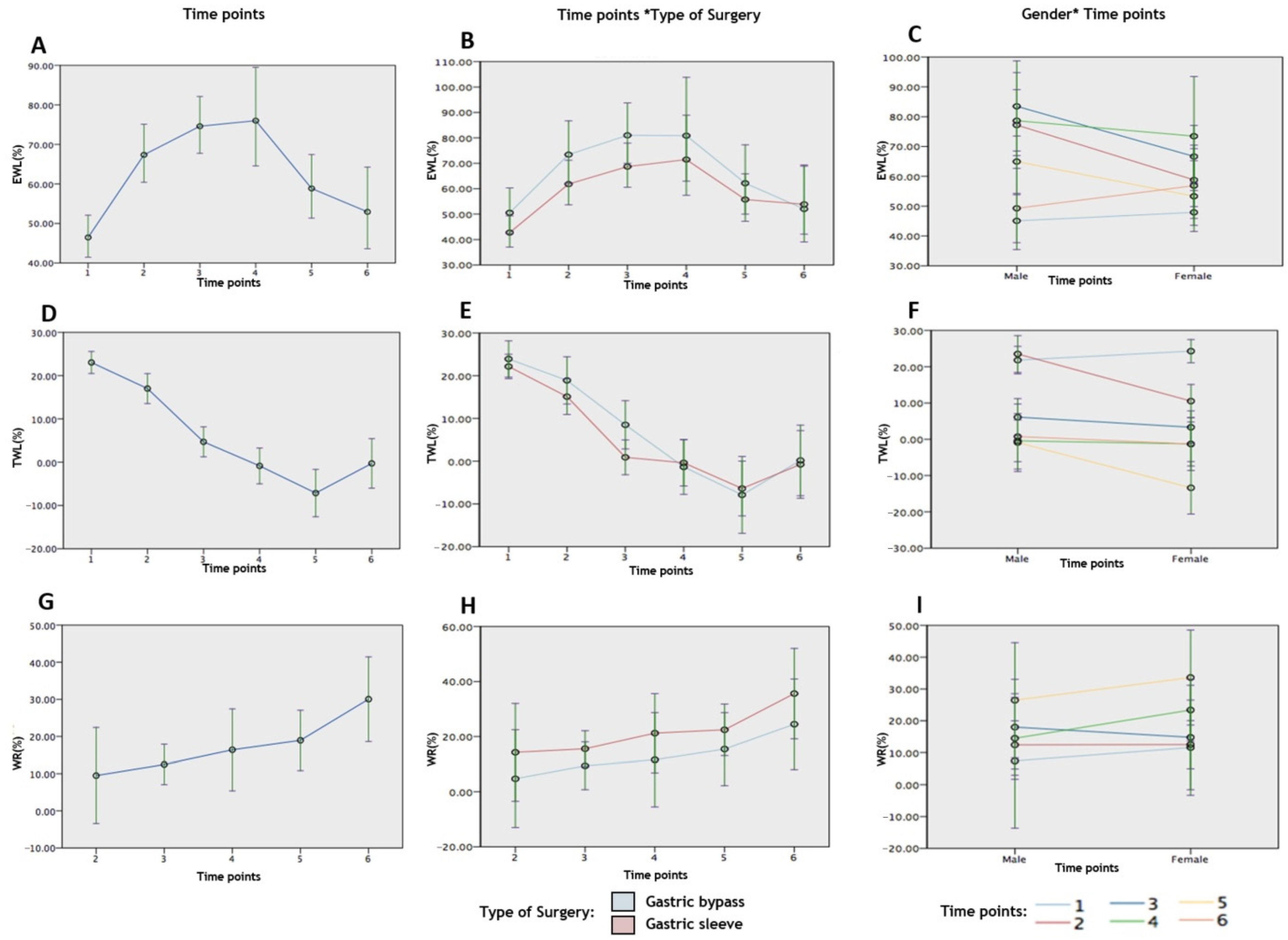
3.1. Univariate Analysis: Generalized Linear Mixed Effects Model Analysis for the Outcome Variables %EWL, %TWL and %WR for Each of the Independent Variables (Time Points, Type of Surgery and Gender)
3.2. Multivariate Analysis: General Linear Mixed Effects Modelling for Each of the Outcome Variables, %EWL, %TWL and %WR with Independent Variables (Time Points, Type of Surgery and Gender)
4. Discussion
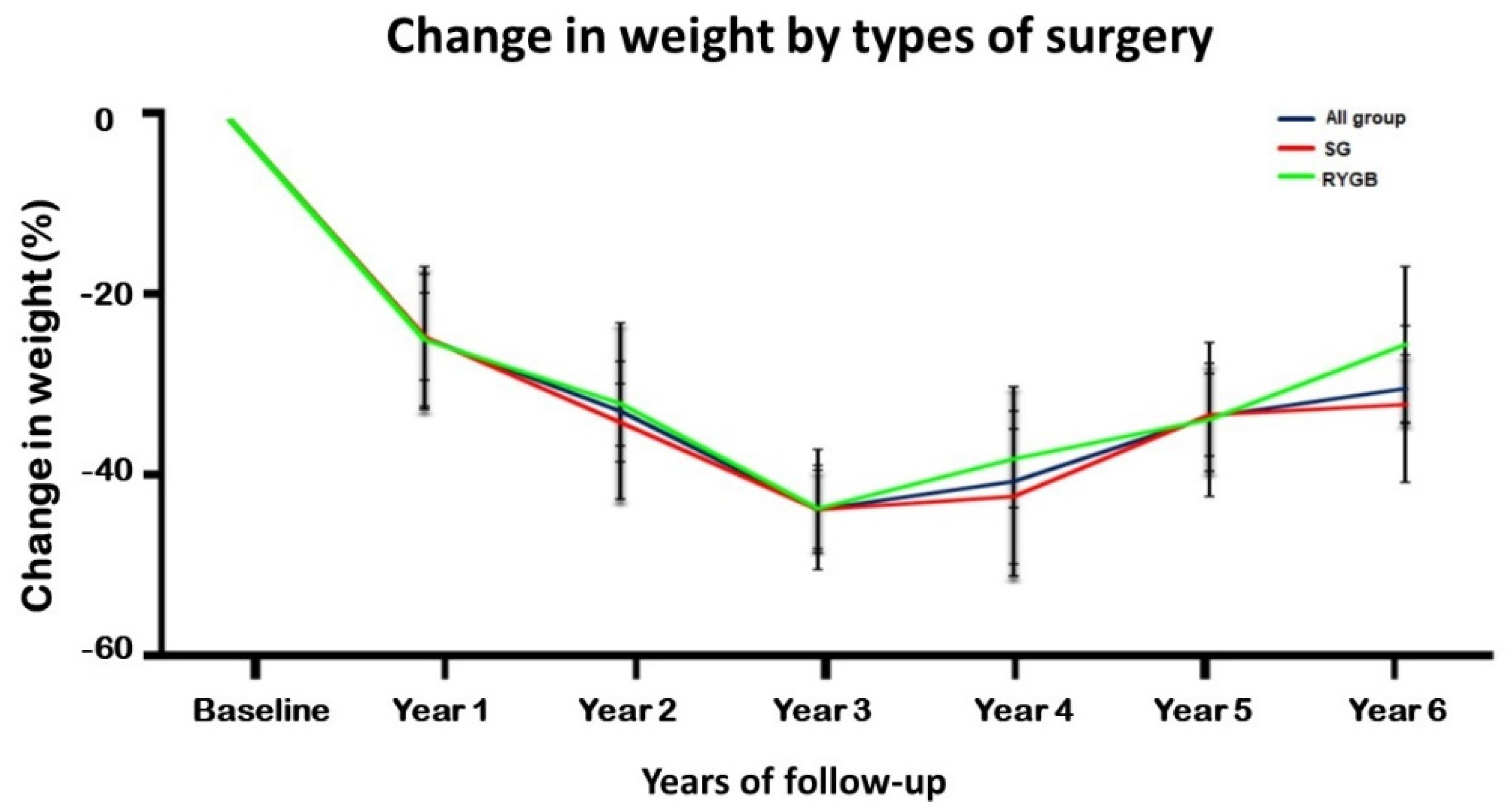
4.1. Weight Evolution in the Overall Bariatric Group
4.2. Weight Loss Patterns between SG and RYGB
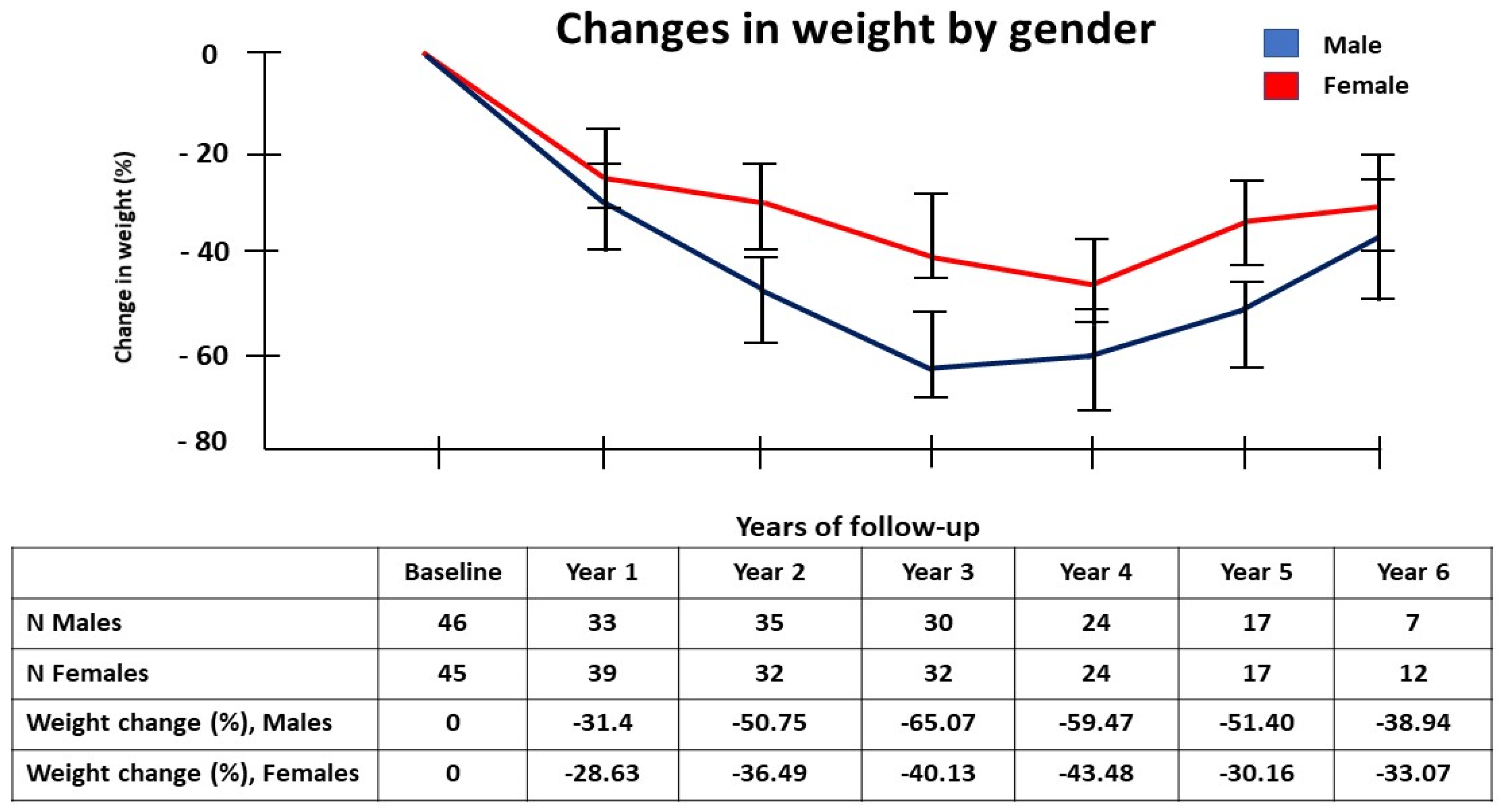
4.3. Weight Loss Changes According to Gender
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Facts about Overweight and Obesity. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 March 2021).
- Memish, Z.A.; El Bcheraoui, C.; Tuffaha, M.; Robinson, M.; Daoud, F.; Jaber, S.; Mikhitarian, S.; Al Saeedi, M.; AlMazroa, M.A.; Mokdad, A.H.; et al. Obesity and associated factors—Kingdom of Saudi Arabia, 2013. Prev. Chronic Dis. 2014, 11, E174. [Google Scholar] [CrossRef] [Green Version]
- Alqarni, S.S.M. A Review of Prevalence of Obesity in Saudi Arabia. J. Obes. Eat. Disord. 2016, 1–6. [Google Scholar] [CrossRef]
- Alfadda, A.A.; Al-Dhwayan, M.M.; Alharbi, A.A.; Al Khudhair, B.K.; Al Nozha, O.M.; Al-Qahtani, N.M.; Alzahrani, S.H.; Bardisi, W.M.; Sallam, R.M.; Riva, J.J.; et al. The Saudi clinical practice guideline for the management of overweight and obesity in adults. Saudi Med. J. 2016, 37, 1151–1162. [Google Scholar] [CrossRef] [PubMed]
- Sjostrom, L.; Narbro, K.; Sjostrom, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [Green Version]
- Geraci, A.A.; Brunt, A.; Marihart, C. The Work behind Weight-Loss Surgery: A Qualitative Analysis of Food Intake after the First Two Years Post-Op. ISRN Obes. 2014, 2014, 427062. [Google Scholar] [CrossRef] [PubMed]
- Mofti, A.B.; Al-Saleh, M.S. Bariatric surgery in Saudi Arabia. Ann. Saudi Med. 1992, 12, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Al-Khaldi, Y.M. Bariatric surgery in Saudi Arabia: The urgent need for standards. Saudi J. Obes. 2016, 4, 1. [Google Scholar] [CrossRef]
- Chou, J.J.; Lee, W.J.; Almalki, O.; Chen, J.C.; Tsai, P.L.; Yang, S.H. Dietary Intake and Weight Changes 5 Years After Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2017, 27, 3240–3246. [Google Scholar] [CrossRef] [PubMed]
- Al-Bader, I.; Khoursheed, M.; Al Sharaf, K.; Mouzannar, D.A.; Ashraf, A.; Fingerhut, A. Revisional Laparoscopic Gastric Pouch Resizing for Inadequate Weight Loss After Roux-en-Y Gastric Bypass. Obes. Surg. 2015, 25, 1103–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, T.D.; Davidson, L.E.; Litwin, S.E.; Kolotkin, R.L.; LaMonte, M.J.; Pendleton, R.C.; Strong, M.B.; Vinik, R.; Wanner, N.A.; Hopkins, P.N.; et al. Health benefits of gastric bypass surgery after 6 years. JAMA 2012, 308, 1122–1131. [Google Scholar] [CrossRef]
- Lauti, M.; Kularatna, M.; Hill, A.G.; MacCormick, A.D. Weight Regain Following Sleeve Gastrectomy—A Systematic Review. Obes. Surg. 2016, 26, 1326–1334. [Google Scholar] [CrossRef]
- Kanerva, N.; Larsson, I.; Peltonen, M.; Lindroos, A.K.; Carlsson, L.M. Changes in total energy intake and macronutrient composition after bariatric surgery predict long-term weight outcome: Findings from the Swedish Obese Subjects (SOS) study. Am. J. Clin. Nutr. 2017, 106, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.C.; Slattery, J.; Bundga, M.E.; Lautz, D.B. Peroral endoscopic reduction of dilated gastrojejunal anastomosis after Roux-en-Y gastric bypass: A possible new option for patients with weight regain. Surg. Endosc. 2006, 20, 1744–1748. [Google Scholar] [CrossRef] [PubMed]
- McGrice, M.; Don Paul, K. Interventions to improve long-term weight loss in patients following bariatric surgery: Challenges and solutions. Diabetes Metab. Syndr. Obes. Targets Ther. 2015, 8, 263–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, M.; Simha, V.; Garg, A. Review: Long-term impact of bariatric surgery on body weight, comorbidities, and nutritional status. J. Clin. Endocrinol. Metab. 2006, 91, 4223–4231. [Google Scholar] [CrossRef] [Green Version]
- Masood, A.; Alsheddi, L.; Alfayadh, L.; Bukhari, B.; Elawad, R.; Alfadda, A.A. Dietary and Lifestyle Factors Serve as Predictors of Successful Weight Loss Maintenance Postbariatric Surgery. J. Obes. 2019, 2019, 7295978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, L.K.; Benotti, P.N.; Dwyer, J.; Roberts, S.B.; Saltzman, E.; Shikora, S.; Rolls, B.J.; Rand, W. Nonsurgical factors that influence the outcome of bariatric surgery: A review. Psychosom. Med. 1998, 60, 338–346. [Google Scholar] [CrossRef]
- Alqahtani, A.R. Reply to Letter to Editor RE: Laparoscopic Sleeve Gastrectomy After Endoscopic Sleeve Gastroplasty: Technical Aspects and Short-Term Outcomes. Obes. Surg. 2020, 30, 338. [Google Scholar] [CrossRef] [Green Version]
- Alqahtani, A.R.; Elahmedi, M.; Alqahtani, Y.A.; Al-Darwish, A. Laparoscopic Sleeve Gastrectomy After Endoscopic Sleeve Gastroplasty: Technical Aspects and Short-Term Outcomes. Obes. Surg. 2019, 29, 3547–3552. [Google Scholar] [CrossRef]
- Carrasco, F.; Papapietro, K.; Csendes, A.; Salazar, G.; Echenique, C.; Lisboa, C.; Diaz, E.; Rojas, J. Changes in resting energy expenditure and body composition after weight loss following Roux-en-Y gastric bypass. Obes. Surg. 2007, 17, 608–616. [Google Scholar] [CrossRef]
- Cooper, T.C.; Simmons, E.B.; Webb, K.; Burns, J.L.; Kushner, R.F. Trends in Weight Regain Following Roux-en-Y Gastric Bypass (RYGB) Bariatric Surgery. Obes. Surg. 2015, 25, 1474–1481. [Google Scholar] [CrossRef] [PubMed]
- Aminian, A.; Jamal, M.; Augustin, T.; Corcelles, R.; Kirwan, J.P.; Schauer, P.R.; Brethauer, S.A. Failed Surgical Weight Loss Does Not Necessarily Mean Failed Metabolic Effects. Diabetes Technol. Ther. 2015, 17, 682–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, J.P.; Jakes, A.D.; Hayden, J.D.; Barth, J.H. Systematic review of definitions of failure in revisional bariatric surgery. Obes. Surg. 2015, 25, 571–574. [Google Scholar] [CrossRef]
- Sabench Pereferrer, F.; Molina Lopez, A.; Vives Espelta, M.; Raga Carceller, E.; Blanco Blasco, S.; Buils Vilalta, F.; Paris Sans, M.; Pinana Campon, M.L.; Hernandez Gonzalez, M.; Sanchez Marin, A.; et al. Weight Loss Analysis According to Different Formulas after Sleeve Gastrectomy With or Without Antral Preservation: A Randomised Study. Obes. Surg. 2017, 27, 1254–1260. [Google Scholar] [CrossRef]
- Cooper, C.L.; Whitehead, A.; Pottrill, E.; Julious, S.A.; Walters, S.J. Are pilot trials useful for predicting randomisation and attrition rates in definitive studies: A review of publicly funded trials. Clin. Trials 2018, 15, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Schauer, P.R.; Bhatt, D.L.; Kirwan, J.P.; Wolski, K.; Aminian, A.; Brethauer, S.A.; Navaneethan, S.D.; Singh, R.P.; Pothier, C.E.; Nissen, S.E.; et al. Bariatric Surgery versus Intensive Medical Therapy for Diabete—5-Year Outcomes. N. Engl. J. Med. 2017, 376, 641–651. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, L.M.S.; Sjoholm, K.; Karlsson, C.; Jacobson, P.; Andersson-Assarsson, J.C.; Svensson, P.A.; Larsson, I.; Hjorth, S.; Neovius, M.; Taube, M.; et al. Long-term incidence of microvascular disease after bariatric surgery or usual care in patients with obesity, stratified by baseline glycaemic status: A post-hoc analysis of participants from the Swedish Obese Subjects study. Lancet. Diabetes Endocrinol. 2017, 5, 271–279. [Google Scholar] [CrossRef] [Green Version]
- Sjoholm, K.; Pajunen, P.; Jacobson, P.; Karason, K.; Sjostrom, C.D.; Torgerson, J.; Carlsson, L.M.; Sjostrom, L.; Peltonen, M. Incidence and remission of type 2 diabetes in relation to degree of obesity at baseline and 2 year weight change: The Swedish Obese Subjects (SOS) study. Diabetologia 2015, 58, 1448–1453. [Google Scholar] [CrossRef]
- Kroes, M.; Osei-Assibey, G.; Baker-Searle, R.; Huang, J. Impact of weight change on quality of life in adults with overweight/obesity in the United States: A systematic review. Curr. Med. Res. Opin. 2016, 32, 485–508. [Google Scholar] [CrossRef]
- Ionut, V.; Bergman, R.N. Mechanisms responsible for excess weight loss after bariatric surgery. J. Diabetes Sci. Technol. 2011, 5, 1263–1282. [Google Scholar] [CrossRef] [Green Version]
- Buchwald, H.; Buchwald, J.N.; McGlennon, T.W. Systematic review and meta-analysis of medium-term outcomes after banded Roux-en-Y gastric bypass. Obes. Surg. 2014, 24, 1536–1551. [Google Scholar] [CrossRef] [PubMed]
- Puzziferri, N.; Roshek, T.B., 3rd; Mayo, H.G.; Gallagher, R.; Belle, S.H.; Livingston, E.H. Long-term follow-up after bariatric surgery: A systematic review. JAMA 2014, 312, 934–942. [Google Scholar] [CrossRef] [Green Version]
- Christou, N.V.; Look, D.; Maclean, L.D. Weight gain after short- and long-limb gastric bypass in patients followed for longer than 10 years. Ann. Surg. 2006, 244, 734–740. [Google Scholar] [CrossRef]
- Diniz Mde, F.; Passos, V.M.; Barreto, S.M.; Linares, D.B.; de Almeida, S.R.; Rocha, A.L.; Diniz, M.T. Different criteria for assessment of Roux-en-Y gastric bypass success: Does only weight matter? Obes. Surg. 2009, 19, 1384–1392. [Google Scholar] [CrossRef] [PubMed]
- Admiraal, W.M.; Celik, F.; Gerdes, V.E.; Dallal, R.M.; Hoekstra, J.B.; Holleman, F. Ethnic differences in weight loss and diabetes remission after bariatric surgery: A meta-analysis. Diabetes Care 2012, 35, 1951–1958. [Google Scholar] [CrossRef] [Green Version]
- Bohdjalian, A.; Langer, F.B.; Shakeri-Leidenmuhler, S.; Gfrerer, L.; Ludvik, B.; Zacherl, J.; Prager, G. Sleeve gastrectomy as sole and definitive bariatric procedure: 5-year results for weight loss and ghrelin. Obes. Surg. 2010, 20, 535–540. [Google Scholar] [CrossRef]
- Ochner, C.N.; Jochner, M.C.; Caruso, E.A.; Teixeira, J.; Xavier Pi-Sunyer, F. Effect of preoperative body mass index on weight loss after obesity surgery. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2013, 9, 423–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastos, E.C.; Barbosa, E.M.; Soriano, G.M.; dos Santos, E.A.; Vasconcelos, S.M. Determinants of weight regain after bariatric surgery. Arq. Bras. Cir. Dig. ABCD Braz. Arch. Dig. Surg. 2013, 26 (Suppl. 1), 26–32. [Google Scholar] [CrossRef]
- Thomas, D.D.; Anderson, W.A.; Apovian, C.M.; Hess, D.T.; Yu, L.; Velazquez, A.; Carmine, B.; Istfan, N.W. Weight Recidivism After Roux-en-Y Gastric Bypass Surgery: An 11-Year Experience in a Multiethnic Medical Center. Obesity 2019, 27, 217–225. [Google Scholar] [CrossRef] [Green Version]
- Nicoletti, C.F.; de Oliveira, B.A.; de Pinhel, M.A.; Donati, B.; Marchini, J.S.; Salgado Junior, W.; Nonino, C.B. Influence of excess weight loss and weight regain on biochemical indicators during a 4-year follow-up after Roux-en-Y gastric bypass. Obes. Surg. 2015, 25, 279–284. [Google Scholar] [CrossRef]
- Still, C.D.; Wood, G.C.; Chu, X.; Manney, C.; Strodel, W.; Petrick, A.; Gabrielsen, J.; Mirshahi, T.; Argyropoulos, G.; Seiler, J.; et al. Clinical factors associated with weight loss outcomes after Roux-en-Y gastric bypass surgery. Obesity 2014, 22, 888–894. [Google Scholar] [CrossRef] [Green Version]
- Wood, M.H.; Carlin, A.M.; Ghaferi, A.A.; Varban, O.A.; Hawasli, A.; Bonham, A.J.; Birkmeyer, N.J.; Finks, J.F. Association of Race With Bariatric Surgery Outcomes. JAMA Surg. 2019, 154, e190029. [Google Scholar] [CrossRef]
- Santo, M.A.; Riccioppo, D.; Pajecki, D.; Kawamoto, F.; de Cleva, R.; Antonangelo, L.; Marcal, L.; Cecconello, I. Weight Regain After Gastric Bypass: Influence of Gut Hormones. Obes. Surg. 2016, 26, 919–925. [Google Scholar] [CrossRef]
- Ionut, V.; Burch, M.; Youdim, A.; Bergman, R.N. Gastrointestinal hormones and bariatric surgery-induced weight loss. Obesity 2013, 21, 1093–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jirapinyo, P.; Jin, D.X.; Qazi, T.; Mishra, N.; Thompson, C.C. A Meta-Analysis of GLP-1 After Roux-En-Y Gastric Bypass: Impact of Surgical Technique and Measurement Strategy. Obes. Surg. 2018, 28, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Tsouristakis, A.I.; Febres, G.; McMahon, D.J.; Tchang, B.; Conwell, I.M.; Tsang, A.J.; Ahmed, L.; Bessler, M.; Korner, J. Long-Term Modulation of Appetitive Hormones and Sweet Cravings After Adjustable Gastric Banding and Roux-en-Y Gastric Bypass. Obes. Surg. 2019, 29, 3698–3705. [Google Scholar] [CrossRef]
- Benaiges, D.; Climent, E.; Goday, A.; Julia, H.; Flores-Le Roux, J.A.; Pedro-Botet, J. Mid-term results of laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy compared-results of the SLEEVEPASS and SM-BOSS trials. Ann. Transl. Med. 2018, 6, S83. [Google Scholar] [CrossRef] [PubMed]
- Pucci, A.; Batterham, R.L. Mechanisms underlying the weight loss effects of RYGB and SG: Similar, yet different. J. Endocrinol. Investig. 2019, 42, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Kaouk, L.; Hsu, A.; Tanuseputro, P.; Jessri, M. Modifiable factors associated with weight regain after bariatric surgery: A scoping review. F1000Research 2019, 8, 615. [Google Scholar] [CrossRef] [PubMed]
- Freire, R.H.; Borges, M.C.; Alvarez-Leite, J.I.; Toulson Davisson Correia, M.I. Food quality, physical activity, and nutritional follow-up as determinant of weight regain after Roux-en-Y gastric bypass. Nutrition 2012, 28, 53–58. [Google Scholar] [CrossRef]
- Xu, H.C.; Pang, Y.C.; Chen, J.W.; Cao, J.Y.; Sheng, Z.; Yuan, J.H.; Wang, R.; Zhang, C.S.; Wang, L.X.; Dong, J. Systematic Review and Meta-analysis of the Change in Ghrelin Levels After Roux-en-Y Gastric Bypass. Obes. Surg. 2019, 29, 1343–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, A.E.; Thornley, C.J.; Blackstone, R.P. Outcomes in Bariatric and Metabolic Surgery: An Updated 5-Year Review. Curr. Obes. Rep. 2020, 9, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Tymitz, K.; Kerlakian, G.; Engel, A.; Bollmer, C. Gender differences in early outcomes following hand-assisted laparoscopic Roux-en-Y gastric bypass surgery: Gender differences in bariatric surgery. Obes. Surg. 2007, 17, 1588–1591. [Google Scholar] [CrossRef]
- Ranasinghe, W.K.; Wright, T.; Attia, J.; McElduff, P.; Doyle, T.; Bartholomew, M.; Hurley, K.; Persad, R.A. Effects of bariatric surgery on urinary and sexual function. BJU Int. 2011, 107, 88–94. [Google Scholar] [CrossRef]
- Infanger, D.; Baldinger, R.; Branson, R.; Barbier, T.; Steffen, R.; Horber, F.F. Effect of significant intermediate-term weight loss on serum leptin levels and body composition in severely obese subjects. Obes. Surg. 2003, 13, 879–888. [Google Scholar] [CrossRef]
- Meguid, M.M.; Glade, M.J.; Middleton, F.A. Weight regain after Roux-en-Y: A significant 20% complication related to PYY. Nutrition 2008, 24, 832–842. [Google Scholar] [CrossRef] [PubMed]
- Vennapusa, A.; Panchangam, R.B.; Kesara, C.; Chivukula, T. Response: Factors Predicting Weight Loss after “Sleeve Gastrectomy with Loop Duodenojejunal Bypass” Surgery for Obesity. J. Obes. Metab. Syndr. 2020, 29, 327–329. [Google Scholar] [CrossRef]
- Barhouch, A.S.; Padoin, A.V.; Casagrande, D.S.; Chatkin, R.; Sussenbach, S.P.; Pufal, M.A.; Rossoni, C.; Mottin, C.C. Predictors of Excess Weight Loss in Obese Patients After Gastric Bypass: A 60-Month Follow-up. Obes. Surg. 2016, 26, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Higa, K.; Ho, T.; Tercero, F.; Yunus, T.; Boone, K.B. Laparoscopic Roux-en-Y gastric bypass: 10-year follow-up. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2011, 7, 516–525. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Variables | |
|---|---|
| Gender | |
| Male Female | 46 (50.5%) 45 (49.5%) |
| Type of Surgery | |
| Sleeve Gastrectomy Roux-en-Y Gastric Bypass | 62 (68.1%) 29 (31.9%) |
| Age at baseline, in years | |
| Mean ± SD Range | 33.3 ± 9.7 17–60 |
| Height, in meters | |
| Mean ± SD Range | 1.64 ± 0.1 1.45–1.90 |
| Pre-surgery weight, in kilograms | |
| Mean ± SD Range | 134.4 ± 33.8 78.1–300.7 |
| Pre-surgery BMI, in kg/m2 | |
| Mean ± SD Range | 49.7 ± 9.9 29.4–83.3 |
| Time Points (in Years) | F-Value | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|
| Outcome Variables | 1st | 2nd | 3rd | 4th | 5th | 6th | ||
| %EWL | 45.46 (21.9) | 65.71 (32.0) | 73.14 (28.8) | 75.12 (43.4) | 58.04 (22.5) | 54.11 (20.3) | 10.82 | <0.0001 |
| %TWL | 22.87 (10.0) | 16.07 (15.6) | 3.47 (13.2) | −0.73 (14.1) | −7.08 (16.4) | −0.49 (12.1) | 43.99 | <0.0001 |
| %WR | – | 10.20 (12.9) | 13.32 (12.1) | 17.58 (29.1) | 20.81 (18.7) | 30.38 (20.9) | 2.72 | 0.034 |
| Outcome Variables, Type of Surgery and Gender | Time Points (in Years) | F-Value | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1st | 2nd | 3rd | 4th | 5th | 6th | ||||
| %EWL | RYGB | 51.21 (21.0) | 71.18 (40.2) | 79.0 (41.1) | 80.04 (52.8) | 60.7 (23.1) | 54.20 (20.3) | 2.89 | 0.018 |
| SG | 42.64 (21.9) | 62.80 (26.7) | 69.91 (18.8) | 72.20 (37.3) | 56.78 (22.6) | 54.02 (21.5) | 9.27 | <0.0001 | |
| %TWL | RYGB | 24.41 (9.1) | 17.23 (14.4) | 8.04 (14.1) | −1.43 (15.6) | −9.96 (13.1) | −0.23 (14.9) | 20.53 | <0.0001 |
| SG | 22.12 (10.5) | 15.4 (16.4) | 1.01 (12.1) | −0.24 (13.2) | −5.58 (18.0) | −0.755 (9.3) | 27.63 | <0.0001 | |
| WR | RYGB | – | 5.42 (6.1) | 9.41 (7.5) | 11.31 (12.5) | 17.91 (16.2) | 26.25 (19.9) | 2.28 | 0.080 |
| SG | – | 14.97 (17.6) | 15.55 (13.8) | 21.76 (36) | 22.44 (20.2) | 35.1 (22.9) | 1.27 | 0.294 | |
| %EWL | Male | 42.96 (24.1) | 74.34 (38.2) | 80.54 (36.1) | 76.26 (48.1) | 63.15 (26.3) | 49.64 (20.5) | 7.22 | <0.0001 |
| Female | 47.52 (19.9) | 58.15 (23.3) | 66.21 (17.3) | 73.84 (38.4) | 52.93 (17.1) | 56.71 (20.7) | 4.74 | <0.0001 | |
| %TWL | Male | 21.32 (10.8) | 22.72 (17.0) | 4.20 (15.5) | −0.23 (17.9) | −0.51 (14.2) | 0.62 (8.6) | 16.67 | <0.0001 |
| Female | 24.13 (9.2) | 10.29 (11.7) | 2.84 (10.9) | −1.34 (7.5) | −13.3 (16.3) | −1.24 (14.3) | 39.15 | <0.0001 | |
| %WR | Male | – | 7.42 (7.1) | 13.28 (13.4) | 20.0 (37.4) | 16.61 (13.4) | 28.33 (18.0) | 1.54 | 0.209 |
| Female | – | 11.59 (15.9) | 13.36 (11.3) | 14.42 (12.8) | 23.62 (21.4) | 31.75 (23.6) | 1.74 | 0.156 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfadda, A.A.; Al-Naami, M.Y.; Masood, A.; Elawad, R.; Isnani, A.; Ahamed, S.S.; Alfadda, N.A. Long-Term Weight Outcomes after Bariatric Surgery: A Single Center Saudi Arabian Cohort Experience. J. Clin. Med. 2021, 10, 4922. https://doi.org/10.3390/jcm10214922
Alfadda AA, Al-Naami MY, Masood A, Elawad R, Isnani A, Ahamed SS, Alfadda NA. Long-Term Weight Outcomes after Bariatric Surgery: A Single Center Saudi Arabian Cohort Experience. Journal of Clinical Medicine. 2021; 10(21):4922. https://doi.org/10.3390/jcm10214922
Chicago/Turabian StyleAlfadda, Assim A., Mohammed Y. Al-Naami, Afshan Masood, Ruba Elawad, Arthur Isnani, Shaik Shaffi Ahamed, and Nora A. Alfadda. 2021. "Long-Term Weight Outcomes after Bariatric Surgery: A Single Center Saudi Arabian Cohort Experience" Journal of Clinical Medicine 10, no. 21: 4922. https://doi.org/10.3390/jcm10214922