Characteristics of Patients Managed without Positive Pressure Ventilation While on Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Data Source and Study Population
2.2. Study Variables and Outcomes
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Acute Respiratory Distress Syndrome Network. Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, R.P.; MacLaren, G.; Boonstra, P.S.; Iwashyna, T.J.; Slutsky, A.S.; Fan, E.; Bartlett, R.H.; Tonna, J.E.; Hyslop, R.; Fanning, J.J.; et al. Extracorporeal membrane oxygenation support in COVID-19: An international cohort study of the Extracorporeal Life Support Organization registry. Lancet 2020. [Google Scholar] [CrossRef]
- Tonna, J.E.; Selzman, C.H.; Mallin, M.P.; Smith, B.R.; Youngquist, S.T.; Koliopoulou, A.; Welt, F.; Stoddard, K.D.; Nirula, R.; Barton, R.; et al. Development and Implementation of a Comprehensive, Multidisciplinary Emergency Department Extracorporeal Membrane Oxygenation Program. Ann. Emerg. Med. 2017, 70, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Tonna, J.E.; Selzman, C.H.; Girotra, S.; Presson, A.P.; Thiagarajan, R.R.; Becker, L.B.; Zhang, C.; Keenan, H.T. American Heart Association’s Get With the Guidelines-Resuscitation, I. Patient and Institutional Characteristics Influence the Decision to Use Extracorporeal Cardiopulmonary Resuscitation for In-Hospital Cardiac Arrest. J. Am. Heart Assoc. 2020, 9, e015522. [Google Scholar] [CrossRef] [PubMed]
- Acharya, D.; Torabi, M.; Borgstrom, M.; Rajapreyar, I.; Lee, K.; Kern, K.; Rycus, P.; Tonna, J.E.; Alexander, P.; Lotun, K. Extracorporeal Membrane Oxygenation in Myocardial Infarction Complicated by Cardiogenic Shock: Analysis of the ELSO Registry. J. Am. Coll Cardiol. 2020, 76, 1001–1002. [Google Scholar] [CrossRef]
- Yeo, H.J.; Cho, W.H.; Kim, D. Awake extracorporeal membrane oxygenation in patients with severe postoperative acute respiratory distress syndrome. J. Thorac. Dis. 2016, 8, 37–42. [Google Scholar] [CrossRef]
- Ellouze, O.; Lamirel, J.; Perrot, J.; Missaoui, A.; Daily, T.; Aho, S.; Petrosyan, A.; Guinot, P.G.; Bouchot, O.; Bouhemad, B. Extubation of patients undergoing extracorporeal life support. A retrospective study. Perfusion 2019, 34, 50–57. [Google Scholar] [CrossRef]
- Langer, T.; Vecchi, V.; Belenkiy, S.M.; Cannon, J.W.; Chung, K.K.; Cancio, L.C.; Gattinoni, L.; Batchinsky, A.I. Extracorporeal gas exchange and spontaneous breathing for the treatment of acute respiratory distress syndrome: An alternative to mechanical ventilation?*. Crit. Care Med. 2014, 42, e211–e220. [Google Scholar] [CrossRef]
- Abrams, D.; Garan, A.R.; Brodie, D. Awake and fully mobile patients on cardiac extracorporeal life support. Ann. Cardiothorac. Surg. 2019, 8, 44–53. [Google Scholar] [CrossRef] [Green Version]
- Pandharipande, P.; Shintani, A.; Peterson, J.; Pun, B.T.; Wilkinson, G.R.; Dittus, R.S.; Bernard, G.R.; Ely, E.W. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology 2006, 104, 21–26. [Google Scholar] [CrossRef]
- Xia, J.; Gu, S.; Li, M.; Liu, D.; Huang, X.; Yi, L.; Wu, L.; Fan, G.; Zhan, Q. Spontaneous breathing in patients with severe acute respiratory distress syndrome receiving prolonged extracorporeal membrane oxygenation. BMC Pulm. Med. 2019, 19, 237. [Google Scholar] [CrossRef] [PubMed]
- Kurihara, C.; Walter, J.M.; Singer, B.D.; Cajigas, H.; Shayan, S.; Al-Qamari, A.; DeCamp, M.M.; Wunderink, R.; Budinger, G.R.S.; Bharat, A. Extracorporeal Membrane Oxygenation Can Successfully Support Patients With Severe Acute Respiratory Distress Syndrome in Lieu of Mechanical Ventilation. Crit. Care Med. 2018, 46, e1070–e1073. [Google Scholar] [CrossRef] [PubMed]
- Nosotti, M.; Rosso, L.; Tosi, D.; Palleschi, A.; Mendogni, P.; Nataloni, I.F.; Crotti, S.; Tarsia, P. Extracorporeal membrane oxygenation with spontaneous breathing as a bridge to lung transplantation. Interact. Cardiovasc. Thorac. Surg. 2013, 16, 55–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuehner, T.; Kuehn, C.; Hadem, J.; Wiesner, O.; Gottlieb, J.; Tudorache, I.; Olsson, K.M.; Greer, M.; Sommer, W.; Welte, T.; et al. Extracorporeal membrane oxygenation in awake patients as bridge to lung transplantation. Am. J. Respir. Crit. Care Med. 2012, 185, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Tonna, J.E.; McKellar, S.H.; Selzman, C.H.; Drakos, S.; Koliopoulou, A.G.; Taleb, I.; Stoddard, G.J.; Stehlik, J.; Welt, F.G.P.; Fair, J.F., 3rd; et al. Exploratory analysis of myocardial function after extracorporeal cardiopulmonary resuscitation vs conventional cardiopulmonary resuscitation. BMC Res. Notes 2020, 13, 137. [Google Scholar] [CrossRef] [PubMed]
- Tonna, J.E.; Johnson, J.; Presson, A.; Zhang, C.; Noren, C.; Lohse, B.; Bento, H.; Barton, R.G.; Nirula, R.; Mone, M.; et al. Short-Term Clinical and Quality Outcomes Have Inconsistent Changes From a Quality Improvement Initiative to Increase Access to Physical Therapy in the Cardiovascular and Surgical ICU. Crit. Care Explor. 2019, 1, e0055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riker, R.R.; Picard, J.T.; Fraser, G.L. Prospective evaluation of the Sedation-Agitation Scale for adult critically ill patients. Crit. Care Med. 1999, 27, 1325–1329. [Google Scholar] [CrossRef]
- Ko, Y.; Cho, Y.H.; Park, Y.H.; Lee, H.; Suh, G.Y.; Yang, J.H.; Park, C.M.; Jeon, K.; Chung, C.R. Feasibility and Safety of Early Physical Therapy and Active Mobilization for Patients on Extracorporeal Membrane Oxygenation. ASAIO J. 2015, 61, 564–568. [Google Scholar] [CrossRef]
- Abrams, D.; Javidfar, J.; Farrand, E.; Mongero, L.B.; Agerstrand, C.L.; Ryan, P.; Zemmel, D.; Galuskin, K.; Morrone, T.M.; Boerem, P.; et al. Early mobilization of patients receiving extracorporeal membrane oxygenation: A retrospective cohort study. Crit. Care 2014, 18, R38. [Google Scholar] [CrossRef] [Green Version]
- Pasrija, C.; Mackowick, K.M.; Raithel, M.; Tran, D.; Boulos, F.M.; Deatrick, K.B.; Mazzeffi, M.A.; Rector, R.; Pham, S.M.; Griffith, B.P.; et al. Ambulation with Femoral Arterial Cannulation Can be Safely Performed on Veno-Arterial Extracorporeal Membrane Oxygenation. Ann. Thorac. Surg. 2018. [Google Scholar] [CrossRef]
- Johnson, J.K.; Lohse, B.; Bento, H.A.; Noren, C.S.; Marcus, R.L.; Tonna, J.E. Improving Outcomes for Critically Ill Cardiovascular Patients Through Increased Physical Therapy Staffing. Arch. Phys. Med. Rehabil. 2019, 100, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.; Nguyen, T.; Taylor, N.; Friscia, M.E.; Budak, M.T.; Rothenberg, P.; Zhu, J.; Sachdeva, R.; Sonnad, S.; Kaiser, L.R.; et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N. Engl. J. Med. 2008, 358, 1327–1335. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All (n = 65) | Presence of Positive Pressure Ventilation on ECMO (n = 48) | Absence of Positive Pressure Ventilation on ECMO (n = 17) | p-Value | |
|---|---|---|---|---|
| Age—yr | 44.3 ± 4.05 | 44.5 ± 2.4 | 43.8 ± 4.1 | p = 0.887 |
| Female Sex—no. (%) | 19 (29.2) | 16 (33.3) | 3 (17.7) | p = 0.222 |
| Male Sex—no. (%) | 46 (70.8) | 32 (66.7) | 14 (82.4) | p = 0.222 |
| Medical Problems—no. (%) | ||||
| End-Stage Renal Disease | 1 (1.54) | 0 (0.0) | 1 (5.9) | p = 0.090 |
| Cancer (active or observation) | 2 (3.1) | 1 (2.08) | 1 (5.9) | p = 0.436 |
| Stroke and/or TIA 1 | 3 (4.62) | 2 (4.2) | 1 (5.9) | p = 0.772 |
| Hypertension | 25 (38.5) | 18 (37.5) | 7 (41.2) | p = 0.789 |
| Hyperlipidemia | 11 (16.9) | 9 (18.8) | 2 (11.8) | p = 0.509 |
| Diabetes | 7 (10.8) | 5 (10.4) | 2 (11.8) | p = 0.878 |
| Coronary artery disease | 10 (15.4) | 8 (16.7) | 2 (11.8) | p = 0.630 |
| Congestive heart failure | 7 (10.8) | 4 (8.3) | 3 (17.7) | p = 0.287 |
| Respiratory disease (COPD 2, Asthma) | 19 (29.2) | 15 (31.3) | 4 (23.5) | p = 0.548 |
| DVT 3 or PE 4 | 1 (1.5) | 1 (2.1) | 0 (0.0) | p = 0.549 |
| Seizures | 0 (0) | 0 (0) | 0 (0) | n/a |
| Cirrhosis of the liver | 0 (0) | 0 (0) | 0 (0) | n/a |
| Unknown | 2 (3.1) | 2 (4.2) | 0 (0) | p = 0.393 |
| None | 7 (10.77) | 5 (10.4) | 2 (11.8) | p = 0.578 |
| All (n = 65) | Presence of Positive Pressure Ventilation on ECMO (n = 48) | Absence of Positive Pressure Ventilation on ECMO (n = 17) | p-Value | |
|---|---|---|---|---|
| Murray Score—mean | 1.34 ± 0.3 | 1.04 ± 0.3 | 2.5 ± 0.6 | p = 0.031 |
| ECMO Duration—days | 14.1 ± 2.2 | 13.7 ± 3.3 | 14.7 ± 2.3 | p = 0.833 |
| Duration of MV 1 prior to ECMO—days | 5.23 ± 0.95 | 5.0 ± 1.1 | 6.1 ± 2.1 | p = 0.634 |
| Ventilator Days—mean | 18.8 ± 2.6 | 16.9 ± 2.9 | 23.9 ± 5.8 | p = 0.240 |
| Ventilator Free Days | ||||
| At day 30—mean | 7.66 ± 1.5 | 5.92 ± 1.6 | 12.5 ± 3.2 | p = 0.049 |
| At day 60—mean | 21.2 ± 3.3 | 15.5 ± 3.7 | 36.9 ± 5.3 | p = 0.003 |
| Ventilator settings (average of first three days on ECMO)—mean | ||||
| PaO2 2/FiO2 3 | 1.0 ± 0.6 | 1.1 ± 0.7 | .87 ± 0.12 | p = 0.183 |
| PEEP | 11.8 ± 0.7 | 11.7 ± 0.9 | 12.1 ± 0.9 | p = 0.779 |
| Respiratory Rate | 20.7 ± 0.8 | 20.7 ± 0.97 | 20.9 ± 1.3 | p = 0.916 |
| Peak Inspiratory Rate | 12.7 ± 0.6 | 12.7 ± 0.8 | 12.7 ± 0.9 | p = 0.982 |
| Compliance | 24.5 ± 3.3 | 21.8 ± 2.7 | 35.3 ± 12.0 | p = 0.101 |
| All (n = 65) | Presence of Positive Pressure Ventilation on ECMO (n = 48) | Absence of Positive Pressure Ventilation on ECMO (n = 17) | p-Value | |
|---|---|---|---|---|
| Time from cannulation to mobilization—days | 14.02 ± 2.3 | 18.3 ± 3.4 | 7.1 ± 1.5 | p = 0.015 |
| Time from cannulation to extubation—days | 10.5 ± 2.3 | 11.5 ± 3.0 | 9.2 ± 3.7 | p = 0.626 |
| Time from extubation to discharge—days | 10.9 ± 1.2 | 11.5 ± 1.7 | 10.1 ± 2.0 | p = 0.599 |
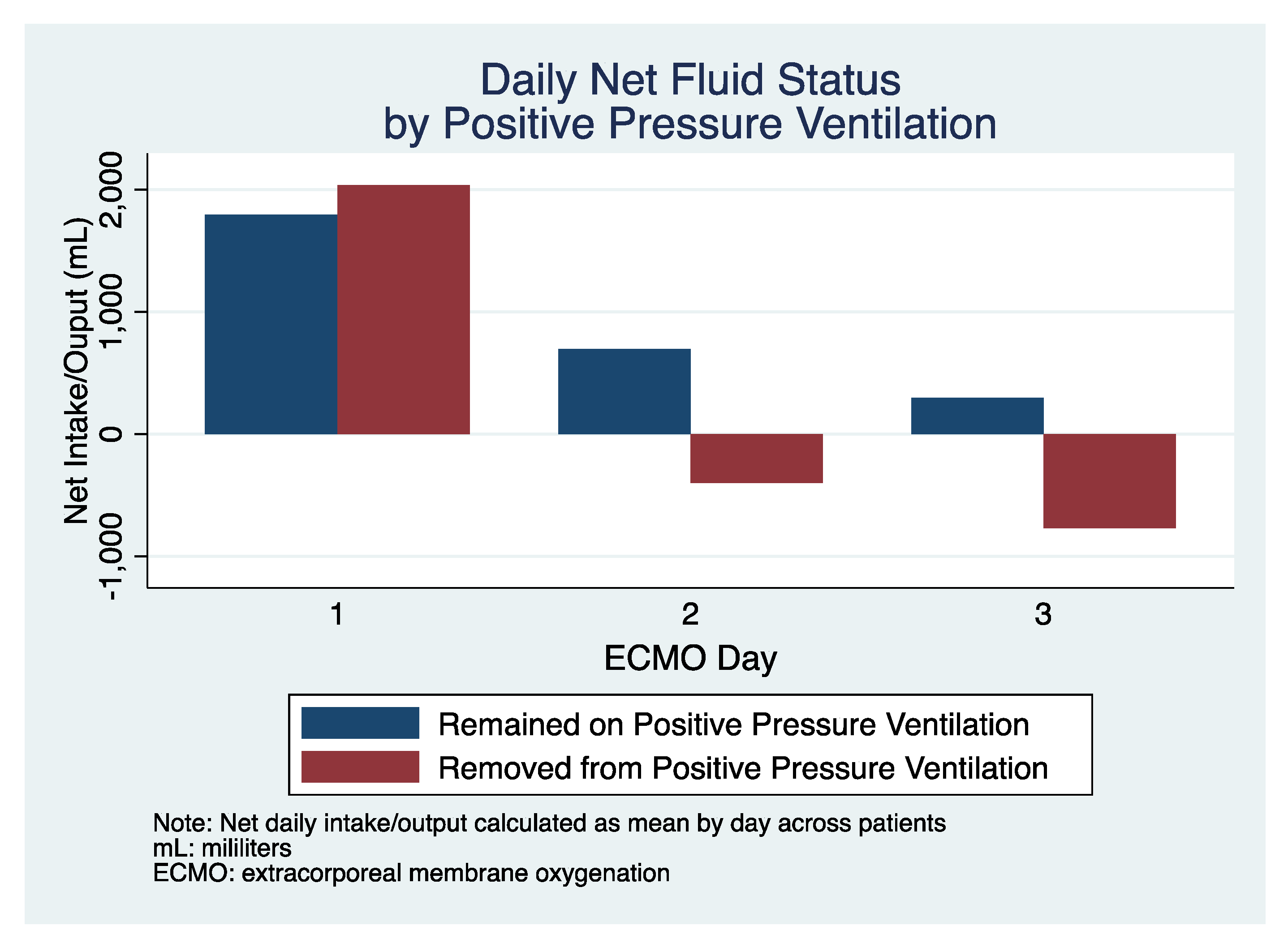
| Total Fluid Balance (first three days)—mL | + 591 (341) | +761 (410) | +176 (624) | p = 0.441 |
| Riker SAS 1 (highest first three days) | 3.01 ± 0.2 | 2.8 ± 0.2 | 3.6 ± 0.3 | p = 0.049 |
| Average time until GCS 11T or greater—days | 9.21 ± 1.2 | 8.1 ± 2.2 | 9.7 ± 1.5 | p = 0.553 |
| LOS 2, if survived to discharge—days (mean) | 37.0 (4.3) | 41.6 (6.4) | 31.0 (5.0) | p = 0.222 |
| Survived to hospital discharge—no. (%) | 39 (60.0) | 22 (45.8) | 17 (100.0) | p < 0.001 |
| Discharge Location—no. (%) | ||||
| Home | 15 (38.5) | 8 (36.4) | 7 (41.2) | p = 0.674 |
| LTAC 3 | 8 (20.5) | 4 (18.2) | 4 (23.5) | |
| SNF 4 | 1 (2.6) | 0 (0) | 1 (5.9) | |
| Rehab | 13 (33.3) | 8 (36.4) | 5 (29.4) | |
| VA | 0 (0) | 0 (0) | 0 (0) | |
| Other Non-VA Hospital | 1 (2.6) | 1 (4.6) | 0 (0) | |
| Other | 1 (2.6) | 1 (4.6) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levin, N.M.; Ciullo, A.L.; Overton, S.; Mitchell, N.; Skidmore, C.R.; Tonna, J.E. Characteristics of Patients Managed without Positive Pressure Ventilation While on Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. J. Clin. Med. 2021, 10, 251. https://doi.org/10.3390/jcm10020251
Levin NM, Ciullo AL, Overton S, Mitchell N, Skidmore CR, Tonna JE. Characteristics of Patients Managed without Positive Pressure Ventilation While on Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. Journal of Clinical Medicine. 2021; 10(2):251. https://doi.org/10.3390/jcm10020251
Chicago/Turabian StyleLevin, Nicholas M, Anna L Ciullo, Sean Overton, Nathan Mitchell, Chloe R Skidmore, and Joseph E Tonna. 2021. "Characteristics of Patients Managed without Positive Pressure Ventilation While on Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome" Journal of Clinical Medicine 10, no. 2: 251. https://doi.org/10.3390/jcm10020251